Want to win an iPod Nano? Head on over to Medgadget and take a guess at who will be the new Nobel prize winners in science. You could win a much-coveted iPod Touch.
(For the brilliant readers of this blog who feel they would qualify, I won't tell if you nominate yourself.)
-Wes
Wednesday, September 30, 2009
Could Health Care Help Fund the 2016 Olympics?
While is it convenient for journalists and policy pundits to constantly point fingers at doctors who order too many tests as the sole cause of the explosion in health care costs, we must not forget other reasons our health care costs in Chicago might be uniquely situated to assist in that process.
- It is an inconvenient truth that the city of Chicago has the highest total sales tax of all major U.S. cities. It is also one of the most complex. 10.25% is levied on all non-perishable goods purchased, while 2% is levied on qualifying food, drugs, medicines and medical appliances.
- Chicago health care, although principally run by "non-profit" health systems sheltered in many ways from large tax obligations, is still "taxed" through secretly cloaked "hospital assessments" on gross revenues folded into insurance payments made to the hospitals. This asessment was approved recently by none other than the federal government whose commander in chief is serving as the Principle Spokesperson to promote the 2016 Olympic games.
- Chicago has, and continues to have, an almost limitless ability to add billion dollar health care facilities to its metropolis. Construction projects have historically been the thing of big unions, and no one knows big unions like health care. While many of these facilities have been substantally supported through philanthropic doles at their outset, the amount of money required to "keep the lights on" at such huge, expensive facilities mandates that beds be full and admissions processed. Need I say more?
- With the increasing consolidation of health care, especially in the lucrative, higher-income areas of Chicago, the ability of insurers to demand concessions on health care pricing has dwindled. Further, the adoption of the electronic medical record (EMR) has profited health care systems greatly by reducing insurance claim denials and shortening the times accounts are in collections. This leads to more revenue, which in turn, leads to more construction. More contruction leads to more... well, you know.
- And last, but not least, are hospital parking rates. I challenge just about any city in the nation to find rates as high as ours. Oh, and those rates are taxed by the City of Chicago.
-Wes
Monday, September 28, 2009
Drilling Down On Cardiology Cuts
Currently, cardiologists are on a treadmill of increasing patient visits to offset declining Medicare payments and increasing overhead. When the government plans on blanket cuts to cardiologists in favor of primary care, the impact will be felt first by those in rural areas that already have a shortage of cardiologists. Then will come pressure on small town practices as they are forced to close. Bigger cities with large health systems will be least affected.
But this is all part of the Grand Plan of health care physician reform: make sure everyone gets insurance so they can "prevent" cardiovascular disease while those that have it can't find a specialist.
I see how this works.
-Wes
But this is all part of the Grand Plan of health care physician reform: make sure everyone gets insurance so they can "prevent" cardiovascular disease while those that have it can't find a specialist.
I see how this works.
-Wes
Sunday, September 27, 2009
The Final Opus
It was midnight and the Emergency Room door opened like a curtain on a Broadway. A lone man sat in blue at the countertop, writing. Behind him, the chorus, working feverishly on the protagonist - the script rehearsed a thousand times before.
Clothes off, Story?, facemask, C-collar, endotracheal tube, breath sounds, telemetry, IV’s, blood work, pulse ox, Stop.
Resume, Pulse?, patches, register, call the lab, Allergies?, epi, atropine, Pressure?, twitching, NG, x-ray, Stop. Pulse?
Resume, pacing wire, max output, capture?, not quite, “potassium?”, not ready, blood gas, foley, Capture! Stop.
Resume, blood gas, no capture, damn, tweak, better, pulse?, yes. Lab?, no, Which meds?, cardiologist, Go.
Vent, hoist, prep, stick, contrast, open, shock, balloon pump, a-line, movement, labs, blood gas, peep, transport, c-spine, CT, Go.
Then intermission.
It’s hard to imagine the enormity and speed of it all. The cast. The direction. The audience in the hall. The cast of characters working together in hopes of seeing a small glimmer of life. From the man in blue who arrived there first, seeing the terrified look on the woman’s face, to the orderly that swept the floor as the curtain fell once more, I wondered.
It’s a strange thing, this concert: brutal, raw, exciting, exhausting. Drama, romance and tragedy together. It’s a story told a thousand times at the world’s most expensive theaters across the country. And as doctors, we receive a free pass backstage to witness, first hand, a drama like no other. Yet despite that privilege and exclusivity, none of us knows how the play will ultimately end.
More often than not, the story ends sadly as the Playwright predicted. The play, sometimes, goes on too long. But before the final curtain is called, the brief respite from the inevitable lends solace to the bereaved as they gather friends and family to reflect on remarkable chapters before them. Finally, with tears and the hugs, quiet descends and the the stage emptied while the cast of characters never hear their much deserved applause.
-Wes
Clothes off, Story?, facemask, C-collar, endotracheal tube, breath sounds, telemetry, IV’s, blood work, pulse ox, Stop.
Resume, Pulse?, patches, register, call the lab, Allergies?, epi, atropine, Pressure?, twitching, NG, x-ray, Stop. Pulse?
Resume, pacing wire, max output, capture?, not quite, “potassium?”, not ready, blood gas, foley, Capture! Stop.
Resume, blood gas, no capture, damn, tweak, better, pulse?, yes. Lab?, no, Which meds?, cardiologist, Go.
Vent, hoist, prep, stick, contrast, open, shock, balloon pump, a-line, movement, labs, blood gas, peep, transport, c-spine, CT, Go.
Then intermission.
It’s hard to imagine the enormity and speed of it all. The cast. The direction. The audience in the hall. The cast of characters working together in hopes of seeing a small glimmer of life. From the man in blue who arrived there first, seeing the terrified look on the woman’s face, to the orderly that swept the floor as the curtain fell once more, I wondered.
It’s a strange thing, this concert: brutal, raw, exciting, exhausting. Drama, romance and tragedy together. It’s a story told a thousand times at the world’s most expensive theaters across the country. And as doctors, we receive a free pass backstage to witness, first hand, a drama like no other. Yet despite that privilege and exclusivity, none of us knows how the play will ultimately end.
More often than not, the story ends sadly as the Playwright predicted. The play, sometimes, goes on too long. But before the final curtain is called, the brief respite from the inevitable lends solace to the bereaved as they gather friends and family to reflect on remarkable chapters before them. Finally, with tears and the hugs, quiet descends and the the stage emptied while the cast of characters never hear their much deserved applause.
-Wes
Wednesday, September 23, 2009
Doctor Payment Reform
It's the holy grail of physician payment reform: ending fee-for-service payments to doctors and, instead, pay doctors based on the quality of care they perform. Remarkably, Congress feels they've found the answer:
... how do we define "quality?"
Medicare has historically withheld payments to physicians unless they performed lock-step "quality measures" before granting release of the remainder of 1.5 percent of the doctors' payments that were billed. Needless to say, this model has been an abysmal failure (subscription) at improving the "quality" of care delivered and has been very expensive to implement. Further, others have noted the challenge of measuring quality on the basis of clinical outcomes.
But this has not dissuaded our legislators from forcing the "quality issue." No, they have proposed to find a fix by the creation of a hugely expensive C.M.S. Innovations Center:
Perhaps I'm too cynical, but I think the subliminal message coming from Washington so far is really this: doctors should be happy becoming salaried employees of larger health systems. This way, the government can pay the health system a bundled fee and the doctors can fight for their share of the kitty.
