He was a bright medical resident in his third year of internal medicine residency - industrious, committed, a team player. He never thought of himself as special. He had studied hard and achieved much in his short 30 years. Not only was he nearing the end of his residency training in Philadelphia, he was married and had his first child about to be born July 19, 2007. Like most first-time wage earners, his $42,000-a-year resident salary didn't go too far as a result.
As a US medicine resident in his third year of training, he would soon be sitting for his Internal Medicine Board examination in the Fall, a requirement to assure his later employability. So he began the process of registration with the American Board of Internal Medicine (ABIM). He read the requirements and the ABIM
"Agreement of Conditions" statement on the their website at the time:
Before electronically signing your application, you will be asked to read the following statement:
"By this application to the American Board of Internal Medicine (the "ABIM"), I agree to be bound by the terms, conditions, and rules set forth in the ABIM's Policies and Procedures for Certification and in this Web site, as they may be amended from time to time.
I understand that by applying, I am entering into a contract with the American Board of Internal Medicine to provide certain health care operations services, including practice assessment and evaluations. The ABIM HIPAA Business Associate Agreement is a part of this contract.
I agree to indemnify, release, and hold harmless the ABIM, its employees, officers, directors, members, agents, and those furnishing information about me to the ABIM from any claims, liability, or damage by reason of any of their acts or omissions, done in good faith, in connection with this application, information furnished to the ABIM, the evaluation of my qualifications, and examinations.
I agree that the ABIM may use my examination performance, training program evaluations, self-evaluations of knowledge and practice performance, and other information for research purposes, including collaboration with other research investigators and scientific publications. In such research, the Board will not identify specific individuals, hospitals, or practice associations. All practice performance data is HIPAA compliant.
I hereby declare under penalty of perjury that the information given in my application is true and correct to the best of my knowledge and beliefs.
I agree to be legally bound by the foregoing."
This statement represented the entirety of his "informed" consent for the ABIM's "research" - and from the looks of things, he was "legally bound" to comply. On the
web page this "Copyrighted Materials" clause was included as well:
Copyrighted Materials
The Board's examinations are confidential and copyrighted under the Federal Copyright Act. Candidates agree not to copy, reproduce, reconstruct by dictation or other means, or disclose examination content in any manner. Board Self-Evaluation Process (SEP) modules are also copyrighted works. Candidates agree not to copy, reproduce, or make any adaptations of the modules in any manner; or to assist someone else in the infringement of this or any Board-copyrighted work.
Professionally and financially unable to do otherwise, he completed his application and paid his $1,135 registration fee for the examination.
A short time later, he turned to his program director to inquire which board review course he should attend. He was recommended to attend the "Arora Board Review" course led by Dr. Rajender Arora MD. Others had gone there and given it good reviews. His Pennsylvania residency program thought highly enough of the Accreditation Council of Graduate Medical Education (ACGME) sanctioned course that they paid his $1000 registration fee. He decided to attend the board review course offered in June 2007 just before his scheduled board examination in August 2007.
The Board Review Course
Five hundred economically vulnerable residents were in attendance at the Arora Board Review course in June 2007. The young doctor thought the course was taught well and helped him gain confidence for the exam questions he might encounter. Dr. Arora was a dynamic teacher and the examples and commentary he provided were helpful at teasing out the critical concepts for the examination. At the end of the course, it was mentioned that if he'd like, he could help "pay-it-forward" to his fellow colleagues by sending Dr. Arora information about the topics and questions he could recall that he encountered on his Board examination.
He studied hard for his examination for the next several months, rising early and staying up late and foregoing other social obligations. He reviewed his texts, journal articles, and board review materials. Then the day came for his examination.
He arrived at the test center, checked in, had his biometric palm scan recorded, deposited his wallet, car keys and mobile phone in a locker, was later searched, and finally admitted into the PearsonVue examination computer room. There beside him were others, pounding on their keyboards taking examinations for other trades. He sat and got comfortable. On his computer screen was a big ABIM logo with his name below and a set of instructions. Just before the timed test began, he read a document that threatened him if he shared content of the test. He had the choice: either click "I Decline" and be escorted out of the examination center and thereby waste his test preparation and potentially sacrifice his career as a physician or click the "I Accept" button to start his examination. He accepted and took his test, yet never received a copy of the agreement that he had just electronically "signed."
