Her breathing had never taken a second thought, except for the past several months. Slowly, gradually, her breathing became work so she came to our emergency room.
Her life had been an full one: married, kids, grandkids - all of whom brought her incredible joy. But since the loss of her husband and all of the changes that occurred in her life as a result, she felt more alone than ever. Perhaps this was the reason the pacemaker she had received some 14 years before just didn't seem so important any more. Her kids and grandkids were what remained now, and for them she was grateful for they had noted she'd become too short of breath with even the slightest effort, so they brought her in.
The chest-xray taken when she came to the Emergency Room showed her pacemaker and prompted the ER staff to ask about it. "She hasn't had a pacer check in a while, " the family mentioned. So we were consulted to check the pacemaker's function.
Before we'd done so, we looked at her EKG and weren't surprised at what it showed. After all, we'd seen this scenario before.
So with some confidence I entered her room. There sitting beside her was one of her sons and a granddaughter. She was propped up in bed wearing a green oxygen face mask that covered her mouth and nose but couldn't suppress her kind smile as I entered. After a brief introduction, I explained what her EKG showed and how I thought a good portion of her shortness of breath might be stemming from her pacemaker's low battery.
In our conversation she mentioned that she had been told her pacemaker battery would need to be changed soon. That was before her husband died. After his funeral, the need for a recheck of her pacemaker was quickly forgotten. So she had not anticipated that the pacemaker might be a cause of her symptoms.
We discussed her options. She could leave things well enough alone if she preferred while we arranged to keep her comfortable for her remaining days, or we could change her pacemaker battery. At the time, she didn't want excessive resuscitation measures and had declared herself a "DNR - Do Not Resuscitate" in the event of cardiac arrest. She thought hard about the choices but wasn't sure...
"Mom, it seems like such a small thing and it might be able to help you feel better! Don't you want to see your grandkids a little longer?" the son pleaded. She listened to him, then looked at me. It was clear she understood the choices and their implications. I suggested she think about it and left the room to give them time to discuss things. Some time later, she asked me to return.
She asked again, "So you think it might help me feel a bit better to have the battery changed?"
I replied, "Honestly, I do, but it's always hard to gauge how much."
So after a few more questions were answered and worried looks shared with her son, she agreed to have her battery replaced. I left the room to document my visit. (After all, nothing happens in medicine any longer unless typing occurs.) Seated next to me was my nurse practitioner, herself transfixed to the computer screen as she returned patient phone calls and made arrangements for procedures to be performed the next day. Next to her was the pacemaker programmer which she wisely brought with her to help check the patient's device. She finished her call and then offered to check the device while I finished my note. I thanked her and continued typing.
It was still relatively early in the afternoon and the eight computer terminals around me were completely occupied by nurses, physical therapists, and residents hammering away and looking stone-faced, somewhat akin to what the New York Times newsroom must look and sound like just before deadline.
Until that sound was shattered by "Call a Code! Code Blue! Get Dr. Fisher!"
Somewhat startled, I looked up to see a sudden shift of the masses. Was that the voice of my nurse practitioner? It couldn't be, could it?
It was.
Poor thing. It seems she placed the wand of the pacemaker programmer over the patient's device, only to see a strange screen on the programmer appear that read something like: "Pacemaker reached ERI 8/13/2013…" followed by a bunch of other text that said something about "Power-on Reset mode" among other things. As she struggled to read the long message and donned a pair of glasses, she noted some twitching in the corner of her eye coming from the patient's direction. She looked up to see a peaceful blank stare on the patient who now laid motionless and unresponsive - a quick glance at the monitor showed it had flat-lined with only a rare agonal ventricular escape rhythm. Realizing what had happened, she was briefly at a loss how to react. This was not supposed to happen. Fleeting thoughts raced through her head like "Seriously?" and "Oh, God, I'm too old for this!" That's when she called out for help.