So far, this seems to be how the government will envision "quality" at an affordable price in the years to come.
I just wonder how many doctors will stick around to find out.
-Wes
Thus, the new language in the Senate Finance bill would finally connect Medicare reimbursements to quality, as opposed to volume.Wow. That sounds great! But there's just one problem...
The measure gives the secretary of Health and Human Services, working with the Centers for Medicare and Medicaid Services, the power to develop quality measurements and a payment structure that would be based on quality of care relative to the cost of care. The secretary would have to account for variables that include geographic variations, demographic characteristics of a region, and the baseline health status of a given provider's Medicare beneficiaries.
The secretary would also be required to account for special conditions of providers in rural and underserved communities.
Additionally, the quality assessments would be done on a group-practice level, as opposed to a statewide level. Thus, the amendment would reward physicians who deliver quality health care even if they are in a relatively low quality region.
The secretary of Health and Human Services would begin to implement the new payment structure in 2015. By 2017, all physician payments would need to be based on quality.
... how do we define "quality?"
Medicare has historically withheld payments to physicians unless they performed lock-step "quality measures" before granting release of the remainder of 1.5 percent of the doctors' payments that were billed. Needless to say, this model has been an abysmal failure (subscription) at improving the "quality" of care delivered and has been very expensive to implement. Further, others have noted the challenge of measuring quality on the basis of clinical outcomes.
But this has not dissuaded our legislators from forcing the "quality issue." No, they have proposed to find a fix by the creation of a hugely expensive C.M.S. Innovations Center:
"It would be funded with $10 billion over the next several years to implement pilot projects and demonstrations to promote new payment reform opportunities. There are quite a few problems with the bill, but this provision is truly visionary. The House legislation, HR 3200, mentions payment reform, but it [provides] only modest funding of $275 million. That’s not enough.I suppose $10 billion compared to $275 million is "truly visionary" if you stand to receive the funds. One wonders what the tax payers will get at the end of the day for this grotesque amount of money.
Perhaps I'm too cynical, but I think the subliminal message coming from Washington so far is really this: doctors should be happy becoming salaried employees of larger health systems. This way, the government can pay the health system a bundled fee and the doctors can fight for their share of the kitty.
So far, this seems to be how the government will envision "quality" at an affordable price in the years to come.
I just wonder how many doctors will stick around to find out.
-Wes
Sunday, September 20, 2009
The Challenge of Health Care Reform
... was eloquently outlined by economist N. Gregory Mankiw, in his article that appeared in the New York Times this morning. He uses the primary prevention of heart disease by taking daily statin drugs to lower cholesterol to make his point about the costs of prevention that leads him to ask a central, but very complicated, question festering in the background of much of the health care debate:
Until then, special interests will continue to wield far too much influence (and price pressure) over those most affected most by the health care delivery transaction.
-Wes
"Despite all the talk about waste and abuse in our health system (which no doubt exists to some degree), the main driver of increasing health care costs is advances in medical technology. The medical profession is always figuring out new ways to prolong and enhance life, and that is a good thing, but those new technologies do not come cheap. For each new treatment, we have to figure out if it is worth the price, and who is going to get it.In answer to his Big Question, I'd vote for the consumer (and I mean the patient rather than hospitals) since they have to pay the tab one way or the other. To that end, price transparency of goods and services should be required for anyone involved in health care delivery. In short, every effort should be made to empower patients in such complicated decision making.
The push for universal coverage is based on the appealing premise that everyone should have access to the best health care possible whenever they need it. That soft-hearted aspiration, however, runs into the hardheaded reality that state-of-the-art health care is increasingly expensive. At some point, someone in the system has to say there are some things we will not pay for. The big question is, who? The government? Insurance companies? Or consumers themselves? And should the answer necessarily be the same for everyone?"
Until then, special interests will continue to wield far too much influence (and price pressure) over those most affected most by the health care delivery transaction.
-Wes
Which Is It: Self-Referral or Gainsharing?
A series of fines have been levied in New Jersey for various fraudulent practices that might have a chilling impact on the way hospital systems do business:
But an even more perplexing problem is posed if there are competing groups vying for the services of one lucrative hospital laboratory, these same "directors" may be perceived as skewing the availability of lab time toward their groups, creating a source of friction for their competition. The defense of such a case can get very expensive for a hospital system.
But just when it appears doctors are starting to get the message about such arrangements, comes a new form of legal kickback: "gain-sharing." Gosh, I don't know why all of this is confusing, do you?
Could this be part of the government's upcoming strategy to save "$500 billion" in Medicare fraud costs? If so, it appears figuring out what is legal and what's not will continue to be next to impossible for physicians, and when there's a need for cash, well, it appears the side with the larger bankroll will win.
But if there's one takeaway from all of this: doctors and hospitals might want to carefully scruitinize their current consulting/employment arrangements.
After all, the government's a little short of cash right now.
-Wes
The doctors -- Ravindra Patel of Scotch Plains, Jasjit Walia of Edison and Rakesh Sahni of Rumson -- agreed to pay a combined $960,000, representing twice the annual salaries they received from the University of Medicine and Dentistry of New Jersey, according to Ralph J. Marra, acting U.S. attorney for New Jersey.Many hospital systems pay non-employed specialist physicians from the surrounding community as "directors" of various specialty departments. In the case of cardiologists or gastroenterologists, one such role might be as "Director of the Catheterization Laboratory" or "Director of the GI Laboratory." Such directors reportedly play a role in assuring proper staffing, scheduling, or as training resources for nurses or technicians. But if no work actually occurs by the contracted physician in kind, then the government can move in. It appears this was the case in New Jersey.
Lawyers for the cardiologists were unavailable for comment last night.
Federal law prohibits doctors from accepting payments in exchange for referring patients. Beginning in 1996, authorities say University Hospital began trying to increase the number of cardiac procedures it performed by offering salaries to doctors in private practices in exchange for referrals.
A criminal inquiry into the program began after a federal monitor -- former U.S. Attorney Herbert J. Stern -- charged many of the doctors were given no-show faculty jobs. Most had few if any research credentials, and few actually taught, authorities said.
But an even more perplexing problem is posed if there are competing groups vying for the services of one lucrative hospital laboratory, these same "directors" may be perceived as skewing the availability of lab time toward their groups, creating a source of friction for their competition. The defense of such a case can get very expensive for a hospital system.
But just when it appears doctors are starting to get the message about such arrangements, comes a new form of legal kickback: "gain-sharing." Gosh, I don't know why all of this is confusing, do you?
Could this be part of the government's upcoming strategy to save "$500 billion" in Medicare fraud costs? If so, it appears figuring out what is legal and what's not will continue to be next to impossible for physicians, and when there's a need for cash, well, it appears the side with the larger bankroll will win.
But if there's one takeaway from all of this: doctors and hospitals might want to carefully scruitinize their current consulting/employment arrangements.
After all, the government's a little short of cash right now.
-Wes
Saturday, September 19, 2009
Repeating History?
After the recent collapse of the stock market created by the sub-prime mortgage mess, my jaw dropped when I saw this sign promoting the "FHA's Purchase Stimulus Act of 2009" (I think they mean the American Recovery and Reinvestment Act of 2009) as I left work today:

No wonder people love government-sponsored programs. They're all about "free money."
-Wes
No wonder people love government-sponsored programs. They're all about "free money."
