American Gastroenterological Association Takes Important First Step to Oppose ABMS MOC® Program
One by one, Internal Medicine subspecialties are fleeing the sinking American Board of Internal Medicine (ABIM) Maintenance of Certification® ship and creating new, non-punitive learning pathways in lieu of "recertification."
Especially important in this proposal is the permanent rejection of the need for additional "Performance Improvement" and "Patient Voice" modules AND the rejection of the high stakes secure examination after initial certification.
Here's why.
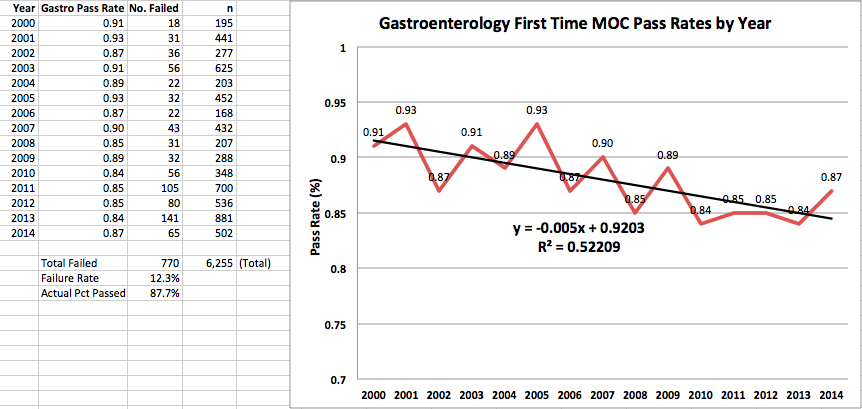
Here are the gastroenterology ABIM Maintenance of Certification secure examination first-time pass rate results for the past 15 years:
(Click to enlarge)
Note the linear regression line of the published first-time pass rates of the ABIM gastroenterology Maintenance of Certification® secure examination has declined steadily by a remarkable 0.5% per year since 2000. The pass rate also changes year to year, suggesting a lack of precision of this testing metric. As more and more gastroenterologists have had to participate in MOC®, this declining pass rate of the secure examination results in a progressively higher number of gastroenterologists that must take time away from caring for patients to retake their MOC® secure examination (and pay for more review courses) to ultimately pass. Yet there are simply no data that taking the MOC® secure examination after a gastroenterologist has practiced a minimum of six years makes them a better or safer gastroenterologist. More importantly, because participation of the American Board of Medical Specialties' (ABMS) MOC® program is increasingly tied to a physician's hospital credentials (likely thanks to the fact that the ABMS and the American Hospital Association are both member boards of the ACGME), clinical gastroenterologists now realize they could lose their ability to practice in a hospital setting without cause if they fail this unproven secure examination metric (see this reference).
Look for other medical and surgical subspecialty organizations to quickly follow suit.
The ABMS's lucrative continuing medical education monopoly over practicing physicians will slowly but surely come to an end.
Correction to your article. No need to publish this! "rejection of the high stakes examination after recertification," should read:
"we reject the high stakes examination after initial certification."
There is a big difference for two reasons. She said after initial certification And the strength of Suzy's words and sentiment "we reject" is important in the live delivery on social media.
Pledge of a return to integrity by governing bodies.
What Suzanne said was even more significant, because of the emotional strength in which she said it. Without addressing in words the ABIM/ABMS corruption and deceit, it is implied in her tone that she pledges AGA's sustained integrity to serve the physician and not the other way around.
I have painfully discovered at the ABIM/ABMS the physician apparently serves the personal bank accounts of politicians like Chris Cassel, or ABMS board members like Lynn Langdon, who undermine the integrity of what it means to be a medical professional. It is clear that Cassel and other like her have worked to serve personal political agendas, and at the same time inuring themselves beyond what is reasonable for a nonprofit society. It is most likely, from the data I have, these types of corrupted bureaucratic institutions are in service of corporate and government monetary interests and not the public interest. To be clear this is my take. But it is especially poignant when you check the facts for yourself concerning the financial misstatements of the ABIM and the well-rehearsed practice of lying about it and the political cover-up. That is far from transparency.
