- 24 July 2012 - ABIM announces Medicare payment incentives for participation in their MOC program on their website.
- August 14, 2012 - Robert Wachter, MD assumes chairmanship of the ABIM, writes missive on his industry-sponsored blog justifying why board certification "matters more than ever." This post shows anticipated collusion for acceptance of MOC as a "quality measure" between Medicare, the Joint Commission, the Federation of State Licensing Boards, and the ABIM Foundation's Choosing Wisely campaign. Wachter fails to mention his simultaneous affiliation as director of IPC The Hospitalist Company, Inc., a company that "is the nation's leading national physician group practice focused on the delivery of hospital medicine and related facility-based services" in that announcement.
- 27 Apr 2013 - Drs. Wachter and Cassel named to Modern Healthcare's "Most Influential Physician Executives."
- 1 Aug 2013 - Robert Wachter, MD receives 1,355 shares of IPC The Hospitalist Company stock options valued at $50.68 per share (Market Value: $68,671.40).
- 12 Jun 2013 - ABMS lobbies Chairman Upton and Ranking Member Waxman of the US House of Representatives Energy and Commerce Committee to have MOC program included in MACRA (the SGR Fix bill) as a physician quality measure.
- 30 June 2013 - Christine Cassel, MD to step down from ABIM as President and CEO of ABIM and ABIM Foundation. Earns $1.7 million as she leaves to begin work at the National Quality Forum.
- 1 July 2013 - Richard Baron, MD becomes ABIM and ABIM Foundation President and CEO
- 25 Sep 2013 - Christine Cassel, MD issued 3706 shares of Premier, Inc (PINC) stock
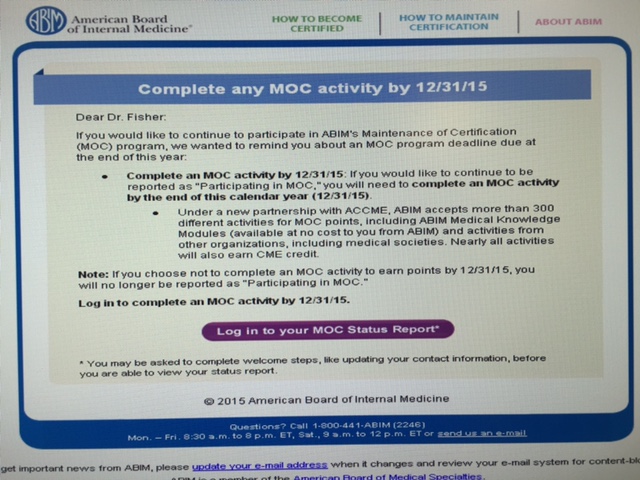
- 31 Dec 2013 - Physicians who participate in MOC program by Dec 2013 are able to claim 0.5% payment incentive from Medicare
- 1 Jan 2014 - ABIM offers either one-time (every 10-years) or annual payment plan option for its MOC program.
- 2 Jan 2014 - Robert Wachter, MD receives another 2,640 shares of ICP The Hospitalist Company stock options valued at $58.50 (Market value: $154,440)
- 10 Dec 2014 - Study appears in JAMA showing no effect of MOC program at improving patient outcomes.
- 16 Dec 2014 - The first detailed review of the MOC corruption appears on this blog with the publishing of "The ABIM Foundation, 'Choosing Wisely' and the $2.3 Million Condominium."
- 30 Jan 2015 - The ABIM is caught in the act if omitting 6 key financial schedules from its 2014 Consolidated Financial Statement that it released to the public.
- 31 Jan 2015 - A virtual tour of the ABIM Foundation's condominium is published.
- 3 Feb 2015 - ABIM issues previously unimaginable apology to the physician community stating "ABIM clearly got it wrong" but fails to mention the financial, tax filing, and financial conflicts of interest of its President and CEO and members of its board leadership.
- 3 Feb 2015 - Physicians (especially this one) are not impressed with ABIM's announcement that failed to acknowledge ABIM's history of serious financial and public reporting actions. Work continues to uncover what's being hidden.