-Wes
Friday, September 18, 2009
The Constitutionality of Mandates
The requirement that people who do not purchase insurance will be fined by our government may not be Constitutional:
-Wes
(In all major health reform bills proposed so far), those who don’t buy insurance would be required to pay a penalty, according to the various health proposals. But this mandate isn’t so much a regulation as a “tax,” and Congress shouldn’t be allowed to tax people just because they are uninsured, argue David Rivkin and Lee Casey, who served in the Justice Department during two Republican administrations. Otherwise, Congress could institute similar “taxes” on anyone who doesn’t follow other orders, such as joining a health club or exercising regularly, they point out.Good point.
-Wes
Thursday, September 17, 2009
OR Fires and Pacemaker Implants
"What we've been advocating for years is that the open delivery of oxygen under the drapes essentially has to stop," with some exceptions such as cardiac pacemaker surgery or operations involving a neck artery, Bruley said.
Most pacemaker and defibrillator implants I know occur with one side of the drape lifted, so the patient can see and interact with the nurse or anethesiologist during a pacemaker or defibrillator implant and oxygen cannot collect beneath the drape. But in the case of a patient being draped so the drape remains completely covering the patient's face during deeper sedation, I could see how such a horrible thing could happen.
Sheesh. Be careful out there.
-Wes
XBox 360 Helps Heart Researchers
 Need good graphics for a research project modeling the electrophysiology of myocardium? Well, sometimes the best ideas come from adapting existing technology used for the gaming community:
Need good graphics for a research project modeling the electrophysiology of myocardium? Well, sometimes the best ideas come from adapting existing technology used for the gaming community:Dr Simon Scarle, a researcher on the Warwick team, used a single Xbox 360 Graphical Processing Unit (GPU) to model how electrical signals were transmitted through damaged heart cells.Maybe this is how we can start to recruit more teens for the basic sciences...
The chip is able to perform parallel processing at a fraction of the cost of a dedicated "cluster" system or a network of PCs.
Dr Scarle said: “You don't quite get the full whammy of a cluster, but it’s close.
"Instead of pumping out stunning graphics, it's reworked; in the case of my research, rather than calculating the position of a structure and texture it's now working out the different chemical levels in a cell."
-Wes
Wednesday, September 16, 2009
Four Digits
It came across my pager (names changed, of course):
At this point I've spent way too much time attempting to answer the page, and am about to give up, when I have an idea. I checked all of the wards I usually travel for a "Ms. Smith." Soon, I find an eligible candidate and note that she's on the surgical floor. I call that floor's number and a nice nurse answers:
Not long ago, to call a phone number in the Chicago area we had to start using the area code in conjunction with the regular seven-digit phone number to place a call due to the exploding number of cell phones being issued. More area codes were quickly added, and communications have fourished.
With the increased consolidation of hospitals to larger health systems, the ability to quickly connect to a specific extension is becoming problematic, especially when we include pager numbers, cell numbers, and ward extentions to the mix.
Simply put: it's death by four digits now.
Suggestion: "Seven is heaven."
-Wes
"Please call Sally 3050 re: Ms. Smith"I called:
"This is OB/GYN, may I help you?"So the call is made. This time, no answer. So I call the Operator:
"May I speak with Sally, please?"
"I'm sorry, there's no Sally here."
"Thanks, I'll try Hospital #2"
"Operator, how may I help you."And so I was connected. It rings and rings and rings. Once again, no answer.
"Yes, can you tell me where extension 3050 is?"
"Um, looks like OB/GYN."
"Whaaaat?" (My mind raced. Who did I see on the OB service??? I had no clue.)
"Um, sorry, I already called them. They didn't know anyone there by the name of Sally."
Operator: "Would you like me to connect you with Hospital #3, maybe they have that extension."
"Yes, please."
At this point I've spent way too much time attempting to answer the page, and am about to give up, when I have an idea. I checked all of the wards I usually travel for a "Ms. Smith." Soon, I find an eligible candidate and note that she's on the surgical floor. I call that floor's number and a nice nurse answers:
"Surgical floor, this is Kerry, can I help you?"Then it hits me once again.
"Yes, are you taking care of Ms. Smith?"
"Yes, I am."
"I was called to a 3050 by Sally, is she there?"
"Nooooo. No one here by that name. Uh, wait a minute, isn't that the resident's pager number?"
Not long ago, to call a phone number in the Chicago area we had to start using the area code in conjunction with the regular seven-digit phone number to place a call due to the exploding number of cell phones being issued. More area codes were quickly added, and communications have fourished.
With the increased consolidation of hospitals to larger health systems, the ability to quickly connect to a specific extension is becoming problematic, especially when we include pager numbers, cell numbers, and ward extentions to the mix.
Simply put: it's death by four digits now.
Suggestion: "Seven is heaven."
-Wes
Tuesday, September 15, 2009
Beware of Computer-directed Lemmings
Older man with demenia falls, hits head.
Wife: "Arnie, Arnie are you all right?" Arnie just mumbles.
Heart rate slow, blood pressure low - paramedics give atropine - heart rate better, blood pressure not so. Comes to ER.
CT of head/neck done - okay. Hemoglobin 9.2
Junctional rhythm, narrow escape.
Patient confused.
Patient admitted.
Lovenox given.
Flu shot administered.
"Um, lovenox?"
"Yep, I saw the DVT alert!"
"Was there a hemorrhage alert, too?"
"Hmmm, I didn't see one..."
-Wes
Wife: "Arnie, Arnie are you all right?" Arnie just mumbles.
Heart rate slow, blood pressure low - paramedics give atropine - heart rate better, blood pressure not so. Comes to ER.
CT of head/neck done - okay. Hemoglobin 9.2
Junctional rhythm, narrow escape.
Patient confused.
Patient admitted.
Lovenox given.
Flu shot administered.
"Um, lovenox?"
"Yep, I saw the DVT alert!"
"Was there a hemorrhage alert, too?"
"Hmmm, I didn't see one..."
-Wes
Boston Scientific's Ultra-Soft Device Advisory
 How do you notify people gently about a device alert that doesn't involve an implanted device, but rather a monitoring device developed for the implanted device? Where does a sophisticated implanted defibrillator device end: with the part that's implanted inside a patient or does it include the peripherals that monitor the implanted device, too?
How do you notify people gently about a device alert that doesn't involve an implanted device, but rather a monitoring device developed for the implanted device? Where does a sophisticated implanted defibrillator device end: with the part that's implanted inside a patient or does it include the peripherals that monitor the implanted device, too?These are the issues that have surfaced with a very recent medical device advisory issued by Boston Scientific on 9 September 2009 in a "Dear Doctor" letter (pdf) I managed to find on their website, and was brought to my attention by an anonymous commenter on this blog:
BackgroundHopefully, all patients with these Communicators have been notified, but how are device clinic nurses and physicians supposed to be notified? I checked with our device clinic nurses and they were unaware of this advisory - is it because we have no patients included in this advisory? (I'm not sure). But what I do know is that the potential to miss clinically important information when we increasingly rely on color-coding of parameters on websites to identify out-of-range parameters is something every doctor and device nurse should be made aware, especially since patients move from one location to another or might not have received notification about their communicator.
Boston Scientific defibrillators include a Daily Measurements feature that conducts several diagnostic tests on a daily basis to monitor the implanted defibrillator and leads. At the next in-clinic visit, test results are displayed on the programmer, with out-of-range results appropriately highlighted.
