Her breathing had never taken a second thought, except for the past several months. Slowly, gradually, her breathing became work so she came to our emergency room.
Her life had been an full one: married, kids, grandkids - all of whom brought her incredible joy. But since the loss of her husband and all of the changes that occurred in her life as a result, she felt more alone than ever. Perhaps this was the reason the pacemaker she had received some 14 years before just didn't seem so important any more. Her kids and grandkids were what remained now, and for them she was grateful for they had noted she'd become too short of breath with even the slightest effort, so they brought her in.
The chest-xray taken when she came to the Emergency Room showed her pacemaker and prompted the ER staff to ask about it. "She hasn't had a pacer check in a while, " the family mentioned. So we were consulted to check the pacemaker's function.
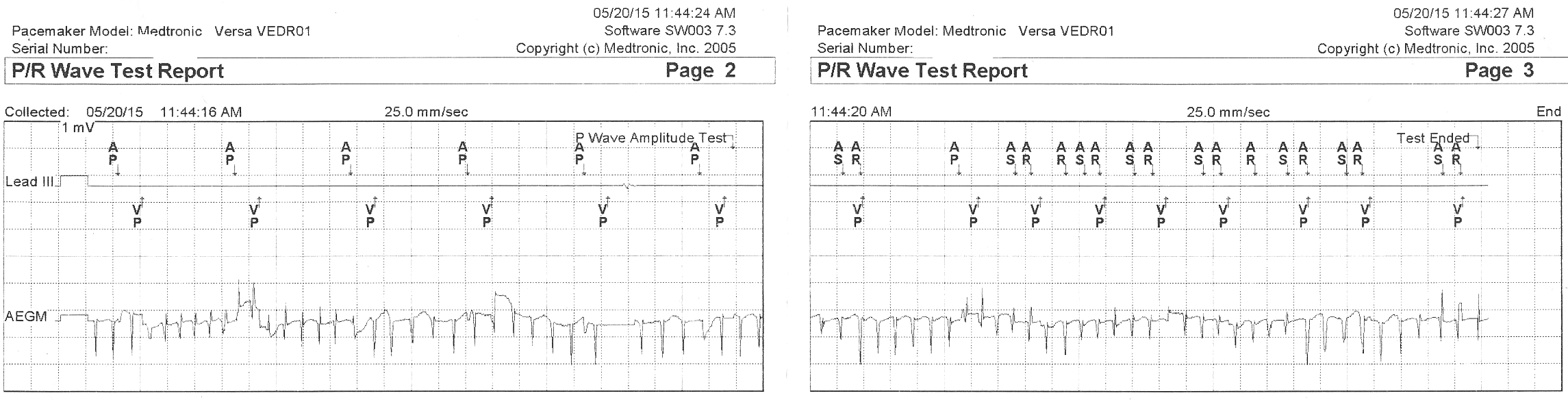
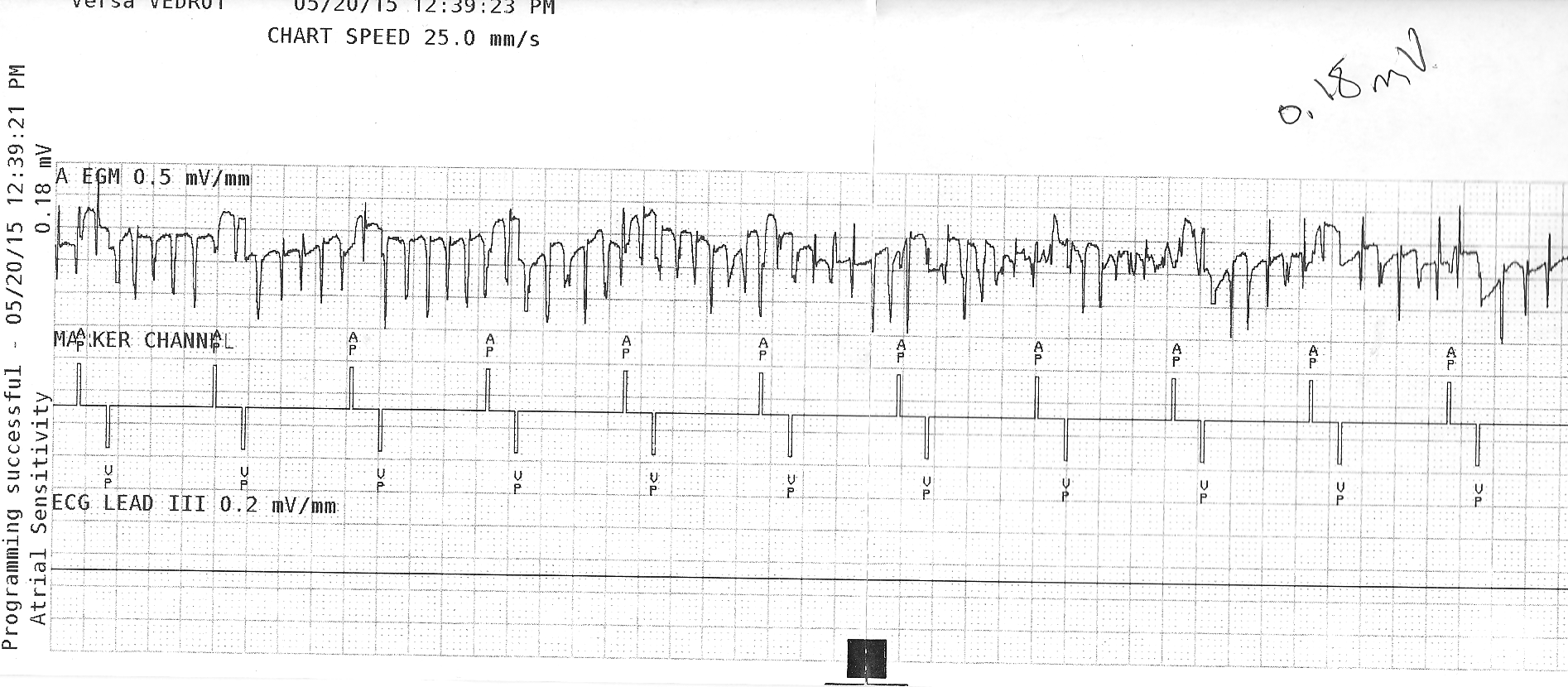
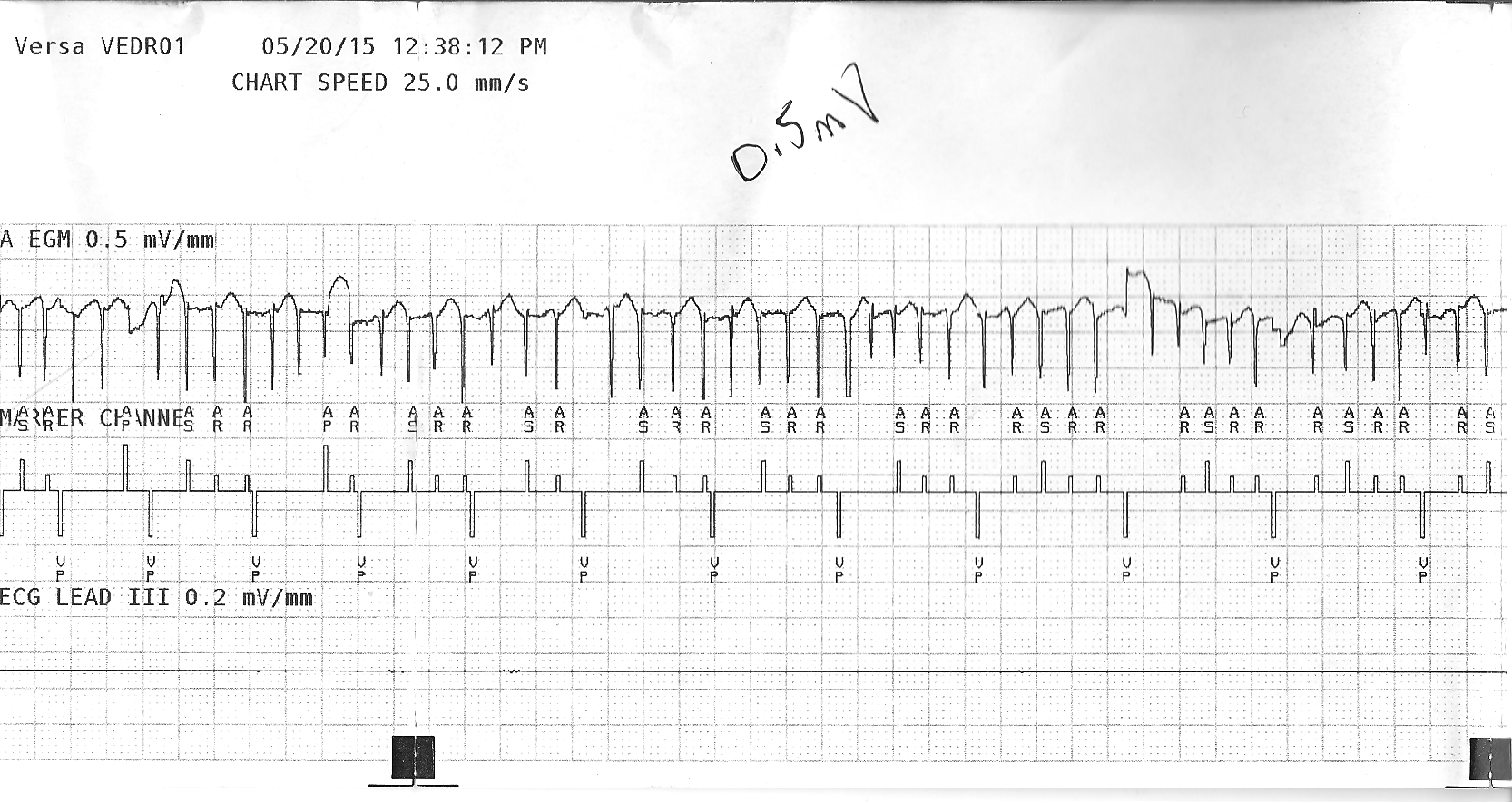
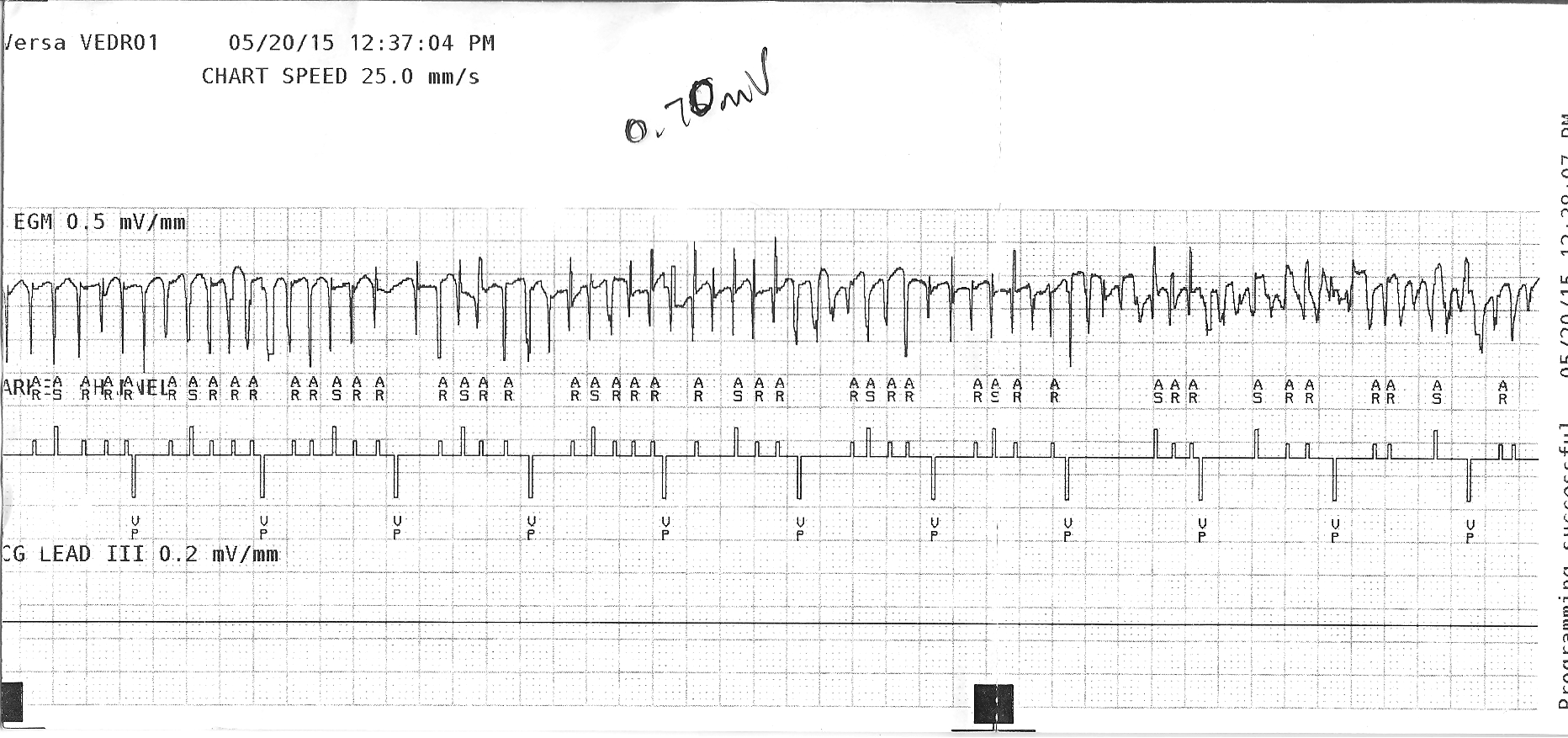
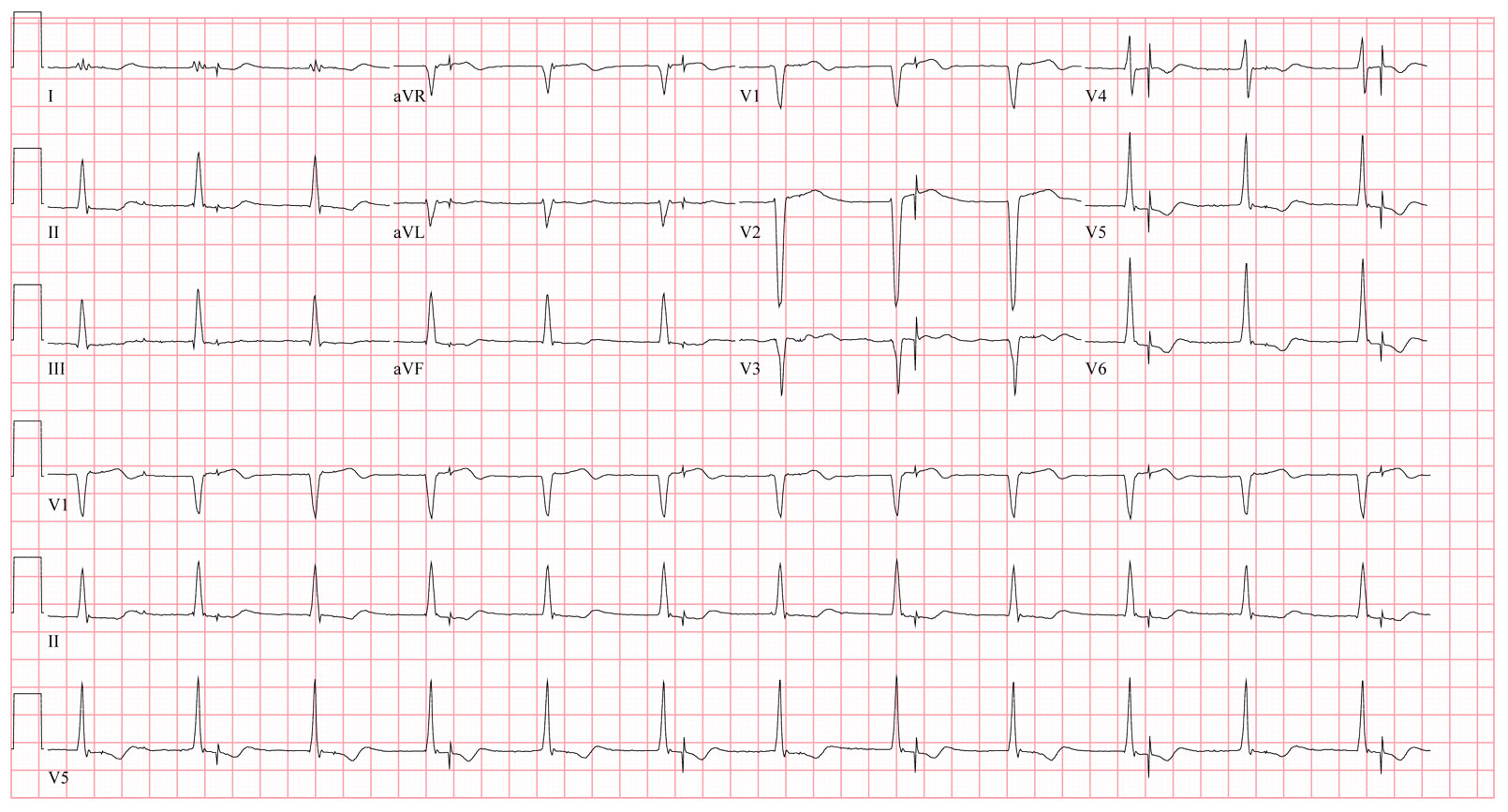
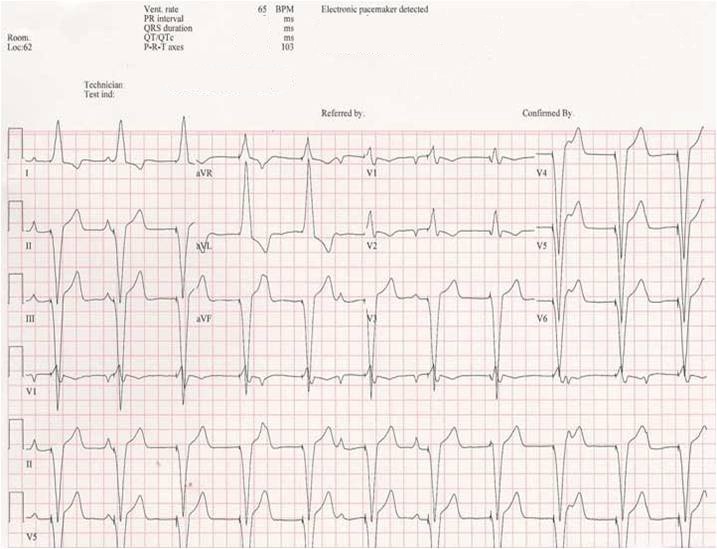