- 16 Feb 2015 - ABIM initially fails to publish full financials for 2014 until pressured to do so. Apparent cover-up continues.
- 10 Mar 2015 - Veteran Newsweek reporter Kurt Eichenwald publishes his first take on the MOC controversy with his article entitled "The Ugly Civil War in American Medicine."
- 11 Mar 2015 - ABIM Board Chairman David H. Johnson, MD issues statement attempting to discredit Eichenwald's article claiming "numerous and serious misstatements, selective omissions, inaccurate information and erroneous reporting." Johnson disputes claims that ABIM pass rates have fallen, that ABIM has a monompoly on re-certification, claimed that Eichenwald was "selective" about the data presented and has a "poor understanding" of the tax records, and that Eichenwald had failed to disclose his wife was an internist.
- 30 Mar 2015 - New board (NBPAS.org) formed and doctors are moving on after more of the financial transgressions come to light.
- 3 Apr 2015 - Dr. Robert Wachter, the former chairman of board at the ABIM, tops Modern Healthcare's Top Fifty Most Influential Physician Executives and is "not afraid to challenge the status quo." Not surprisingly, Dr. Christine Cassel again makes the list as well.
- 7 Apr 2015 - Kurt Eichenwald's next Newsweek article on the ABIM MOC program, "A Certified Medical Controversy," is published and begins to target many of ABIM Board Clair David H. Johnson's criticisms.
- 8 May 2015 - Consequences to physicians who fail their unproven MOC re-certification secure examination published online.
- 21 May 2015 - Kurt Eichenwald's third expose on the ABIM's finances called "Medical Mystery: Making Sense of ABIM's Financial Report" hits the pages of Newsweek disclosing the unreported lobbying efforts and the convoluted and large payments made to the ABIM leadership including $1,712,847 made to Christine Cassel, MD in fiscal year 2014.
- 22 May 2015 - Richard Baron, MD publishes another official ABIM response to Kurt Eichenwald's articles claiming "we have never made any effort to obfuscate, hide or delay ABIM's financial information." Baron did not acknowledge that they failed to release all of their audited financials (see 16 Feb 2015 entry on this timeline). Baron also fails to mention that the ABIM failed to release 12 years of audited financials requested by a reporter from the Wall Street Journal in August 2014. Additional attempts to obtain the reports from the PA Attorney General's office were also unsuccessful. Financial data were only obtained after a request was made to the office of the Pennsylvania governor's press secretary.
- 23 May 2015 - ABIM, it's finances, and the great revolving door collusion between the National Quality Forum, the ABIM, ABIM Foundation, and other specialty organizations published.
- 31 May 2015 - The ABIM's tax-filing cover-up of its lobbying activities with Congress exposed.
- 29 June 2015 - Robert Wachter, MD attempts to defend the actions of the ABIM on his blog after leaving his post as Chairman and speaks out. No corporate conflicts of interest are specifically mentioned by Dr. Wachter. Comments to his post are worth a read.
- 28 July 2015 - An independent cost analysis of the ABMS MOC program in published before print in the Annals of Internal Medicine.
- 15 Aug 2015 - ABIM Foundation tries to bury its old "About Us" webpage that claimed the creation date of the Foundation was in 1999 by editing the page to disclose the correct date of origin (1989) and then includes information regarding "$55 million" that was transferred from the ABIM to its Foundation from 1989 to 2007. The amount transferred was actually much larger and made secretly without disclosing the Foundation's existence to the physician community or public until 1999. The reasons for the secrecy and large annual payments made to the now defunct 1838 Investment Advisors (a spin-off of Drexel Burham Lampert financial fiasco - most of whom were indicted) made during that time have never been investigated or disclosed. One thing is now clear: it does NOT appear the sole reason for creation of the ABIM Foundation was to define and promote the term "medical professionalism" as originally claimed by the Foundation.
- 9 Sep 2015 - The ABIM's prior activities stumping for Big Tobacco in 1963 are revealed, lending less credibility to their claim that their certification program is for "public good."
