I had a patient with non-valvular atrial flutter denied dabigatran (Pradaxa®) by their insurer recently. The patient had diabetes, hypertension and has had a heck of a time maintaining therapeutic blood thinning levels (prothrombin times).
But those are the rules, you see. Only patients with non-rheumatic atrial fibrillation can get dabigatran, I was told. Dabigatran was never approved for atrial flutter, only atrial fibrillation. Never mind the stroke risk in non-rheumatic atrial flutter, like atrial fibrillation, has been found to be significant.
For my patient, dabigatran would have been the perfect solution.
But increasingly I'm finding the patient is not mine, they're someone else's. Someone else who tells me their rules - someone who has little to no responsibility for the patient, outside of their accounts receivable. Oh sure, I suppose my patient could pay for the drug themself if the drug weren't so horribly expensive, but shouldn't the judgement of a person ultimately responsible for a patient's well-being be trusted to decide the best therapy for a patient? Evidently not. Doctors, as we continuously hear time and time again in the media and will our politically correct health care reformers, are the problem with costs in health care and costs, above all else, must be reigned in.
So we return, my patient and me, to warfarin and subtherapeutic and supratherapeutic INR's with their increased risks of stroke and bleeding because those in charge tell me they know better.
Short term savings with long term implications, because I'm no longer allowed to think in the world of Paint-by-Numbers medicine.
This is what happens when doctors are excluded from the health care playbook.
-Wes
Tuesday, September 27, 2011
Monday, September 26, 2011
EKG Du Jour #24: Reversals
In the spirit of connecting via social media, this EKG Du Jour hails from the great Aussie blog, Life in the Fast Lane.
(There's lots to learn on many levels.)
-Wes
(There's lots to learn on many levels.)
-Wes
I Wish I Had A Million Dollars
I wish I had a million dollars that I could use to convince my patients to stop smoking.
I wish I had a million dollars to get my patients to take their medicines.
I wish I had a million dollars to get people to shape up and lose weight.
I wish I had a million dollars to make sure people just listened to me so they would always wear their seatbelts and never use their cell phones while driving.
Heck, I just wish I had a million dollars myself.
But I don't.
That's because I'm a doctor: I don't offer people a million dollars to take my advice. I especially don't dangle the prospect of them earning that money if they follow my "non-medical" advice as I pose as one who gives medical "information" either. Nor do I pretend to think that I will change peoples' behavior with money.
But there are those who believe in the Keynesian economics of health care delivery where, if we just throw a bunch of money at these problems, they're all going to go away; that they're going to make a difference in millions of peoples' lives as they watch TV. Unfortunately, this theory of economics hasn't worked out so well for our economy and I really don't see why we should think this type of thinking should work so well for health care. Can we really change behavior of weight gain without changing the psychology and sociology of the home?
But there will always be ideologues in the world of marketing who believe in the power of Keynesian economics. After all, the money's not theirs; marketers get their dollars from advertisers. That way, like Oprah, they can offer a million dollars to promote, entice, market, and maybe even deceive - especially when they only give their million to a person the marketer chooses as their "winner" because they've followed their self-imposed health rules that follow a pre-ordained rubric.
Marketers have use this approach for years with things like The Price is Right, Jeopardy, and (my favorite) The Wheel of Fortune! We absolutely love this stuff. Like bugs to a light, we are drawn to the easy money that isn't.
But when it comes to health care, I just hope we really think about what we're getting for someone else's million.
-Wes
I wish I had a million dollars to get my patients to take their medicines.
I wish I had a million dollars to get people to shape up and lose weight.
I wish I had a million dollars to make sure people just listened to me so they would always wear their seatbelts and never use their cell phones while driving.
Heck, I just wish I had a million dollars myself.
But I don't.
That's because I'm a doctor: I don't offer people a million dollars to take my advice. I especially don't dangle the prospect of them earning that money if they follow my "non-medical" advice as I pose as one who gives medical "information" either. Nor do I pretend to think that I will change peoples' behavior with money.
But there are those who believe in the Keynesian economics of health care delivery where, if we just throw a bunch of money at these problems, they're all going to go away; that they're going to make a difference in millions of peoples' lives as they watch TV. Unfortunately, this theory of economics hasn't worked out so well for our economy and I really don't see why we should think this type of thinking should work so well for health care. Can we really change behavior of weight gain without changing the psychology and sociology of the home?
But there will always be ideologues in the world of marketing who believe in the power of Keynesian economics. After all, the money's not theirs; marketers get their dollars from advertisers. That way, like Oprah, they can offer a million dollars to promote, entice, market, and maybe even deceive - especially when they only give their million to a person the marketer chooses as their "winner" because they've followed their self-imposed health rules that follow a pre-ordained rubric.
Marketers have use this approach for years with things like The Price is Right, Jeopardy, and (my favorite) The Wheel of Fortune! We absolutely love this stuff. Like bugs to a light, we are drawn to the easy money that isn't.
But when it comes to health care, I just hope we really think about what we're getting for someone else's million.
-Wes
Saturday, September 24, 2011
National Consolidation of Heart Programs: A New Paradigm?
With the announcement of Cleveland Clinic offering cardiothoracic surgery services to Charlotte, North Carolina after their collaboration with Central Dupage Hospital in Illinois, a new cardiovascular surgery paradigm is taking shape:
-Wes
The Novant-Cleveland Clinic affiliation is not the first such collaboration for a Charlotte-area hospital. In 2010, CaroMont Health, which operates Gaston Memorial Hospital, announced a partnership with Columbia HeartSource, part of New York Presbyterian Hospital/Columbia University Medical Center. CaroMont doctors visit the N.Y. hospital, and N.Y. doctors have scrubbed in on surgeries at Gaston Memorial. Doctors confer about patient cases weekly, and CaroMont offers procedures that weren't available before.This is all about the race to tertiary care access which is increasingly being restricted. The hospital system that offers continued access to advanced therapies will hold a competetive (not to mention) financial advantage.
"This is really a new paradigm in medicine," said Dr. Paul Kurlansky, a cardiac surgeon with Columbia HeartSource. It's a way for top-tier academic medical programs to share what they know with community hospitals and begin to reduce disparities in medical care across the U.S., Kurlansky said. "You will start seeing this increasingly throughout the country."
-Wes
Friday, September 23, 2011
And now: Bach
The power of the cello (stolen shamelessly from my son's Facebook wall for your entertainment):
-Wes
-Wes
Thursday, September 22, 2011
EKG Du Jour #23 - With Increasing Prevalence: The Awful EKG
"Hey, Wes! I've been holding on to this EKG from a recent clinic visit with a patient of mine who presented with chest pain and thought it would make a cool EKG for your 'EKG Du Jour' series! I never could get a good tracing and I'm pretty sure my EKG machine works properly:"

For now, forget the chest pain. What's the patient's principle diagnosis?
(Trust me: you'll be seeing more of this.)
-Wes
h/t: Gary Novak, MD
Clue #1: Still uncertain? A major hint to the answer is here, so look only if you must.
Clue #2: By the way, this is not the same diagnosis as Happy's patient.
Clue #3: Here's an example of why I think we'll be seeing plenty of this.
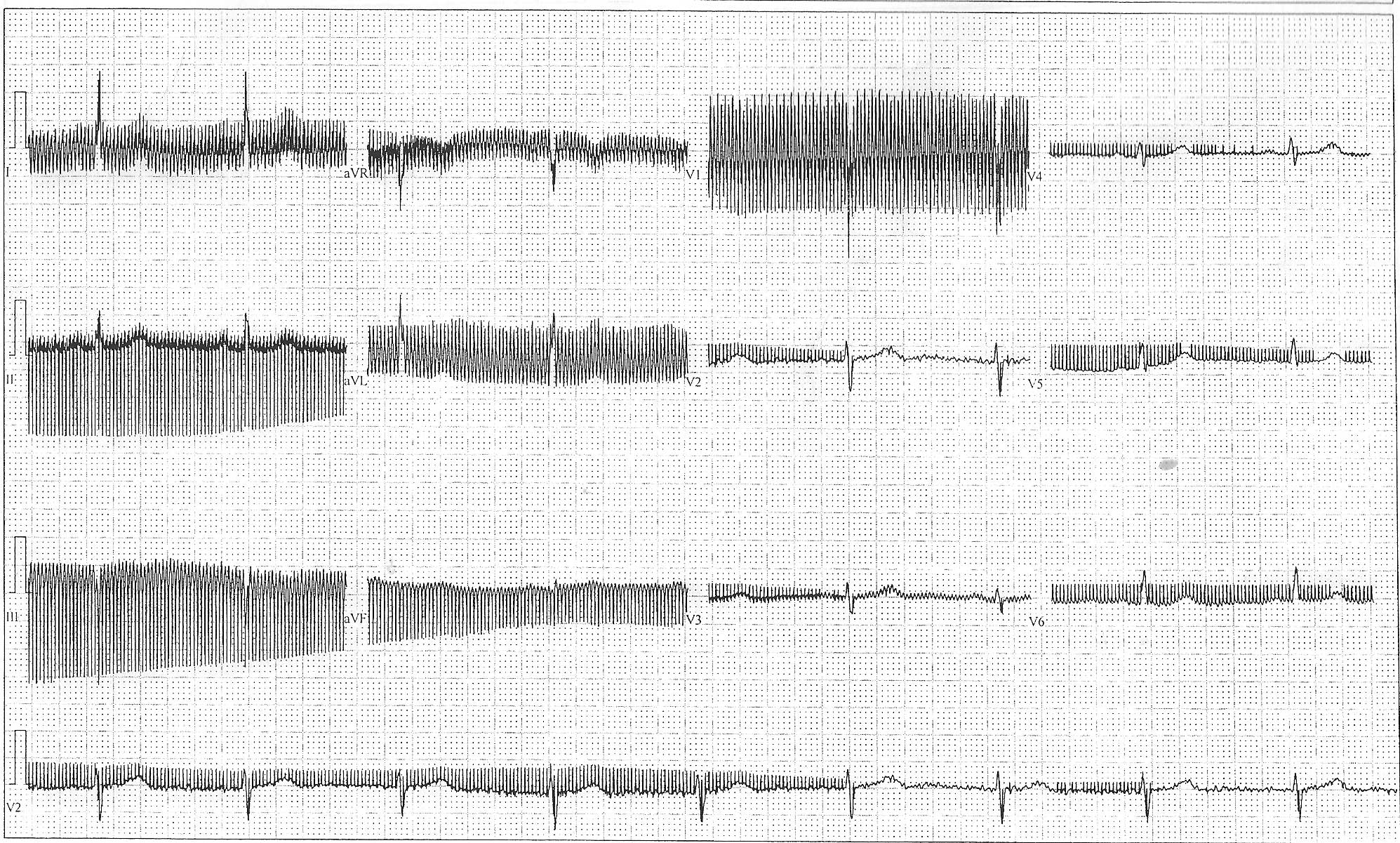
Click image to enlarge
For now, forget the chest pain. What's the patient's principle diagnosis?