He thought he did well on his certifying examination. He remembered the general concepts of the questions and while he couldn't remember all of the questions and distractors, he was eager to share what he remembered of the test with the person who helped him prepare, Dr. Arora. After all, others likely did the same for him. He decided to communicate with Dr. Arora via e-mail to thank him for his help and share with him what he could recall as a way to "pay it forward" to others as requested.
Time passed. In late October, 2007 he received
notification that he had passed his boards and felt relieved that he had at least secured himself the potential for gainful employment as a "Board certified" internal medicine physician. He had no intention of repeating that ordeal, at least not in the immediate future. As life would have it, his medical passion had evolved to physical medicine and rehabilitation. His second child was born November 10, 2009 and because residency slots were tough to obtain, he moonlighted to bridge the gap before his second residency in his chosen field began.
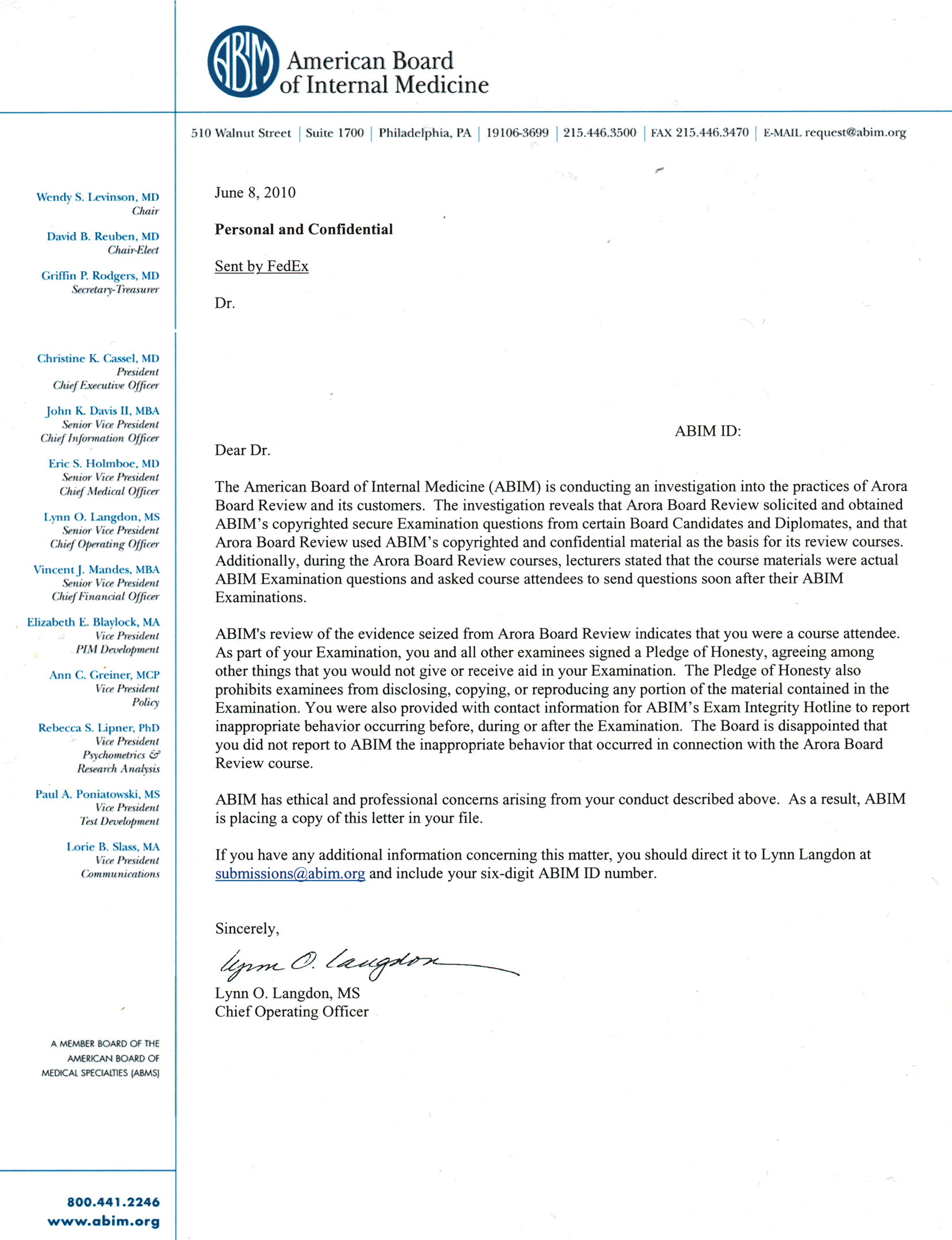
On June 8, 2010, he received a
sanction letter from the ABIM. In that letter the young doctor learned that the ABIM had
suspended his certification for three years because they alleged that he had shared question content from memory with Dr. Arora in violation of the ABIM's "Pledge of Honesty." His board certification status was immediately revoked without due process.