- 15 Sep 2015 - Veteran Newsweek reporter Kurt Eichenwald publishes his last installment of a four-part series on the ABIM scandal entitled, "To the Barricades! The Doctors' Revolt Against ABIM is Succeeding!" highlighting how the ABIM MOC program has hurt physicians and patient care and what doctors are doing about it.
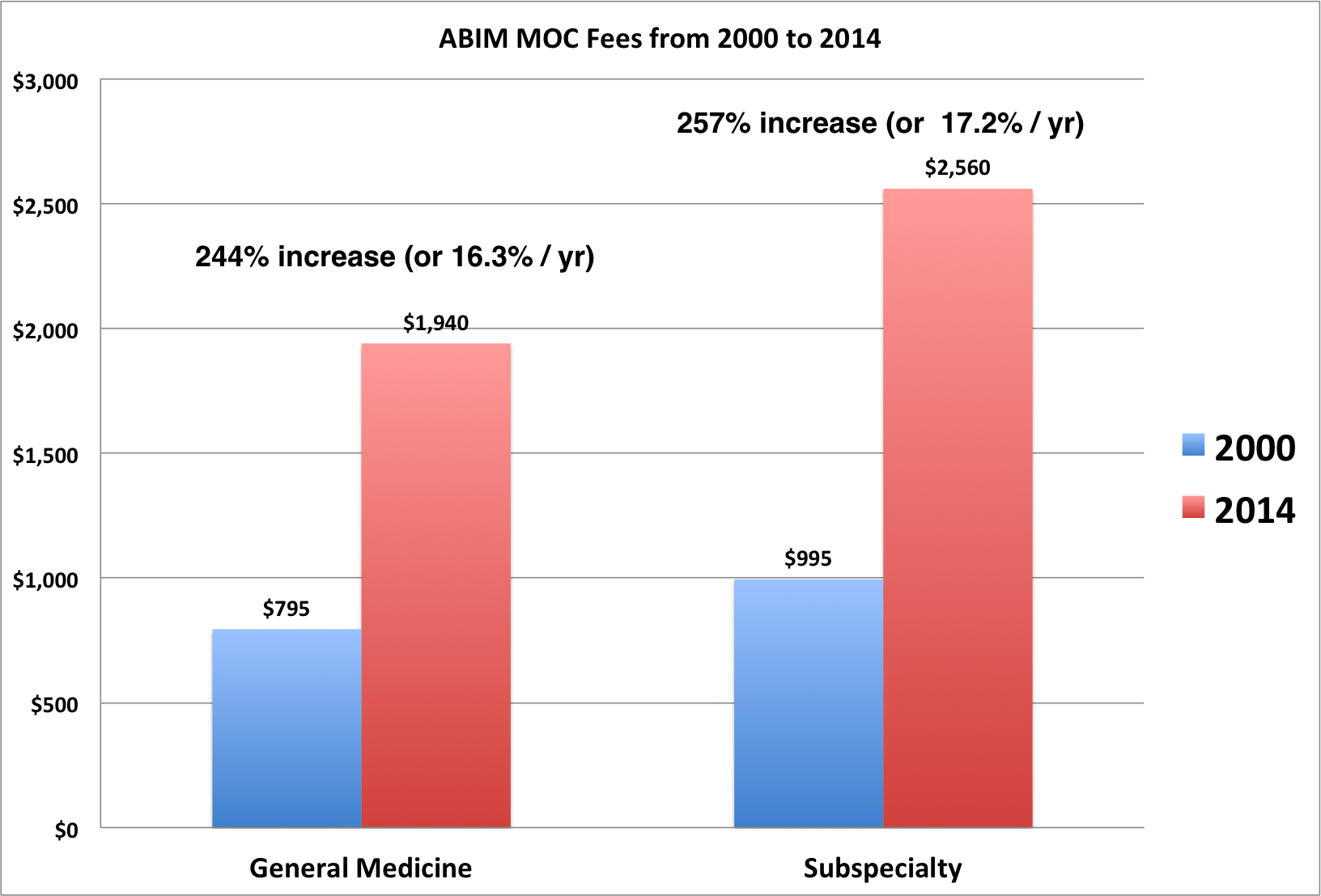
- 23 Sep 2015 - Graph of the growth in ABIM MOC Fees from 2000-2014 published showing at least 244% growth in cost (16.3%/year - far exceeding inflation) to internists over that 15-year time period.