Before we'd done so, we looked at
her EKG and weren't surprised at what it showed. After all, we'd seen
this scenario before.
So with some confidence I entered her room. There sitting beside her was one of her sons and a granddaughter. She was propped up in bed wearing a green oxygen face mask that covered her mouth and nose but couldn't suppress her kind smile as I entered. After a brief introduction, I explained what her EKG showed and how I thought a good portion of her shortness of breath might be stemming from her pacemaker's low battery.
In our conversation she mentioned that she had been told her pacemaker battery would need to be changed soon. That was before her husband died. After his funeral, the need for a recheck of her pacemaker was quickly forgotten. So she had not anticipated that the pacemaker might be a cause of her symptoms.
We discussed her options. She could leave things well enough alone if she preferred while we arranged to keep her comfortable for her remaining days, or we could change her pacemaker battery. At the time, she didn't want excessive resuscitation measures and had declared herself a "DNR - Do Not Resuscitate" in the event of cardiac arrest. She thought hard about the choices but wasn't sure...
"Mom, it seems like such a small thing and it might be able to help you feel better! Don't you want to see your grandkids a little longer?" the son pleaded. She listened to him, then looked at me. It was clear she understood the choices and their implications. I suggested she think about it and left the room to give them time to discuss things. Some time later, she asked me to return.
She asked again, "So you think it might help me feel a bit better to have the battery changed?"
I replied, "Honestly, I do, but it's always hard to gauge how much."