(Trust me: you'll be seeing more of this.)
-Wes
h/t: Gary Novak, MD
Clue #1: Still uncertain? A major hint to the answer is here, so look only if you must.
{kind=link}
Clue #2: By the way, this is not the same diagnosis as Happy's patient.
Clue #3: Here's an example of why I think we'll be seeing plenty of this.
Wednesday, September 21, 2011
Taking the Plunge Into Social Media
With the increased internet connectivity of doctors, nurses, medical residents and medical students, I find more and more health care people interested in taking the plunge into the social media world. Many of these same people wisely see the advantages and the potential disadvantages to entering this space, so they are appropriately reluctant to dive "all in." Nowhere is there more caution than with the medical professions, especially physicians. While there is no one way to dabble in the world of social media, for those looking to embark cautiously on this course, I might be able to offer an approach that is not too dissimilar from a child learning to swim.
The Baby Pool
Where to start?
While many might attempt to enter social media through simple "micro-blogging" sites like Twitter, realize that this is (professionally) a bit like diving into the deep end of the social media pool before learning how to swim. That's because Twitter is a two-way interactive medium; you can receive AND send out tweets there. For medical professionals constrained under HIPAA, it might be better to take a cautious approach to utilize a one-way (receiving) medium first by using a "feed reader" like Google Reader or BlogLines. A feed reader is a program that reads news feeds that are automatically sent out to the internet as a standardized "Really Simple Syndication (RSS) feed" anytime there is something new published. Feed readers allow you to "subscribe" to a site's feed so that anything new published can be collected and categorized by the feed reader program on your computer. Almost all of today's newspapers, scientific and popular media journals, and blogs provide "feeds" whenever things are published to the internet. To help people locate the feed from a particular site, many post the standardized RSS feed symbol shown to the right. As a helpful tip, I have learned that most weekly medical journal and local newpaper health care section feeds are published to the internet either Monday evenings or early morning Tuesdays. Check your feed reader first thing each Tuesday morning and you'll have tons of articles to review from the select journals to which you've decided to "subscribe." The real beauty of a feed reader, though, is that you can then scan hundreds (I'm not kidding) of these article feeds in minutes to find the few that interest you. If they're not of interest (and most aren't) then they are marked as "read" and replaced with new articles when they come available. This system is fast, efficient, valuable for every doctor, nurse, or medical nerd out there. Once you master a feed reader, THEN I would consider moving to the more "social" aspect of social media and start to interact with others. This is when you'll move from the shallow end to the deep end of the social media pool.
To help people locate the feed from a particular site, many post the standardized RSS feed symbol shown to the right. As a helpful tip, I have learned that most weekly medical journal and local newpaper health care section feeds are published to the internet either Monday evenings or early morning Tuesdays. Check your feed reader first thing each Tuesday morning and you'll have tons of articles to review from the select journals to which you've decided to "subscribe." The real beauty of a feed reader, though, is that you can then scan hundreds (I'm not kidding) of these article feeds in minutes to find the few that interest you. If they're not of interest (and most aren't) then they are marked as "read" and replaced with new articles when they come available. This system is fast, efficient, valuable for every doctor, nurse, or medical nerd out there. Once you master a feed reader, THEN I would consider moving to the more "social" aspect of social media and start to interact with others. This is when you'll move from the shallow end to the deep end of the social media pool.
The Deep End
But why wait? What's so bad about jumping in to the "deep end" of social media (a blog/Twitter/Facebook, etc.)?
Simply put: the deep end is where you can drown as a health care professional.
Caution, especially as a doctor on the internet, should be the rule. Also, despite how smart you may think you are and how much you want to say about your brilliance on a particular topic, you can bet your bippy that there is someone smarter out there. If you're a smart as$, plan to be handed your butt. (Heck, humbling others is the most popular sport in the blog-o-sphere!) Save yourself plenty of angst: be humble and write respectfully. If you do, you'll be rewarded with respect. Along the same line: if you make a mistake, admit it. Say something you shouldn't have? Own up to it and correct the error. Upset someone? Decide if you should reconsider. Yes, public figures are easier to slam (and get away with it) than private ones since it comes with the territory. But the line between respectful disagreement and slander is a line you don't want to explore in court. So choose your targets carefully and really consider playing nice (or at least nice enough). Don't get me wrong, I think it's important for passionate professionals to stand up for what they believe, but realize that there is likely to be others just as passionate about the counter argument you propose. As a rule of thumb, you'll get more mileage if you make it a point to consider the counter-argument in your blog post or tweet. Remember that your words on the internet have permanence and unless there's a real defensible reason to go there, you might want to tone that rant down a bit.
Better yet, sleep on it before you publish it.
Joining the Diving Team
Every developing physician blogger I know hits a few snags along the way. Suffice it to say there is no single right or wrong way to approach social media as a doctor. Learn from those that have passed before you. Write them a private note. Comment on a few blogs to get the feel of the pace and tenor of the interchange. Once you're up and running you'll soon be joining the team of advanced aquatics: the diving team. These are the people that multi-task using their feeder daily, their blog to make a point, and firing off posts to Twitter and Facebook (or Google +) via a feedburner, then making a video blog or internet radio show. Seriously, it's whatever you have the time and passion for.
For me, I've chose to stick with a blog. I find it hard enough to keep updates to it on a regular basis while keeping my day job. And while I can't always get to comments for instant replies (who can as a doctor?), I find them entertaining and informative. For the sake of a modicum of brevity, I won't dwell on the specifics of how to write a blog. Many others have already covered this topic in depth. I would make a few important points, though. If you decide to make a blog (favorites seem to be Wordpress or Google's Blogger as starting points), decide early if you want to accept comments on your blog or not. Those who accept comments on their blog can learn a great deal from others, but when you decide to accept comments, you also accept additional responsibilities. For this reason, I always recommend moderating your comments. Moderating allows you to review comments before posting them to your blog. Bloggers have been held legally responsible for comments made by others that appear on their blog and it's the sad reality of the internet that there are sometimes wacko's out there that latch on to a blog and won't let go. Stay in control and moderate. Perhaps most important as a doctor-blogger, moderating comments permits better complicance with HIPAA standards in the event an inappropriate comment should appear. Also, make sure to use links liberally and reference your sources. This provides credibility to your argument(s). It's also nice to acknowledge the work of fellow bloggers by offering "hat tips (or 'h/t')" containing a link to their work if appropriate. Finally, be sure to add a disclaimer to your blog. This isn't the place to offer medical advice - ever.
In summary then, be careful, be respectful, be smart and soon you'll be using the wide array of social media springboards, like Problogger.net, to launch your online presence to new heights and opportunities.
Oh yeah, and one more thing...
... most of all, have fun.
-Wes
The Baby Pool
Where to start?
While many might attempt to enter social media through simple "micro-blogging" sites like Twitter, realize that this is (professionally) a bit like diving into the deep end of the social media pool before learning how to swim. That's because Twitter is a two-way interactive medium; you can receive AND send out tweets there. For medical professionals constrained under HIPAA, it might be better to take a cautious approach to utilize a one-way (receiving) medium first by using a "feed reader" like Google Reader or BlogLines. A feed reader is a program that reads news feeds that are automatically sent out to the internet as a standardized "Really Simple Syndication (RSS) feed" anytime there is something new published. Feed readers allow you to "subscribe" to a site's feed so that anything new published can be collected and categorized by the feed reader program on your computer. Almost all of today's newspapers, scientific and popular media journals, and blogs provide "feeds" whenever things are published to the internet.
The Deep End
But why wait? What's so bad about jumping in to the "deep end" of social media (a blog/Twitter/Facebook, etc.)?
Simply put: the deep end is where you can drown as a health care professional.
Caution, especially as a doctor on the internet, should be the rule. Also, despite how smart you may think you are and how much you want to say about your brilliance on a particular topic, you can bet your bippy that there is someone smarter out there. If you're a smart as$, plan to be handed your butt. (Heck, humbling others is the most popular sport in the blog-o-sphere!) Save yourself plenty of angst: be humble and write respectfully. If you do, you'll be rewarded with respect. Along the same line: if you make a mistake, admit it. Say something you shouldn't have? Own up to it and correct the error. Upset someone? Decide if you should reconsider. Yes, public figures are easier to slam (and get away with it) than private ones since it comes with the territory. But the line between respectful disagreement and slander is a line you don't want to explore in court. So choose your targets carefully and really consider playing nice (or at least nice enough). Don't get me wrong, I think it's important for passionate professionals to stand up for what they believe, but realize that there is likely to be others just as passionate about the counter argument you propose. As a rule of thumb, you'll get more mileage if you make it a point to consider the counter-argument in your blog post or tweet. Remember that your words on the internet have permanence and unless there's a real defensible reason to go there, you might want to tone that rant down a bit.
Better yet, sleep on it before you publish it.
Joining the Diving Team
Every developing physician blogger I know hits a few snags along the way. Suffice it to say there is no single right or wrong way to approach social media as a doctor. Learn from those that have passed before you. Write them a private note. Comment on a few blogs to get the feel of the pace and tenor of the interchange. Once you're up and running you'll soon be joining the team of advanced aquatics: the diving team. These are the people that multi-task using their feeder daily, their blog to make a point, and firing off posts to Twitter and Facebook (or Google +) via a feedburner, then making a video blog or internet radio show. Seriously, it's whatever you have the time and passion for.
For me, I've chose to stick with a blog. I find it hard enough to keep updates to it on a regular basis while keeping my day job. And while I can't always get to comments for instant replies (who can as a doctor?), I find them entertaining and informative. For the sake of a modicum of brevity, I won't dwell on the specifics of how to write a blog. Many others have already covered this topic in depth. I would make a few important points, though. If you decide to make a blog (favorites seem to be Wordpress or Google's Blogger as starting points), decide early if you want to accept comments on your blog or not. Those who accept comments on their blog can learn a great deal from others, but when you decide to accept comments, you also accept additional responsibilities. For this reason, I always recommend moderating your comments. Moderating allows you to review comments before posting them to your blog. Bloggers have been held legally responsible for comments made by others that appear on their blog and it's the sad reality of the internet that there are sometimes wacko's out there that latch on to a blog and won't let go. Stay in control and moderate. Perhaps most important as a doctor-blogger, moderating comments permits better complicance with HIPAA standards in the event an inappropriate comment should appear. Also, make sure to use links liberally and reference your sources. This provides credibility to your argument(s). It's also nice to acknowledge the work of fellow bloggers by offering "hat tips (or 'h/t')" containing a link to their work if appropriate. Finally, be sure to add a disclaimer to your blog. This isn't the place to offer medical advice - ever.
