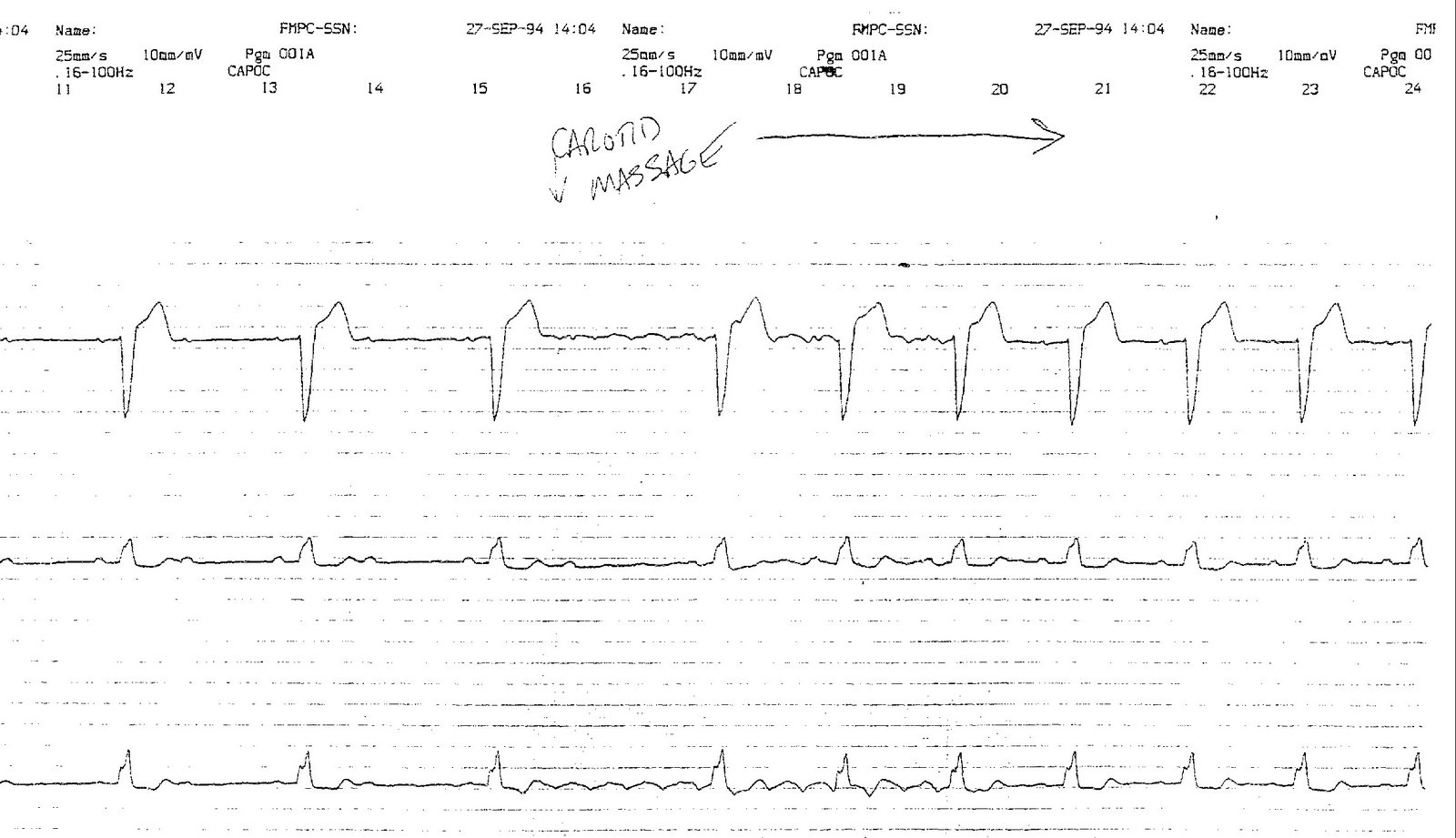
An elderly man presents to the ER for a laceration of his hand and was noted to be bradycardic. An rhythm strip was performed and documented a wide complex, bradycardic rhythm. You are asked to see him.
He was completely asymptomatic, but the ER doctors were concerned and thought he might need a pacemaker. You decide to perform carotid massage, with the results shown:
Click image to enlarge
-Wes
PS: (EP's: please refrain for about 12 hours or so to let others have some fun... thanks!)
13 comments:
Can an ophthalmologist try: Appears to be in 2:1 block at first (cannot see any vertical grid marks so can't tell rate), with p-p interval lengthening with each cycle. Carotid massage drops ventricular rate, and atrial beats return out of sync with what they were before the carotid massage caused the shrt asystolic period. That's as far as I can go with it (Also assume lbbb since name of image is lbbb.jpg)
eyedoc-
For clarification, the carotid massage begins half way through the strip and continues throughout the right half of the rhythm strip shown.