That is why it is so heartening that the AGA presenter, with clear tone, takes a stand AGAINST 'blatant deviations' which harm practice interests and 'disruptions' of ongoing educational needs of professional working physicians. And I hear a "yes we hear you" voice that is concerned about the disruptive elements in medicine today that are roadblocks to real service to the public.
If I am wrong, Suzy, please correct me on this blog.
The excellent reporter, Wes Fisher, who maintains this 'news blog' has the best gut instinct for truth and falsehood as any reporter I have seen in my life.
I believe, furthermore, Wes would agree with my latter statement that the AGA is taking a stand against corruption of the medical profession and sending a clear message to the bureaucrats who may be in high places, but are completely out of touch with the plain common sense medical reality of today. The spokesperson for the AGA has communicated in her important pre-announcement that physicians will not be deceived again.
The clear voice and the integrity of the person relating this important turning point in the MOC crisis and its significance to the working professional is unmistakable!
Yes, we heard you and the task force's commitment to serve the public trust loud and clear, Suzy!
Read the AACE statement about MOC and lifelong learning as well. They support initial certification only, not MOC. The same strength and integrity. They dropped out of Choosing Wisely also. A very wise choice.
Now it is time for all to stand up and give their real voices as Suzanne in behalf of the AGA has.
Dear Arthur MD, I am interested to hear what you think. You have a useful blog and I enjoyed your Bob Dylan song. It was fun and creative. Quite good actually. I also appreciated some of the clarifications over medical issues that I, as a patient, would not have thought of reading your blog. I don't care if you rub me wrong by calling me a rube, if that is who you were directing your comment to, and if it is name-calling. Maybe it is just a fun comment. I like it myself because I had to look up the meaning of "rube". I'm still am not clear on it's meaning and origin. Never used the word before. But, I think it applies to me. I am a rube as far as I can tell; so far at least. I did grow up on a farm. Worked hard for my family. Not much time to think. Is that what you meant by rube, a farm girl. I probably will never use the word myself, but I do like words and etymologies. Thanks.
But here's my big rub. It's not about words but the falseness of the reality behind people who control our lives more and more. I hate it. I feel what is going on here is not just about MOC; it is about everything that we have lost control of in our lives. Is this just me or do you feel that too in your profession and in your life? To be clear about what I mean. I have the startling perception and experience that my life is not my own, if it ever was, and I share in the frustration with these doctors who, I assume like you, are getting the shaft every which way by the governing bodies, measurement assurance forums, CMS, private insurers and so on; the face of medicine today is almost sterile today. And the way I am herded through a mechanized process is not dignified. I have witnessed the loss of so many good doctors like you who do care about their patients and who think for themselves--not just what they are regimented to say and think. Are you a part of such a system or a small group?
No time to say all that disturbs me, but all my docs now are part of a HMO, which I hate. I have no choice. I want diversity of choice. I don't have the opportunity to choose what does not exist anymore. I can't get medications. Not covered anymore. I spend half the time talking on the phone to insurance people who don't know squat. And there is ineptness and corruption behind it all. I grew up on a small farm and a handshake used to be your word. That is gone. You can't believe anybody it seems.
I was asleep when they passed the ACA. Where were you? Description does not match the promised coverage. There seems to be less and less coverage. Is that what is meant by universal. Everyone suffers universally. I trusted the government to do the right thing. Did you fully understand what it would mean? ACA? What does it mean for you as a doctor. I would like to know your thoughts about things. Your points of view so the discussion is not all a one-way road. What does MOC mean to you?
What do I want?
In a world where we seem to have less and less voice in government and medicine, I want you and all physician to have a voice or at least some voice and have it counted. Then I will have my voice back, someone who is listened to.