In summary then, be careful, be respectful, be smart and soon you'll be using the wide array of social media springboards, like Problogger.net, to launch your online presence to new heights and opportunities.
Oh yeah, and one more thing...
... most of all, have fun.
-Wes
Tuesday, September 20, 2011
Thoracic Impedance Monitoring Fails to Limit Heart Failure Admissions
Imagine being able to detect heart failure before it happens. The potential to offer significant cost reductions in health care might be significant.
So device makers created a way that implantable defibrillators could measure a drop in impedance between the pulse generator can and the lead in the patient's heart. Lower impedance should mean more water in the chest, suggesting fluid overload.
It seemed, well, so logical.
But with today's release of the DOT-HF trial, it seems that all that thoracic impedance information contained in an ICD, when used to alert the patient to a fluid accumulation in their chest, has the potential to create more rather than fewer hospitalizations:
Moral of the story: more data from ICDs is not necessarily better when it comes to predicting heart failure exacerbations.
-Wes
References:
van Veldhuisen DJ, et al. "Intrathoracic Impedance Monitoring, Audible Patient Alerts, and Outcome in Patients With Heart Failure." Circulation 2011 http://circ.ahajournals.org/content/suppl/2011/09/18/CIRCULATIONAHA.111.043042.DC1.html
Udelson JE. "T.M.I. (Too Much Information)?" Circulation http://circ.ahajournals.org/content/early/2011/09/19/CIRCULATIONAHA.111.067819.citation
So device makers created a way that implantable defibrillators could measure a drop in impedance between the pulse generator can and the lead in the patient's heart. Lower impedance should mean more water in the chest, suggesting fluid overload.
It seemed, well, so logical.
But with today's release of the DOT-HF trial, it seems that all that thoracic impedance information contained in an ICD, when used to alert the patient to a fluid accumulation in their chest, has the potential to create more rather than fewer hospitalizations:
METHODS AND RESULTS: We studied 335 patients with chronic heart failure who had undergone implantation of an implantable cardioverter-defibrillator alone (18%) or with cardiac resynchronization therapy (82%). All devices featured a monitoring tool to track changes in intrathoracic impedance (OptiVol) and other diagnostic parameters. Patients were randomized to have information available to physicians and patients as an audible alert in case of preset threshold crossings (access arm) or not (control arm). The primary end point was a composite of all-cause mortality and heart failure hospitalizations. During 14.9+/-5.4 months, this occurred in 48 patients (29%) in the access arm and in 33 patients (20%) in the control arm (P=0.063; hazard ratio, 1.52; 95% confidence interval, 0.97–2.37). This was due mainly to more heart failure hospitalizations (hazard ratio, 1.79; 95% confidence interval, 1.08–2.95; P < 0.022), whereas the number of deaths was comparable (19 versus 15; P = 0.54). The number of outpatient visits was higher in the access arm (250 versus 84; P < 0.0001), with relatively more signs of heart failure among control patients during outpatient visits. Although the trial was terminated as a result of slow enrollment, a post hoc futility analysis indicated that a positive result would have been unlikely. CONCLUSION: Use of an implantable diagnostic tool to measure intrathoracic impedance with an audible patient alert did not improve outcome and increased heart failure hospitalizations and outpatient visits in heart failure patients.Postulating why this unexpected result was seen, Dr. James E. Udelson in an accompanying editorial suggested several reasons:
In the DOT-HF trial, among the episodes of HF hospitalization, only 60% were preceded by an alert condition, where impedance readings fell below the prespecified threshold indicting risk. In other words, the sensitivity of the impedance alert to predict a HF episode was only modest. This is actually consistent with previous studies, and false-positives seem common, as well.Almost half of the outpatient visits in the treatment group were a result solely of an alert, which may have resulted in a drive to more intervention and possibly hospitalization.
Moral of the story: more data from ICDs is not necessarily better when it comes to predicting heart failure exacerbations.
-Wes
References:
van Veldhuisen DJ, et al. "Intrathoracic Impedance Monitoring, Audible Patient Alerts, and Outcome in Patients With Heart Failure." Circulation 2011 http://circ.ahajournals.org/content/suppl/2011/09/18/CIRCULATIONAHA.111.043042.DC1.html
Udelson JE. "T.M.I. (Too Much Information)?" Circulation http://circ.ahajournals.org/content/early/2011/09/19/CIRCULATIONAHA.111.067819.citation
Ninety-six Buttons of Choice on the Wall
"Ninety-six buttons of choice on the wall,
Ninety-six buttons of choice...
Take one down, pass it around,
Ninety-five buttons of choice on the wall..."
Seriously, are all these action buttons on today's EMR's necessary on the main patient care screen? Increasingly, more and more action buttons are appearing - so much so that we even have to scroll down "below the fold."
EMR developers should take a page from Google: keep the main screen for the management of patient care full of plenty of white space.
Yours in IT consultancy -
-Wes
Grand Rounds is Up
Grand Rounds, the weekly collection of the some of the best in online medical writing from all (doctors, nurses, patients, healthcare professionals) is hosted this week by none other than the one and only Ramona Bates, MD at the Suture for a Living blog.
-Wes
-Wes
Monday, September 19, 2011
When the Electronic Medical Record Died
It's never supposed to happen of course. But it happened today: the computer froze and could not be resurrected - a brief interlude to the daily clinic routine.
The reactions are predictable:
"Damn it. What the hell's wrong?... Let's try to re-boot.... (a long pause) ... A switch turned off, then on... Come on, baby!!!!!... Shoot, still nothing!"
Clicks upon clicks, then an embarrassed look on your face. "Sorry, Ms. Jones. Usually this system works great..." !@#$^%&$)#! "Seriously, um, .... just a moment." The doctors walked out of the exam room.
"Hey, you guys having the same problem I'm having?"
"Yeah, our terminal's not responding either. I think we've got a Code Green."
(Editor's note: I know what you're thinking... don't go there...)
"How about a piece of paper? Oh, and a pen? Anybody got a pen? Damn, where are the pharmaceutical reps when you need them?" The office manager sprung to action: "I'll get out the Code Green box!" You figure there's a plan, but seriously, this is it? Some archaic progress notes appear, the medical assistant found a pen, then some interesting order forms that you've never seen before appear. "Dang, I have to fill those out?" You think, "How will the lab and xray get these?" "Do we call the orders in? Maybe someone walks them down. Hey, maybe the patient can help out!" After all, the only way out is through this mess. But it didn't stop there:
"What about that prescription - anybody got a prescription pad?"
"No, got rid of those a long time ago. We're electronic now, remember? Can't use them any more."
"No? Shoot, what do we do?"
"Try calling it in," someone shouts from down the hall.
"Why didn't I think of that? Good thing I have my handy, dandy cell phone!" Google is consulted, the number for the patient's preferred pharmacy appears, the call is made and order placed on the recorder. The patient is impressed: "Thanks, doc! That was nice of you to call it in for me." We shook hands. Mission accomplished.
Sorry, no 'After Visit Summary" was given to the patient, no medication list was printed. No copy of the note was sent back to the referring, no orders to verify, no orders pending, no quality assurance pay-for-performance measures were completed, no billing codes entered and as a result, no bill instantly submitted. Surely our quality measures took a hit.
Instead there was just a handshake, a look in the eye, and an "Appreciate your patience" message tacitly transmitted. In return: "No problem, doctor, I appreciate your help with this."
Suddenly it dawned on me: "Damn, it's like the good old days!"
Oh sure, it took a little longer and I'm sure my notes were illegible to anyone but the most seasoned of veteran nurses. Whether I get paid for these visits remains to be seen, too. But this once, for a tiny moment of time, I experienced a blast from the past that proved, beyond a shadow of a doubt, that the computers are about the computers, rules, protocols and billing while health care was still about the doctor and the patient.
Like turning off the TV and computer at home, it was a brief but beautiful respite from the daily monotony of a thousand keyboard clicks. Sure, the transition from electronic medical record to a paper-based one was abrupt and challenging. But I found patients responded to our efforts with much more appreciation, not just an aire of expectation. And despite the challenges of the day, it was good to know that I can still be a doctor that thinks out of the box and not just a clerical secretary.
-Wes
The reactions are predictable:
"Damn it. What the hell's wrong?... Let's try to re-boot.... (a long pause) ... A switch turned off, then on... Come on, baby!!!!!... Shoot, still nothing!"
Clicks upon clicks, then an embarrassed look on your face. "Sorry, Ms. Jones. Usually this system works great..." !@#$^%&$)#! "Seriously, um, .... just a moment." The doctors walked out of the exam room.
"Hey, you guys having the same problem I'm having?"
"Yeah, our terminal's not responding either. I think we've got a Code Green."
(Editor's note: I know what you're thinking... don't go there...)
"How about a piece of paper? Oh, and a pen? Anybody got a pen? Damn, where are the pharmaceutical reps when you need them?" The office manager sprung to action: "I'll get out the Code Green box!" You figure there's a plan, but seriously, this is it? Some archaic progress notes appear, the medical assistant found a pen, then some interesting order forms that you've never seen before appear. "Dang, I have to fill those out?" You think, "How will the lab and xray get these?" "Do we call the orders in? Maybe someone walks them down. Hey, maybe the patient can help out!" After all, the only way out is through this mess. But it didn't stop there:
"What about that prescription - anybody got a prescription pad?"
"No, got rid of those a long time ago. We're electronic now, remember? Can't use them any more."
"No? Shoot, what do we do?"
"Try calling it in," someone shouts from down the hall.
"Why didn't I think of that? Good thing I have my handy, dandy cell phone!" Google is consulted, the number for the patient's preferred pharmacy appears, the call is made and order placed on the recorder. The patient is impressed: "Thanks, doc! That was nice of you to call it in for me." We shook hands. Mission accomplished.
Sorry, no 'After Visit Summary" was given to the patient, no medication list was printed. No copy of the note was sent back to the referring, no orders to verify, no orders pending, no quality assurance pay-for-performance measures were completed, no billing codes entered and as a result, no bill instantly submitted. Surely our quality measures took a hit.
Instead there was just a handshake, a look in the eye, and an "Appreciate your patience" message tacitly transmitted. In return: "No problem, doctor, I appreciate your help with this."
Suddenly it dawned on me: "Damn, it's like the good old days!"