To supplement in-clinic visits, the LATITUDE Patient Management system enables clinicians to monitor the status of the implanted system remotely between clinic visits. Status information from the implanted defibrillator is transferred by an in-home communicator to the LATITUDE Website according to a schedule set by the clinician. If Daily Measurements are programmed On in the implanted defibrillator (nominally On) and the desired Alerts are configured On in LATITUDE, out-of-range Daily Measurements will generate a corresponding Red or Yellow Alert on the LATITUDE Website.
Description
Boston Scientific has determined that alert conditions for a limited subset of out-of-range Daily Measurements related to leads may not be recognized by Model 6476 (United States) or Model 6468 (Europe) LATITUDE in-home communicators. If a communicator fails to recognize a valid alert situation, notification for this or subsequent alerts for the same test will not be displayed for physician review on the LATITUDE Website. However, Daily Measurement values uploaded from the implanted defibrillator will be available from the ALL PATIENTS page after completion of the next full device interrogation, which occurs during Weekly Device Alert Interrogations and scheduled remote follow-ups.
Although a limited subset of alerts may not display on the LATITUDE Website, it is important to note that all Daily Measurement tests within the implanted defibrillator function normally, and results will be displayed as designed when the defibrillator is interrogated with a programmer.
Rate of Occurrence
We have identified 8 missed Red Alerts and 223 missed Yellow Alerts from approximately 19,000 patients in the United States with implanted Boston Scientific defibrillators followed with a LATITUDE Model 6476 Communicator. One missed Yellow Alert has been identified from approximately 50 patients in Europe followed with a LATITUDE Model 6468 Communicator. However, root cause analysis indicates that both communicators are subject to missed alerts at the same rate of occurrence. The observed rate for a missed Red Alert (highest priority) has been approximately 0.01% per month of monitoring. No patient deaths or injuries have been associated with this communicator behavior.
Whether a targeted letter posted on a company's website is adequate notification to electrophysiology personnel nationwide about this type of advisory, whether it affects our patients directly or not, probably is not adequate either.
After all, we're ultimately responsible to our patients.
-Wes
Monday, September 14, 2009
ICDs in Women: The New York Times Gets It Wrong
If there are potential "shortcomings in the data," then you shouldn't print a misleading title: "Survey Shows Heart Device Aids Men More Than Women." Rather, a better title would have been, "More Data are Needed to Understand the Effectiveness of Defibrillators in Women." Do we really want to withhold defibrillators from women on the basis of such a retrospective literature meta-analysis?
But then, it's the New York Times.
A much better review, including a comment on the study in question by yours truly and fellow EP blogger Dr. Rich Fogoros, can be found over at Larry Husten's Cardiobrief blog.
-Wes
But then, it's the New York Times.
A much better review, including a comment on the study in question by yours truly and fellow EP blogger Dr. Rich Fogoros, can be found over at Larry Husten's Cardiobrief blog.
-Wes
Another Cool ICD Tattoo
A friend of one of our device nurses who has an implantable cardiac defibrillator (ICD) had a truly reflective moment recently when she tried to decide what would be a cool tattoo to don. She saw one of our t-shirts and used it as an inspiration for her tattoo. I must say, I like her design better:

Heh.
-Wes
Heh.
-Wes
Sunday, September 13, 2009
Circular Reasoning
Here's a dumb thought: If you want to save costs on medical devices to the federal government, require a tax fee concessions of $4 billion dollars from the medical device companies to fund a health care overhaul.
Now either that $4 billion will get added to the cost of devices (and the patient/insurer's tab) or the device companies will decide that they must pay the fee to maintain their current pricing.
Government pressures hospitals and doctors by paying less, so hospitals keep the heat on medical device makers to lower costs so they can make their margins.
It all sounds good, right?
But according to one analyst, it seems device makers would rather pay the fee than make their prices transparent:
Why do the patients always seem to lose with these government-mandated scenarios?
-Wes
Now either that $4 billion will get added to the cost of devices (and the patient/insurer's tab) or the device companies will decide that they must pay the fee to maintain their current pricing.
Government pressures hospitals and doctors by paying less, so hospitals keep the heat on medical device makers to lower costs so they can make their margins.
It all sounds good, right?
But according to one analyst, it seems device makers would rather pay the fee than make their prices transparent:
But the mechanism for how devices companies might pay matters more than what they pay, according to Morgan Stanley analyst David Lewis. "A 'flat tax' is preferable, in our view, to targeted industry fees as our larger concern is the creation of more infrastructure intended to catalyze pricing transparency," he said.And so, with the fee, the government pays itself while the medical device prices continue to remain inflated.
Why do the patients always seem to lose with these government-mandated scenarios?
-Wes
Friday, September 11, 2009
The Importance of Blogs and Device Advisories
Yesterday, I reported on this blog the trouble Medtronic had experienced with and earlier batch of defibrillators due to a low-voltage capacitor problem from an outside supplier back in 2005 or 2006. The problem was identified in a relatively small number of devices and has not affected their devices' functionality, but the expected battery life of these batch of devices was discovered to be shorter than they had expected. A root cause analysis was undertaken and the capacitor issue was identified. After consulting their physician advisory panel, they elected to notify all doctors who implant their devices about the issue and provided the patients' names that they were aware of to doctors to help facilitate patient notification.
Importantly, there was not a press release.
Personally, I think this was a good thing. As of this moment, I was only able to find one reference to this advisory in once major newspaper, the Wall Street Journal. No doubt, the news will spread rapidly from there.
But it will not spread like a press release would: fired instantaneously to every news organization around the globe always looking for the next tidbit to report, especially tidbits that create lots of angst. Importantly, the piece from the Wall Street Journal did not include a hyperlink where patients would look up if their device was affected.
It has been interesting to also see who has been reading my blog post on this matter. Sitemeter is handy for that. At first, it was lots of hits from medtronic.com, but not too soon thereafter came guidant.com, bostonscientific.com, and the like.
There is no question that these device manufacturers are fierce competitors. As such, let's just say they like to keep things relatively private between themselves. But these device manufacturers may also use the same outside vendors for supplies, including low-voltage capacitors in their circuitry and maybe, just maybe, by getting the information out about one manufacturer's design problem, others will check their old devices as well.
So while blogs have been controvertial for their ability to spread news, good or bad, at lightning speed, the fact that they don't appear at first on the Nightly News or front page of major newspapers might just be a good thing while effectively communicating the issues to our patients (and other interested parties) without terrorizing the masses.
-Wes
Importantly, there was not a press release.
Personally, I think this was a good thing. As of this moment, I was only able to find one reference to this advisory in once major newspaper, the Wall Street Journal. No doubt, the news will spread rapidly from there.
But it will not spread like a press release would: fired instantaneously to every news organization around the globe always looking for the next tidbit to report, especially tidbits that create lots of angst. Importantly, the piece from the Wall Street Journal did not include a hyperlink where patients would look up if their device was affected.
It has been interesting to also see who has been reading my blog post on this matter. Sitemeter is handy for that. At first, it was lots of hits from medtronic.com, but not too soon thereafter came guidant.com, bostonscientific.com, and the like.
There is no question that these device manufacturers are fierce competitors. As such, let's just say they like to keep things relatively private between themselves. But these device manufacturers may also use the same outside vendors for supplies, including low-voltage capacitors in their circuitry and maybe, just maybe, by getting the information out about one manufacturer's design problem, others will check their old devices as well.