His mind spun. "How in the world?... What happened?" His life, quite frankly, had gone from idyllic to uncertain in an instant. He couldn't sleep. He was humiliated and had to tell his wife. But one thing he was sure of: he didn't want to have to take the test again. Four years of medical school. Three years of residency. Night call. Sleepless nights. Finally, realizing the magnitude of what had happened to him and the possible lifelong ramifications, he retained a lawyer.
He spoke with his lawyer - someone he'd worked with earlier. She was sympathetic. So calls were made to the ABIM's lawyers. At first, ABIM lawyers were unyielding: it was a three-year sanction and then he had to retake the examination.
A short time later, his lawyer called him to tell him about
this article that had appeared in the
Wall Street Journal June 9, 2010. He was not the only one; there were 138 others. His penalty could have been worse, he was told. At least he wasn't formally sued but his privileges to practice medicine were temporarily suspended at one of his hospitals from 2010 through part of 2011 and compromised his ability to moonlight to pay for his children's daycare.
"I can't take that test again. I just started my residency!" he thought. After pleading with ABIM, the sanction was reduced from three years to one on July 28, 2010, but he
appealed this decision since the financial and professional implications of even a one-year sanction were devastating.
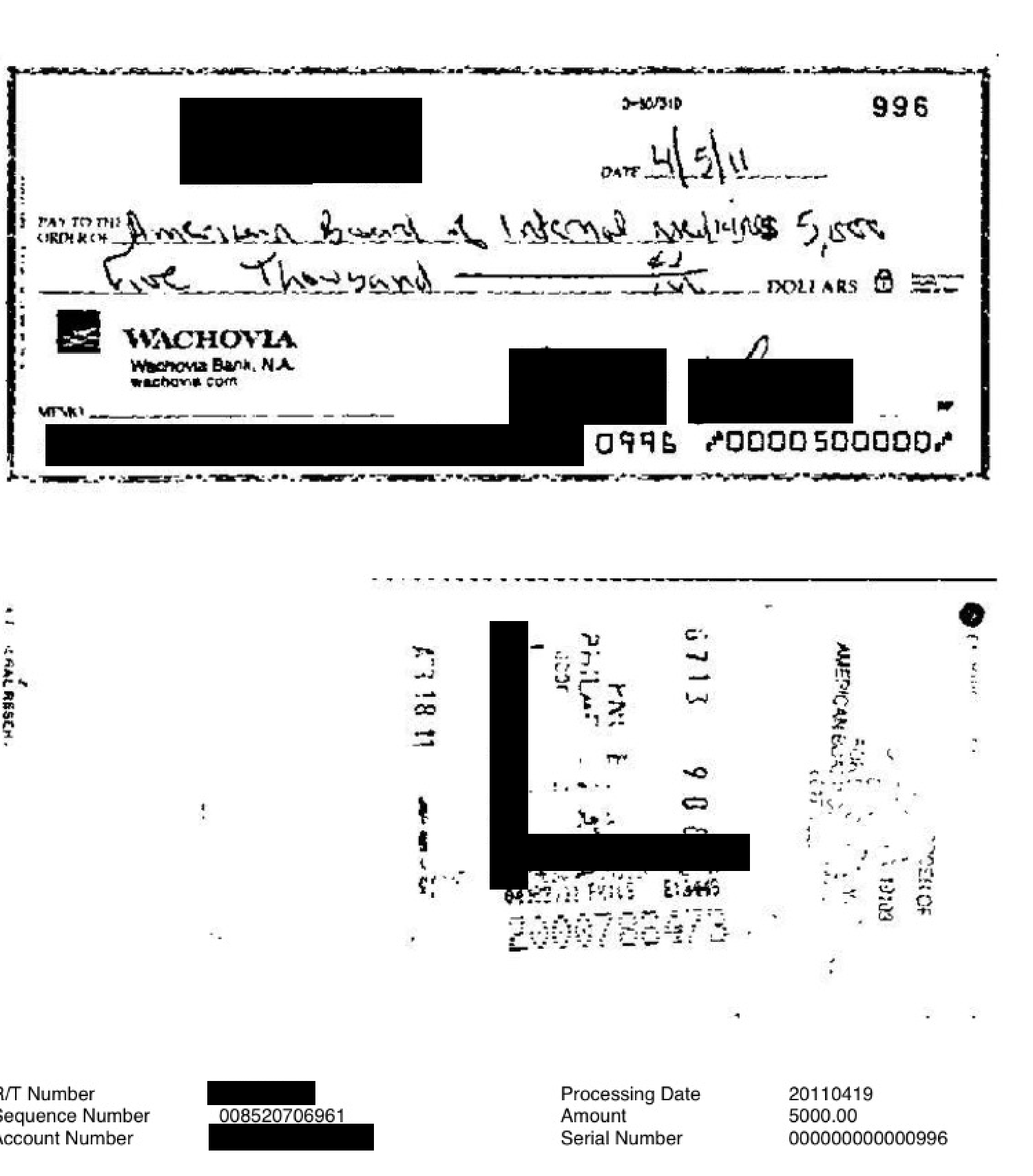
Months later after more letters and were exchanged a plea "deal" was struck with the ABIM April 5, 2011 - the ABIM agreed to settle with the doctor for a
$5000 fine along with
20 hours of community service in a medical-related charity and proof of completion of an ethics course.
What choice did he have but to agree to those terms?
 |
Cancelled Check Paid to ABIM to Reinstate Board Certification*
(Click to enlarge) |
Finally on 1 Sep 2011, the young physician's Board certification was
reinstated but the scars linger. From now on, he must always explain that he was "sanctioned" by the ABIM when completing a hospital credentials' packet or being licensed by his state. Needless to say, he no longer practices in a hospital setting.