Oh sure, it took a little longer and I'm sure my notes were illegible to anyone but the most seasoned of veteran nurses. Whether I get paid for these visits remains to be seen, too. But this once, for a tiny moment of time, I experienced a blast from the past that proved, beyond a shadow of a doubt, that the computers are about the computers, rules, protocols and billing while health care was still about the doctor and the patient.
Like turning off the TV and computer at home, it was a brief but beautiful respite from the daily monotony of a thousand keyboard clicks. Sure, the transition from electronic medical record to a paper-based one was abrupt and challenging. But I found patients responded to our efforts with much more appreciation, not just an aire of expectation. And despite the challenges of the day, it was good to know that I can still be a doctor that thinks out of the box and not just a clerical secretary.
-Wes
The Hive
He came for a second opinion, of course he did. You could see it in the eyes: the disbelief, the uncertainty, the despair. "Sleep deprived," he'd call it, then apologize for his abruptness. He was much too young to look death in the face, so he pretended not to notice the pathology.
As doctors, we are given a gift and a curse at the same time: the opportunity to peer into the circumstances of life in ways unimaginable. We see images that are so profound they haunt as we lie awake perplexed, imagining the unthinkable that lies ahead based on our understanding of anatomy, physiology, and yes, pathology. We wrestle quietly in the wee hours of the morning, looking toward the ceiling hoping to find an answer, yet often, despite our knowing better, none come. It is hard to return to sleep.
We roll over to see a peaceful head next to us, grateful for what we've got, knowing full well our patient yearns for the opportunity to experience such a moment just once more. No words are spoken, no thoughts exchanged as we we wrestle with images so profound that they humble our soul, then flip it upside down and turn it inside out as if to reinforce our human frailty and limitations.
From the moment we start medical school with the unsettling slice of a blade though the juicy grey skin of a cadaver, we struggle to rationalize the meaning of such an act. Of course we cut that skin to learn how to help others! I'm going to be a doctor!
If only it were so simple.
With time and a million experiences, we later realize our skills of compartmentalization have a function - like the well deck of a mothership that lowers to accept smaller ships - to gather our psyche while simultaneously sheilding our loved ones and patients from the gruesome realities we've witnessed. These images are ours forever, quietly tucked away and compartmentalized into a carefully-constructed hive of rationalization. Stored, but never forgotten.
Until one day, another image enters.
And suddenly, like rapping a stick upon the hive at two in the morning, the images swarm once again.
-Wes
As doctors, we are given a gift and a curse at the same time: the opportunity to peer into the circumstances of life in ways unimaginable. We see images that are so profound they haunt as we lie awake perplexed, imagining the unthinkable that lies ahead based on our understanding of anatomy, physiology, and yes, pathology. We wrestle quietly in the wee hours of the morning, looking toward the ceiling hoping to find an answer, yet often, despite our knowing better, none come. It is hard to return to sleep.
We roll over to see a peaceful head next to us, grateful for what we've got, knowing full well our patient yearns for the opportunity to experience such a moment just once more. No words are spoken, no thoughts exchanged as we we wrestle with images so profound that they humble our soul, then flip it upside down and turn it inside out as if to reinforce our human frailty and limitations.
From the moment we start medical school with the unsettling slice of a blade though the juicy grey skin of a cadaver, we struggle to rationalize the meaning of such an act. Of course we cut that skin to learn how to help others! I'm going to be a doctor!
If only it were so simple.
With time and a million experiences, we later realize our skills of compartmentalization have a function - like the well deck of a mothership that lowers to accept smaller ships - to gather our psyche while simultaneously sheilding our loved ones and patients from the gruesome realities we've witnessed. These images are ours forever, quietly tucked away and compartmentalized into a carefully-constructed hive of rationalization. Stored, but never forgotten.
Until one day, another image enters.
And suddenly, like rapping a stick upon the hive at two in the morning, the images swarm once again.
-Wes
Saturday, September 17, 2011
The FDA Drug Safety Communication I'd Like to See
FDA (Food and Drug Administration): Drug Safety Communication - Excessive FDA Drug Safety Communications
[Posted 09/17/2011]
AUDIENCE: Physicians, Patients
ISSUE: FDA has notified healthcare professionals and patients of ongoing safety review and labeling changes for drugs such as Zofran (ondansetron, ondansetron hydrochloride and generics). It has been determined by the FDA that the FDA may be on the brink of creating a "Boy Who Cried Wolf" scenario by notifying doctors of prolonged QT intervals in drugs twenty years after their first market approval. Further, notifications such as these included two studies from 2005 and 2008 which were both written by the same lead author. The FDA realizes it is now 2011. An FDA investigation to determine if this same author now works for the FDA is ongoing.
BACKGROUND: Zofran (ondansetron) is in a class of medications called 5-HT3 receptor antagonists and is one of the few effective and remarklably safe drugs that doctors have used for years. While QT-prolonging effects with this medication have been seen in small controlled trials (see the FDA's references), realize that limitations to at least one of those trials existed, since 21% of an 85-patient study had prolonged QT before the drug was administered. Also note that the second trial only included a whopping 8 patients in the study group.
RECOMMENDATION: The FDA recommends that FDA Drug Safety Communications be inspected closely. Errant recommendations based on dated, single-center studies are becoming the norm and doctors are advised that excessive FDA Safety Communications may be forthcoming because certain government exployees are working hard to perform exhaustive literature searches with litle relevance to clinical experience.
That is all.
As always, healthcare professionals and patients are encouraged to report adverse events or side effects related to the use of these products to the FDA's MedWatch Safety Information and Adverse Event Reporting Program:
Complete and submit the report Online: www.fda.gov/MedWatch/report.htm
Download form or call 1-800-332-1088 to request a reporting form, then complete and return to the address on the pre-addressed form, or submit by fax to 1-800-FDA-0178
[09/17/2011 - Drug Safety Communication - FDA]
-Wes
See also WhiteCoat's take.
Friday, September 16, 2011
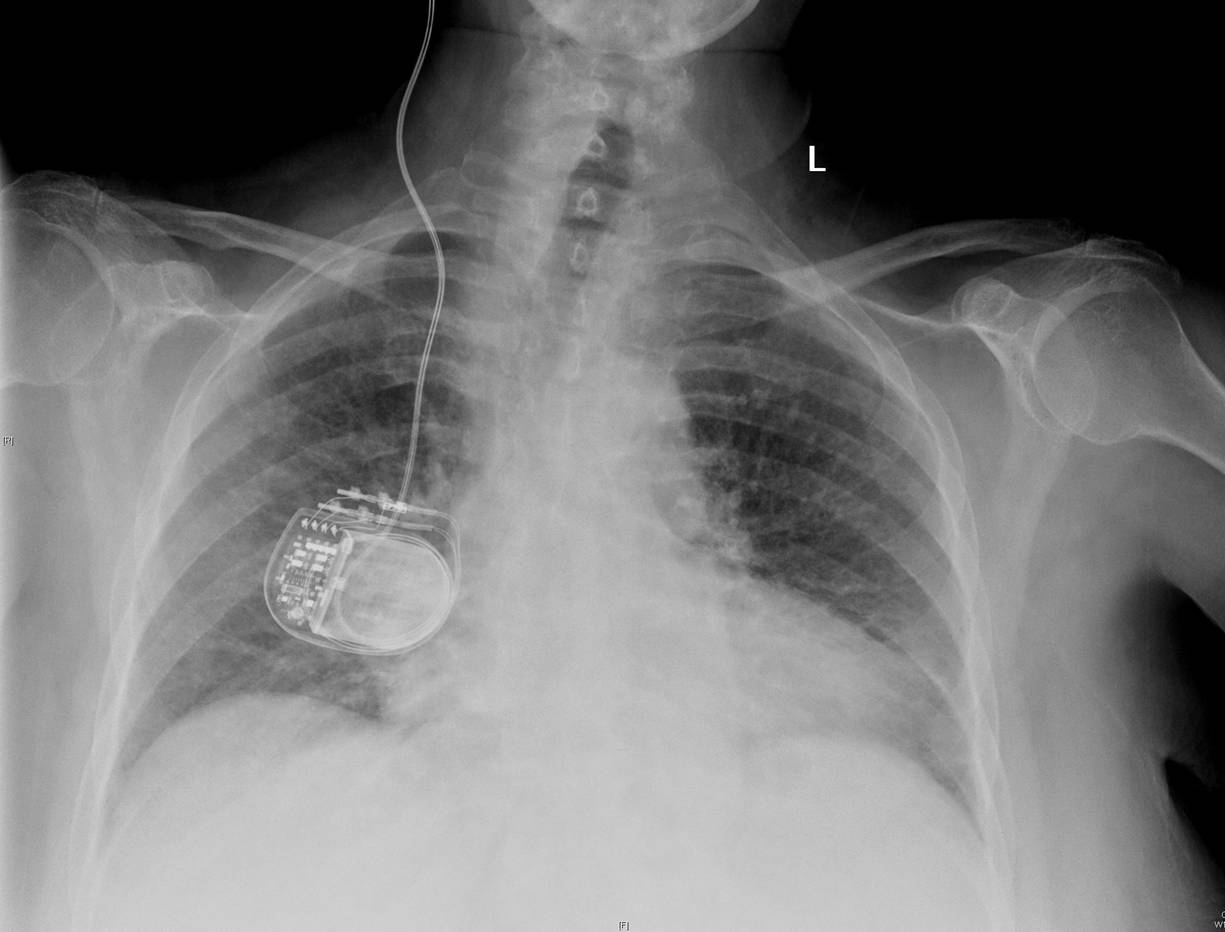
Sometimes, It's the Little Things
A little fun for Friday afternoon:
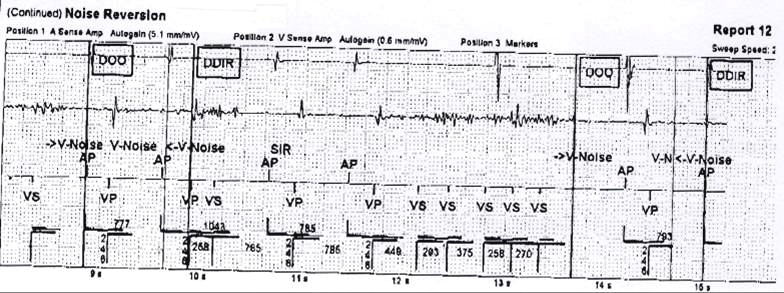
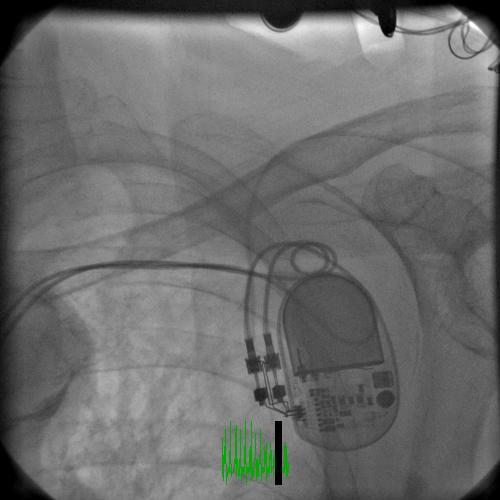
A new patient presents for a pacemaker check and is found to have a number of "noise reversion" notifications nine months after his St. Jude dual chamber pacemaker was implanted at an outside institution. The electrograms from one of those noise reversions are seen here:

The patient was not pacemaker-dependent. Arm motion and manipulation of the pocket failed to reproduce the noise and his lead appeared to be working properly at the time of evaluation with normal (stable) impedances and capture thresholds.