So while blogs have been controvertial for their ability to spread news, good or bad, at lightning speed, the fact that they don't appear at first on the Nightly News or front page of major newspapers might just be a good thing while effectively communicating the issues to our patients (and other interested parties) without terrorizing the masses.
-Wes
Thursday, September 10, 2009
A New Medtronic Defibrillator Advisory Issued Today
Today, an announcement was issued to doctors implanting Medtronic's Concerto and Virtuoso wireless implantable cardiac defibrillator's (ICDs) that a certain lot of 5,200 devices in the US of the total 158,000 implanted worldwide have demonstrated premature battery depletion due to a faulty battery capacitor containing porous copper. A total of 230 devices returned so far have demonstrated this problem. The capacitor was manufactured by an outside vendor, and more recent models of these devices manufactured reportedly no longer have this capacitor.
The notification is not a recall and does suggest any of the devices have failed and no deaths have been reported as a result of this notification. It is recommended that physicians continue the routine follow-up of these devices every three months and the patient alert feature be programmed "ON-High" for the Low Voltage Battery alert.
You can look up specific serial numbers of Concerto biventricular defibrillators(Model C154DWK) or Virtuoso DDDR defibrillators (Model D154AWG) models that might be affected at http://CVSNList.medtronic.com.
-Wes
The notification is not a recall and does suggest any of the devices have failed and no deaths have been reported as a result of this notification. It is recommended that physicians continue the routine follow-up of these devices every three months and the patient alert feature be programmed "ON-High" for the Low Voltage Battery alert.
You can look up specific serial numbers of Concerto biventricular defibrillators(Model C154DWK) or Virtuoso DDDR defibrillators (Model D154AWG) models that might be affected at http://CVSNList.medtronic.com.
-Wes
Wednesday, September 09, 2009
On the President's Health Care Address

I just finished watching the well-delivered, but frankly heavily partisan, health care reform speech by President Obama. After seeing it, I did not think it was a game changer, but no doubt others will be wooed by the authoritative tone set by the President. The speech was clearly not aimed toward the Republicans in the Congress but rather appeared, in my view, to be a warning shot and "call to action" to the conservative and moderate Blue Dog Democrats as the President struggles to win their support of the Public Option and his plan for health care reform. Hard to see the Republicans nuzzling up to the President at this point and the strategy seems to have shifted to getting a bill through by reconciliation.
There were good points made early and late in the speech, like the need for reform and the need to provide insurance options to those who cannot afford it, making the denial of pre-existing conditions illegal, and even the requirement that insurers can't cancel coverage mid-way. But these reforms were no-brainers. And while there was no question that the best part of the speech was the heartfelt memory of Ted Kennedy through a letter he wanted opened after his death that reinforced his desire to define the "character" of the country through this initiative, there were some glaring problems with the speech as well.
First, I thought the President did a poor job as he spoke "directly" to seniors, convincing them how the hundreds of billions of cost savings he proposed to discover in Medicare and Medicaid would not affect their benefits in the program. Simply put, our seniors are smarter than that. This remains a major problem for the President and the reform efforts underway.
More importantly for doctors, there was the issue of medical malpractice reform. It was interesting to review what the President actually said:
Now finally, many in this chamber, particularly those of the Republican side of the aisle, have insisted that reforming medical malpractice laws will bring down the cost of health care. (Republican side of the aisle finally applauds, to which the President points out: "There you go. There you go." and then continues.)That was it. Medical malpractice reform by putting patient safety first. You could see the members of Congress sitting there somewhat stunned and with puzzled looks on their faces. They weren't sure if they should clap or not.
Malpractice law is not a silver bullet. I have talked to enough doctors to know that defensive medicine may be contributing to unnecessary costs.
So... so, I am proposing that we move forward on a range of ideas to put patient safety first and let doctors focus on practicing medicine. I know that the Bush administration authorized demonstration projects in individual states to test these ideas. I think that is a good idea and I am directing my Secretary of Health and Human Services to move forward in this initiative today.
But a quick check on what the President was referring to can be found in the medical literature. In 2006, Hilary Clinton and Barack Obama co-authored a "perspective" piece published in the New England Journal of Medicine entitled "Making Patient Safety the Centerpiece of Medical Liability Reform." (Note: I have discussed my concern regarding the use of medical journals for political commentary previously). In this article, Clinton and Obama stated:
Instead of focusing on the few areas of intense disagreement, such as the possibility of mandating caps on the financial damages awarded to patients, we believe that the discussion should center on a more fundamental issue: the need to improve patient safety.So there you have it. It will be medical liability reform through more safety supervisors, hand soap dispensers, operative "time outs" and hall monitors. No unseemly caps on financial damages. Boy, the Bar Association members must be giving each other "high fives" for how well the President handled that part of his speech, don't you think?
But despite all this, an even more surprising and memorable moment came when the President promised not to pay for coverage of illegal aliens in any government health care reform bill and a Republican Congressman blurted out so all could hear, "You lie!" The Democratic side of the aisle immediately booed the vocal Republican Congressman. The look on Nancy Pelosi's face as she sat befuddled behind the President following the outburst was, as they say, priceless. And while this was a tense moment that passed quickly, it reinforced the passionate nature of the debate for all Americans and served as a reminder of how hard it will be to pass any bill of this scope and magnitude.
-Wes
Photo credit: Whitehouse.gov
What We Won't Hear Tonight
President Obama plans to spell out this vision of health care reform to the US in a nationally televised address to both houses of Congress tonight. His speech represents a defining moment in the health care reform effort - a defining moment for our nation. The Democrats know it. And the Rebublicans know it. (Unfortunately Oprah missed the importance of the evening and is holding her own affair here in Chicago.)
We will hear references to the unsustainable nature of our current entitlement systems, about how not acting now on health care reform only threatens to make things worse. We can expect references to Ted Kennedy. We will see someone in the balcony that was denied insurance. We will hear of he plight of millions of Americans (will they use the number 46, 47 or 50 million?) without insurance. Will will hear of reaching accross the aisle. We will hear something about a trigger. And we will hear about the public option:
But what we won't hear is this:
Congress has already exempted itself from the Public Option.
-Wes
We will hear references to the unsustainable nature of our current entitlement systems, about how not acting now on health care reform only threatens to make things worse. We can expect references to Ted Kennedy. We will see someone in the balcony that was denied insurance. We will hear of he plight of millions of Americans (will they use the number 46, 47 or 50 million?) without insurance. Will will hear of reaching accross the aisle. We will hear something about a trigger. And we will hear about the public option:
President Barack Obama, in a high-stakes speech Wednesday to Congress and the nation, will press for a government-run insurance option in a proposed overhaul of the U.S. health-care system that has divided lawmakers and voters for months.The speech will be eloquently delivered. And the House and Senate will sit as they always do, interrupting the speech with thundrous applause on multiple occasions.
White House officials say the president will detail what he wants in the health-care overhaul, as well as say he is open to better ideas on a government plan if lawmakers have them.
Democratic plans call for requiring most Americans to carry health insurance. Failure to comply could cost families as much as $3,800 a year, according to a new Senate proposal.
But what we won't hear is this:
Congress has already exempted itself from the Public Option.
-Wes
Tuesday, September 08, 2009
Do Social Security Workers Make More Than Doctors?