Commentary: In retrospect what this young doctor didn't realize at the time was that the Arora Board Review course was secretly recorded as part of an ABIM-sanctioned "investigation," apparently without law enforcement oversight. On the basis of that recording and evidence gathered by a undisclosed ABIM employee that secretly attended the review course, this "evidence" was presented before a federal judge by Christine Cassel, MD, Ms. Rebecca Baranowski, and A. Benjamin Mannes (the ABIM's currently employed "Director of Investigations" who carries two felony convictions (for impersonating a police officer and carrying an unregistered firearm) and has unfettered access to the ABIM diplomat's files and personal information). On the basis of that information, the ABIM was granted a writ to seize under seal after providing $10,000 in collateral so Federal Marshals could secretly invade Dr. Arora's residence with ABIM attorneys accompanying them. According to court documents, the ABIM obtained images of Dr. Arora's computers, hard drives, and 36 boxes of course materials. To the best of my knowledge and belief and on the basis of this ABIM "letter of concern," only after obtaining those computers did the ABIM discover the emails of who attended the Arora Board Review Course course and had communicated electronically with Dr. Arora. The earlier communications with Dr. Arora were thought to be private and occurred without financial renumeration to either party of any kind. As such, it appears the raid was little more than a fishing expedition for physicians' emails and addresses who attended the board review course. It appears to me that because the young doctor's email to Dr. Arora was found on one of those computers, and he represented a vulnerable target, he was immediately sanctioned without due process. Dr. Arora, on the other hand, worked a separate settlement deal with the ABIM that has never been made public.
Same Course, Different Doctors, Different Sanctions
Another Arora Board Review
sanctioned physician-attendee had a different penalty imposed. Not only was this physician sanctioned for three years initially, this physician was later forced to sign an agreement with the ABIM that he had committed an ethical violation, had his upcoming subspecialty medical board examination cancelled, and was required to re-take his internal medicine certification examination. But this was not his most difficult problem.