The ventricular lead was reprogrammed to a unipolar mode and observed. He returned two weeks later for a reassessment and the same findings were found. He was ultimately taken to the EP lab for lead revision.
A venogram was performed just before the procedure that disclosed the following:

A therapeutic procedure was performed.
What was done?
-Wes
Spoiler Alert: Can't wait? Here's the post-procedure film.
A new patient presents for a pacemaker check and is found to have a number of "noise reversion" notifications nine months after his St. Jude dual chamber pacemaker was implanted at an outside institution. The electrograms from one of those noise reversions are seen here:
Click image to enlarge
The patient was not pacemaker-dependent. Arm motion and manipulation of the pocket failed to reproduce the noise and his lead appeared to be working properly at the time of evaluation with normal (stable) impedances and capture thresholds.
The ventricular lead was reprogrammed to a unipolar mode and observed. He returned two weeks later for a reassessment and the same findings were found. He was ultimately taken to the EP lab for lead revision.
A venogram was performed just before the procedure that disclosed the following:
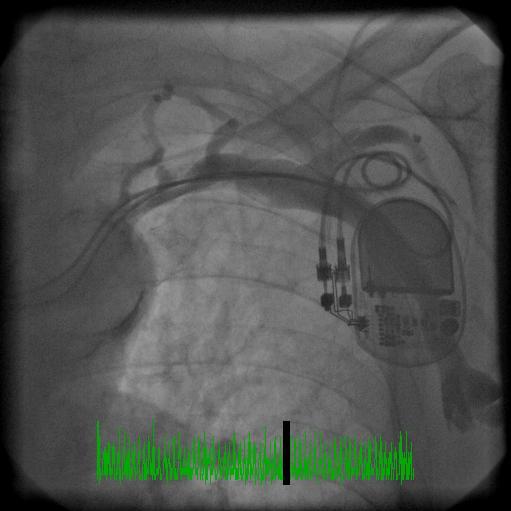
A therapeutic procedure was performed.
What was done?
-Wes
Spoiler Alert: Can't wait? Here's the post-procedure film.
{kind=link}
G.O.M.E.R.
Get. Out. Of. My. Emergency. Room.
Courtesy of your state Health Care Authority. Oh, but at the same time, make sure you're educated about the symptoms of heart disease and stroke.
-Wes
Courtesy of your state Health Care Authority. Oh, but at the same time, make sure you're educated about the symptoms of heart disease and stroke.
-Wes
Thursday, September 15, 2011
We've Hit the Jackpot With A Million Hearts
I don't know what I was thinking with my last post about the Health and Human Services' Million Hearts initiative. I thought the whole point of this program was to save money. At the time, I was less than optimistic that the government could acurately reach their goal given the problems with many of the principles behind their program. For instance, maybe it was just me, but how typing on an electronic medical record system would save those lives was lost on me.
But at the time, I had no idea this whole campaign was based on fear.
Watch this introductory video I found on the brand new Million Hearts website, all paid for (of course) with your tax payer dollars:
Listen to all that horrible stuff that can happen to you! And they look like such nice, ordinary people. Man, if that doesn't scare you into seeing your doctor, I don't know what will!
I have now seen the light: this is going to be awesome! (* Cha-ching! *)
You know: terrified, low risk people clamoring for an appointment insisting on all kinds of blood draws, testing, EKGs, and sophisticated imaging tests! And for all those tests with false positives, maybe an angio, too! We're about to make a fortune on this program all in the name of "cost savings!" Baby, there's NOTHING like screening low risk people when it comes to making money: Yeeeeeee haaaaaa!
Boys and girls, step right up! Help our heath care system save money, will you? (* Yuck yuck yuck *) After all (wink wink) it's about saving a million lives! You did see that video above, didn't you? No? Make sure you do: this is really BAD stuff!
Boy, no WONDER the American Medical Association, the American Heart Association, the American College of Cardiology, Walgreens, United Healthcare and a whole host of other "private interests" want to support this program: it's not just about the hearts, it's about the Benjamins!
Even better: they're on Facebook and Twitter! (Hope their video goes viral! Pssst: here's the link: http://www.youtube.com/embed/poc1eTuJJfc)
Absolutely, positively, brilliant. (I hope our health care system's marketing team is watching.)
After all, nothing sells like fear.
-Wes
But at the time, I had no idea this whole campaign was based on fear.
Watch this introductory video I found on the brand new Million Hearts website, all paid for (of course) with your tax payer dollars:
Listen to all that horrible stuff that can happen to you! And they look like such nice, ordinary people. Man, if that doesn't scare you into seeing your doctor, I don't know what will!
I have now seen the light: this is going to be awesome! (* Cha-ching! *)
You know: terrified, low risk people clamoring for an appointment insisting on all kinds of blood draws, testing, EKGs, and sophisticated imaging tests! And for all those tests with false positives, maybe an angio, too! We're about to make a fortune on this program all in the name of "cost savings!" Baby, there's NOTHING like screening low risk people when it comes to making money: Yeeeeeee haaaaaa!
Boys and girls, step right up! Help our heath care system save money, will you? (* Yuck yuck yuck *) After all (wink wink) it's about saving a million lives! You did see that video above, didn't you? No? Make sure you do: this is really BAD stuff!
Boy, no WONDER the American Medical Association, the American Heart Association, the American College of Cardiology, Walgreens, United Healthcare and a whole host of other "private interests" want to support this program: it's not just about the hearts, it's about the Benjamins!
Even better: they're on Facebook and Twitter! (Hope their video goes viral! Pssst: here's the link: http://www.youtube.com/embed/poc1eTuJJfc)
Absolutely, positively, brilliant. (I hope our health care system's marketing team is watching.)
After all, nothing sells like fear.
-Wes
Wednesday, September 14, 2011
A Million Hearts or A Million Dreams?
Yesterday, Thomas R. Frieden, M.D., M.P.H., and Donald M. Berwick, M.D., M.P.P. used the bulliest of scientific pulpits, the New England Journal of Medicine, to announce their "Million Hearts" initiative aimed at "preventing" heart attacks and strokes.
Now I do not hold a Masters in public health or public policy, but I do know a thing or two about evidenced-based medicine and cardiology. So it seems only appropriate that a cardiologist should comment on the proclamations made by an infectious disease specialist and pediatrician who promise to "save a million hearts," especially when we consider the billions of taxpayer dollars that have been or will be allocated to their programs.
I suspect neither of these highly accomplished men from public policy circles knows if, or exactly how, they will save a million lives nor how they should appropriately measure the effect of their initiative. That is not the point. Sexy program names are the point and making sure those names appear in a scientific journal within reach of treating cardiologists is especially the point.
We should acknowledge that the authors have been very good at dangling statistics of death and destruction caused by heart attacks and stroke to drive their policies. After all, while cardiovascular disease has remained the number one killer of Americans year after year, it is also the biggest driver of health care costs in America. I have no doubt these two non-cardiovascular specialists are proposing their initiative as a straw dog in an effort to gain the public's favor while simultaneously working around the clock to reduce cardiovascular spending. This is, after all, about a money shift, not just about more good ideas for improving cardiovascular outcomes.
How do I know?
I know because you will not hear from these men about the changes underway to limit access to cardiologists by forcing their consolidation with larger health care systems. I know because doctors are scrambling to these systems in an effort per preserve their income in a system intent on cost cutting. I know because government regulators are also working to restrict access to technologies have proven efficacy at saving lives and prolonging life for our older seniors, like wearable defibrillators whose use is being "reconsidered" and percutaneous aortic valves that still wait to gain approval (likely with significant restrictions to their use) here in the US. I also know because even with all the waste, fraud, and abuse measures underway to the cost of health care delivery in America, there will still be a need to cut America's health care system payments by at least 10-20% over the next ten years to maintain the program's fiscal solvency.
So given these overriding needs to cut costs, Americans should expect there are rock-hard data upon which the authors have based their need to start such a "million heart" initiative. Sadly, there are not. In fact, when we dig deeper we find the health care dollars spent on many of the cornerstone programs that serve as the foundations to their theories have lacked sufficient data to even justify their continuation. Yet, they ignore these data.
Let's look closer at the six cornerstone "principles" upon which their "million hearts" initiatives rest:
But we should realize what these feel-good perspective pieces are really about: they're about the money. More specifically, this perspective piece serves as a distraction to the money cuts and a money shifts from real-life proven therapies to mostly unproven, costly initiatives based on dreamy projections of public good rather than actual patient outcomes. As a result, we are now seeing the modus operandi of our government health care leaders of the future: placing feel-good happy-face programs in place based upon mostly unproven, theoretical data in favor of funding more expensive, better-proven therapies that really do save lives.
-Wes
Addendum: John Mandrola, MD offers his more heart-healthy take.
Now I do not hold a Masters in public health or public policy, but I do know a thing or two about evidenced-based medicine and cardiology. So it seems only appropriate that a cardiologist should comment on the proclamations made by an infectious disease specialist and pediatrician who promise to "save a million hearts," especially when we consider the billions of taxpayer dollars that have been or will be allocated to their programs.
I suspect neither of these highly accomplished men from public policy circles knows if, or exactly how, they will save a million lives nor how they should appropriately measure the effect of their initiative. That is not the point. Sexy program names are the point and making sure those names appear in a scientific journal within reach of treating cardiologists is especially the point.
We should acknowledge that the authors have been very good at dangling statistics of death and destruction caused by heart attacks and stroke to drive their policies. After all, while cardiovascular disease has remained the number one killer of Americans year after year, it is also the biggest driver of health care costs in America. I have no doubt these two non-cardiovascular specialists are proposing their initiative as a straw dog in an effort to gain the public's favor while simultaneously working around the clock to reduce cardiovascular spending. This is, after all, about a money shift, not just about more good ideas for improving cardiovascular outcomes.
How do I know?