The poor son and granddaughter sitting in the corner were stunned, not knowing what had just happened. A horde of medical personnel swept in to the room and ushered them out, terrified. I entered the fray and saw my pleasant patient lying there motionless, small puffs of condensation appearing on her face mask and her pupils somewhat dilated. The monitor, too, was devoid of motion, except for an occasional blip seen one the screen. I reached for a pulse. It correlated to the monitor. Not much at all.
"Can we get some atropine and epi?" A asked the code team nervously assembled, not knowing what to do in this "no code" situation. Fortunately, I removed the programmer head from her chest and watched her breathing carefully. Seconds seemed like hours as my poor nurse practitioner stood beside me with her mind scrambling. "Come on guys, we need those meds… What's taking so long?… " she snipped. "Get the pacing patches!" They still were rifling through the drawers of the crash cart when she offered like a pro: "Guys, the purple box!" And within a second, the purple box appeared. The first medication was administered as time seemed to stand still. An occasional blip, then more people in the room. "What can we do?" the anesthesiologist asked.
I looked at the monitor dreading the thought of starting CPR given her wishes, or the what I might say to the stunned family at her bedside if we didn't.
But then, just as unexpectedly as it had begun, a paced rhythm resumed on the monitor! "Hold it!" I said, "I think we have a pulse!" And like a wilted daisy that just received its water, she immediately regained consciousness and wondered what all the fuss was about.
"What happened? Where did all these people come from? Why are they here?"
"It seems your pacemaker battery is a lot lower than anyone expected, Ms. Jones (not her real name). When we checked it, we must have used some of the last energy that pacemaker had. It looks like we need to take you our laboratory and replace that battery right away!"
She smiled and looked up at me with her precious eyes gleaming. Here we were, total strangers just minutes before, now bound together by some unimagineable force. She looked so comfortable lying there, then out of nowhere she reached up to me and grabbed my head, pulling it toward her oxygen mask in an attempt to give me a kiss right through it.
"Thank you," she whispered and smiled, "Thank you."
After reassuring her family and explaining what had happened, we hurried off to the EP lab, our eyes transfixed on her monitor and me still reeling from that beautiful and totally unexpected kiss...
... plastic face mask and all.
-Wes
Showing posts with label EKG. Show all posts
Showing posts with label EKG. Show all posts
Friday, May 01, 2015
Monday, November 18, 2013
When We Empower Patients to Pay for Expertise
"I know what you're thinking, punk. You're thinking "did he fire six shots or only five?" Now to tell you the truth I forgot myself in all this excitement. But being this is a .44 Magnum, the most powerful handgun in the world and will blow you head clean off, you've gotta ask yourself a question: "Do I feel lucky?" Well, do ya, punk?Today, Alivecor accounced the launch of their AliveInsights(TM) EKG interpretation service where patients decide with their own dollars and sense, who interprets the single-lead EKG generated by Alivecor's EKG iPhone case. If the patient feels fine with a technician and wants a response in 30 minutes, they can get their answer if they elect to pay $2. If that same patient wants a "Board Certified" US cardiologist to interpret their tracing and are are willing to wait up to 24 hours, they can elect to cough up $12 instead.Harry Callihan (played by Clint Eastwood) in "Dirty Harry"
Gee, which would you take?
My bet is that Alivecor's guessing people will accept the cheaper alternative. But will prescribing doctors?
It is an interesting model. I learned from Dr. Dave Alpert, the inventor of the Alivecor iPhone case, that "board certified" cardiologists get to keep $10 of the interpretation fee for providing the service - no insurance forms to fill out, no worry about a technical fee for the patient - just a plain ol' cash payment model.
Perhaps what is most interesting to me is how incredibly disruptive this model is to our current medical model.
But there are other concerns for doctors who might elect to "prescribe" an Alivecor case to their patients.
If the patient elects to pay $2 and a "technician" mis-reads the EKG, is the prescribing physician legally responsible for adverse outcomes that might occur? Who is responsible if a cardiologist mis-reads the transmitted EKG - the prescribing physician or the interpreting physician (presuming they are not always the same individual)?
These are interesting questions to ponder as this service launches. Certainly other issues are likely to arise where the lines of patient responsibility become blurred. Still, I like the fact that Alivecor is moving head-on into this space. It sets an exciting opportuntity for patients to have more control over their health concerns, and if this helps them, then all the better.
So as Harry Callihan said, "Feel lucky, punk?"
-Wes
Saturday, September 21, 2013
Shadow Puppet: An App That Lets iPhone Pictures Tell a Story