Paramedic here:
Definitely a 2nd degree AV Block. I believe it is Winky based on the response to the Vagal Maneuver. (I've only been reading this blog for a few months, can I assume that youtube video has already been posted?)
From my understanding, the second p wave in each cycle does not conduct to the ventricles as it falls during the Effective Refractory Period of the Action Potential.
The Vagal maneuver slows the stimuli from the SA node, allowing them to fall on either the Relative Refractory Period or afterwards.
The slow repolarization of the AV node is likely due to previous damage. As to whether an asymptomatic man needs a pacemaker? I'll leave that to the experts.
It looked to me as if the carotid massage slowed the sinus rate to the point where you have 1:1 conduction, rather than 2:1.
There is a problem with the conduction system. The sinus node is attempting to initiate beats that, as Yoni wrote, are during the refractory period. By slowing the sinus node, all of the impulses fall outside of repolarization and are conducted. So the rate increases.
How much lidocaine did he receive as a local anesthetic?
If the lidocaine wears off and the heart rate returns to what should be normal, does he need anything else?
Is this likely to happen again without antiarrhythmics on board?
I'm still trying to figure out the reason for a carotid massage...
Initially 2:1 block. Although with 2:1 conduction one can't apply the classic criteria to distinguish type 1 from type 2 block (no consecutively conducted beats seen prior to drop)it's virtually certain this is type 2 evidenced by LBBB. Moreover, type 1 block would get worse with vagal maneuvers.
Tissues at the level of the block (His-Purkenje)have all or none conduction (absolute refractory period). During the initial part of the strip every other atrial impulse falls inside the ARP resulting in 2:1 conduction. CSP slows sinus rate but doesn't affect the ARP. Thus every atrial impulse falls outside the ARP and is conducted. (The vagi don't reach the His-Purkinje cells).
Type 2 block even when asymptomatic requires PPM
One more point I'd like to make---
The more I think about this tracing the more interesting it is. It's a good example of how artificial the concepts of "block" and "degree of block" really are. This patient went from "second degree block" to "no block" although his conduction system did not improve one iota. The lesson is that conduction ratio must always be considered in the context of rate. 2:1 conduction with an atrial rate of 120 means one thing. 2:1 conduction with an atrial rate on 70 means quite another. This is a point Barney Marriott was fond of making many years ago.
rw donnell-
Nice work!
This was an interesting case I encountered some time ago. The clinical question was: is this Mobitz I proximal 2:1 AV nodal block (which might not need a pacemaker) or Mobitz II 2:1 (distal) AV nodal block that should have a pacemaker? In this case, carotid sinus massage was used to differentiate the two forms of AV block.
An easy way to understand this is diagrammed in this figure. Imagine the AV nodal area being represented by two stop lights synchronized to change from red to green when cars pass between them at 35 MPH. If a series of cars (P waves in this instance) approach the first "light" at 40 MPH, they may pass the first stop light, but occassionally one will have to stop before the next stop light turns green again (panel A). If one slows the P waves slightly from 40 MPH to 35 PMH in the proximal AV node (through the use of carotid sinus nassage), then every P wave can pass through BOTH stop lights and make it to the ventricle (Panel B), thereby INCREASING the ventricular heart rate.
This defines the "gap phenomenon" well known to electrophysiologists and is remembered by the mantra: "proximal delay facilitates distal conduction."
The fact that carotid sinus massage facilitates ventricular conduction in this case proves the patient has an abnormal distal His-Purkinje conduction system and is at high risk for the development of higher-degrees of AV block. As such, he should have a permanent pacemaker implanted, even though he was asymptomatic.
Now that, my friends, is the cheapest example of an EP study I can find.
What a great EKG. What is the CPT code for carotid massage? I bet it pays a $1000 bucks. Also, be careful with the Bundle of His. You don't want any feminists claiming discrimination. How about the gender neutral Bundle of Hermy
Almost tried this on a pt today to put my new found knowledge into practice.
Saw him in nuc med for his p-myo.
He was in 2:1 AV block with a rate in the mid 40s. Really wanted to try the carotid massage, but decided I couldn't justify it because he already has a pending appt for pacer implantation.
CardioNP
Wes-
Great ECG, and an EP classic. I would add that while the response to carotid sinus massage confirms the diagnosis, it really is not absolutely necessary--there is enough information even in the 2:1 block segment. Specifically, proximal block in the AV node is a phenomenon of high vagal tone (assuming you're not in the EP lab pacing the atrium at really fast rates). In this case, the sinus rate during 2:1 block is 85bpm, and thus not consistent with a high vagal tone state. Hence block must be distal, not proximal.
Ted Chow
Nice ECG and good explanation in the comments!
Good Job! :)
Post a Comment