Physicians are like Rodney Dangerfields today getting little respect. I respect you and that is why I want to know what you think about all this. Put it on your blog, here on your friend Wes' blog, or direct me to where you wrote something.
22,881 internists REJECT the abim MOC and test AACE REJECTS the ABIM MOC and test AAPS has a lawsuit against the ABIM Possible illegal accounting principles Probable illegal 501-c(3)violations Lying about their evidence based proof Exorbitant fees Failing internists to up their retake test money Forcing MDs away from their practice with ridiculous pt mgmt. and voice Support of NBPAS Buying the condo Exorbitant salaries Intimidation (see von muller) And now the AGA rejecting the moc and test
Don't expect the ACC to show the same COURAGE and reject the ABIM and their unreasonable MOC demands despite the undeniably galvanized membership that is in opposition. Never in the history of the ACC, has membership been so united on a subject yet national leadership in ACC refuses to move forward like the gastroenterologists. National ACC has their heads so stuck in the trough of greed taking money from hard working cardiologists and the government to implement policies that are less likely beneficial to the profession and more likely detrimental.
Thank you for sharing AGA's video on twitter. I hate twitter, it's crude, but I watched it happily yesterday when I saw that good women's face.
But then I had to replay it again on your blog to make sure I was not dreaming. Thank you for the good pinch and correcting the typo. I was sure I got her message straight. It hit me hard in the gut and solar plexus with her truth. It is more than a first step in my mind. Listen to her.
I wanted to say a few more things. I did grow up on a farm, even though some would think me dumb for it. But there was a time and place that I remember where people told the truth to each other. You had to. If you did not, you were out of business.
Why???
Everybody depended on one another. That is what I recall. One break in the link and you would lose your crops or livestock. Kids wouldn't eat. The only real insurance we had was each other.
I want that time of honesty and decency back.
I have followed this ABIM scandal here after reading Newsweek in the spring. As a lay person I have learned a lot and appreciate that you will not let these serious allegations of corruption and outlandish examples of obvious lying be ignored.
If you can't trust the value of those folks in Philadelphia, Chicago or Washington they are just like a penny on the railroad track--pretty much useless except as an ornament.
But if those people at the ABIM lied to you, and I believe they did, then they are already out of business. Medicine is a place where if you lie someone dies and that cannot be allowed.
I live in a rural part of America where there are many Medicare and Medicaid patients. Some local hospitals have closed, squeezed out, and the kind of runaround for everything you get now is hurting and killing people already! If the drive does not get you first.
Do you want their names? Do you want my name?
I want more maybe than you all do. The lawn has been mowed too short. I want medicine to grow back. I want some real people back.
The American College of Rheumatology says " WE'VE HAD ENOUGH !!!!!!"
Highlights include strong beliefs that:
• The current ABIM MOC program does not meet the educational needs of rheumatologists and should be modified to allow physicians to develop and implement a continuing professional development plan relevant to his/her professional roles and responsibilities.
• The ABIM should not reinstate the Practice assessment, Patient Voice and Patient Safety requirements as part of the recertification process, because they are redundant with existing requirements that measure and report the quality of care patients receive such as PQRS, Meaningful Use and Value Based Modifier reporting. Additionally, patient voice and patient safety are already assessed by health institutions, accountable care organizations and state and local licensing requirements.
• The secure, closed-book, high-stakes MOC examination should be eliminated, because it is not an appropriate means of assessing clinical knowledge or decision-making for the purpose of recertification.
• The ABIM should fund an independent, external review to examine the performance and impact of its program, including all policies, procedures, organizational structure and governance; and commit to revising the program if the independent evaluation does not identify a substantial benefit to patient care.
The position statement also addresses the redundancy of physicians being required to obtain both CME and MOC medical knowledge credits, the need to reduce program costs, and the desire for evidence the program is improving physician competence.