- 25 Sep 2015 - ABIM's own Maintenance of Certification First-Time Pass Rates from 2000-2014 are published and document a negative pass rate trend line over that period of time in every subspecialty of internal medicine except Geriatric Medicine. The data trend stands in stark contrast to ABIM Board Chair David H. Johnson, MD's statement regardng MOC pass rates made 11 March 2015.
- 11 Nov 2015 - Concerning conflicts of interest with Christine Cassel, MD and the little-known company CECity, Inc. are published. Cassel's long-standing relationship with Premier, Inc. raises real questions regarding possible insider funding of CECity to prop up its value prior to its purchase by Premier, Inc. on 4 August 2015 for $400 million.
- 23 Nov 2015 - TeamHealth (TMH) acquires IPC The Hospitalist Company for $80.25 per share netting Dr. Wachter and his university, the University of California, San Francisco, a comfortable profit.
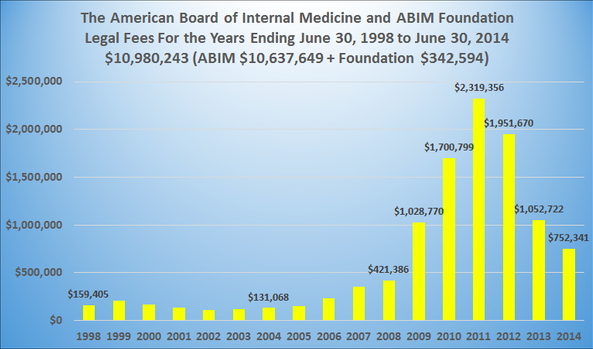
- 23 Nov 2015 - Graph of ABIM legal fees pre-ABMS MOC program (instituted in 2005) vs. post-MOC (ongoing) appears.
- 29 Nov 2015 - ABMS's income stream for selling daily updates of physician certification status from the unproven and un-vetted data gathered from its member boards via ABMSSolutions.org disclosed bringing the legitimacy of the entire ABMS MOC empire sharply into question.
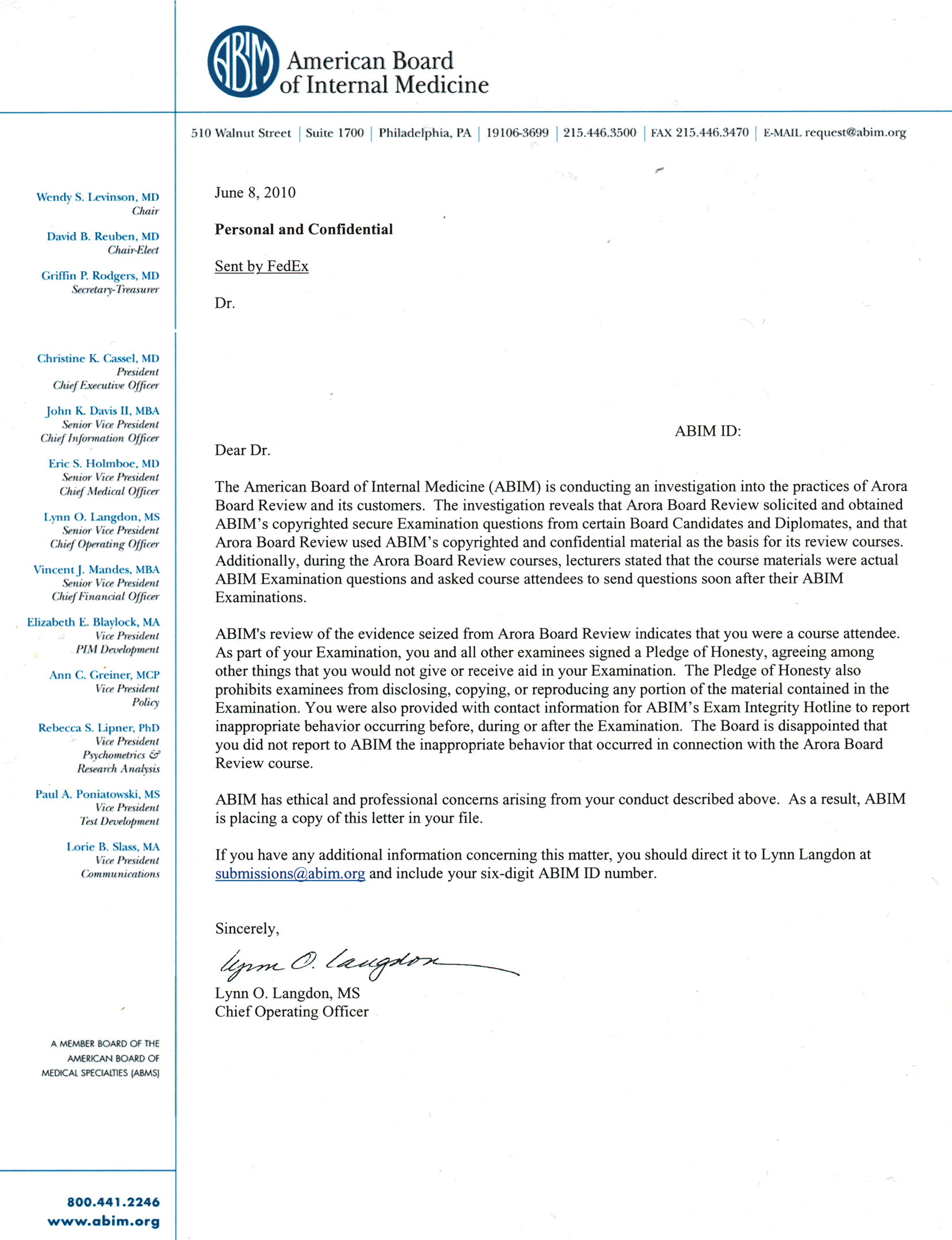
- 6 December 2015 - A copy of the physician sanction letter issued June 8, 2010 surfaces on this blog and gives a glimpse into the strongman/boss tactics used by the ABIM to protect their certification monopoly. The tactics used to track down physicians late after they participated in a board review course years before are now coming under intense scrutiny.
- 16 Dec 2015 - ABIM announces its intent to extend its practice assessment decision through 2018.