They say a picture is worth that thousand words, but nowhere is this more true than with a new, free, iPhone app called Shadow Puppet that lets you turn selected photographs on your iPhone into a narrated video storyline.
I saw this app reviewed over at Techcrunch and immediately saw its potential as a teaching aid. The app allows you to pick a series of iPhone photos from your camera roll, order them, and then record a narrative about your pictures. What is unique is that you can zoom or move between photos as you tell your story, annotating them by touching areas on the photo that you are discussing as it records the video. (Very cool).
Here's my very first video I made with the app describing the new Zio XT patch monitor that records 14-days of a patient's heart rhythm that we've been using in our clinic. Simply made, these video clips are easily shared via email, Facebook or Twitter. For this particular video, I still had to edit portions of the patient's report on Photoshop, then sent the images to my iPhone but, still, that was easily done.
Want to teach a fellow how to implant a pacemaker? Take some photos and show them! Have an EKG that has a finding that you're not sure about? Snap a picture (without patient identifying information, of course) , annotate it with your question and send it to your EP! Simple, elegant, and who knows, maybe even life-saving.
-Wes
I saw this app reviewed over at Techcrunch and immediately saw its potential as a teaching aid. The app allows you to pick a series of iPhone photos from your camera roll, order them, and then record a narrative about your pictures. What is unique is that you can zoom or move between photos as you tell your story, annotating them by touching areas on the photo that you are discussing as it records the video. (Very cool).
Here's my very first video I made with the app describing the new Zio XT patch monitor that records 14-days of a patient's heart rhythm that we've been using in our clinic. Simply made, these video clips are easily shared via email, Facebook or Twitter. For this particular video, I still had to edit portions of the patient's report on Photoshop, then sent the images to my iPhone but, still, that was easily done.
Want to teach a fellow how to implant a pacemaker? Take some photos and show them! Have an EKG that has a finding that you're not sure about? Snap a picture (without patient identifying information, of course) , annotate it with your question and send it to your EP! Simple, elegant, and who knows, maybe even life-saving.
-Wes
Tuesday, August 13, 2013
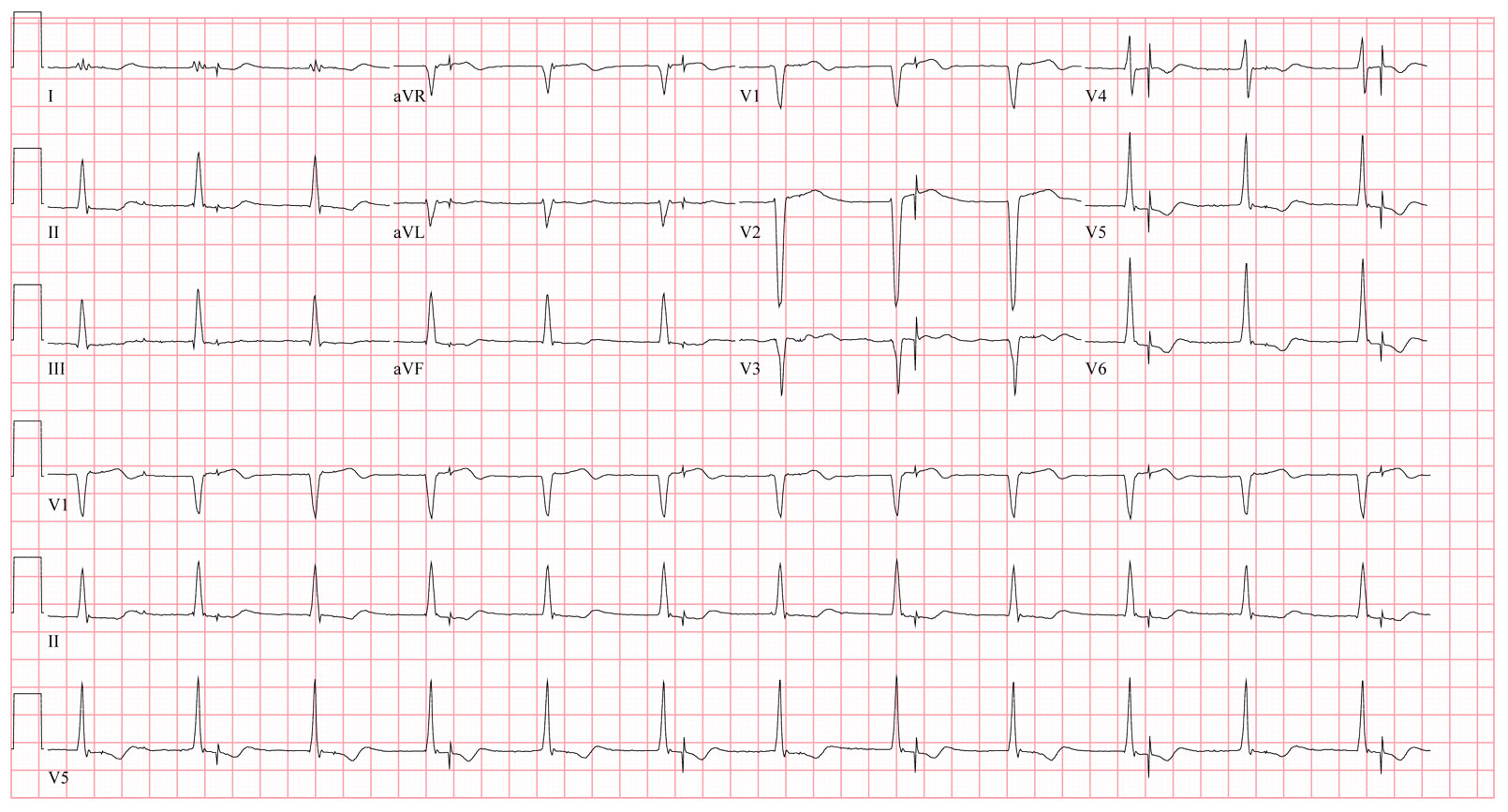
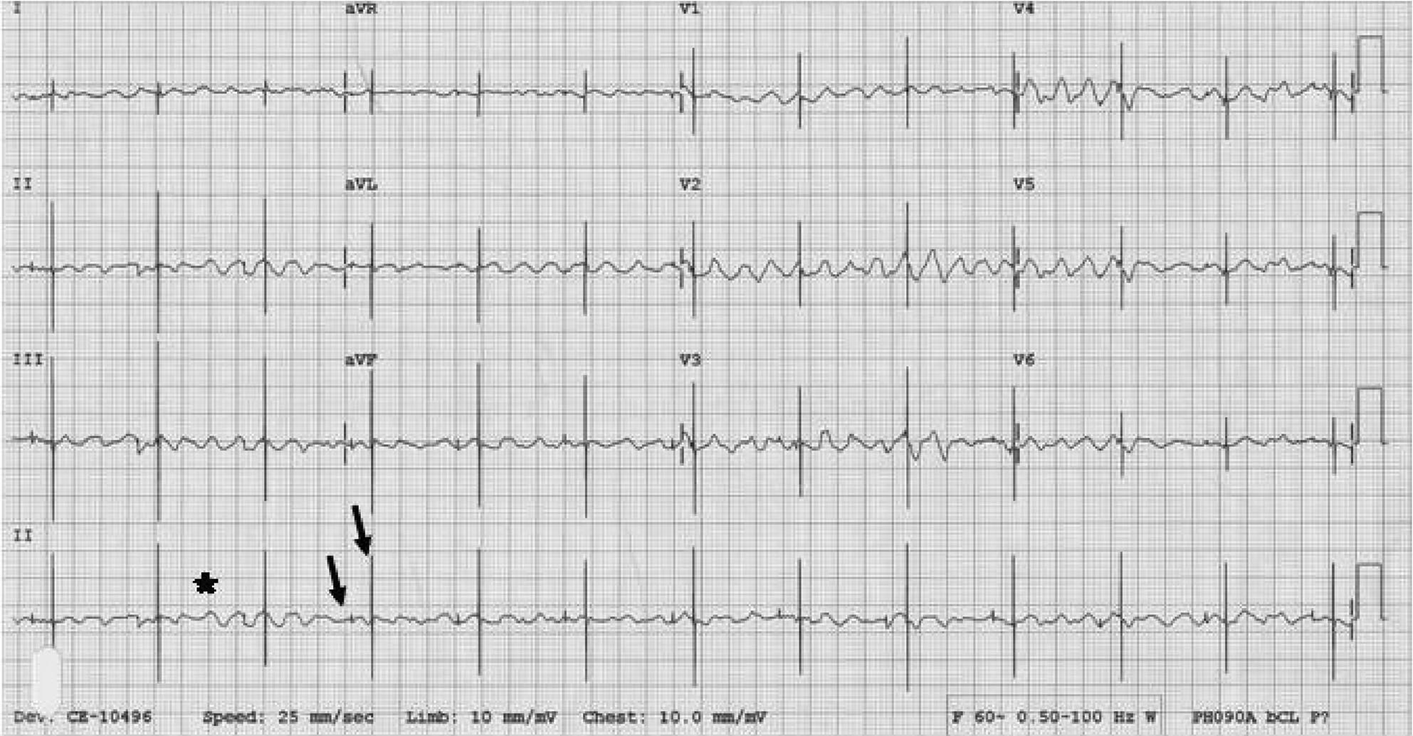
EKG Du Jour 32: The Misfiring Pacemaker
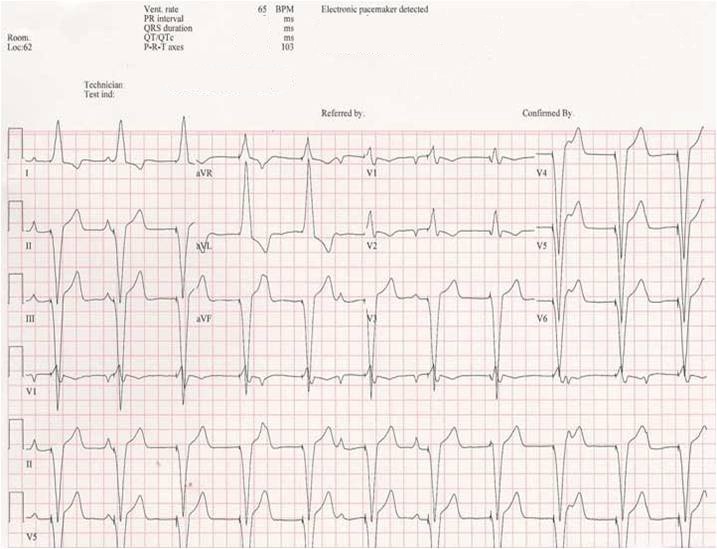
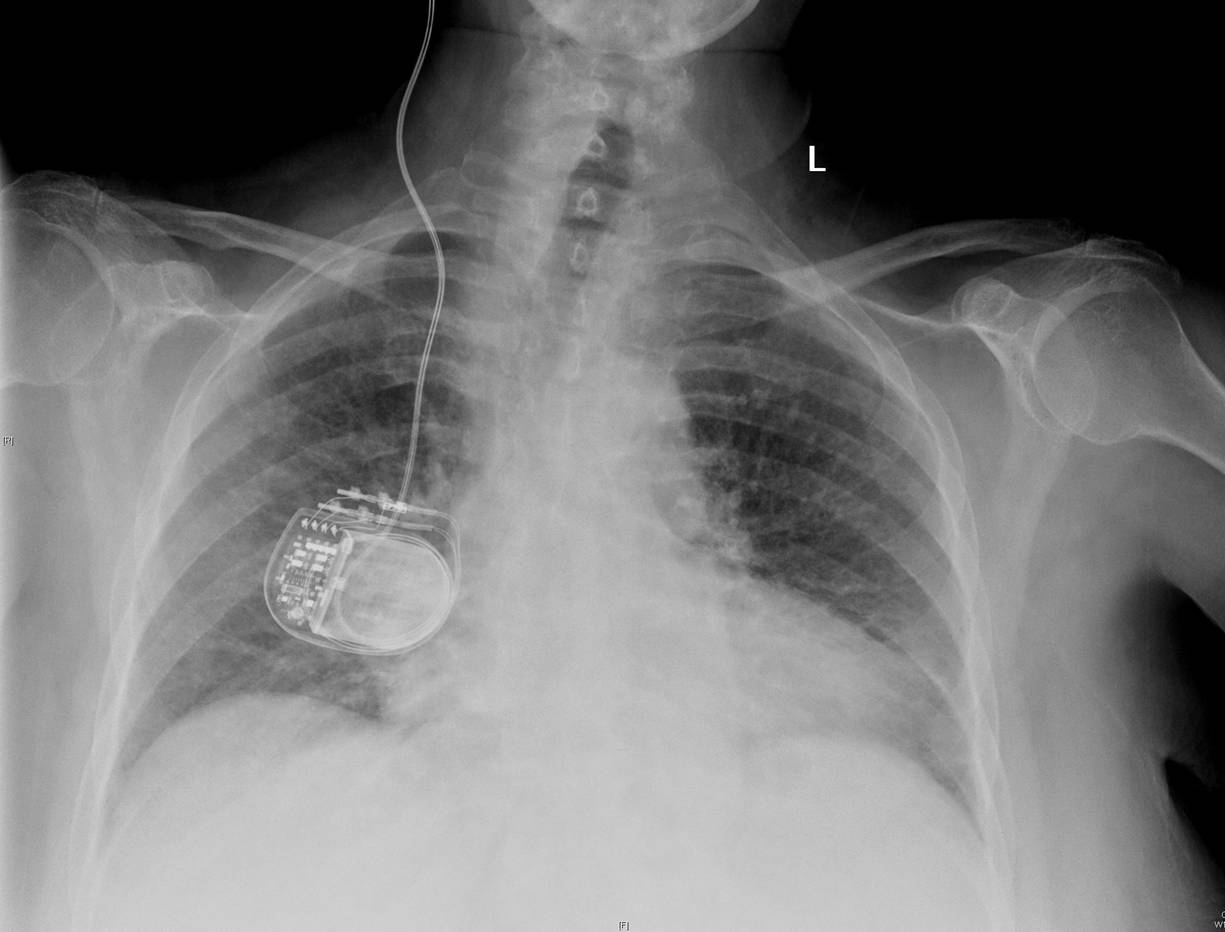
A dual chamber pacemaker was implanted the prior day by a local surgeon in the operating room. The next morning, an EKG is obtained that showed the following:
You checked the CXR and all leads appeared to be in the proper location.
Does the patient have to go back to the operating room? Why or why not?
-Wes
 |
| Click to enlarge |
Does the patient have to go back to the operating room? Why or why not?
-Wes
Friday, May 03, 2013
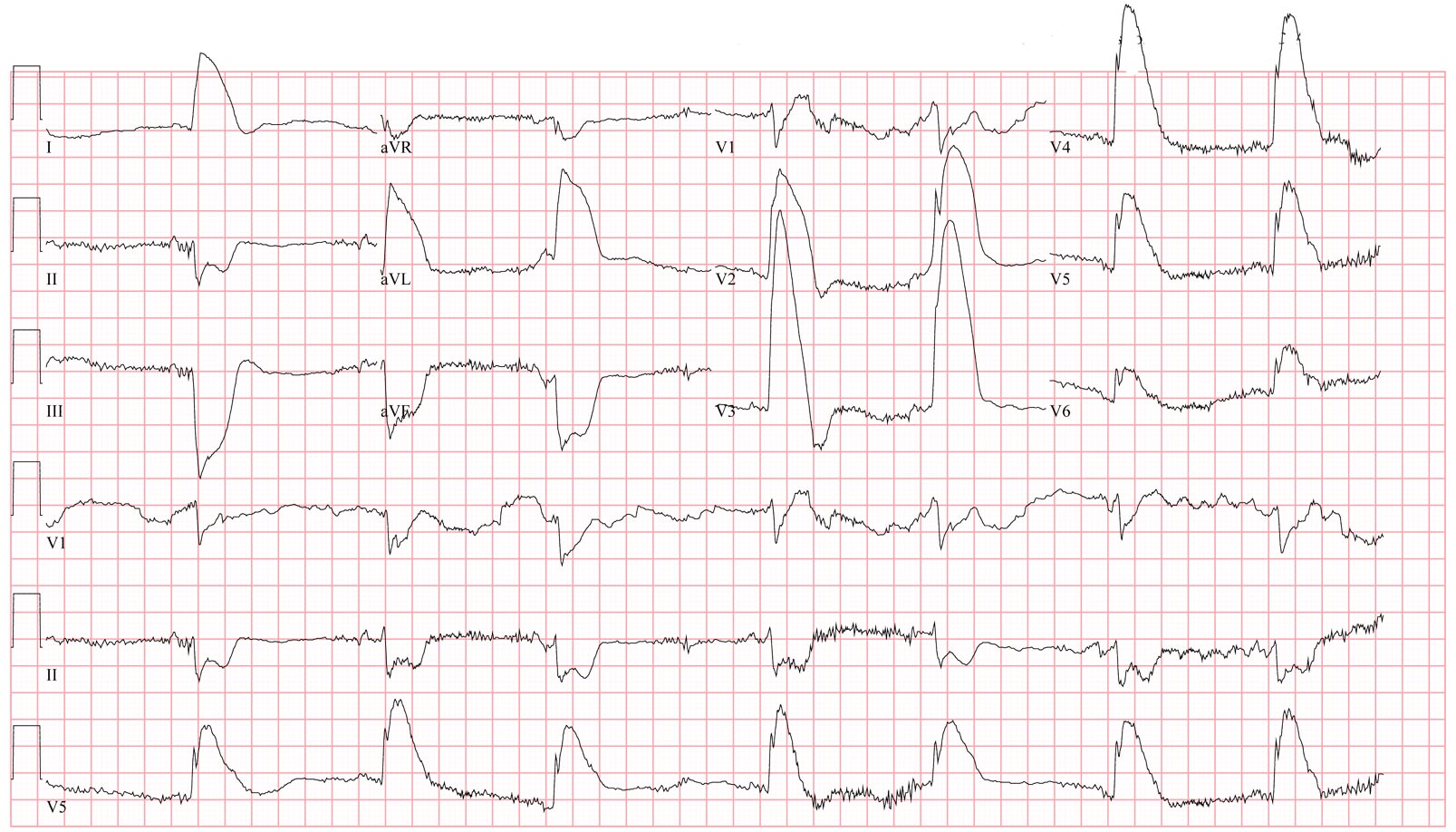
EKG Du Jour #31: A Case of Chest Pain
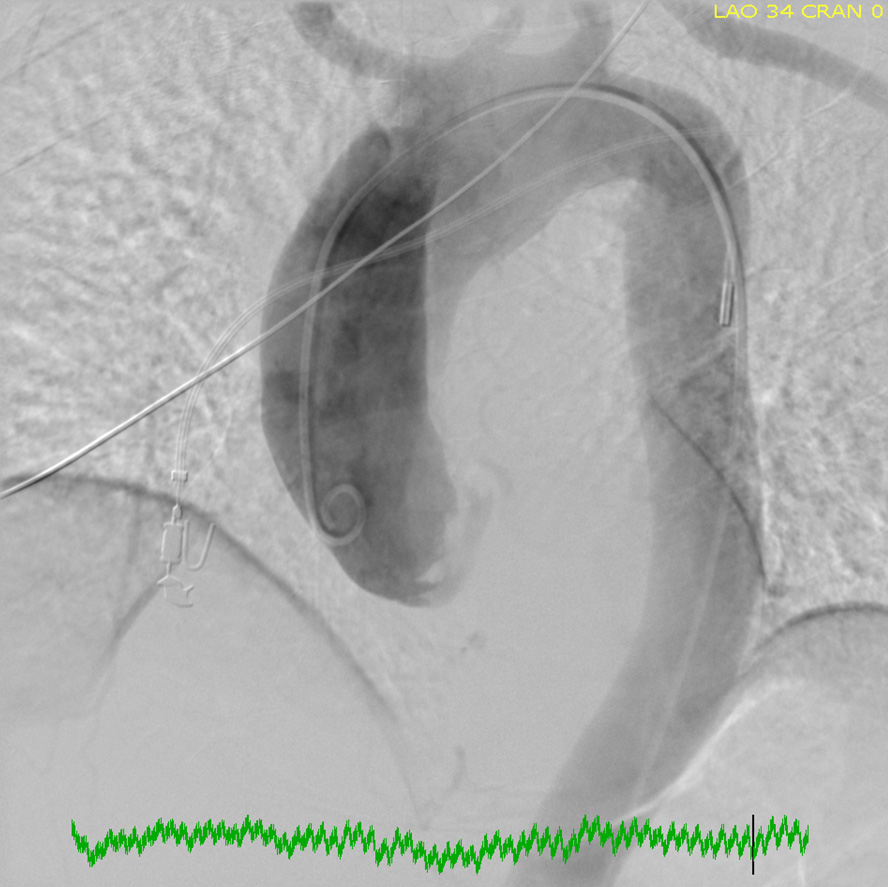
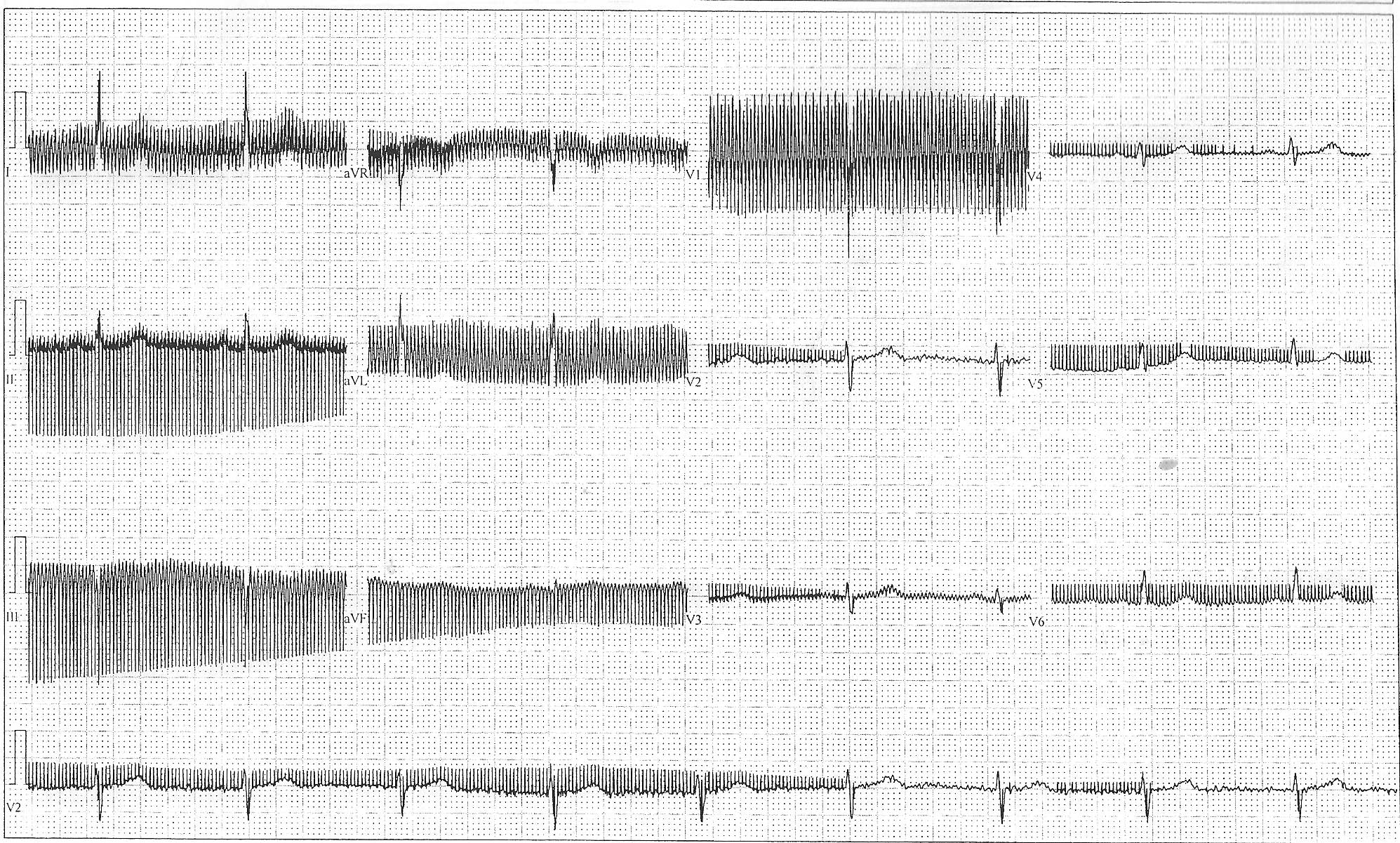
A 61 year old patient presented to your ER with chest pain, low blood pressure, and this EKG:
Now before you leap to the answer at the link provided below, ask yourself:
(a) What is this?
(b) What could cause this?
(c) How would you manage it?
And when you've really thought about it, click here for the answer but be prepared to describe what you see and what you'd do next.
-Wes
P.S.: (Yeah, I'm giving the answer now because it's Friday)
 |
| (Click image to enlarge) |
Now before you leap to the answer at the link provided below, ask yourself:
(a) What is this?
(b) What could cause this?
(c) How would you manage it?
And when you've really thought about it, click here for the answer but be prepared to describe what you see and what you'd do next.
-Wes
P.S.: (Yeah, I'm giving the answer now because it's Friday)
Tuesday, April 16, 2013
How to Change The Battery in Your iPhone's Alivecor Heart Monitor Case
After recording about 120 electrocardiogram (ECG) tracings from your Alivecor iPhone case, the device will suddenly stop recording EKGs when the battery in the case cover runs low. Fortunately, replacing the battery is a very simple process.
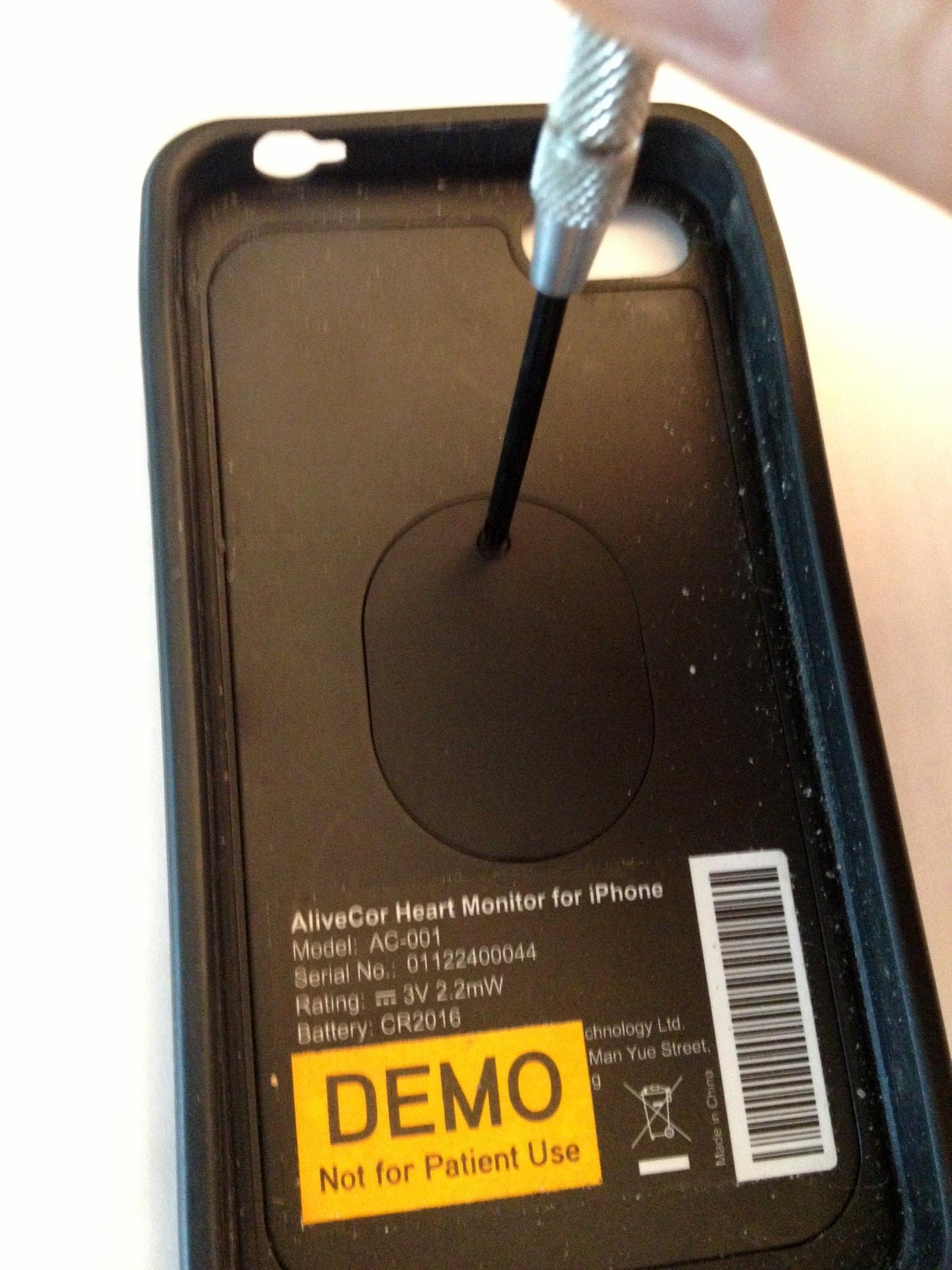
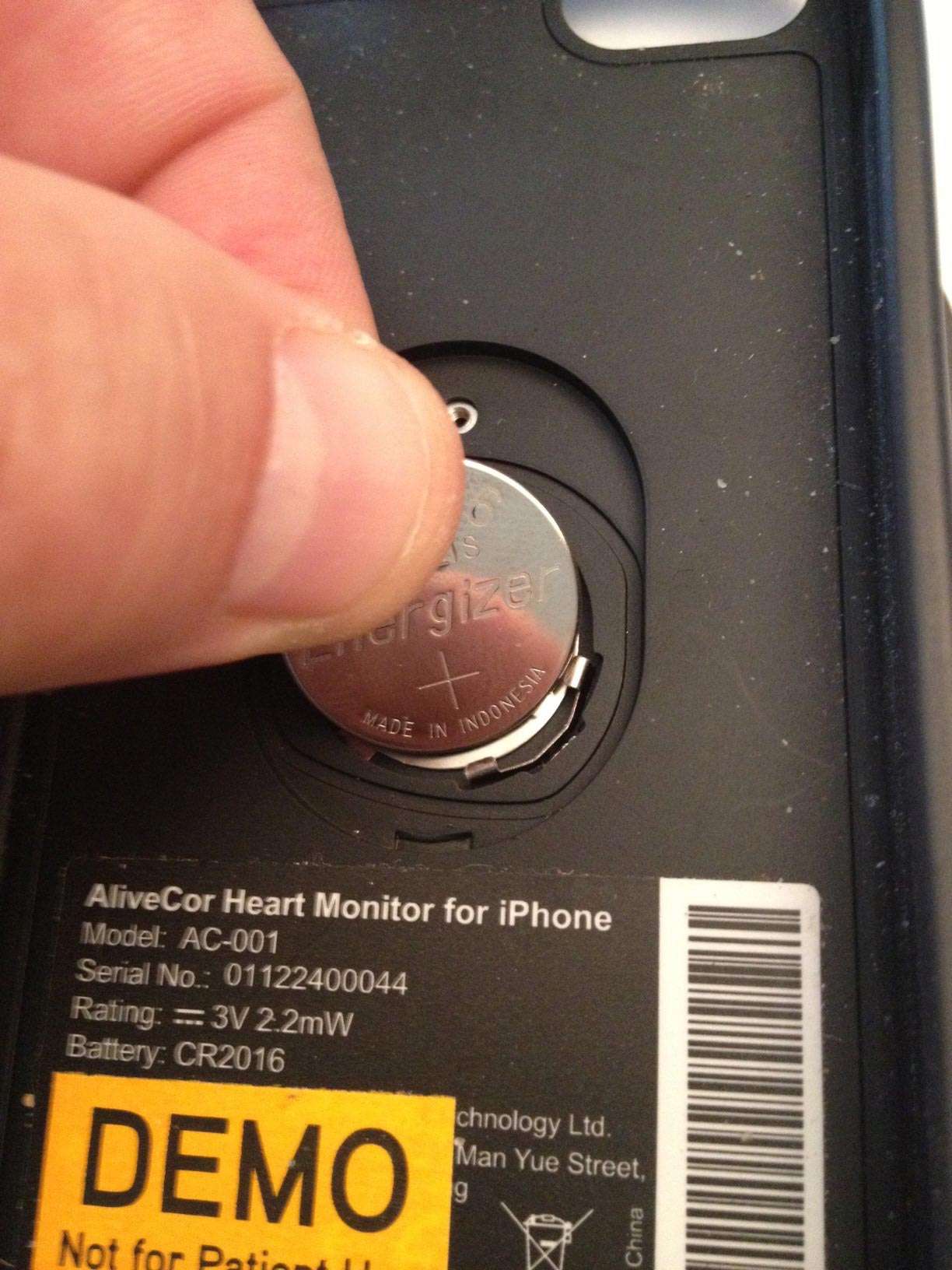
First, assemble all of the items needed: (1) a new 3-volt model 2016 battery (I got mine from Walgreens), (2) a tiny Phillips screw driver (used to repair eye-glasses and often found in hardware stores), and (3) your Alivecor iPhone case as seen below (Excuse the DEMO sticker - I was a beta-tester for the iPhone 4S case):
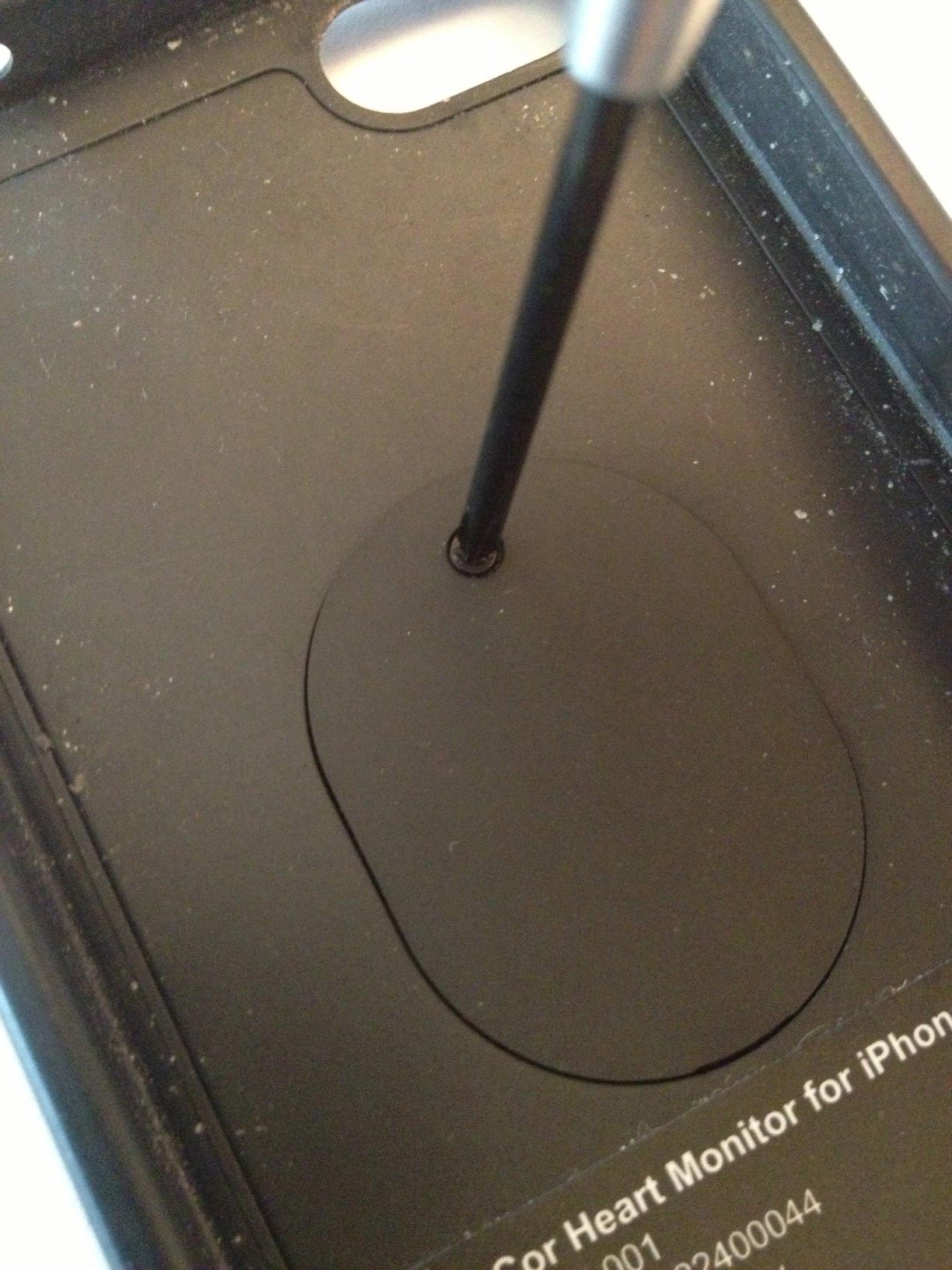
Next, unscrew the plate on the inner side of the iPhone case as shown:

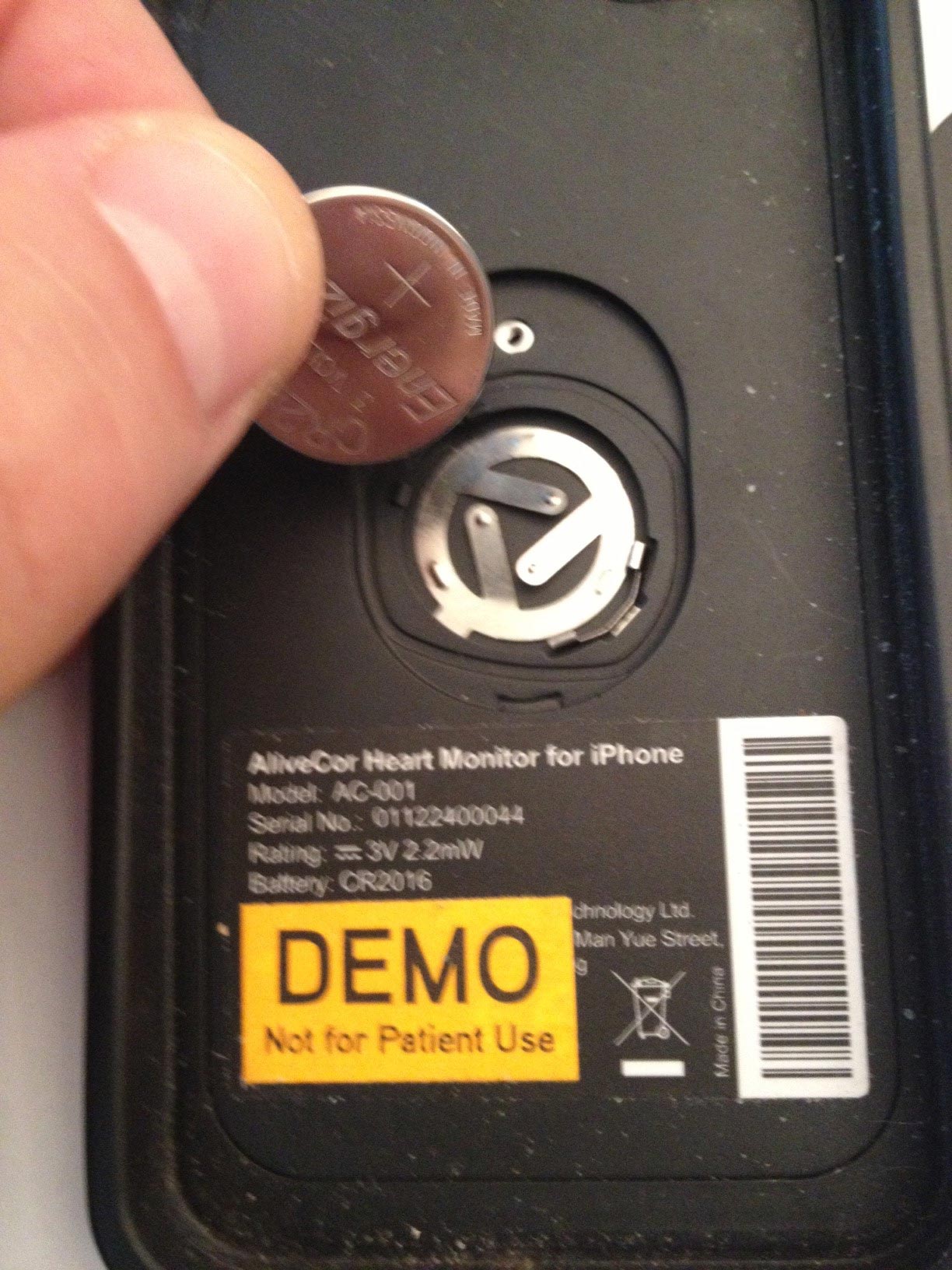
This will reveal the old battery below the case cover. Set the cover aside using care not to lose the tiny screw that attached the cover to the case:

In the upper left corner of the battery holder is a small recess where the battery can be carefully pryed from the holder as shown:

Carefully remove the battery to reveal the contacts below it:

Take the new replacement battery and remove the adhesive backing on the battery before installing it back in the holder:

Be sure to place the replacement battery in the holder with the writing side up, using care to first place it beneath the metallic retaining clips in the lower right side of the battery holder:

Once seated back in the case, screw back on the cover:

Then just place the cover on your iPhone and you'll be good for another 100-130 ECG tracings or so!
-Wes
First, assemble all of the items needed: (1) a new 3-volt model 2016 battery (I got mine from Walgreens), (2) a tiny Phillips screw driver (used to repair eye-glasses and often found in hardware stores), and (3) your Alivecor iPhone case as seen below (Excuse the DEMO sticker - I was a beta-tester for the iPhone 4S case):
 |
| Click to enlarge |
This will reveal the old battery below the case cover. Set the cover aside using care not to lose the tiny screw that attached the cover to the case:

In the upper left corner of the battery holder is a small recess where the battery can be carefully pryed from the holder as shown:

Carefully remove the battery to reveal the contacts below it:
Take the new replacement battery and remove the adhesive backing on the battery before installing it back in the holder:

Be sure to place the replacement battery in the holder with the writing side up, using care to first place it beneath the metallic retaining clips in the lower right side of the battery holder:
Once seated back in the case, screw back on the cover:
Then just place the cover on your iPhone and you'll be good for another 100-130 ECG tracings or so!
-Wes
Sunday, February 24, 2013
How Big Data's Fueling Complacency
"What's the most important finding on this chest x-ray?"
There he was, standing before 5 ICU residents, each peering at a chest film on displayed on the over-sized computer screen.
"Um, the pleural effusion?" whimpered a third-year resident.
"No!" barked the attending.
The others, standing dumbfounded in front of the computer display, searching for another finding but finding none, stood silently.
"Come on, folks! Look!"
And try as they may, no one saw it.
"The name, folks, the name!" the attending said impatiently.
And there it was, a tiny reminder of whose x-ray it was, quietly lurking in tiny print in the upper right corner of the computer screen, unmagnified.
But wait, the name was correct. What the heck was he talking about?
Closer inspection showed another critical piece of information, totally lost on almost everyone standing there: the date of birth of the patient. It was not the same as the patient being discussed. They were looking at the wrong patient's chest x-ray. Never mind that their patient had a chest tube placed on the opposite side that wasn't shown on the displayed chest x-ray. Yet they were already trying to make decisions for care.
***
I recently taught an EKG reading class and had a similar experience to the one above. Since July, I've been teaching the basics of EKG reading at least once a month: rate, rhythm, axis, intervals - you know the drill, right?
But I (once again) asked about the axis of an EKG tracing we were discussing some six months later. A room full of at least twenty residents sat quietly. No one answered.
I kept my composure. I prodded them gently, hoping to hear an answer yet none came. Were they on call? Distracted by their cell phones or pending work? Am I THAT boring?
Still nothing.
So I reviewed how we determine EKG axis, and quickly, a few remembered the concept and gratefully, responded correctly.
But these experiences got me thinking about the effects Big Data is having on our residents today and its tendency to build complacency. Why learn something if you're always spoon-fed it right?
Admittedly, our medical data explosion has prevented us from knowing everything there is to know about anatomy, physiology, pathology, treatment options and the like. There is a role for access to Big Data.
But increasingly the data we feed our residents and medical schools is nothing but printed characters: x-ray reports, EKG interpretations, study results like "ejection fraction:" all limited to the 256 ASCII character set. Residents no longer feel the need to look at the raw image and formulate their own opinion - they'll just look at the printed report. They expect the data to be fed to them in printed format. They expect the reading to be correct. In a way, they're growing up expecting to be spoon fed just the black-and-white answers rather than the brilliant data provided by pictures. Just "google it."
Never mind the computer says "atrial fibrillation" because the original EKG contains noise.
Such an "Big Data-entitled" approach to health care is extremely dangerous, especially if the data upon which decisions are based, are wrong. Residents should never forget two things my father always told me:
"Garbage in, garbage out" and "expect what you inspect."
-Wes
There he was, standing before 5 ICU residents, each peering at a chest film on displayed on the over-sized computer screen.
"Um, the pleural effusion?" whimpered a third-year resident.
"No!" barked the attending.
The others, standing dumbfounded in front of the computer display, searching for another finding but finding none, stood silently.
"Come on, folks! Look!"
And try as they may, no one saw it.
"The name, folks, the name!" the attending said impatiently.
And there it was, a tiny reminder of whose x-ray it was, quietly lurking in tiny print in the upper right corner of the computer screen, unmagnified.
But wait, the name was correct. What the heck was he talking about?
Closer inspection showed another critical piece of information, totally lost on almost everyone standing there: the date of birth of the patient. It was not the same as the patient being discussed. They were looking at the wrong patient's chest x-ray. Never mind that their patient had a chest tube placed on the opposite side that wasn't shown on the displayed chest x-ray. Yet they were already trying to make decisions for care.
***
I recently taught an EKG reading class and had a similar experience to the one above. Since July, I've been teaching the basics of EKG reading at least once a month: rate, rhythm, axis, intervals - you know the drill, right?
But I (once again) asked about the axis of an EKG tracing we were discussing some six months later. A room full of at least twenty residents sat quietly. No one answered.
I kept my composure. I prodded them gently, hoping to hear an answer yet none came. Were they on call? Distracted by their cell phones or pending work? Am I THAT boring?
Still nothing.
So I reviewed how we determine EKG axis, and quickly, a few remembered the concept and gratefully, responded correctly.
But these experiences got me thinking about the effects Big Data is having on our residents today and its tendency to build complacency. Why learn something if you're always spoon-fed it right?
Admittedly, our medical data explosion has prevented us from knowing everything there is to know about anatomy, physiology, pathology, treatment options and the like. There is a role for access to Big Data.
But increasingly the data we feed our residents and medical schools is nothing but printed characters: x-ray reports, EKG interpretations, study results like "ejection fraction:" all limited to the 256 ASCII character set. Residents no longer feel the need to look at the raw image and formulate their own opinion - they'll just look at the printed report. They expect the data to be fed to them in printed format. They expect the reading to be correct. In a way, they're growing up expecting to be spoon fed just the black-and-white answers rather than the brilliant data provided by pictures. Just "google it."
Never mind the computer says "atrial fibrillation" because the original EKG contains noise.
Such an "Big Data-entitled" approach to health care is extremely dangerous, especially if the data upon which decisions are based, are wrong. Residents should never forget two things my father always told me:
"Garbage in, garbage out" and "expect what you inspect."
-Wes
Wednesday, February 13, 2013
When Patients Can Obtain Their Own EKG