“We are encouraged by the recent changes the ABIM has made and hope the ABIM will strongly take into consideration the position of the College and our members as it continues to reform the MOC program,” said Joel Block, MD, ACR Committee on Education chair.
From ABIM Blog > Announcements > ABIM’s Design Principles Author: Richard J. Baron, MD, MACP August 27, 2015
Announcements ABIM governance, design principles, MOC We have been seeking ways to improve and support change, and I’m happy to say that a recent result was developing and implementing a set of design principles to guide decision-making at ABIM.
The design principles are grounded in values we’ve gathered from the internal medicine community, and allow for members of the ABIM Board and Council to answer a key question as we move forward with future changes: “Did we get this right?” The principles are organized as short, aspirational and informative guidelines that give ABIM a framework for staying aligned with community values – which include important tenets, such as transparency, involving stakeholders, public interest and fidelity to the internal medicine community’s shared purpose.
I look forward to updating you about further progress as we continue to review, consider and incorporate your feedback and re-examine the MOC program in partnership with the community.
ABIM’s Design Principles:
Shared purpose and impact first. Does the solution align with and advance the internal medicine community’s shared purpose and will it have the desired impact on the community? Patients are the North Star. How does the solution align with the public interest? How is it good for patients? Simplicity and relevancy. Are the solutions easy to understand and applicable to many in the community? Are they relevant? Are they attentive to the burden on and benefit to physicians? Think internal and external. Have both internal and external stakeholders contributed to the solution? Has the impact of the solutions on ABIM and the community been considered? Always include the WHY, the HOW, and the WHO. Will the community understand ABIM’s decision and how it was reached? Balance community-centered design with ABIM’s expertise and research. Have the expert decision makers given appropriate consideration to the possible solutions that emerged from the community? Participation, not just communication. Did ABIM develop solutions with the community and not for them? Will they believe that they had a role in developing the solution? Transparent decisions. Can ABIM easily explain why a particular decision was made and why another possible solution was rejected?
***************
More cotton candy published by Dr. Baron. Sounds great from a superficial view but when you attempt to look for substantive answers to legitimate concerns raised by ABIM diplomates, there is none. I personally would settle for Dr. Baron or any of the ABIM principals to provide a straight answer to just one question: Will ABIM ever consider implementing *any* change that includes a reduction in their revenue stream? From my perspective, Maintenance of Revenue appears to be the only sacrosanct principle at ABIM, everything else is flexible, including ABIM's situational ethics.
16 comments:
Correction to your article. No need to publish this!
"rejection of the high stakes examination after recertification," should read:
"we reject the high stakes examination after initial certification."
There is a big difference for two reasons. She said after initial certification
And the strength of Suzy's words and sentiment "we reject" is important in the live delivery on social media.
Anony 11:07 AM -
Correction made. Thanks for bringing this to my attention.
-Wes
Pledge of a return to integrity by governing bodies.
What Suzanne said was even more significant, because of the emotional strength in which she said it. Without addressing in words the ABIM/ABMS corruption and deceit, it is implied in her tone that she pledges AGA's sustained integrity to serve the physician and not the other way around.
I have painfully discovered at the ABIM/ABMS the physician apparently serves the personal bank accounts of politicians like Chris Cassel, or ABMS board members like Lynn Langdon, who undermine the integrity of what it means to be a medical professional. It is clear that Cassel and other like her have worked to serve personal political agendas, and at the same time inuring themselves beyond what is reasonable for a nonprofit society. It is most likely, from the data I have, these types of corrupted bureaucratic institutions are in service of corporate and government monetary interests and not the public interest. To be clear this is my take. But it is especially poignant when you check the facts for yourself concerning the financial misstatements of the ABIM and the well-rehearsed practice of lying about it and the political cover-up. That is far from transparency.