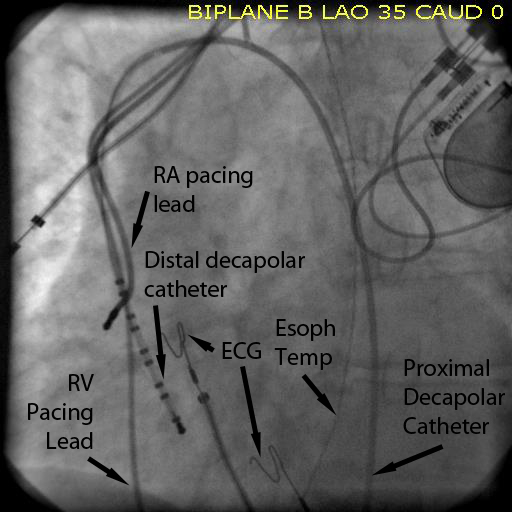
So after a few more questions were answered and worried looks shared with her son, she agreed to have her battery replaced. I left the room to document my visit. (After all, nothing happens in medicine any longer unless typing occurs.) Seated next to me was my nurse practitioner, herself transfixed to the computer screen as she returned patient phone calls and made arrangements for procedures to be performed the next day. Next to her was the pacemaker programmer which she wisely brought with her to help check the patient's device. She finished her call and then offered to check the device while I finished my note. I thanked her and continued typing.
It was still relatively early in the afternoon and the eight computer terminals around me were completely occupied by nurses, physical therapists, and residents hammering away and looking stone-faced, somewhat akin to what the
New York Times newsroom must look and sound like just before deadline.
Until that sound was shattered by "Call a Code! Code Blue! Get Dr. Fisher!"
Somewhat startled, I looked up to see a sudden shift of the masses. Was that the voice of my nurse practitioner? It couldn't be, could it?
It was.
Poor thing. It seems she placed the wand of the pacemaker programmer over the patient's device, only to see a strange screen on the programmer appear that read something like: "Pacemaker reached ERI 8/13/2013…" followed by a bunch of other text that said something about "Power-on Reset mode" among other things. As she struggled to read the long message and donned a pair of glasses, she noted some twitching in the corner of her eye coming from the patient's direction. She looked up to see a peaceful blank stare on the patient who now laid motionless and unresponsive - a quick glance at the monitor showed it had flat-lined with only a rare agonal ventricular escape rhythm. Realizing what had happened, she was briefly at a loss how to react. This was not supposed to happen. Fleeting thoughts raced through her head like "Seriously?" and "Oh, God, I'm too old for this!" That's when she called out for help.
The poor son and granddaughter sitting in the corner were stunned, not knowing what had just happened. A horde of medical personnel swept in to the room and ushered them out, terrified. I entered the fray and saw my pleasant patient lying there motionless, small puffs of condensation appearing on her face mask and her pupils somewhat dilated. The monitor, too, was devoid of motion, except for an occasional blip seen one the screen. I reached for a pulse. It correlated to the monitor. Not much at all.
"Can we get some atropine and epi?" A asked the code team nervously assembled, not knowing what to do in this "no code" situation. Fortunately, I removed the programmer head from her chest and watched her breathing carefully. Seconds seemed like hours as my poor nurse practitioner stood beside me with her mind scrambling. "Come on guys, we need those meds… What's taking so long?… " she snipped. "Get the pacing patches!" They still were rifling through the drawers of the crash cart when she offered like a pro: "Guys, the purple box!" And within a second, the purple box appeared. The first medication was administered as time seemed to stand still. An occasional blip, then more people in the room. "What can we do?" the anesthesiologist asked.
I looked at the monitor dreading the thought of starting CPR given her wishes, or the what I might say to the stunned family at her bedside if we didn't.
But then, just as unexpectedly as it had begun, a paced rhythm resumed on the monitor! "Hold it!" I said, "I think we have a pulse!" And like a wilted daisy that just received its water, she immediately regained consciousness and wondered what all the fuss was about.
"What happened? Where did all these people come from? Why are they here?"
"It seems your pacemaker battery is a lot lower than anyone expected, Ms. Jones (not her real name). When we checked it, we must have used some of the last energy that pacemaker had. It looks like we need to take you our laboratory and replace that battery right away!"
She smiled and looked up at me with her precious eyes gleaming. Here we were, total strangers just minutes before, now bound together by some unimagineable force. She looked so comfortable lying there, then out of nowhere she reached up to me and grabbed my head, pulling it toward her oxygen mask in an attempt to give me a kiss right through it.
"Thank you," she whispered and smiled, "Thank you."
After reassuring her family and explaining what had happened, we hurried off to the EP lab, our eyes transfixed on her monitor and me still reeling from that beautiful and totally unexpected kiss...
... plastic face mask and all.
-Wes






{kind=link}