I know because you will not hear from these men about the changes underway to limit access to cardiologists by forcing their consolidation with larger health care systems. I know because doctors are scrambling to these systems in an effort per preserve their income in a system intent on cost cutting. I know because government regulators are also working to restrict access to technologies have proven efficacy at saving lives and prolonging life for our older seniors, like wearable defibrillators whose use is being "reconsidered" and percutaneous aortic valves that still wait to gain approval (likely with significant restrictions to their use) here in the US. I also know because even with all the waste, fraud, and abuse measures underway to the cost of health care delivery in America, there will still be a need to cut America's health care system payments by at least 10-20% over the next ten years to maintain the program's fiscal solvency.
So given these overriding needs to cut costs, Americans should expect there are rock-hard data upon which the authors have based their need to start such a "million heart" initiative. Sadly, there are not. In fact, when we dig deeper we find the health care dollars spent on many of the cornerstone programs that serve as the foundations to their theories have lacked sufficient data to even justify their continuation. Yet, they ignore these data.
Let's look closer at the six cornerstone "principles" upon which their "million hearts" initiatives rest:
- Principle 1: Focus - The authors claim that "communication, clinical measurements, reporting by physicians and health care facilities, and health care systems will emphasize improving ABCS (Aspirin therapy administration, Blood pressure management, Cholesterol lowering, and Smoking cessation)." Few data support this claim. In fact, clinical measurement programs, like pay-for-performance measures, have failed to affect outcomes in smaller pilot programs here in the US and in a larger population studies overseas. Despite this, additional money for these programs continues to be promoted by these authors. We should really ask why.
- Principle 2: Health Information Technology (HIT) - The authors claim that "HIT enables providers and facilities to provide cardiovascular care and target intervention to patients in need of intensified care through registries and EHR (electronic health records) functions used at the point of care." While this sounds great, the data so far do not support this assumption when outcomes are actually measured:
In fact, EMRs (electronic medical records) were associated with significantly improved performance in only one measure — giving diet advice to high-risk adults. They didn’t improve performance in things including giving aspirin for coronary artery disease, depression treatment or blood-pressure measurement.
- Principle #3 - Clinical innovations - The authors claim: Innovations such as team-based care, patient-centered medical homes and interventions to promote adherence will be supported, evaluated, and disseminated rapidly to increase the effective use of ABCS practices." In other words, they haven't figured out if any of these "innovations" actually work. Truth be known, patient-centered medical home pilot projects have been a bit of a disappointment so far. Still, our authors press on absolutely convinced, (convinced I tell you!) that these measures will work despite data to the contrary.
- Principle #4: Policies and programs to reduce smoking and effects of second-hand smoke - This program is likely to be cost-effective. But we should temper our enthusiasm for these efforts now that the anti-smoking message is firmly established in our schools and public consciousness.
- Principle #5: Policies for reducing sodium content of food - While it is one thing to project the number of lives saved from modest sodium restriction in the diet, its an entirely different thing to suggest public policy will change people's individual lifestyle decisions. Good luck getting Americans to restrict sodium to 3 grams per day, especially when people can buy a salt shaker. If Drs. Frieden and Berwick could also impact the farm subsidies for corn that have been criticised as a significant contributor to our current obesity epidemic, they might gain favor with cardiologists, but politics are not likely to permit such a move.
- Principle #6: Policies at eliminating artificial trans fats in the diet - The authors expect to "further reduce the level of trans fats that increase LDL cholesterol levels, lower HDL cholesterol levels that increases the risk of heart attacks." This principle requires the authors to accept the cholesterol theory of reducing heart attacks, but recent studies are debunking that theory. Take the recent high-profile NIH-sponsored AIM-HIGH trial comparing statin to statin plus niacin therapy in patients with cardiovascular disease and low HDL levels. (This study was designed to show that increasing HDL levels with niacin would improve heart attack and stroke outcomes.) This study was stopped 18 months ahead of schedule not only because it was determined to be extremely unlikely that the increase in HDL produced by niacin would improve outcomes, but also because of an unexpected increase in strokes among the patients receiving niacin, a drug known to increase HDL. Support for the results of this study come from earlier trials on non-statin cholesterol lowering medications that lowered cholesterol but never reduced the outcomes of heart attack and stroke. Only statins as a class of drugs have shown such a benefit. So what gives? Doctors are not sure, but it's more about the statins than it is about the cholesterols. Still, such analyses are unimportant to our policy-makers intent on moving their agenda forward. You see it is far better to espouse non-factual takes in the New England Journal of Medicine unencumbered by critical discussion. Worse, given what we now know about elevating HDL levels from the AIM-HIGH trial, their programs could even have a deleterious effect to public health.
But we should realize what these feel-good perspective pieces are really about: they're about the money. More specifically, this perspective piece serves as a distraction to the money cuts and a money shifts from real-life proven therapies to mostly unproven, costly initiatives based on dreamy projections of public good rather than actual patient outcomes. As a result, we are now seeing the modus operandi of our government health care leaders of the future: placing feel-good happy-face programs in place based upon mostly unproven, theoretical data in favor of funding more expensive, better-proven therapies that really do save lives.
-Wes
Addendum: John Mandrola, MD offers his more heart-healthy take.
Tuesday, September 13, 2011
For Your Safety: How to Prescribe an Antiarrhythmic Drug
First, read an 8-page treatment guideline.
Next, read the 26-page prescribing information.
Next, read the patient's 3-page medication guide.
Next, fill out a database form for the drug company to add yourself to their new-and-improved database (even though you've already registered with them once before) once again before January 1, 2012.
Next, (and this is important), agree to the following:
I have no idea where the every "three month" suggested lab testing and EKG requirement came from and have to wonder: if I sign their form, what is the economic burden to patients who must pay for this mandated testing? Who will enforce these requirements? Will following these recommendations absolve a doctor from potential liability with this medication? Do any of these requirements tell us anything about problems with the medication after they are prescribed?
No.
But these requirements make our regulators feel good while ignoring the very real financial and time costs that they impose directly on patients and doctors.
For instance, I called the company and asked if they would provide me their required Medication Guide to give my patients. They politely suggested I take the time to print out the guide from their TikosynREMS.com website for each patient. Or better yet, maybe I could have my staff make copies of the three-page form for my patients!
Gee, thanks.
No doubt we'll soon have PradaxaREMS.com, EliquisREMS.com, SeroquelREMS.com, ViagraREMS.com and hundreds to thousands of other REMS websites, each with their own prescribing guides, patient medication quides and database registrations.
Safety first, remember?
I just wonder when I'll have the time to see all of my other patients.
-Wes
Next, read the 26-page prescribing information.
Next, read the patient's 3-page medication guide.
Next, fill out a database form for the drug company to add yourself to their new-and-improved database (even though you've already registered with them once before) once again before January 1, 2012.
Next, (and this is important), agree to the following:
- That patients initiated or reinitiated on the medication should be admitted for three days and a bunch of other stuff with that,
- That you understand that following the treatment initiation and dosing guidelines in the drug's label will decrease the chance of a drug-induced arrhythmia
- That you will inform the patients of the risk of arrhythmias
- That you will need to see them for an EKG and blood tests every three months
- That you will provide a Medication Guide to each patient at the initiation and re-initiation of the drug's therapy and that you will review the contents of the medication guide personally with each patient.
I have no idea where the every "three month" suggested lab testing and EKG requirement came from and have to wonder: if I sign their form, what is the economic burden to patients who must pay for this mandated testing? Who will enforce these requirements? Will following these recommendations absolve a doctor from potential liability with this medication? Do any of these requirements tell us anything about problems with the medication after they are prescribed?
No.
But these requirements make our regulators feel good while ignoring the very real financial and time costs that they impose directly on patients and doctors.
For instance, I called the company and asked if they would provide me their required Medication Guide to give my patients. They politely suggested I take the time to print out the guide from their TikosynREMS.com website for each patient. Or better yet, maybe I could have my staff make copies of the three-page form for my patients!
Gee, thanks.
No doubt we'll soon have PradaxaREMS.com, EliquisREMS.com, SeroquelREMS.com, ViagraREMS.com and hundreds to thousands of other REMS websites, each with their own prescribing guides, patient medication quides and database registrations.
Safety first, remember?
I just wonder when I'll have the time to see all of my other patients.
-Wes
Know What Barry Knows
.. and Get Back in Rhythm with Barry Manilow!
But you should also know this: as a physician who sees patients who already can't afford many of their antiarrhythmic and anticoagulant medications, these advertising and awareness campaigns are enough to make me avoid Sanofi products.
I know of no other way to stop this lunacy.
-Wes
But you should also know this: as a physician who sees patients who already can't afford many of their antiarrhythmic and anticoagulant medications, these advertising and awareness campaigns are enough to make me avoid Sanofi products.
I know of no other way to stop this lunacy.
-Wes
Education: Our New Direct-to-Doctor Advertising Initiative
Dear doctors:
I just want to make sure that your are "aware" of atrial fibrillation and its options for management at our new site that offers 1 AMA PRA Category 1 Credits™ credits through a local institution of higher learning.
With love,
Sanofi-Aventis
I just want to make sure that your are "aware" of atrial fibrillation and its options for management at our new site that offers 1 AMA PRA Category 1 Credits™ credits through a local institution of higher learning.
With love,
Sanofi-Aventis
The Idiocy of ICD-10: W22.02XD
In the interest of brevity and efficiency, I'll let this speak for itself:
-Wes
Related posts: Ten Times the Fun or my favorite: If Lawyers Billed Like Doctors
It's not clear how many klutzes want to notify their insurers that a doctor visit was a W22.02XA, "walked into lamppost, initial encounter" (or, for that matter, a W22.02XD, "walked into lamppost, subsequent encounter").If people want to know why they can't get an appointment in 2014 and why doctors are frustrated with our current health care system, look no further than ICD-10.
-Wes
Related posts: Ten Times the Fun or my favorite: If Lawyers Billed Like Doctors
Monday, September 12, 2011
Elementary, My Dear Watson
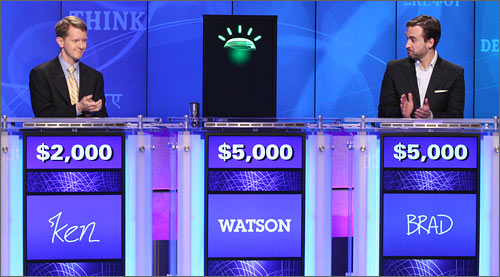
We should ask ourselves that question now, especially since your insurer might be using Watson to mine your electronic medical record to determine if your claim will be paid.
Wellpoint, one of the nation's largest insurers is joining forces with IBM to use Watson as a medical decision support tool:
The first Watson deployment would come early next year with WellPoint nurses who manage complex patient cases and review treatment requests from medical providers.As such, shouldn't such a computer program be subject to the same rigors as the medical device industry to achieve FDA clearance? Would regulators even be able to comprehend how Watson reaches it's comclusions as it culls through "200 million pages of information in less than three seconds?"