That is why it is so heartening that the AGA presenter, with clear tone, takes a stand AGAINST 'blatant deviations' which harm practice interests and 'disruptions' of ongoing educational needs of professional working physicians. And I hear a "yes we hear you" voice that is concerned about the disruptive elements in medicine today that are roadblocks to real service to the public.
If I am wrong, Suzy, please correct me on this blog.
The excellent reporter, Wes Fisher, who maintains this 'news blog' has the best gut instinct for truth and falsehood as any reporter I have seen in my life.
I believe, furthermore, Wes would agree with my latter statement that the AGA is taking a stand against corruption of the medical profession and sending a clear message to the bureaucrats who may be in high places, but are completely out of touch with the plain common sense medical reality of today. The spokesperson for the AGA has communicated in her important pre-announcement that physicians will not be deceived again.
The clear voice and the integrity of the person relating this important turning point in the MOC crisis and its significance to the working professional is unmistakable!
Yes, we heard you and the task force's commitment to serve the public trust loud and clear, Suzy!
Read the AACE statement about MOC and lifelong learning as well. They support initial certification only, not MOC. The same strength and integrity. They dropped out of Choosing Wisely also. A very wise choice.
Now it is time for all to stand up and give their real voices as Suzanne in behalf of the AGA has.
The rubes are beginning to self-identify.
The 'devil is the details' but.....
Hopefully the end of ABIM as we know it has begun.
Lynn Langdon must be trying to get a 'golden parachute' added to her contract right now.
Hey Lynn, why don't you apologize for trying to ruin Sarah Von Muller's life?
It really will make you feel better.
Dear Arthur MD,
I am interested to hear what you think. You have a useful blog and I enjoyed your Bob Dylan song. It was fun and creative. Quite good actually. I also appreciated some of the clarifications over medical issues that I, as a patient, would not have thought of reading your blog. I don't care if you rub me wrong by calling me a rube, if that is who you were directing your comment to, and if it is name-calling. Maybe it is just a fun comment. I like it myself because I had to look up the meaning of "rube". I'm still am not clear on it's meaning and origin. Never used the word before. But, I think it applies to me. I am a rube as far as I can tell; so far at least. I did grow up on a farm. Worked hard for my family. Not much time to think. Is that what you meant by rube, a farm girl. I probably will never use the word myself, but I do like words and etymologies. Thanks.
But here's my big rub. It's not about words but the falseness of the reality behind people who control our lives more and more. I hate it. I feel what is going on here is not just about MOC; it is about everything that we have lost control of in our lives. Is this just me or do you feel that too in your profession and in your life?
To be clear about what I mean. I have the startling perception and experience that my life is not my own, if it ever was, and I share in the frustration with these doctors who, I assume like you, are getting the shaft every which way by the governing bodies, measurement assurance forums, CMS, private insurers and so on; the face of medicine today is almost sterile today. And the way I am herded through a mechanized process is not dignified. I have witnessed the loss of so many good doctors like you who do care about their patients and who think for themselves--not just what they are regimented to say and think. Are you a part of such a system or a small group?
No time to say all that disturbs me, but all my docs now are part of a HMO, which I hate. I have no choice. I want diversity of choice. I don't have the opportunity to choose what does not exist anymore. I can't get medications. Not covered anymore. I spend half the time talking on the phone to insurance people who don't know squat. And there is ineptness and corruption behind it all. I grew up on a small farm and a handshake used to be your word. That is gone. You can't believe anybody it seems.
I was asleep when they passed the ACA. Where were you? Description does not match the promised coverage. There seems to be less and less coverage. Is that what is meant by universal. Everyone suffers universally. I trusted the government to do the right thing. Did you fully understand what it would mean? ACA? What does it mean for you as a doctor. I would like to know your thoughts about things. Your points of view so the discussion is not all a one-way road. What does MOC mean to you?
What do I want?
In a world where we seem to have less and less voice in government and medicine, I want you and all physician to have a voice or at least some voice and have it counted. Then I will have my voice back, someone who is listened to.
