What is Maintenance of Certification® (MOC®)?
Is it an educational program for physicians? If you think so, you are wrong.
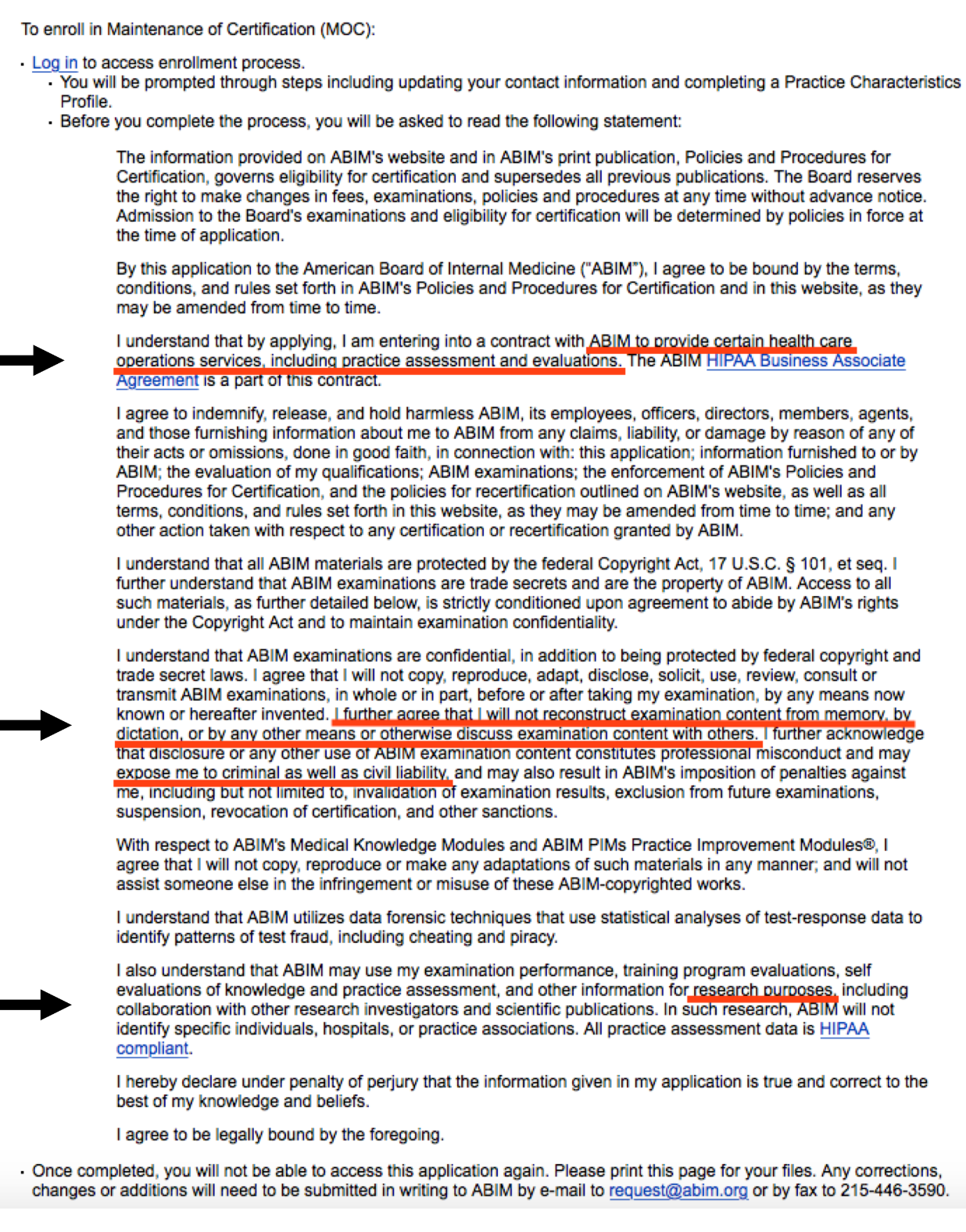
MOC® has almost nothing to do with physician education, but according to the
contract we must sign, involves "certain health care service operations, including practice assessment and evaluations." Most importantly, it allows physicians' personal and practice data to be shared with an unlimited number of third parties through a
HIPAA Business Agreement.
Let me be clear. MOC® is not really about physician education. Instead, MOC® allows a physician's personal data to be shared with data registries and large corporations who profit from those data. For instance, our MOC® and survey data are shared with (sold to?) Premier, Inc. (
PINC, the $4.3 billion owners of CECity, Inc.), the largest healthcare performance improvement company that serves 3,900 hospitals and health systems and approximately 150,000 other providers and organizations." (Remember, Christine Cassel, MD, former President and CEO of the American Board of Internal Medicine,
served on the board of Premier, Inc at one time and earned plenty of
money and stocks in that capacity while at the ABIM.)
It also allows physician data to be sold to
ABMS Solutions, LLC, a for-profit wholly-owned subsidiary of the American Board of Medical Specialties that is based in Atlanta, Georgia, who then sells your MOC® status, updated every 24-hours, to others, and a company never mentioned in disclosures published in our major medical journals. They will also plan to share these data with the
Disciplinary Action Notification System database owned by the privately-held non-profit Federation of State Medical Boards that
solicits "Affiliate Members, Official Observers, and Courtesy Members."
Again, MOC® is not about physician education. It is about collusion with multi-billion dollar companies, including Wolters Kluwer, and Pearson, LLC, and even our own politically-powerful American College of Cardiology that who owns the NCDR procedural registries and sells access to them to hospitals with
MOC® as its demographics supplier (a full explanation of how this works is available
here).
Why is the understanding of this "definition" of MOC® so important?
Multiple states are enacting legislation to prevent MOC® as a cudgel to limit a physician's ability to hold hospital credentials, be on insurance panels, or obtain state licensure. Our physician data are that important to these companies they will stop at nothing to be sure we sign that MOC® agreement.
What if the ABMS re-brands MOC® to some other "product" at their December 4th meeting with all of those state medical societies frustrated with what MOC® has become? Might the American Board of Medical Specialties and their collaborators skirt existing "anti-MOC®" legislation?
Current anti-MOC® legislation must anticipate this and not include "MOC®" but "MOC® or any other health care serve operation that may include practice assessment or evaluations that requires a physician to sign a HIPAA Business Agreement to which they are not parties" in their language.
Physicians enacting anti-MOC® legislation need to understand the legal definition of MOC®. That way they can write legislation that is lasting, meaningful and enforceable, irrespective of how MOC® is ultimately re-branded.
MOC® is broken and must end. Not because it's a failed physician education experiment. It's broken because of its threats to physician civil liberties and threatens the doctor-patient relationship at it's most intimate level, thanks to the age old business motivators, money, power, and greed.
-Wes

{kind=link}
{kind=link}
{kind=link}
{kind=link}