After learning of the ABIM's sanction, his state licensure board also
required the physician pass a "maintenance of certification" examination, take an ethics course with an "unconditional pass," do 50 hours of community service, pay a $1000 fine, and provide peer review references before state would re-issue this state license to practice medicine. His online credential verification still documents his sanction today. All of these actions did not include the legal expenses the physician incurred to defend himself with two separate state licensure boards (WA and TX) and the ABIM itself.
Ongoing Litigation
Some nine years after the June 2007 Arora Board Course, the ABIM has still not finished sanctioning physicians. Jaime Salas Rushford, MD, a Puerto Rican physician who attended the same Arora Board Review course, learned of his
sanction by the ABIM on 8 May 2012. In his sanction letter, his certification was revoked indefinitely. Shortly thereafter, Salas Rushford also learned that he had been
sued by the ABIM as well. What the ABIM had not anticipated was that Dr. Salas Rushford's parents are lawyers. They filed a
counter-suit (begins on page 32). The case has been ongoing four years later and full details of the ABIM's operations and tactics are being systematically uncovered in documents on Dr. Salas Rushford's website,
doctorsjustice.com. Millions of dollars in legal fees paid by physician diplomats continue to flow to the ABIM's legal team. Unfortunately for all US physicians, this story is far from over and will likely become, as described by the Pennsylvania Medical Society in their recent
vote of no confidence (more
here), "the
most expensive medical mistake in the history of medical education."
Epilog
Given what we now know about the ABIM's
long-standing tenuous financial condition, the
"research" the ABIM performed and funded from these vulnerable diplomat's exam fees without true informed consent, the
undisclosed lobbying that ABIM participated in as a non-profit outside of federal regulations, the
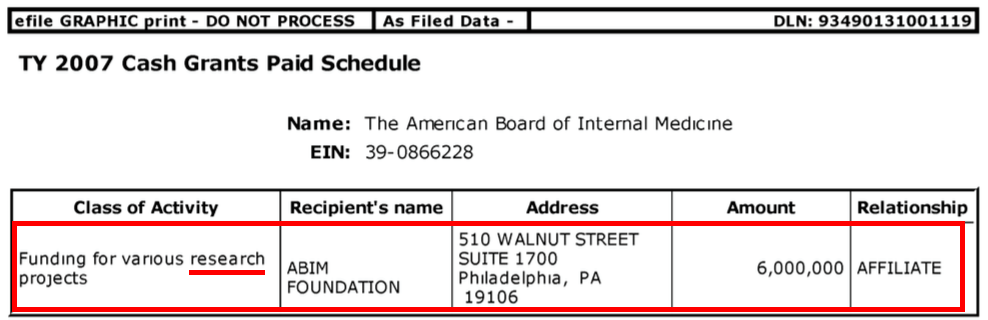
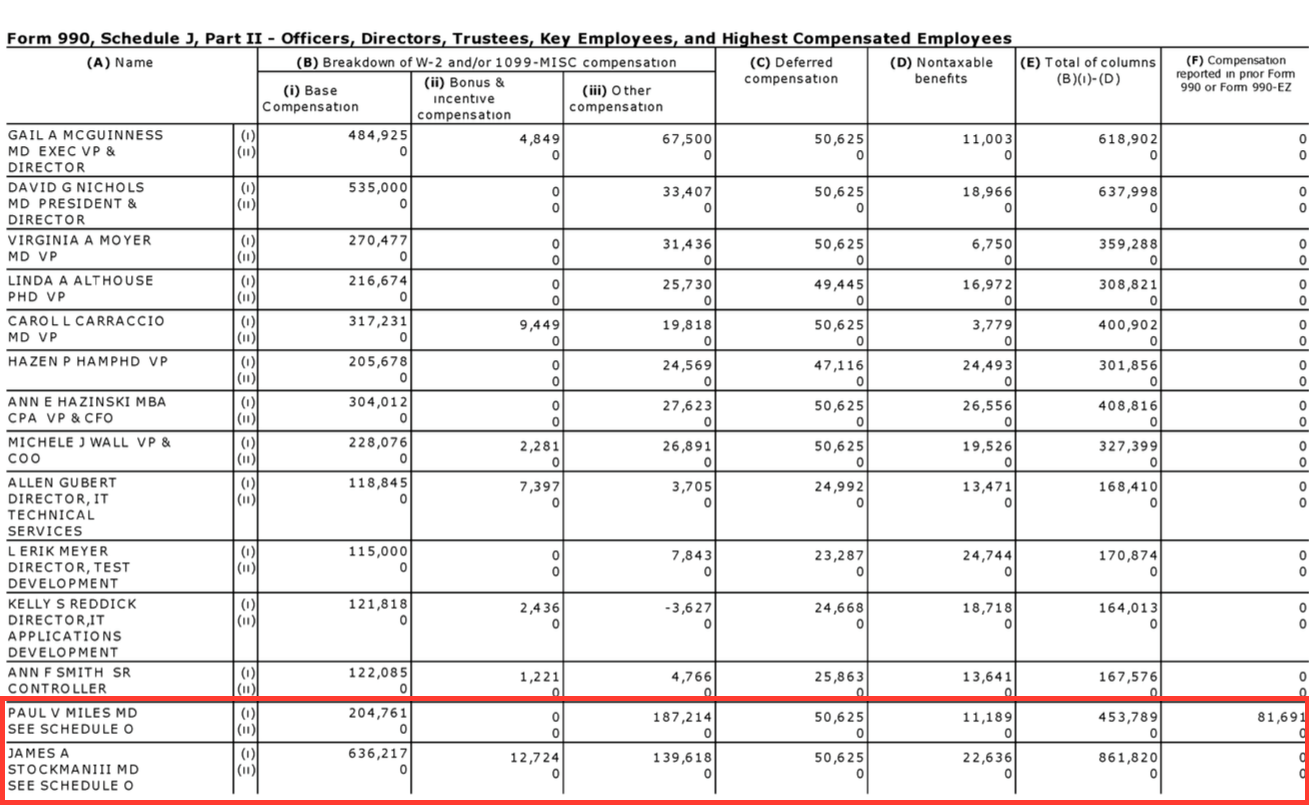
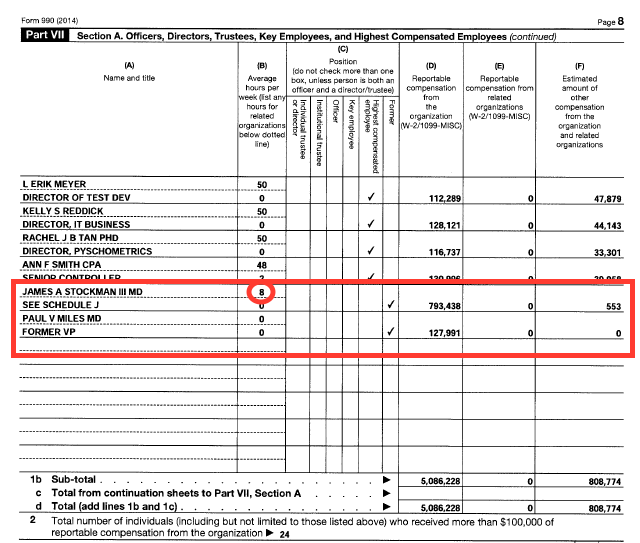
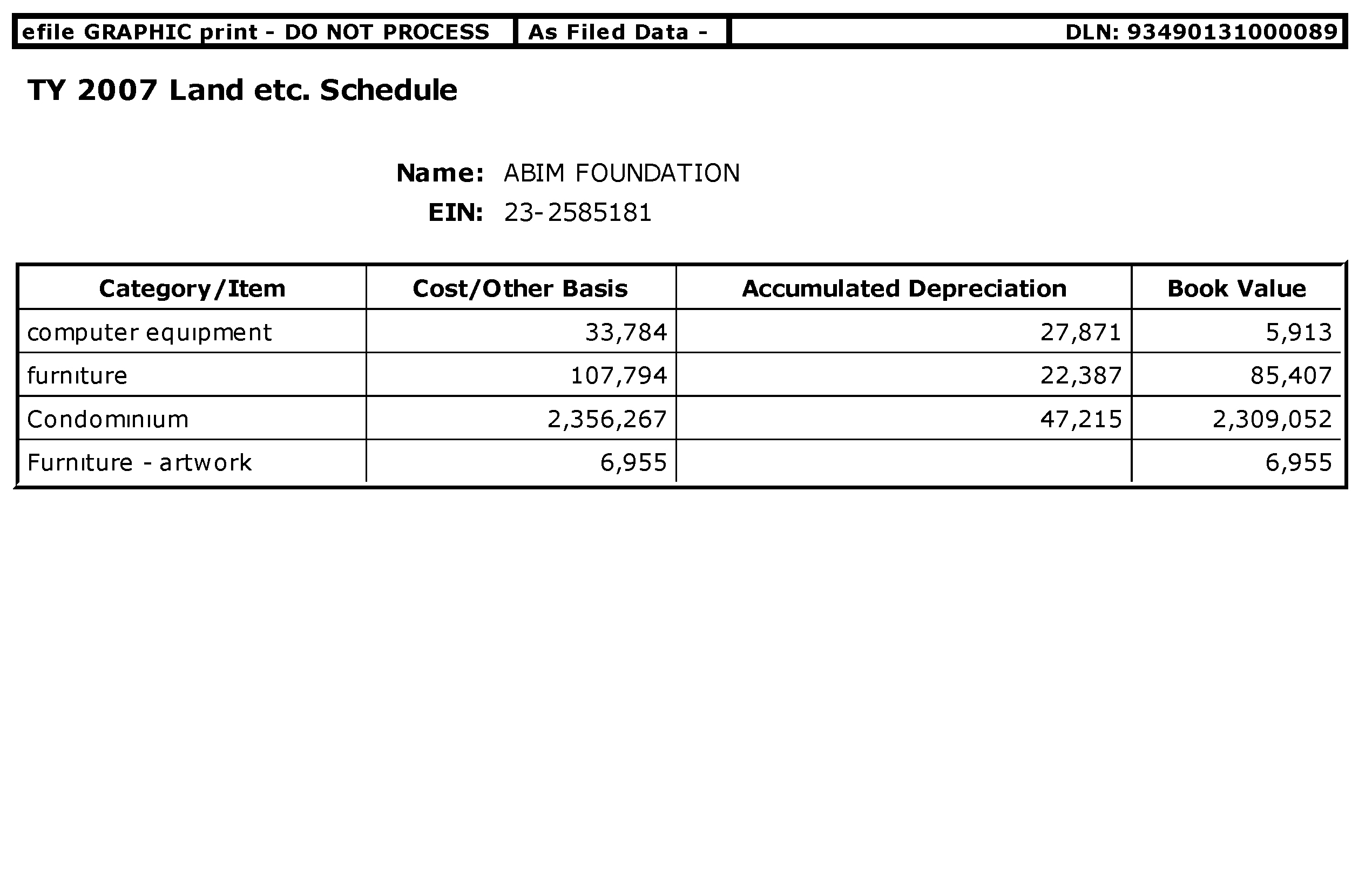
years of fraudulent tax filings, the funneling of $55 million of ABIM diplomat fees to
fund the ABIM Foundation that performed additional "research" and
purchased a luxury condominiums for its use, it is hard to imagine the ABIM has physicians' or our patients' best interests in mind. Furthermore, the American Board of Medical Specialties' (ABMS) (who overseas all of the
ABMS member boards, including the ABIM) earlier
Senate testimony that claimed they are expanding "new kinds of (undisclosed) partnerships with public payers, private payers, and particular patients and consumer groups who represent them to get a deeper appreciation for the kinds of information they seek and their expectations for care..." with numerous undisclosed revenue streams, there is only one question to ask of these unaccountable cartel-like physician credentialing "non-profit" organizations now.
Did the ABIM act in the public's best interest by sanctioning the many vulnerable resident physicians who attended the Arora Board Review course or did they engage in extortion for the ABIM/ABMS's financial benefit as a result of the ABIM's financial largess using police-state tactics?
-Wes
“The arc of the moral universe is long, but it bends towards justice.”
― Martin Luther King Jr.
*The redacted canceled check and redacted documents above were all used with the ABIM diplomats' permission.


{kind=link}
{kind=link}