While this sounds nice, how, exactly, does one become a "prescribed patient?" Once a doctor "prescribes" such a device, what are his responsibilities? Does this obligate the physician to 24/7/365 availability for EKG interpretations? How are HIPAA-compliant tracings sent between doctor and patient? How are the tracings and medical care documented in the (electronic) medical record? What are the legal risks to the doctor if the patient transmits OTHER patient's EKG's to OTHER people, non-securely?
At this point, no one knows. We are entering into new, uncharted medicolegal territory.
But the legal risks for prescribing a device to a patient are, sadly, probably real, especially since the FDA has now officially sanctioned this little iPhone case as a real, "live" medical device. But I must say, I am not a legal expert in this area and would defer to others with more legal expertise to comment on these thorny issues.
This issue came up because a patient saw the device demonstrated in my office and wanted me to prescribe it for them. So I sent AliveCor's Dr. Dave Alpert a tweet and later received this "how to" e-mail response from their support team:
Dear Dr. Fisher,It is clear AliveCor wants to provide the device and its app, but will not be responsible for the interpretation of EKG's. That is up to the doctor and their patient how to manage the clinical expectations of this technology. While some patients could probably perform EKG interpretation basics, I would guess most don't really understand what that wavy line means. Hence, this is where a discussion should be held with a patient BEFORE prescribing this device and the expectations defined before its use.
Thank you for your interest in the AliveCor Heart Monitor. I'm writing in response to your tweet to Dr. Dave (Alpert) yesterday. Below are the instructions; in addition these instructions can be found at www.alivecor.com (click on the “Buy Now” link in the upper right corner).
To obtain a monitor for your patients, please follow these steps:
1. Write a prescription for the “AliveCor Heart Monitor for iPhone 4/4S”
2. Ask your patient to go to here and submit the following:
a. The prescriber’s information - your name, address, phone number, license number and license state or NPI (National Provider Identifier)
b. A copy of the prescription (attach a scanned copy or photo)
3. Go to www.alivecor.com and click on the “Buy Now” link in the upper right to purchase the monitor
a. In the “NPI/State Medical Lic #” enter “Prescription”
NOTE: The patient's credit card will be charged once they place their order, however we can’t process their order unless we have received their prescription.
Please know that at this time AliveCor does not provide any ECG interpretation, diagnosis or analysis of the data obtained with the monitor. Patients will be instructed to contact you, their physician, regarding any questions they may have regarding their recordings.
Please let me know if you have any questions.
Regards,
For me, I am happy to provide interpretations free of charge when needed as long as it is convenient and non-disruptive to my clinical responsibilities and personal life. There are only so many hours of the day and since I must value that time, cannot bill for this EKG-reading service, and have no quality control over the caliber of the recordings submitted, I consider my interpretations of tracings sent to me to be provided to the patient as a "good Samaritan" in every legal sense of the term. Patients who have clinically worrisome symptoms and need emergent analysis of their heart rhythm should seek help in an emergency department or call 911 and not expect a doctor to provide an immediate interpretation of their tracing, unless such an arrangement is defined clearly between doctor and patient before issuing the device. Expecting a doctor to make urgent clinical decisions based on this single-lead EKG app is of limited utility, in many (and maybe most) instances in my view, so patients should look at this device as a convenient adjunct to more conventional medical care. While it might come one day, the AliveCor iPhone EKG has simply has never been tested for emergency use as of the time of this writing.
So I may do a test run to see how it goes on a test basis but I can already see some legal concerns for doctors who prescribe this device. Until a clear interpretation workflow is established that can provide comprehensive coverage of interpretations paired with a well-defined and easy-to-use interface with a medical record system, patients should understand doctors' possible hesitation to prescribing this device to a multitude of patients for personal use.
-Wes
Wednesday, December 05, 2012
An Inside Look at AliveCor's iPhone ECG Case
|
| The back of my demo AliveCor ECG iPhone 4s Case |
 |
| AliveCor ECG Setup Screen (beta) |
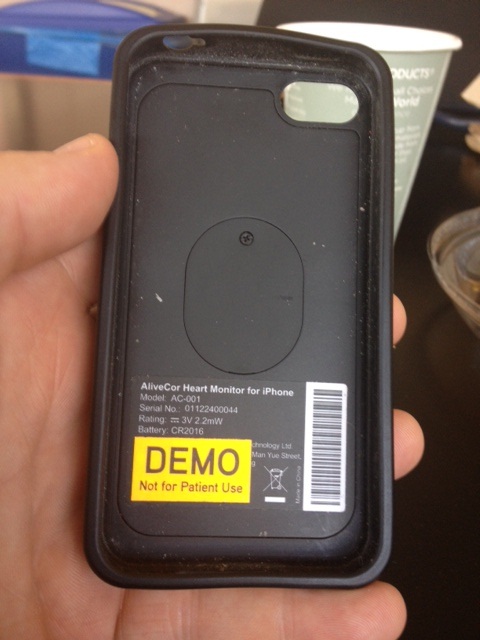 |
| Inside of My Demo AliveCor iPhone Case Note: no wires. |
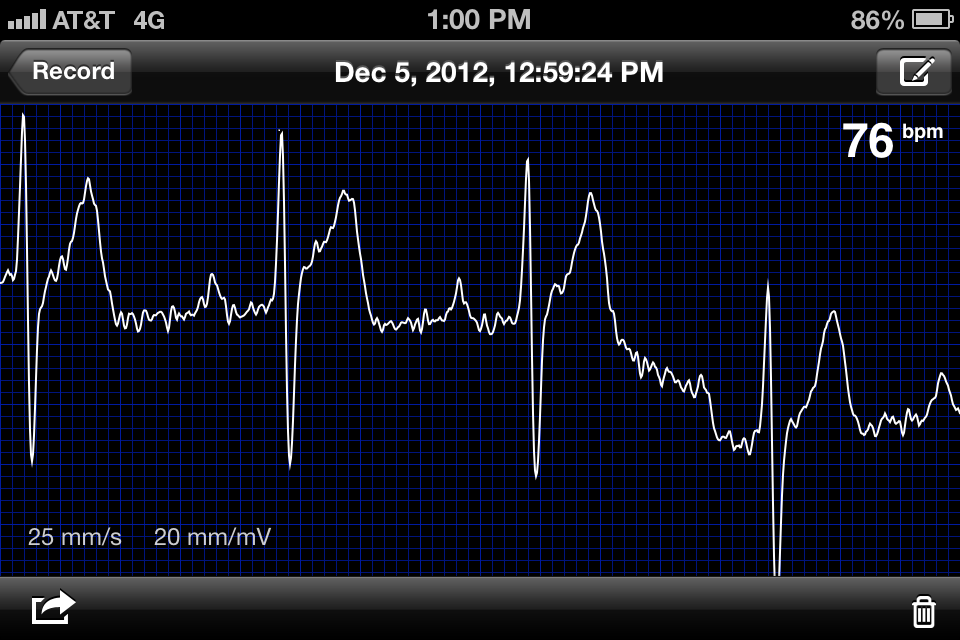 |
| My unretouched ECG recorded with my hands today (yep 1st degree AV block!) |
Lead I of the standard EKG was recorded with the left and right hand holding the device with the left and right hand fingertips touching the electrodes on the back of the case. It was important to hold the device with the iPhone's round button to the right to assure the device did not record an inverted lead I.
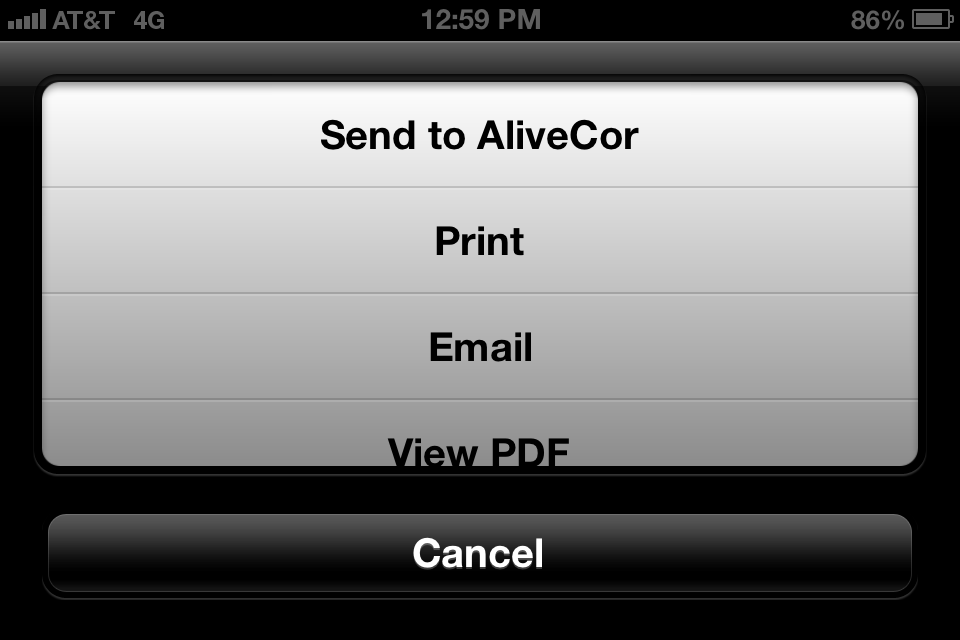 |
| Options for sending tracings (beta) |
Physician Reactions
Without exception, every physician I showed this device recognized this device as a compliment to the doctor's stethoscope. It was a uniform hit as they gazed in amazement at the device's ability to record their real-time ECG. I found this device was capable of instantly differentiating the irregular rhythm of atrial fibrillation from the irregular rhythm caused by premature atrial or premature ventricular beats or even atrial flutter with variable AV conduction. Some care was required to get noise-free tracings or to obtain the appropriate EKG vector on the chest with which to identify lower-amplitude atrial arrhythmias. But most limb leads can be replicated by the device (hold the R electrode with the hand and apply the left electrode to the knee to see lead II, for instance), or angle the leads in different directions on the patient's chest to obtain a new QRS vector. (Obviously, the angle the electrodes were placed on the chest to acquire a particular limb lead requires some rudimentary knowledge of ECG basics.)
Patient Reactions
Perhaps the most interesting aspect of this device is what happened when it is placed in the hands of patients and friends unfamiliar with ECG tracings. Their first reaction as they sit transfixed at their own ECG tracing dancing across the screen is "Cool! .... But what does it MEAN?" Then comes "Am I okay?" And then of course when tracings are compared between friends: "Why is my heart rate so much faster/slower than his/hers?" Or you might hear: "Man, I'm out of shape!" And if the device occasionally had difficulty calculating the heart rate from a noisy tracing, three little dashes would appear instead, leading the person to ask, "Does this mean I'm dead?" Any one of these reactions could came from generally healthy people who have never had a major medical problem.
What was more interesting to me was the nuanced reaction I noticed from patients who had had a complex medical history before but were seeing this device outside a medical facility for the first time. When they encountered this device in a social setting, it was common that these patients refused to have their tracing performed "for fun" for fear they might be sent packing to the nearest medical establishment. IT became immediately clear that discretion should be exercised if the device is to be passed about at cocktail parties. (Yes, doctor, not everyone wants to see your cool gizmo.) Hence, it appears that deploying this device on the general public has some challenges ahead, but I suspect it will come: gradually at first, then more generally. It is clear that this really does take an understanding of ECGs to use effectively, so doctors (or techs) familiar with ECGs will have to be involved. Liability and responsibility for reading remains a thorny issue one the device is released to the public. I suspect these are relatively easy issues to resolve for AliveCor going forward.
Still, for doctors and medically-savvy patients, this device is a game-changer. The number of ECG tracings obtained in clinics will probably diminish one day as this device enjoys a wider distribution amongst physicians since it doesn't require a special technician or equipment to obtain much of the information doctors need to manage their arrhythmia patients. But caution with this single lead ECG device should be maintained, too. Because multiple ECG leads are not collected simultaneously, the device could miss the subtle findings of a heart attack in locations remote from the there the single tracing is collected by the device. Still, for routine rhythm analysis, this device has huge potential for time-savings, practical rhythm interpretation, and maybe even the potential to provide for considerable technical health care cost savings.
-Wes
PS: I have no commercial interest in AliveCor (darn it).
The AliveCor iPhone ECG Case website
Wednesday, September 12, 2012
The Irony of Why EKG Class Was Cancelled
I look forward to teaching our housestaff the basics of EKGs each year. Moments where I can leap from worker-bee clinician to the quiet confines of a lecture hall is rejuvenating. Seeing eyes widen as they grasp basic insights to the wealth of information contained in biologic signals even more so. So I carve some time at the beginning of each year with the chief residents to commit to this endeavor far in advance.
This year, I arrived a little early for my lecture with a stack of EKG’s, ready to bring down the screen, load the Powerpoint presentation, and collect my thoughts. Unlike most lecture days, the lecture hall door was closed when I arrived. I quietly cracked the door and peered in: there, in their new, carefully pressed white coats, was a sea of residents. I was elated, expecting that attendance at this lecture would be especially high since I already had a captive audience.
So I closed the door quietly and paced in the halls waiting for the lecture before mine to conclude.
The nearby secretaries noticed me and politely said hello and I, in turn, smiled and acknowledged their greeting. I grabbed a quick cup of coffee from the coffee pot and sipped the nectar in my quiet moment of reverie before class.
But something was askew. The secretaries seemed a bit uncomfortable.
“Doctor Fisher? Oh, I’m so sorry, the lecture hall is being used today for our annual Transitional Residency program review. Let me see if I can find another lecture hall for you.”
She logged on her computer and scanned the available spaces. She clicked and clicked and clicked.
“Well, there is a room on the fifth floor…. Um, maybe not. I see there’s only 15 chairs in there… Let me keep trying.”
“Thanks so much,” I said.
About this time, the doors from my previously-arranged lecture hall opened and a sea of smiling residents poured out from the room. Some headed to the washroom, others checking their beepers. Others appeared to be heading back to the wards. I was puzzled.
I glanced in the lecture hall to see several well-dressed women sitting before a pile of 3-ring binders full of papers, one of which was opened. They chatted with each other, occasionally giggling, but very professionally so. There behind them was a tray of uneaten donuts and other treats and a coffee dispenser neatly arranged on a tray behind them. Boy, those looked tasty! I smiled as I thought to myself: “No wonder their attendance was so good.”
A few moments later, one of the Chief Residents came to me with his tail between his legs and apologized profusely. “I’m SO sorry, Dr. Fisher, we forgot to call you about this change of schedule!”
The poor guy. Sent with full flak jacket in place to take the hit. But I knew exactly how he felt as he tried to keep all the various clinical and administrative scheduling balls in the air.
“No problem,” I said. “We’ll do this another time.”
But as I walked back to my office, I couldn’t help but wonder what we’re creating as housestaff are corralled before bureaucrats who ask them how their residency is going while their own residency's EKG training was silently sabotaged.
It’s kind of like those uneaten donuts behind those well-dressed ladies: food for thought.
-Wes
This year, I arrived a little early for my lecture with a stack of EKG’s, ready to bring down the screen, load the Powerpoint presentation, and collect my thoughts. Unlike most lecture days, the lecture hall door was closed when I arrived. I quietly cracked the door and peered in: there, in their new, carefully pressed white coats, was a sea of residents. I was elated, expecting that attendance at this lecture would be especially high since I already had a captive audience.
So I closed the door quietly and paced in the halls waiting for the lecture before mine to conclude.
The nearby secretaries noticed me and politely said hello and I, in turn, smiled and acknowledged their greeting. I grabbed a quick cup of coffee from the coffee pot and sipped the nectar in my quiet moment of reverie before class.
But something was askew. The secretaries seemed a bit uncomfortable.
“Doctor Fisher? Oh, I’m so sorry, the lecture hall is being used today for our annual Transitional Residency program review. Let me see if I can find another lecture hall for you.”
She logged on her computer and scanned the available spaces. She clicked and clicked and clicked.
“Well, there is a room on the fifth floor…. Um, maybe not. I see there’s only 15 chairs in there… Let me keep trying.”
“Thanks so much,” I said.
About this time, the doors from my previously-arranged lecture hall opened and a sea of smiling residents poured out from the room. Some headed to the washroom, others checking their beepers. Others appeared to be heading back to the wards. I was puzzled.
I glanced in the lecture hall to see several well-dressed women sitting before a pile of 3-ring binders full of papers, one of which was opened. They chatted with each other, occasionally giggling, but very professionally so. There behind them was a tray of uneaten donuts and other treats and a coffee dispenser neatly arranged on a tray behind them. Boy, those looked tasty! I smiled as I thought to myself: “No wonder their attendance was so good.”
A few moments later, one of the Chief Residents came to me with his tail between his legs and apologized profusely. “I’m SO sorry, Dr. Fisher, we forgot to call you about this change of schedule!”
The poor guy. Sent with full flak jacket in place to take the hit. But I knew exactly how he felt as he tried to keep all the various clinical and administrative scheduling balls in the air.
“No problem,” I said. “We’ll do this another time.”
But as I walked back to my office, I couldn’t help but wonder what we’re creating as housestaff are corralled before bureaucrats who ask them how their residency is going while their own residency's EKG training was silently sabotaged.
It’s kind of like those uneaten donuts behind those well-dressed ladies: food for thought.
-Wes
Saturday, September 08, 2012
EKG Du Jour #27: Caught in the Act
I've been looking at EKG's for over 20 years and I'm not sure I've ever seen this captured on a 12-lead electrocardiogam outside the EP laboratory.
The patient was admitted with some vague chest discomfort. The initial EKG and troponins were normal, but they decided to admit the patient anyway for observation. Once on the ward after being given some heparin and aspirin, the patient was feeling perfectly fine - wanted to go home - but the second set of troponins returned positive. The first year resident decided to order a second EKG.
The EKG technician came dutifully, performed the EKG, and before she knew it, all hell broke loose:
Fortunately, the patient did well after a quite bit of work in the cath lab.
Remember this story. It might just save a life.
-Wes
The patient was admitted with some vague chest discomfort. The initial EKG and troponins were normal, but they decided to admit the patient anyway for observation. Once on the ward after being given some heparin and aspirin, the patient was feeling perfectly fine - wanted to go home - but the second set of troponins returned positive. The first year resident decided to order a second EKG.
The EKG technician came dutifully, performed the EKG, and before she knew it, all hell broke loose:
 |
| Click image to enlarge |
Fortunately, the patient did well after a quite bit of work in the cath lab.
Remember this story. It might just save a life.
-Wes
Tuesday, May 01, 2012
The Dark Side of EKG Screening in Athletes
They sat nervously with their son in the doctor's office, wondering why they were there. John was, after all, the picture of health and had just received a scholarship to Stanford University to play soccer. His mother and father had been to every soccer match through his formative years, enduring the travel schedule with its weekends away from home, long hours, horrible weather. John was staring at his iPhone, his mother clutching a Kleenex. John's father stared out the window. It was raining.
The door opened.
"Hello, I'm Dr. Kiljoy. They asked me to see your son about a finding on his EKG."
"Hello," they said back.
"As you know, we've been looking into EKG's in athletes because we have suspected for some time that an EKG will help us better detect students who might be at risk for sudden cardiac death while participating in sports. You know, even if we can prevent one death in these young people, it would be worth it. None of us want a young person to die. That New York Times article yesterday... dang... with that crying family and all right there at the top... poor boy collapsed, people had no clue what happened at first, people thought he overheated, then waited... only later did they find that AED. Then it didn't work 'cause the battery was dead. So sad! We really are trying to prevent that from ever happening. Seriously. Sad as hell. And to think we could have caught this if that teenager had just had an EKG..."
"Yes, of course!" said John's mother. "I'm SO glad you did this! We'll be so reassured to know that John's going to be okay. "
A pause filled the room...
"He IS going to be okay, isn't he?" she asked.
"Well, Mrs Smith, we're not sure, we have to run some other tests. You see he had a slight elevation to his ST segments in these leads here, see? Then look at his heart rate, it's so slow! And that voltage here, it's more than we usually see... It's probably okay, but I'm going to order an echo to look at his chamber sizes."
"Okay..."
"And a then I'm going to have one of our EP people see him to make sure he doesn't have a congenital ion channel disorder..."
"A what?"
"A channelopathy - a genetic defect of some ion channels in his heart - the most common form is called Brudaga Syndrome..."
"How do you spell that?" She waited with pen and paper to jot it down...
"B-R-U-G-A-D-A. Look, he's probably okay, be we want to be absolutely sure, especially with that ST segment elevation in those leads... We'll also check a stress test to make sure his heart rate comes up appropriately with exercise and that there aren't any funny EKG changes with exercise that might suggest an anomalous coronary artery - I've seen three people die like a dog with that one!"
"How often does that happen?" she asked.
"Well, it's pretty uncommon, but if it's there, sometimes we have to do open heart surgery to reimplant it so that it won't get pinched between the pulmonary artery and aorta when he exercises."
"But he's never had a problem! And no one has ever died suddenly in our family - ever!"
"Mrs. Smith. Remember why we're doing this: John's safety. This is all about John's safety."
"And if you find something in all these tests, then what?"
"Well, he wouldn't be able to play soccer."
John's eyes suddenly lift from his cell phone. "What did you say?" he asked.
"You won't be able to play soccer," Dr. Kiljoy repeated.
"Mom, what the f#$*!? If I don't play soccer, I don't go to Stanford. If I don't go to Stanford, I'll never play soccer again! Are you serious?"
The father, sensing his son's concern, returns to the room from his window transcendental meditation.
"Son, let's just get the tests. Your mother's concerned."
"Mom's concerned? What the hell do you mean 'Mom's concerned?' What about me? I never wanted to get this frickin' EKG anyway! Look, I'm FINE. I never so much as farted wrong. We have no family history of heart disease. I've never felt my heart race, I've never passed out, I'm faster than everyone else on my team and we just won the State Championship! How's THAT for a stress test? I've worked my ass off for YEARS to get this scholarship. And now, just because of this EKG with bullshit findings that don't pertain to kids my age they're going to do a million tests just to be sure? Seriously? Honestly Dad, you gotta be kidding me... How much is all this gonna cost, huh? And maybe I'll lose my scholarship, too? How much is THAT worth?"
"John, honey, it's for your safety," his mother whispers, tears streaming down her cheeks. "We love you so. We just don't want anything bad to happen to you...."
"Your Mom's right, John. We just want to be sure... really....", Dr. Kiljoy continued.
John looked up at Dr. Kiljoy, and said slowly, painfully, with tears in his eyes:
"Doctor, f*&% you."
-Wes
P.S.: For more, please see Dr. John M's take on the New York Times's abysmal reporting on this issue.
The door opened.
"Hello, I'm Dr. Kiljoy. They asked me to see your son about a finding on his EKG."
"Hello," they said back.
"As you know, we've been looking into EKG's in athletes because we have suspected for some time that an EKG will help us better detect students who might be at risk for sudden cardiac death while participating in sports. You know, even if we can prevent one death in these young people, it would be worth it. None of us want a young person to die. That New York Times article yesterday... dang... with that crying family and all right there at the top... poor boy collapsed, people had no clue what happened at first, people thought he overheated, then waited... only later did they find that AED. Then it didn't work 'cause the battery was dead. So sad! We really are trying to prevent that from ever happening. Seriously. Sad as hell. And to think we could have caught this if that teenager had just had an EKG..."
"Yes, of course!" said John's mother. "I'm SO glad you did this! We'll be so reassured to know that John's going to be okay. "
A pause filled the room...
"He IS going to be okay, isn't he?" she asked.
"Well, Mrs Smith, we're not sure, we have to run some other tests. You see he had a slight elevation to his ST segments in these leads here, see? Then look at his heart rate, it's so slow! And that voltage here, it's more than we usually see... It's probably okay, but I'm going to order an echo to look at his chamber sizes."
"Okay..."
"And a then I'm going to have one of our EP people see him to make sure he doesn't have a congenital ion channel disorder..."
"A what?"
"A channelopathy - a genetic defect of some ion channels in his heart - the most common form is called Brudaga Syndrome..."
"How do you spell that?" She waited with pen and paper to jot it down...
"B-R-U-G-A-D-A. Look, he's probably okay, be we want to be absolutely sure, especially with that ST segment elevation in those leads... We'll also check a stress test to make sure his heart rate comes up appropriately with exercise and that there aren't any funny EKG changes with exercise that might suggest an anomalous coronary artery - I've seen three people die like a dog with that one!"
"How often does that happen?" she asked.
"Well, it's pretty uncommon, but if it's there, sometimes we have to do open heart surgery to reimplant it so that it won't get pinched between the pulmonary artery and aorta when he exercises."
"But he's never had a problem! And no one has ever died suddenly in our family - ever!"
"Mrs. Smith. Remember why we're doing this: John's safety. This is all about John's safety."
"And if you find something in all these tests, then what?"
"Well, he wouldn't be able to play soccer."
John's eyes suddenly lift from his cell phone. "What did you say?" he asked.
"You won't be able to play soccer," Dr. Kiljoy repeated.
"Mom, what the f#$*!? If I don't play soccer, I don't go to Stanford. If I don't go to Stanford, I'll never play soccer again! Are you serious?"
The father, sensing his son's concern, returns to the room from his window transcendental meditation.
"Son, let's just get the tests. Your mother's concerned."
"Mom's concerned? What the hell do you mean 'Mom's concerned?' What about me? I never wanted to get this frickin' EKG anyway! Look, I'm FINE. I never so much as farted wrong. We have no family history of heart disease. I've never felt my heart race, I've never passed out, I'm faster than everyone else on my team and we just won the State Championship! How's THAT for a stress test? I've worked my ass off for YEARS to get this scholarship. And now, just because of this EKG with bullshit findings that don't pertain to kids my age they're going to do a million tests just to be sure? Seriously? Honestly Dad, you gotta be kidding me... How much is all this gonna cost, huh? And maybe I'll lose my scholarship, too? How much is THAT worth?"
"John, honey, it's for your safety," his mother whispers, tears streaming down her cheeks. "We love you so. We just don't want anything bad to happen to you...."
"Your Mom's right, John. We just want to be sure... really....", Dr. Kiljoy continued.
John looked up at Dr. Kiljoy, and said slowly, painfully, with tears in his eyes:
"Doctor, f*&% you."
-Wes
P.S.: For more, please see Dr. John M's take on the New York Times's abysmal reporting on this issue.
Wednesday, February 01, 2012
EKG Du Jour #25 - The Exercise Enthusiast - Explained
Sorry about the delay, but unlike most of the EKG Du Jour series of EKG's, I elected to make a separate post to explain the interesting tracings that first appeared here.
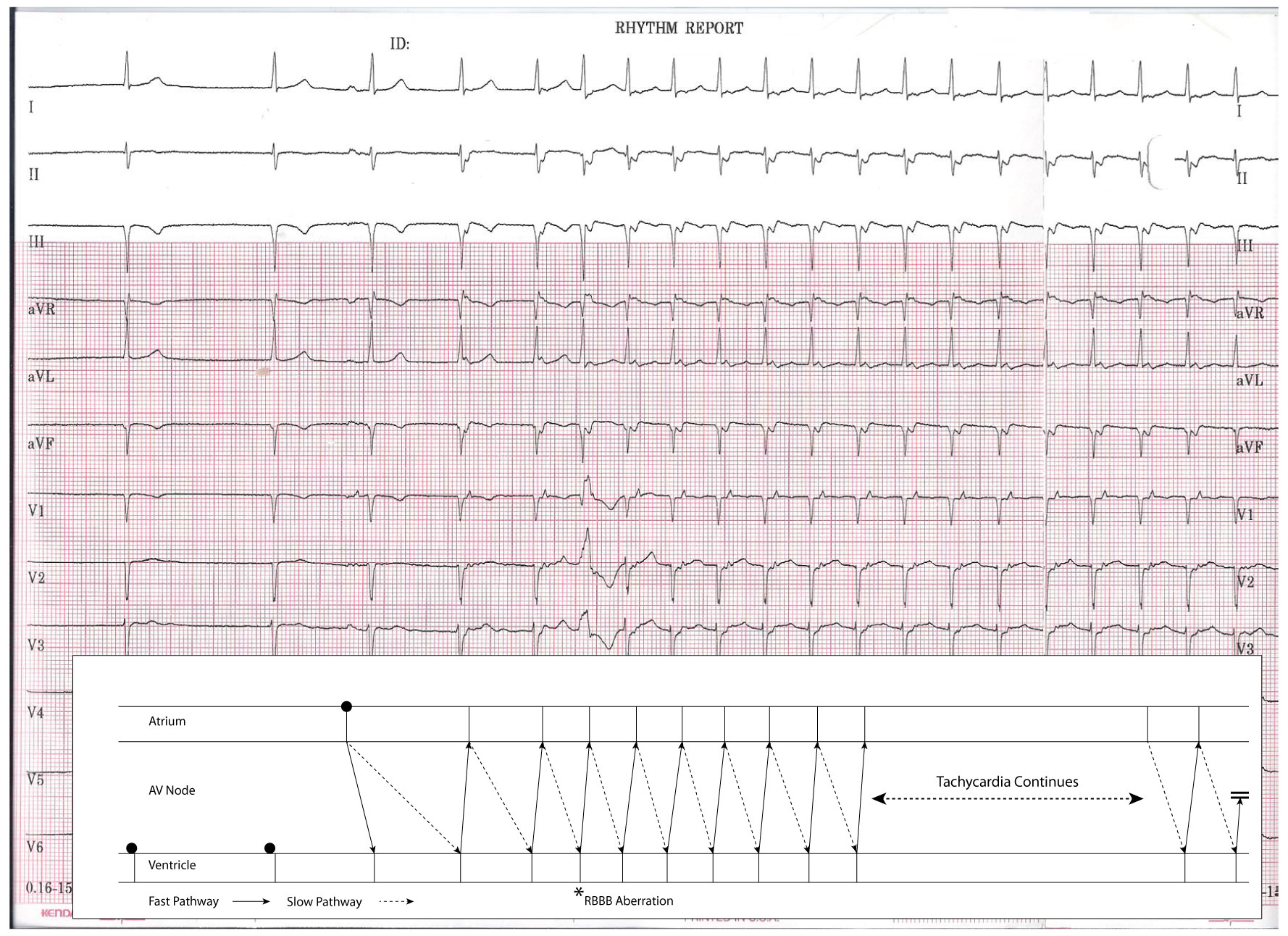
As a refresher, the original 12-lead rhythm strip obtained on this healthy, asymptomatic individual looked like this when he presented for evaluation of two near syncopal spells:

The third beat is where things get interesting. Here, a P wave is clearly seen that conducts to the ventricle with a normal PR interval. What is unsual, however, is the finding that the fourth beat (that appears to be junctional) occurs earlier than one would expect than a junctional escape beat to occur (based on the earlier two junctional beats). In effect, this fourth beat appears "pulled in" earlier to the preceding beat, but also has a clearly visible retrogradely-conducted P wave (best seen in V1) that occurs immediately after the QRS complex. At this point, the patient is in a supraventricular tachycardia that accelerates slightly with the fifth beat occurring earlier - probably because of hemodynamic alterations that occur due to the unusual cardiac activation sequence (slightly decreased BP and increased catecholamine level).
The sixth beat is a widened QRS complex of RBBB morphology. This beat is either a PVC (less likely) or (more likely) an aberrantly-conducted supraventricular beat. This beat aberrates because of the long-short nature of the initiation of the tachycardia that finds the right bundle branch refractory while the left bundle branch conducts to the ventricle. With continued tachycardia, the right bundle branch recovers and the tachycardia continues with a narrow QRS morphology.
The very last beat of the tracing defines the end of the run of supraventricular tachycardia.
So how did the tachycardia initiate?
This is an example of a normal P wave initiating SVT due to AV nodal "double-fire." That is, a single atrial beat conducts down BOTH the fast and slow pathway of the AV node. In this case, typical AV nodal reentrant tachycardia was initiated by a single sinus beat in this gentleman.
Here is the above tracing explained using a favorite of EP's -- a ladder diagram:

-Wes
As a refresher, the original 12-lead rhythm strip obtained on this healthy, asymptomatic individual looked like this when he presented for evaluation of two near syncopal spells:
Click image to enlarge
The third beat is where things get interesting. Here, a P wave is clearly seen that conducts to the ventricle with a normal PR interval. What is unsual, however, is the finding that the fourth beat (that appears to be junctional) occurs earlier than one would expect than a junctional escape beat to occur (based on the earlier two junctional beats). In effect, this fourth beat appears "pulled in" earlier to the preceding beat, but also has a clearly visible retrogradely-conducted P wave (best seen in V1) that occurs immediately after the QRS complex. At this point, the patient is in a supraventricular tachycardia that accelerates slightly with the fifth beat occurring earlier - probably because of hemodynamic alterations that occur due to the unusual cardiac activation sequence (slightly decreased BP and increased catecholamine level).
The sixth beat is a widened QRS complex of RBBB morphology. This beat is either a PVC (less likely) or (more likely) an aberrantly-conducted supraventricular beat. This beat aberrates because of the long-short nature of the initiation of the tachycardia that finds the right bundle branch refractory while the left bundle branch conducts to the ventricle. With continued tachycardia, the right bundle branch recovers and the tachycardia continues with a narrow QRS morphology.
The very last beat of the tracing defines the end of the run of supraventricular tachycardia.
So how did the tachycardia initiate?
This is an example of a normal P wave initiating SVT due to AV nodal "double-fire." That is, a single atrial beat conducts down BOTH the fast and slow pathway of the AV node. In this case, typical AV nodal reentrant tachycardia was initiated by a single sinus beat in this gentleman.
Here is the above tracing explained using a favorite of EP's -- a ladder diagram:
Click image to enlarge
-Wes
Thursday, January 26, 2012
EKG Du Jour #25 - The Exercise Enthusiast
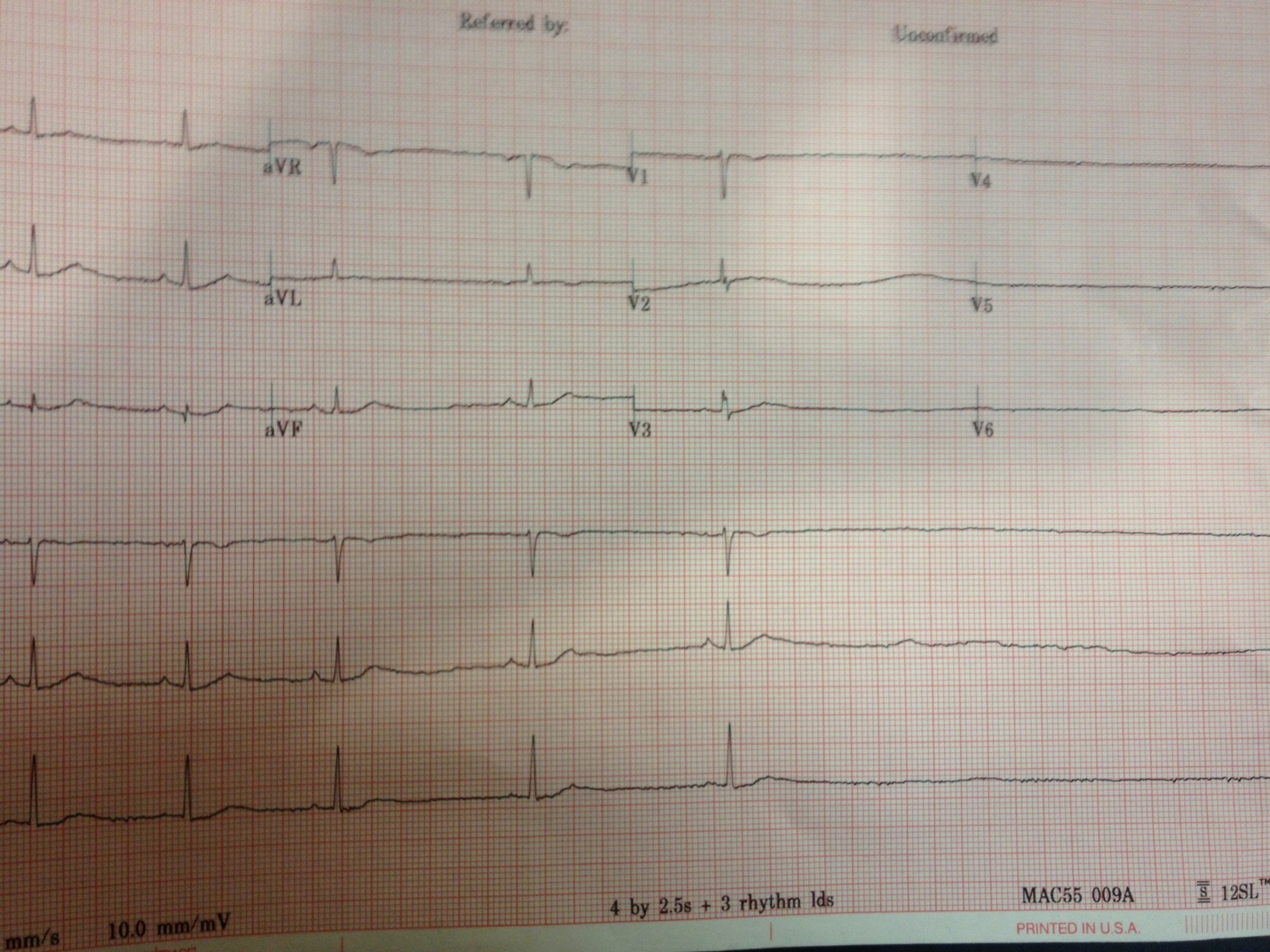
He was a 65 year-old previously healthy avid exercise enthusiast on no medications who was referred for evaluation of two near-syncopal episodes. The first episode occurred approximately 10 minutes after he stopped exercising on a treadmill. He felt he had to grab the wall to prevent himself from falling.
The second occurred after riding his bike home from the gym. Just after riding his bike home, he became very lightheaded and felt he had to sit on his front porch and nearly lost consciousness. His symptoms passed after resting for about 20 minutes.
While having his blood pressure checked, the nurse noted an irregular pulse. He felt fine and was unaware of his heart rhythm. A 12-lead rhythm strip was obtained and two representative 12-lead rhythm strips from the recording are shown below:

Any ideas? What therapy (therapies?) would you recommend?
-Wes
Strips used with patient permission.
The second occurred after riding his bike home from the gym. Just after riding his bike home, he became very lightheaded and felt he had to sit on his front porch and nearly lost consciousness. His symptoms passed after resting for about 20 minutes.
While having his blood pressure checked, the nurse noted an irregular pulse. He felt fine and was unaware of his heart rhythm. A 12-lead rhythm strip was obtained and two representative 12-lead rhythm strips from the recording are shown below:
Click image to enlarge
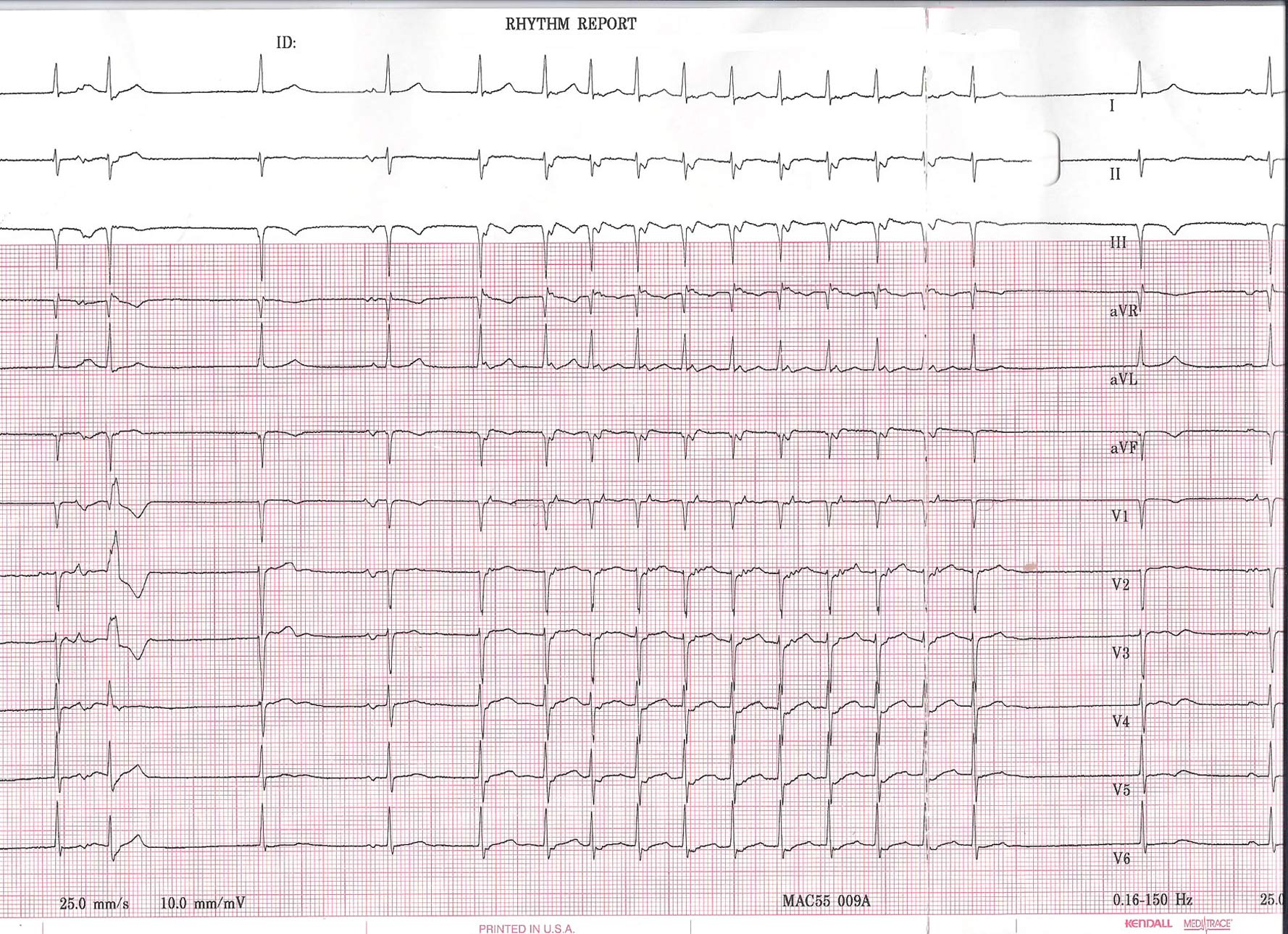
Click image to enlarge
Any ideas? What therapy (therapies?) would you recommend?
-Wes
Strips used with patient permission.
Friday, December 23, 2011
{kind=link}
{kind=link}
Sunday, November 13, 2011
When Screening Teenage Athletes for Sudden Cardiac Arrest Risk, History Matters
Before reaching for tests like EKGs to screen teen athletes, we should first ask ourselves if we've taken a careful history:
The new study consisted of Madsen and his fellow researchers sending out surveys to every pediatrician and family practice doctor in Washington State. They received a good response–surveys were returned by 72 percent of pediatricians and 56 percent of family practitioners.-Wes
The results were disheartening:
Dr. Gaurav Arora, associate director of electrophysiology at the Children’s Hospital of Pittsburgh and an assistant professor of pediatrics at the University of Pittsburgh, was surprised to see the number of physicians in the new study who said they didn’t ask every teen athlete about fainting or chest pain. He said, “Those are red flags in young athletes.”
- 28 percent of doctors surveyed failed to always ask if a teen experienced chest pain during exercise.
- 22 percent of doctors surveyed failed to always ask if the teen ever fainted without a known cause or explanation.
- 26 percent of doctors surveyed failed to always ask about early deaths in their family history.
- 67 percent failed to always ask about heart disease in their family history.
Monday, September 26, 2011
EKG Du Jour #24: Reversals
In the spirit of connecting via social media, this EKG Du Jour hails from the great Aussie blog, Life in the Fast Lane.
(There's lots to learn on many levels.)
-Wes
(There's lots to learn on many levels.)
-Wes
Thursday, September 22, 2011
EKG Du Jour #23 - With Increasing Prevalence: The Awful EKG
"Hey, Wes! I've been holding on to this EKG from a recent clinic visit with a patient of mine who presented with chest pain and thought it would make a cool EKG for your 'EKG Du Jour' series! I never could get a good tracing and I'm pretty sure my EKG machine works properly:"

For now, forget the chest pain. What's the patient's principle diagnosis?
(Trust me: you'll be seeing more of this.)
-Wes
h/t: Gary Novak, MD
Clue #1: Still uncertain? A major hint to the answer is here, so look only if you must.
Clue #2: By the way, this is not the same diagnosis as Happy's patient.
Clue #3: Here's an example of why I think we'll be seeing plenty of this.
Click image to enlarge
For now, forget the chest pain. What's the patient's principle diagnosis?
(Trust me: you'll be seeing more of this.)
-Wes
h/t: Gary Novak, MD
Clue #1: Still uncertain? A major hint to the answer is here, so look only if you must.
{kind=link}
Clue #2: By the way, this is not the same diagnosis as Happy's patient.
Clue #3: Here's an example of why I think we'll be seeing plenty of this.
Friday, August 19, 2011
EKG Du Jour #22: A Rare Classic
I offer this gem to the EKG enthusiasts out there to ponder. It's not every day we find a 12-lead EKG of this from a post-operative patient with an ischemic cardiomyopathy:


Click image to enlarge
Friday, July 01, 2011
EKG Du Jour #22: A Cool Case of Fibrillation
... sadly, the EKG is not mine, but rather was published in this week's edition of Circulation:

The story is this: an asymptomatic gentleman with an left ventricular assist device and implanted St. Jude biventricular implantable cardiac defibrilaltor had an episode of syncope and presented to the ER with this EKG.
Some interesting points are made in the discussion section of this case report published in Circulation (sorry, subscription required).
Definitely worth a read (and the link contains the answer).
-Wes
Reference: Zalkind D, Aleong R, Sauer W, Nguyen DT. 'Unusual Fibrillation in the Emergency Department After Fall." Circulation 2011;123;e641-e642.
Click image to enlarge
The story is this: an asymptomatic gentleman with an left ventricular assist device and implanted St. Jude biventricular implantable cardiac defibrilaltor had an episode of syncope and presented to the ER with this EKG.
Some interesting points are made in the discussion section of this case report published in Circulation (sorry, subscription required).
Definitely worth a read (and the link contains the answer).
-Wes
Reference: Zalkind D, Aleong R, Sauer W, Nguyen DT. 'Unusual Fibrillation in the Emergency Department After Fall." Circulation 2011;123;e641-e642.
Subscribe to:
Comments (Atom)