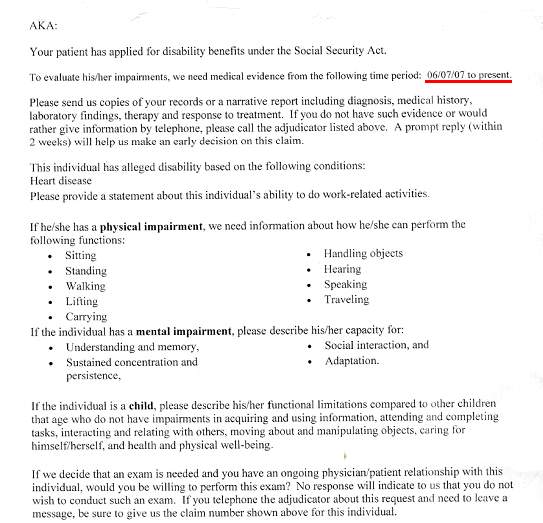
This week, like many doctors in primary care, I was sent a request by the Social Security to provide "medical evidence" that one of my patients was disabled so they could collect Social Security benefits. As part of that request, I was asked to provide evidence since June 6th, 2007, that my patient qualified for disability on the basis of "alledged" diagnosis of "Heart Disease."
I was asked to send "copies of records or a narrative report including diagnosis, medical history, laborary findings, treatment and response to treatment." Beyond this, I also had to include physical and emotional impairment assessments and a functional assessment of their ability to sit, stand, walk, lift carry, handle objects, hear, speak, travel, and wash their car, view films, and eat bon bons (well, kind of).
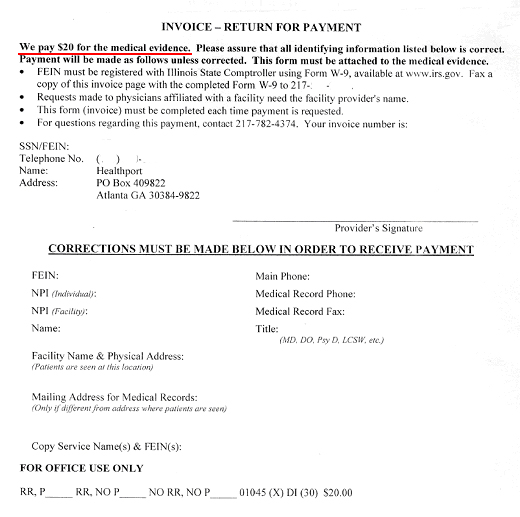
And for this copying, writing, mailing, collating what might I see from the government to compensate my time? Well, if I attach this invoice that requires a Federal Employee Identification Number filed through form W-9 available at www.irs.gov (yes, Virginia, this compensation is taxed), I might receive...
...drum roll, please...
... twenty dollars.
Now looking up the lowest paygrade of Social Security worker's annual compensation of $29,726 and accounting for the 13 vacation days, 13 paid sick leave days, and 10 federal holidays they get paid, I estimate the least expensive Social Security employee makes a bit more than $16.50 an hour.
If we assume that the paperwork they just asked for takes about 2 hours collectively of office staff and doctor time, I think it's clear that doctors' payment for this service provided on behalf of our patients is substantially less than what the Social Security administration pays their own staff.
I wonder what else the government has in store for us.
-Wes
{kind=link}
I was asked to send "copies of records or a narrative report including diagnosis, medical history, laborary findings, treatment and response to treatment." Beyond this, I also had to include physical and emotional impairment assessments and a functional assessment of their ability to sit, stand, walk, lift carry, handle objects, hear, speak, travel, and wash their car, view films, and eat bon bons (well, kind of).
And for this copying, writing, mailing, collating what might I see from the government to compensate my time? Well, if I attach this invoice that requires a Federal Employee Identification Number filed through form W-9 available at www.irs.gov (yes, Virginia, this compensation is taxed), I might receive...
{kind=link}
...drum roll, please...
... twenty dollars.
Now looking up the lowest paygrade of Social Security worker's annual compensation of $29,726 and accounting for the 13 vacation days, 13 paid sick leave days, and 10 federal holidays they get paid, I estimate the least expensive Social Security employee makes a bit more than $16.50 an hour.
If we assume that the paperwork they just asked for takes about 2 hours collectively of office staff and doctor time, I think it's clear that doctors' payment for this service provided on behalf of our patients is substantially less than what the Social Security administration pays their own staff.
I wonder what else the government has in store for us.
-Wes
Sunday, September 06, 2009
What Is Wrong With You People?
"I don't know what could be more clear," said Representative Bruce Braley, Democrat of Iowa, who has read aloud from a section of the House bill with the title "No Federal Payments for Undocumented Aliens.""Heath Care Debate Revives Immigration Battle,"
New York Times, 6 Sep 2009
From House Bill 3200, page 143:
SEC. 246. NO FEDERAL PAYMENT FOR UNDOCUMENTED
4 ALIENS.
5 Nothing in this subtitle shall allow Federal payments
6 for affordability credits on behalf of individuals who are
7 not lawfully present in the United States.
Taxpayers are concerned whether they will have to foot the bill for illegal aliens in the upcoming health care bill. Many ask good questions, like how will health care workers know who's an illegal alien? If they are included, how will it be paid for? These are important questions that we would hope could be dealt with squarely, openly and with full transparency.
But this is a sensitive topic for Congressmen interested in securing reelection.
During the summer recess, many Congressmen were barraged by questions to this effect. So it was interesting reading this New York Times piece this morning on whether illegal aliens will be covered under the new health care plan before Congress. On one hand we have Congressmen placating his constituents by assuring voters that "I don't know how it could be more clear" as they suggest taxpayers will not fund illegal aliens, but careful inspection discloses that illegal aliens will just not be eligible for federal subsidies to reduce their payments for federally-supplied health insurance.
But from here, it gets even more byzantine:
... the report finds that the House bill would not prohibit illegal immigrants from enrolling in a health insurance exchange. The exchange would allow participants to buy coverage from one of several plans, including a public option offered by the federal government.So here we have illegal aliens, already strapped for cash, paying their "full payment" and if they don't, the tax man will come after them (which is confusing to me, because I didn't know that illegal aliens pay taxes).
At the same time, illegal immigrants would not be exempt from the obligations in the House bill. According to the research service, most illegal immigrants in the country would be required to buy health insurance or face tax penalties.
And since they would be barred from subsidies, they would have to pay for coverage at full rates, regardless of their income level.
So what is wrong with the public? How could they possibly be confused?
Here's a thought: the only real way out of these shameful machinations is to deal with the immigration and health care issue separately, incrementally, and without this shell game. Doesn't the American public deserve a more thorough discussion of this issue, rather than shoving it in to our upcoming health care legislation?
My personal sense of it is that such an issue will never be decided at the Emergency Room door. Rather, it is part of a systemic immigration control and reform question that involves our borders, employee verification, and a decision about existing illegal immigrants.
What we're observing instead, is a Congress is too scared to deal with this issue honestly.
-Wes
Saturday, September 05, 2009
What Not To Call A Nurse
I have no idea how this topic came up, but I was performing a permanent pacemaker implant yesterday, and someone said to me,
After a lengthy discussion, there appeared to be a general consensus amongst the nurses and techs in our lab that "Sugar" was okay.
Just never, ever call a nurse "Honey."
Consider yourself warned.
-Wes
Is that okay, Hun?And a nurse giggled and then blurted out:
Oh I hate when patient's call me "Honey!" "Sugar" is fine, but "Honey?" Never!And so the other names like "Nutrasweet" were briefly entertained, as was "Candy." The chuckles continued.