Or will this device be grandfathered in under a 510K exemption? After all, it's just a computer right? Seriously, what could go wrong with clinical decisions based on cold, hard, incomplete data sets that are extrapolated to patients?
Wait, I know!
It's the Daily Double!
-Wes
More Troubles for St. Jude's Riata Defibrillator Leads?
From the Minneapolis Star Tribune:
-Wes
Researchers in Ireland have discovered a possible problem with a heart defibrillator component made by St. Jude Medical Inc. in which wires that run from the device to the heart may poke through the outer coating of their cable.It should be noted that the "study" referenced in this artice was actually an abstract published in the European Heart Journal's September supplement edition. I could not find it online yet, but a copy of the source abstract can be found on CafePharma, the medical device / pharmaceutical industry representative's anonymous messaging board.
The study looked at 212 patients in Ireland who received St. Jude's Riata defibrillator lead and found that 15 percent had suffered such an "insulation breach," which could interfere with the device's life-saving therapy. Normal screening of the device or even X-rays may not pick up the breach, and patients would have no outward clue that their lead wire may be compromised.
-Wes
Sunday, September 11, 2011
In Their Memory

The cross, found by recovery crews, that carried a portion of twisted fuselage
One World Trade Center, Ground Zero, New York City, NY
Friday, September 09, 2011
Handoffs, Passoffs, and Liftoffs
The image of a team of track stars sprinting a 400-meter relay while carrying a little aluminum tube and passing it, effortlessly, without breaking stride is what I think of when I hear the term "handoff." In medicine, a "handoff" is more like sprinting the same race, or at least trying to, and passing a 100-kilogram boulder: there is simply nothing smooth about it.
In earlier times, doctors worked exclusively at one clinic and usually one hospital. There would classically be a "morning report" where attending, medical residents, interns, and a chief resident would assemble to hear the calamities that occurred the night before, discuss and dissect the most interesting cases, perhaps learn a tidbit from the highly respected "chief resident" - the Grand Pubah of all things medical - who had their whopping 1 year of independent clinical experience but plenty of time to assemble a case discussion to point out things you should have known.
The morning report was well-attended. It was, after all, a requirement for graduate medical education and actually a heck of a lot of fun. There was something strangely bonding that occurs when you see your colleague get embarrassed for their lack of understanding just as you had been the day before. It was never punitive (at least not usually), mind you, but rather constructed to make damn sure you never forgot the lapse in judgement you had made the night before.
Late afternoon "check-out" was a different matter. That meeting was never supervised by attendings and served as a "working" meeting between residents where cases were passed to the night call team. Not uncommonly, there were residents who had been there from the preceding night: they got to go first listing their patients' name, a brief problem list, pressing issues that needed to be checked, and so on. No brag, just fact.
And surprisingly, it usually worked.
But why did it work?
I think it worked because we were given responsibility. It was our butt on the line as you worked mano-a-mano with the patients you had to cover. We all knew were going to have to face the music the next morning if things didn't work out so well. The better the night went, the easier morning report was. The better the night went, the better your credibility with the nurses grew. The better the night went, the better the chances of getting selected for a residency slot. The better the night went, the better you slept the next day knowing the patients did well under your care.
Today, things are different. For resident trainees, there are more change of shifts with more handoffs, fewer patients per resident, and fewer hours in which to see the patients you are given from the group before. More dispersion, less ownership. But this is not always the resident's fault. In fact, when a problem arises on one or two patients during an evening call, it is now not uncommon for residents to have to handoff a handoff, having never seen or touched some of the patients they had heard about at their earlier signout. Fortunately, the dedicated (paid) GME physician-instructors are still consistently there at morning reports, but those with day-to-day clinical experience, the attendings and specialists tasked with making their own rounds each day, are at morning reports much less often. That's because they are seeing their growing inpatient populations no longer "covered" by housestaff and working to maintain productivity standards.
Handoffs for attendings themselves are also a growing problem as credentials for doctors are no longer are issued for one hospital, but a system of hospitals. Rarely do attendings meet face-to-face these days: a phone call will have to do since not uncommonly they're at one hospital and clinic one day and a different hospital and clinic the next. That's right, as challenged as handoffs for GME have become, the handoff issues for attending physicians with the consolidation of health care institutions underway isn't even being discussed.
Increasingly, I see the electronic medical record filling the handoff void between attendings. Lists can be assembled, short notes compiled with the patient's name/room number/institution attached to the particulars, leaving the on-call doctor to forage through the electronic chart for details as needed. Messy, lumbering, but it does work, yet (and this is important) it has nothing to do with the "handoff skills" our single-center residents are learning today.
I dream of the day I can text my colleague my signout list from my cell phone without having to worry about the HIPAA police. I dream of the day I can receive an EKG or a chest-xray without being threatened with the concern of litigation. I dream of the day when we can collaborate and work together again, whether virtually or in person, instead of in silos of responsibility.
Imagine: liftoffs rather than passoffs while making a 100-kilogram boulder as light as an aluminum tube.
Well, at least I can still dream, right?
-Wes
In earlier times, doctors worked exclusively at one clinic and usually one hospital. There would classically be a "morning report" where attending, medical residents, interns, and a chief resident would assemble to hear the calamities that occurred the night before, discuss and dissect the most interesting cases, perhaps learn a tidbit from the highly respected "chief resident" - the Grand Pubah of all things medical - who had their whopping 1 year of independent clinical experience but plenty of time to assemble a case discussion to point out things you should have known.
The morning report was well-attended. It was, after all, a requirement for graduate medical education and actually a heck of a lot of fun. There was something strangely bonding that occurs when you see your colleague get embarrassed for their lack of understanding just as you had been the day before. It was never punitive (at least not usually), mind you, but rather constructed to make damn sure you never forgot the lapse in judgement you had made the night before.
Late afternoon "check-out" was a different matter. That meeting was never supervised by attendings and served as a "working" meeting between residents where cases were passed to the night call team. Not uncommonly, there were residents who had been there from the preceding night: they got to go first listing their patients' name, a brief problem list, pressing issues that needed to be checked, and so on. No brag, just fact.
And surprisingly, it usually worked.
But why did it work?
I think it worked because we were given responsibility. It was our butt on the line as you worked mano-a-mano with the patients you had to cover. We all knew were going to have to face the music the next morning if things didn't work out so well. The better the night went, the easier morning report was. The better the night went, the better your credibility with the nurses grew. The better the night went, the better the chances of getting selected for a residency slot. The better the night went, the better you slept the next day knowing the patients did well under your care.
Today, things are different. For resident trainees, there are more change of shifts with more handoffs, fewer patients per resident, and fewer hours in which to see the patients you are given from the group before. More dispersion, less ownership. But this is not always the resident's fault. In fact, when a problem arises on one or two patients during an evening call, it is now not uncommon for residents to have to handoff a handoff, having never seen or touched some of the patients they had heard about at their earlier signout. Fortunately, the dedicated (paid) GME physician-instructors are still consistently there at morning reports, but those with day-to-day clinical experience, the attendings and specialists tasked with making their own rounds each day, are at morning reports much less often. That's because they are seeing their growing inpatient populations no longer "covered" by housestaff and working to maintain productivity standards.
Handoffs for attendings themselves are also a growing problem as credentials for doctors are no longer are issued for one hospital, but a system of hospitals. Rarely do attendings meet face-to-face these days: a phone call will have to do since not uncommonly they're at one hospital and clinic one day and a different hospital and clinic the next. That's right, as challenged as handoffs for GME have become, the handoff issues for attending physicians with the consolidation of health care institutions underway isn't even being discussed.
Increasingly, I see the electronic medical record filling the handoff void between attendings. Lists can be assembled, short notes compiled with the patient's name/room number/institution attached to the particulars, leaving the on-call doctor to forage through the electronic chart for details as needed. Messy, lumbering, but it does work, yet (and this is important) it has nothing to do with the "handoff skills" our single-center residents are learning today.
I dream of the day I can text my colleague my signout list from my cell phone without having to worry about the HIPAA police. I dream of the day I can receive an EKG or a chest-xray without being threatened with the concern of litigation. I dream of the day when we can collaborate and work together again, whether virtually or in person, instead of in silos of responsibility.
Imagine: liftoffs rather than passoffs while making a 100-kilogram boulder as light as an aluminum tube.
Well, at least I can still dream, right?
-Wes
Thursday, September 08, 2011
Data Security: A Rising Problem for Electronic Health Records
It was kind of funny reading this recent article from the New York Times that focuses on a relatively small health data breach from Stanford Hospital's emergency room:
The real question that should be asked is this: What is the Department of Health and Human Services going to do about all of these data breaches? They seem to be intent on assuring us they're doing a good job enforcing these breaches, but we have to wonder.
So far, it seems they really can't do much to stem the tide: there are just too many people with computers claiming a "need to know" that have access to patients' private health data.
-Wes
Addendum: Make that 7.9 million records breached since 2009. (h/t: PDara, MD via Twitter)
Related: KevinMD blog: Your medical information is not private, and it's sold routinely.
A medical privacy breach involving Stanford Hospital in Palo Alto, Calif., led to the public posting of data for 20,000 emergency room patients, including names and diagnosis codes, on a commercial Web site for nearly a year, the hospital has confirmed."Medical security breaches are not uncommon" is an understatement. According to the Department of Health and Human Services, 5,408,977 people have had their medical data lost or stolen, so an article that cries foul of 0.37% of this 2010 total seems fairly trivial. Worse, the reported trend is rising.
Since discovering the breach last month, the hospital has been investigating how a detailed spreadsheet made its way from one of its vendors, a billing contractor identified as Multi-Specialty Collection Services, to a Web site called Student of Fortune, which allows students to solicit paid assistance with their schoolwork.
Gary Migdol, a spokesman for Stanford Hospital and Clinics, said the spreadsheet first appeared on the site on Sept. 9, 2010, as an attachment to a question about how to convert the data into a bar graph.
Although medical security breaches are not uncommon, the Stanford breach was notable for the length of time that the data remained publicly available without detection.
The real question that should be asked is this: What is the Department of Health and Human Services going to do about all of these data breaches? They seem to be intent on assuring us they're doing a good job enforcing these breaches, but we have to wonder.
So far, it seems they really can't do much to stem the tide: there are just too many people with computers claiming a "need to know" that have access to patients' private health data.
-Wes
Addendum: Make that 7.9 million records breached since 2009. (h/t: PDara, MD via Twitter)
Related: KevinMD blog: Your medical information is not private, and it's sold routinely.