Physicians are like Rodney Dangerfields today getting little respect. I respect you and that is why I want to know what you think about all this. Put it on your blog, here on your friend Wes' blog, or direct me to where you wrote something.
Thank you in advance for your response.
Lets see...
22,881 internists REJECT the abim MOC and test
AACE REJECTS the ABIM MOC and test
AAPS has a lawsuit against the ABIM
Possible illegal accounting principles
Probable illegal 501-c(3)violations
Lying about their evidence based proof
Exorbitant fees
Failing internists to up their retake test money
Forcing MDs away from their practice with ridiculous pt mgmt. and voice
Support of NBPAS
Buying the condo
Exorbitant salaries
Intimidation (see von muller)
And now the AGA rejecting the moc and test
Did I miss anything?
Don't expect the ACC to show the same COURAGE and reject the ABIM and their unreasonable MOC demands despite the undeniably galvanized membership that is in opposition. Never in the history of the ACC, has membership been so united on a subject yet national leadership in ACC refuses to move forward like the gastroenterologists. National ACC has their heads so stuck in the trough of greed taking money from hard working cardiologists and the government to implement policies that are less likely beneficial to the profession and more likely detrimental.
Dr Fisher,
Thank you for sharing AGA's video on twitter. I hate twitter, it's crude, but I watched it happily yesterday when I saw that good women's face.
But then I had to replay it again on your blog to make sure I was not dreaming. Thank you for the good pinch and correcting the typo. I was sure I got her message straight. It hit me hard in the gut and solar plexus with her truth. It is more than a first step in my mind. Listen to her.
I wanted to say a few more things. I did grow up on a farm, even though some would think me dumb for it. But there was a time and place that I remember where people told the truth to each other. You had to. If you did not, you were out of business.
Why???
Everybody depended on one another. That is what I recall. One break in the link and you would lose your crops or livestock. Kids wouldn't eat. The only real insurance we had was each other.
I want that time of honesty and decency back.
I have followed this ABIM scandal here after reading Newsweek in the spring. As a lay person I have learned a lot and appreciate that you will not let these serious allegations of corruption and outlandish examples of obvious lying be ignored.
If you can't trust the value of those folks in Philadelphia, Chicago or Washington they are just like a penny on the railroad track--pretty much useless except as an ornament.
But if those people at the ABIM lied to you, and I believe they did, then they are already out of business. Medicine is a place where if you lie someone dies and that cannot be allowed.
I live in a rural part of America where there are many Medicare and Medicaid patients. Some local hospitals have closed, squeezed out, and the kind of runaround for everything you get now is hurting and killing people already! If the drive does not get you first.
Do you want their names? Do you want my name?
I want more maybe than you all do. The lawn has been mowed too short. I want medicine to grow back. I want some real people back.
The American College of Rheumatology says " WE'VE HAD ENOUGH !!!!!!"
Highlights include strong beliefs that:
• The current ABIM MOC program does not meet the educational needs of rheumatologists and should be modified to allow physicians to develop and implement a continuing professional development plan relevant to his/her professional roles and responsibilities.
• The ABIM should not reinstate the Practice assessment, Patient Voice and Patient Safety requirements as part of the recertification process, because they are redundant with existing requirements that measure and report the quality of care patients receive such as PQRS, Meaningful Use and Value Based Modifier reporting. Additionally, patient voice and patient safety are already assessed by health institutions, accountable care organizations and state and local licensing requirements.
• The secure, closed-book, high-stakes MOC examination should be eliminated, because it is not an appropriate means of assessing clinical knowledge or decision-making for the purpose of recertification.
• The ABIM should fund an independent, external review to examine the performance and impact of its program, including all policies, procedures, organizational structure and governance; and commit to revising the program if the independent evaluation does not identify a substantial benefit to patient care.