After a lengthy discussion, there appeared to be a general consensus amongst the nurses and techs in our lab that "Sugar" was okay.
Just never, ever call a nurse "Honey."
Consider yourself warned.
-Wes
Number 2001
Hard to believe that since starting this blog, this is post number 2001.
It has been an interesting ride.
Looking back, it all started (honestly) as a way to talk about the t-shirt website that my wife and I developed in 2005. Innocent enough, certainly, but not very exciting after the initial novelty wore off [though I still like our t-shirts! :) ]
Not long after this blog began, my father fell gravely ill and I soon found the opportunity to put down in words what it was like to experience those times was therapeutic in a way. I often look back to those posts and find they ground me. My mother reads those posts still. I guess I didn't realize how much I enjoyed writing. Soon, I experimented with new ways to express emotional moments I encountered in my day to day dealings with life and medicine - some posts better than others and most with typos - but hey, it's me.
Better still, I have been introduced to some incredibly wonderful people through this blog. Interesting, passionate folks! Great friends. Some wackos. Some people stranger than others, certainly, but from all walks of life and all kinds of vocations. Although I could live without the not-so-clever spam artists out there, here in this little electronic nest everyone is an equal, everyone has a chance to say something that makes a difference. It didn't take long for me to be humbled by the breadth of knowledge that exists here in the blog-o-sphere.
I still am.
It's a strange thing, this addiction to the blog-o-sphere. I find my passion for the hobby ebbs and flows. Sometimes I have a steady stream of thoughts or opinions on things, other times the mind's a void for days. But when I can't find the words, others do (and usually with much more eloquence than I could ever muster). To those folks: thank you.
So as this strange source of endless entertainment and learning continues, it's only appropriate that I take a moment to thank all of you who have stopped by to share your thoughts, if only briefly.
We're all better for it.
Cheers-
-Wes
It has been an interesting ride.
Looking back, it all started (honestly) as a way to talk about the t-shirt website that my wife and I developed in 2005. Innocent enough, certainly, but not very exciting after the initial novelty wore off [though I still like our t-shirts! :) ]
Not long after this blog began, my father fell gravely ill and I soon found the opportunity to put down in words what it was like to experience those times was therapeutic in a way. I often look back to those posts and find they ground me. My mother reads those posts still. I guess I didn't realize how much I enjoyed writing. Soon, I experimented with new ways to express emotional moments I encountered in my day to day dealings with life and medicine - some posts better than others and most with typos - but hey, it's me.
Better still, I have been introduced to some incredibly wonderful people through this blog. Interesting, passionate folks! Great friends. Some wackos. Some people stranger than others, certainly, but from all walks of life and all kinds of vocations. Although I could live without the not-so-clever spam artists out there, here in this little electronic nest everyone is an equal, everyone has a chance to say something that makes a difference. It didn't take long for me to be humbled by the breadth of knowledge that exists here in the blog-o-sphere.
I still am.
It's a strange thing, this addiction to the blog-o-sphere. I find my passion for the hobby ebbs and flows. Sometimes I have a steady stream of thoughts or opinions on things, other times the mind's a void for days. But when I can't find the words, others do (and usually with much more eloquence than I could ever muster). To those folks: thank you.
So as this strange source of endless entertainment and learning continues, it's only appropriate that I take a moment to thank all of you who have stopped by to share your thoughts, if only briefly.
We're all better for it.
Cheers-
-Wes
Friday, September 04, 2009
Funding Health Care Reform - The Military Option
Every year of my 13 and a half years of active duty service in the US Navy it sat in the corner. Dark. A symbolic reminder of our mission. To protect and defend the Constitution of the United States. And the President.
'It' was the coronary care unit bed reserved just for the President. In my 13.5 years of service, I saw it used one morning: when preparations were made to perform cardioversion on then George Bush, Sr. after he developed atrial fibrillation while at Camp David. Remarkably, the room never was used since the President reportedly converted to sinus rhythm after an overnight loading dose of Procainamide. I remember the country breathed a collective sigh of relief that Dan Quayle wouldn't have to assume command of the country for those brief seconds of unconsciousness. (Politics is funny like that.) So the room was darkened again, just in case.
Recall that Washington had three military hospitals at the time: Walter Reed, Bethesda Naval hospital, and Andrews Air Force base. Why? Egos. Never mind that any serviceman would receive excellent care at any one of the facilities. Commanders fought to preserve their branches health care facilities tooth and nail. Commanders knew that relinquishing control of this benefit was a sign of weakness.
Things are a bit better now. In 2005, the Base Realignment and Closure committee recommended Walter Reed be closed. Presently, construction is underway to expand Bethesda Naval Medical Center so it can consolidate Walter Reed's Army care in the new facility. Tons of tax-payers money, but hey, it's needed for our military medicine mission.
Or is it?
This is not a small question in this time of great concern over where we get the money to pay for our nation's health care reform. Do we really need the duplicity of health care services offered by our military medical centers? Washington DC already has tons of civilian medical centers. Because of challenges the military has is recruiting subspecialists (neuroradiology was short-staffed when I was there), they often contract out services from civilian counterparts to fill staffing requirements - often at greater cost to them than their military equivalents. Other shortcomings exist as well: Bethesda is not even a Level 1 trauma center - mostly because of the security detail that limits access to the facility. (Imagine: a military center that doesn't see much trauma!) So they send their surgical residents to do rotations at the city's trauma centers. I, too, had to attend a civilian facility to learn my craft on the government's nickle. And at least six civilian medical centers are within a stone's throw of Bethesda.
Military medicine permits some interesting military-specific training, like biologic and chemical warfare training with all it's MOP gear. (Looks like fun, right?) But is there really a need for these facilities and all the personnel infrastructure they require as we struggle to find a way to fund our nation's health care? The government already has the glacially slow, underpaying Tricare and Tricare Prime insurance for our military members so they can receive care at civilian facilities when military medicine cannot fulfill the servicemen and servicewomens' needs.
The bottom line is, we should carefully reevaluate all our options for spending our precious health care resources wisely, and this includes greatly reducing or shuttering our military health care facilities.
-Wes
'It' was the coronary care unit bed reserved just for the President. In my 13.5 years of service, I saw it used one morning: when preparations were made to perform cardioversion on then George Bush, Sr. after he developed atrial fibrillation while at Camp David. Remarkably, the room never was used since the President reportedly converted to sinus rhythm after an overnight loading dose of Procainamide. I remember the country breathed a collective sigh of relief that Dan Quayle wouldn't have to assume command of the country for those brief seconds of unconsciousness. (Politics is funny like that.) So the room was darkened again, just in case.
Recall that Washington had three military hospitals at the time: Walter Reed, Bethesda Naval hospital, and Andrews Air Force base. Why? Egos. Never mind that any serviceman would receive excellent care at any one of the facilities. Commanders fought to preserve their branches health care facilities tooth and nail. Commanders knew that relinquishing control of this benefit was a sign of weakness.
Things are a bit better now. In 2005, the Base Realignment and Closure committee recommended Walter Reed be closed. Presently, construction is underway to expand Bethesda Naval Medical Center so it can consolidate Walter Reed's Army care in the new facility. Tons of tax-payers money, but hey, it's needed for our military medicine mission.
Or is it?