Wednesday, September 07, 2011
The Flywheel
(With apologies to Harry Chapin)
A child arrived just the other day. He came to the world in the usual way..."I had the most amazing case today! His heart rate was so slow..."
"Doctor, we're impressed at how things are going."
He learned to walk while I was away..."Thanks for helping out when we were short-staffed..."
There were planes to catch and bills to pay, he learned to walk while I was away."You've had a good month. You should see your bonus with your next paycheck."
He was talking before I knew it..."We're thinking about opening a new lab at our other hospital. We'd like you to help us with the design..."
My son turned ten just the other day..."Just a little longer, honey, I've got to finish this talk..."
He said, "Thanks for the ball, Dad, come on let's play..."I'll try and make it, but today's schedule looks horrible."
Can you teach me to throw, I said "Not today... I got a lot to do.""Doctor, your next available new-patient appointment is in two months. You have no open appointments. Should we double-book her?"
Well, he came home from college just the other day..."Your privileges may be suspended if you don't complete your two chart deficiencies."
"We need someone to teach EKGs to third year medical students."
Son, I'm proud of you, can you sit for a while?"Another good month. Your top-box scores are better, too."
What I'd really like, Dad, is to borrow the car keys. See you later, can I have them, please?"Congrats on your pregnancy, Ms. Wonder Nurse! Don't worry about a thing, we've needed to cross-train our other staff anyway..."
I called him up just the other day..."Doctor Frigamafratz's daughter needs an appointment before going back to college..."
I said, "I'd like to see you if you don't mind.""Are you on call again this weekend?"
He said, "I'd love to, Dad, if I can find the time.""When you get done with clinic, I was wondering if you could see two consults at Hospital OverThere? Oh, and don't forget the 7 am meeting tomorrow."
And as I hung up the phone it occurred to me, my boy was just like me.-Wes
P.S.: The inspiration for this post.
Tuesday, September 06, 2011
Taking Matters In To Your Own Hands

Despite having a living will for about 30 years, she said the tattoo meant there was be "no excuse" for error.Talk about taking one for the team!
"The tattoo is immediate... no excuse for not knowing what I thought," she said.
The grandmother, who is diabetic but said she was not seriously ill, said she got the idea from a retired nurse, who did something similar in 2003.
She said her willingness to not be resuscitated would "save money" for the NHS.
Good for her.
-Wes
(P.S.: Be sure to take the poll in the sidebar to the right!)
P.P.S.: The poll, which asked the following question:
"A cardiac arrest patient is brought to your ER with CPR in progress. A DNR tattoo is seen and no family is available. You would:
1) Continue CPR/ACLS as indicated
2) Stop CPR/ACLS immediately"
There were 85 respondents, 39 (39%) of whom would continue CPR and 53 (60%) who would stop CPR immediately.
Jobs Jobs Jobs - Grand Rounds is Up
Witty, pithy, and clever as always, Dr. Rich's belated Labor Day edition of Grand Rounds is up.
-Wes
-Wes
Monday, September 05, 2011
When Nurses Wear "Do Not Disturb" Signs
It was supposed to be one of a series of "measures to improve safety, reliability, patient experience, staff satisfaction and efficiency of medicine management." Instead, the wearing of red "tabards" by nurses that read "Do Not Disturb" while they distributed medications has proven to be the straw that broke the camel's back in England. While the "Do Not Disturb" message on the tabards was replaced with a message that reads "Drug Round in Progress," isn't the message the same?
Directive Number 99365.23a: "In the Name of Safety, Do Not Bother Me While I Hand Out Medications."
It seems almost too incredible to believe and yet, this is how it's playing out now in England's National Health Service.
I'm not sure I've seen a better example of where the caring professions are heading in a world of government-directed health care delivery; where personal responsibility is slowly replaced by personnel mandates. Can every single aspect of human interaction and decision-making be controlled by a Central Patient Safety Authority?
American's should heed this warning from our friends across the pond, especially when our Director of CMS and former safety czar states:
Quality.
Quantity.
Lower Cost.
Pick any two.
For those of us who live in the real world, we should ask ourselves a seemingly simple question: Where are we willing to cut the quality of the health care delivery in America in favor of lowering costs and covering more of the uninsured?
-Wes
h/t: Norman Briffa MD of the Thinking Allowed - Conversation with a Chestcracker blog
Directive Number 99365.23a: "In the Name of Safety, Do Not Bother Me While I Hand Out Medications."
It seems almost too incredible to believe and yet, this is how it's playing out now in England's National Health Service.
I'm not sure I've seen a better example of where the caring professions are heading in a world of government-directed health care delivery; where personal responsibility is slowly replaced by personnel mandates. Can every single aspect of human interaction and decision-making be controlled by a Central Patient Safety Authority?
American's should heed this warning from our friends across the pond, especially when our Director of CMS and former safety czar states:
Improving care and lowering costs are at the heart of the Affordable Care Act. As a pediatrician, as a patient and now as administrator of the Centers for Medicare & Medicaid Services, I have seen our health care system both at its best and at its worst. We know that system that we want — and with the ACA, we can have it.Sorry, but when cost containment is involved in the equation (and this remains Priority One for our much larger health care US Health Care system) and we want to cover more of the uninsured in America, eventually something has to give.
Quality.
Quantity.
Lower Cost.
Pick any two.
For those of us who live in the real world, we should ask ourselves a seemingly simple question: Where are we willing to cut the quality of the health care delivery in America in favor of lowering costs and covering more of the uninsured?
-Wes
h/t: Norman Briffa MD of the Thinking Allowed - Conversation with a Chestcracker blog
Friday, September 02, 2011
A Few Aphorisms to Remember

While this question startled those who had never experienced his candor before, it always served to remind his staff and colleagues of his patient's post-operative reality and his sensitivity to it. Invariably, his post-op visit would be concluded with "Ya know, you're gonna be alright."
And ya know, more often than not, he was usually right.
Needless to say, he made quite an impression with people over the years. No one worked harder or worked crazier hours: transplant services, heart attacks, shootings and motor vehicle accidents have a way of doing that to you.
But he was always a man who lead by example, never from above.

But later in the evening there came a point where this man wanted to say a few words of thanks himself to those with whom he had had the pleasure to work with over the many, many years. As he said, "There are two ways to talk about things like this, one a somber, melancholic reflection and what this all means, or as I'd like to prefer right now, a reflective, more lighthearted way. I think I'll stick with the more lighthearted way tonight."
He reached in to his pocket and pulled a small green notecard, but dusk had given way to dark at the outdoor affair and reading was nearly impossible. Several people sprang forth with a Tiki-torch and and a flashlight app to assist his vision because everyone wanted to hear what he might say.
He began:
"Thank you all for coming. It is wonderful to see so many colleagues, nurses, trainees, and former patients here. My wife will soon be happy knowing that hers will be the only woman's voice that I'll be talking to in the middle of the night from now on."When the laughter subsided, he continued:
"I'd like to share a few aphorisms with you. For those unfamiliar with what an aphorism is, it's a little saying that usually has a meaning that goes beyond the saying itself. They're what has guided me and things that I want to leave with you.Thank you, John, for everything.
First, medicine is a contact sport. It's one thing to get in there and play the game, but more often than not you're going to get knocked down. It's how people get back up and overcome their disappointments that will determine their success.
Second, medicine is a full-time job. Medicine knows no day and no night. Time in medicine is not measured in minutes or hours, it is measured in years.
Third, have courage. Try new things. Stretch yourself. There will come times when you have to do things that no one else will. Have courage.
Fourth, when you call me in the middle of the night remember, keep the 'crit over 30 and I'll sign just about anything you want in the morning.
Also, I've found a little saying that works pretty well in the ICU when I sign out to my team and colleagues at 10PM: "Go ahead, take the rest of the night off."
Finally, if you remember nothing else, remember this:
You're in charge."
Oh, and one more thing:
Go Duke!
:)
-Wes
Thursday, September 01, 2011
Of Pens and Payoffs
It's the ultimate irony to this casual observer.
Remember when doctors were chastised for accepting a pen worth pennies from a pharmaceutical company due to the pharmaceutical industry's pervasive marketing techniques that swayed the prescribing practices of millions of doctors?
Bad doctors.
We should have known better: all that covert marketing influence created by all those pens. No doubt thanks to that former practice we were single-handedly raising health care costs for Americans every time we looked at our pop-up Viagra pens. Man were we dogs!
Dirty. Rotten. Scoundrels. All.
So thank GOODNESS that the FDA can raise the fees it extracts from those same drug companies for their purposes! Certainly there would never be any influence on members of the FDA, especially since the negotiations between the FDA and the pharmaceutical lobbying organization were "relatively smooth." Let's see: A 6% increase to the 62% of the $930 million the FDA spends annually to review new pharmaceutical applications?
Around here, we call this "The Chicago Way:"
It's just a little money for a few pens.
Really."
-Wes
Remember when doctors were chastised for accepting a pen worth pennies from a pharmaceutical company due to the pharmaceutical industry's pervasive marketing techniques that swayed the prescribing practices of millions of doctors?
Bad doctors.
We should have known better: all that covert marketing influence created by all those pens. No doubt thanks to that former practice we were single-handedly raising health care costs for Americans every time we looked at our pop-up Viagra pens. Man were we dogs!
Dirty. Rotten. Scoundrels. All.
So thank GOODNESS that the FDA can raise the fees it extracts from those same drug companies for their purposes! Certainly there would never be any influence on members of the FDA, especially since the negotiations between the FDA and the pharmaceutical lobbying organization were "relatively smooth." Let's see: A 6% increase to the 62% of the $930 million the FDA spends annually to review new pharmaceutical applications?
Around here, we call this "The Chicago Way:"
They pull a knife, you pull a gun. He sends one of yours to the hospital, you send one of his to the morgue. That's the Chicago way."Influence? What influence? I'm not seein' no stinkin' influence of these payments to our government officials! No way!
–Jim Malone, "The Untouchables"
It's just a little money for a few pens.
Really."
-Wes
Dr. Charles 2011 Poetry Contest
From The Examining Room of Dr. Charles blog:
-Wes
Announcing the second annual Poetry Contest!Last year's winning entries were impressive. Why not give it a try?
An award will be given to the writer who submits for consideration the most outstanding poem within the realm of health, science, or medicine.
The contest starts today and ends September 31st, 2011. The winners will be chosen shortly thereafter by an elite group of 8 judges (other doctors, friends with literary training, and select bloggers).
The contest is open to everyone.
-Wes
Your Beatin' Heart....
... could someday be donated to someone warm, toasty, and beating in a box:

Public relations video here.
-Wes

Public relations video here.
-Wes
Subscribe to:
Posts (Atom)