- 17 Dec 2015 - Christine Cassel, MD leaves her role as the President and CEO of the National Quality Forum (in charge of setting "quality" standards for the nation's hospitals) to join the leadership team of Kaiser Permanente's School of Medicine. Dr. Cassel had long-standing financial dealings with Kaiser since at least 2003.
My prediction for 2016: the ABIM collapse under its own spending weight but not before "grants" are issued from the ABIM Foundation back to the ABIM to support its operations.
If the ABIM does collapse, what happens to the certification process for US internal medicine physicians? Clearly, significant change (including electable board members and disclosure of conflicts of interest publicly) are of paramount importance. Returning board certification to a lifetime designation also seems paramount since the MOC program continues to prove itself as highly destructive to our profession.
So stay tuned in 2016. It promises to be an interesting year as more revelations regarding the ABMS MOC program develop.
-Wes
Addendum: 28 Dec 2015 @13:04 - Post updated to include 27 Dec 2012 and the failure of Dr. Baron to report his conflicts as Director of the Seamless Care Model Group in the NEJM publication. Also, 28 July 2015 was added to include the cost analysis of the ABMS MOC program published in the Annals of Internal Medicine.
Addendum: 28 Dec 2015 @ 13:21 - 27 Dec 2015 deleted from timeline - Author of the NEJM piece was Robert Baron from the University of California, San Francisco, not Richard Baron, MD - hence why there was no disclosure of this conflict on the NEJM publication. I regret the error.
Addendum 30 Dec 2015 @ 10:45 - Timeline updated with additional information revealed on 23 Sep 2015 and 23 Nov 2015 regarding growth of costs and legal fees.