This is not a small question in this time of great concern over where we get the money to pay for our nation's health care reform. Do we really need the duplicity of health care services offered by our military medical centers? Washington DC already has tons of civilian medical centers. Because of challenges the military has is recruiting subspecialists (neuroradiology was short-staffed when I was there), they often contract out services from civilian counterparts to fill staffing requirements - often at greater cost to them than their military equivalents. Other shortcomings exist as well: Bethesda is not even a Level 1 trauma center - mostly because of the security detail that limits access to the facility. (Imagine: a military center that doesn't see much trauma!) So they send their surgical residents to do rotations at the city's trauma centers. I, too, had to attend a civilian facility to learn my craft on the government's nickle. And at least six civilian medical centers are within a stone's throw of Bethesda.
Military medicine permits some interesting military-specific training, like biologic and chemical warfare training with all it's MOP gear. (Looks like fun, right?) But is there really a need for these facilities and all the personnel infrastructure they require as we struggle to find a way to fund our nation's health care? The government already has the glacially slow, underpaying Tricare and Tricare Prime insurance for our military members so they can receive care at civilian facilities when military medicine cannot fulfill the servicemen and servicewomens' needs.
{kind=link}
The bottom line is, we should carefully reevaluate all our options for spending our precious health care resources wisely, and this includes greatly reducing or shuttering our military health care facilities.
-Wes
Thursday, September 03, 2009
Strong-arming Caregivers
"Hey Sally, us guys wanna help you wid your kid, see? Maybe gets you a few more dollas, ya know. All ya gots to do is sign dis here form and we'll take care of da rest, capeesh?"
"Uh, I'm not sure I really want unions representing me as I care for my son at home."
"Whatdyamean? Everybody knows dat da governor here in Illinois is on board. Heck he allowed collective bargaining by, ya know, 'individual providers of home-based support services.' So dat means you, Sally. We're nothing but angels, really."
"Are you saying I can go on strike and not wipe my son's rear end?"
"Hey, not so harsh, Sally! You know we'd never suggest such a thing! Look, for a mere $2000 a year, we'll represent your interests down state. It'll be nothin' but roses, seriously. I mean, look at 'em. No one's got answers on nuthin' down der. Ain't it time to make some heads roll? Comeon, Sal. Sign da form."
-Wes
"Uh, I'm not sure I really want unions representing me as I care for my son at home."
"Whatdyamean? Everybody knows dat da governor here in Illinois is on board. Heck he allowed collective bargaining by, ya know, 'individual providers of home-based support services.' So dat means you, Sally. We're nothing but angels, really."
"Are you saying I can go on strike and not wipe my son's rear end?"
"Hey, not so harsh, Sally! You know we'd never suggest such a thing! Look, for a mere $2000 a year, we'll represent your interests down state. It'll be nothin' but roses, seriously. I mean, look at 'em. No one's got answers on nuthin' down der. Ain't it time to make some heads roll? Comeon, Sal. Sign da form."
-Wes
Wednesday, September 02, 2009
Divide and Conquer Is "Working"
So what happens when CMS threatens to cut cardiologists' and oncologists' payments by 10-11% and shift money to primary care?
It gets ugly.
As a result, tensions between primary care doctors and specialists might even spill over to training programs:
It gets ugly.
As a result, tensions between primary care doctors and specialists might even spill over to training programs:
Tensions are rising among doctors, said Ted Epperly, 55, president of the American Academy of Family Physicians in Leawood, Kansas, in a telephone interview. Epperly runs a family practice in Boise, Idaho, and teaches at the University of Washington School of Medicine in Seattle.-Wes
Specialist colleagues have implied his support for the Medicare changes may cost his students, he said.
While family-care students typically spend parts of their three-year residencies training with specialists, “What I’ve heard is ‘maybe we just won’t have time any longer to teach your residents,’” Epperly said.
Tuesday, September 01, 2009
MADIT-CRT and the Device Industry's Image Problem
"In MADIT-CRT, 12 patients would need to be treated to prevent a single heart-failure event, whereas in the REVERSE trial, 20 patients would need to be treated to delay a heart-failure hospitalization. Is this money that could be spent more wisely? If the indication for CRT is expanded to all stage C patients with a low LVEF and a QRS duration of more than 120 msec, regardless of current symptoms or the duration of medical therapy, the potential "indication creep" in patients who are unlikely to derive a mortality benefit will alter the benefit-to-safety ratio and tip the score on cost-effectiveness even further in the wrong direction. Given the sobering facts about the costs of health care confronting us now and in the future, it appears prudent that any expanded indication for CRT in less symptomatic patients should be confined to patients with a QRS duration of more than 150 msec and in whom previous marked symptoms have been controlled with optimal medical therapy."
- Mariell Jessup, M.D.
Department of Medicine, Cardiovascular Division, University of Pennsylvania School of Medicine, Philadelphia.
Editorial: New England Journal of Medicine
That most implanted heart devices don't help patients has long been of concern to cardiologists, and has led to device sales well below manufacturers' projections. "We need better patient-specific identifications for who actually will benefit from these expensive devices," said Douglas P. Zipes, the former president of the American College of Cardiology, in a statement. "This study may widen the net to capture more patients for (heart resynchronizers). But whether that is appropriate should be questioned."
Wall Street Journal, 1 Sep 2009
The e-mail from my local Boston Scientific rep came at 07:30AM today: "MADIT-CRT Published!"
For those unfamiliar, the MADIT-CRT trial was designed to determine if combined implantable cardiac defibrillator (ICD)-cardiac resynchronization therapy (CRT-D) would reduce the risk of mortality and heart failure (HF) events by approximately 25% in subjects who were in New York Heart Association (NYHA) functional Class II with non-ischemic or ischemic cardiomyopathy and subjects who are in NYHA functional Class I with ischemic cardiomyopathy, left ventricular dysfunction (ejection fraction [EF] < or = 0.30), and prolonged intraventricular conduction (QRS duration > or = 130 ms). 60% of patients were randomized to CRT-D and 40% to ICD only.
And while the study proved that CRT combined with ICD decreased the risk of heart-failure events in relatively asymptomatic patients with a low ejection fraction and wide QRS complexes, the mortality between the two arms was not different.
This might be the biggest news coming from the trial: are reduced hospitalizations alone going to be enough to justify the expense of broader application of this technology?
Maybe it's the timing of this trial - released as America is struggling to find ways to reign in our health care costs as we reshape our entire health care system. Maybe its an erosion of trust spcialists have in a system that threatens to cut their payments 11% while device costs seem to remain relatively constant year to year. Whatever it is, there seems to be a new shift in cardiologists' and electrophysiologists' attitudes toward many of our most expensive preventative heart failure treatment technologies: are the costs of these devices paired with the number needed to treat really cost effective to our system as a whole?
In the past, the US has always lead the way in adopting primary prevention for heart failure and sudden death. While this has been laudible, it has also been expensive.
{kind=link}
And ironically, the expense of this incredible technology might now be biting us on the hind side. As evidenced by the quotes above - from loyal doctors who know and understand the wonders of this technology - the device industry has a serious problem. Unless more value than a hospitalization or two is gained with their technology, the device industry will struggle as their ultimate customers begin to think twice about adopting new indications on basis of these softer clinical endpoints.
-Wes
Reference: Moss AJ, et. al, Cardiac-Resynchronization Therapy for the Prevention of Heart-Failure Events, New Engl J Med September 1, 2009 (10.1056/NEJMoa0906431).
Subscribe to:
Posts (Atom)