The position statement also addresses the redundancy of physicians being required to obtain both CME and MOC medical knowledge credits, the need to reduce program costs, and the desire for evidence the program is improving physician competence.
“We are encouraged by the recent changes the ABIM has made and hope the ABIM will strongly take into consideration the position of the College and our members as it continues to reform the MOC program,” said Joel Block, MD, ACR Committee on Education chair.
http://www.newswise.com/articles/view/639095/?sc=rsmn
From ABIM Blog > Announcements > ABIM’s Design Principles
Author: Richard J. Baron, MD, MACP August 27, 2015
Announcements ABIM governance, design principles, MOC
We have been seeking ways to improve and support change, and I’m happy to say that a recent result was developing and implementing a set of design principles to guide decision-making at ABIM.
The design principles are grounded in values we’ve gathered from the internal medicine community, and allow for members of the ABIM Board and Council to answer a key question as we move forward with future changes: “Did we get this right?” The principles are organized as short, aspirational and informative guidelines that give ABIM a framework for staying aligned with community values – which include important tenets, such as transparency, involving stakeholders, public interest and fidelity to the internal medicine community’s shared purpose.
I look forward to updating you about further progress as we continue to review, consider and incorporate your feedback and re-examine the MOC program in partnership with the community.
ABIM’s Design Principles:
Shared purpose and impact first. Does the solution align with and advance the internal medicine community’s shared purpose and will it have the desired impact on the community?
Patients are the North Star. How does the solution align with the public interest? How is it good for patients?
Simplicity and relevancy. Are the solutions easy to understand and applicable to many in the community? Are they relevant? Are they attentive to the burden on and benefit to physicians?
Think internal and external. Have both internal and external stakeholders contributed to the solution? Has the impact of the solutions on ABIM and the community been considered?
Always include the WHY, the HOW, and the WHO. Will the community understand ABIM’s decision and how it was reached?
Balance community-centered design with ABIM’s expertise and research. Have the expert decision makers given appropriate consideration to the possible solutions that emerged from the community?
Participation, not just communication. Did ABIM develop solutions with the community and not for them? Will they believe that they had a role in developing the solution?
Transparent decisions. Can ABIM easily explain why a particular decision was made and why another possible solution was rejected?
***************
More cotton candy published by Dr. Baron. Sounds great from a superficial view but when you attempt to look for substantive answers to legitimate concerns raised by ABIM diplomates, there is none. I personally would settle for Dr. Baron or any of the ABIM principals to provide a straight answer to just one question: Will ABIM ever consider implementing *any* change that includes a reduction in their revenue stream? From my perspective, Maintenance of Revenue appears to be the only sacrosanct principle at ABIM, everything else is flexible, including ABIM's situational ethics.
Dr. Baron must be in some delusional state .
22,800 internists say NO MORE MOC AND TEST.
AGA say NO MORE MOC AND TEST.
AACE say NO MORE MOC AND TEST
ACR say NO MORE MOC AND TEST.
And he's talking about improving MOC?
He's "clearly got it wrong.
Dr. Baron , I'm sure you're reading this.
Why don't you post here and post your ideas including POST MOC/POST TEST ideas ?
Can pt. VOICE be far behind?
Here's my *ASSESSMENT 2015*
Dr. Baron refuses to hear 22800 internists.
Lynn Langdon can hide but only the truth will set her free.
MOC (MAINTAINENCE OF CASH).... is DOA.
Secure Exam..... GONE
AGA, AACE and ACR are right.
No, Dr. Wes, the ABIM will not be investigated despite their egregious behavior. Lets see who gets investigated...
http://drwes.blogspot.com/2011/01/doj-investigating-defibrillator.html?utm_source=feedburner&utm_medium=twitter&utm_campaign=Feed:+DrWes+%28Dr.+Wes%29&utm_content=Twitterrific
What makes you think ABIM won't be investigated ? It hopefully will be a moot point as doctors "vote with their feet".
Post a Comment