Wednesday, October 30, 2019
What Gives?
WHAT GIVES the American Board of Internal Medicine the ability to take away years of schooling, mountains of prior testing, sleepless nights of residency, and months of study for initial Board certification that we all had to pass?
WHAT GIVES the American Board of Internal Medicine the authority to magically un-certify physicians for not purchasing or their Maintenance of Certification program?
WHAT GIVES the American Board of Internal Medicine the right to take away over 25 years of my expertise with catheter ablation or pacemaker implantation when they've never once examined the quality of my work or spoken with my patients?
WHAT GIVES the American Board of Internal Medicine the right to tell insurance companies and hospitals when my board certification expires so those companies can suddenly refuse to issue payments or revoke my hospital privileges claiming by skills as a physician have expired?
The American Board of Internal Medicine says it is developing new strategies of physician testing in the name of improved patient care, but WHAT GIVES for those physicians it has de-certified and are now jobless?
Removing physicians with years of patient care experience because they refuse to pay a fee or perform needless computer tasks is not in the best interest of patient safety or quality of care.
So WHAT GIVES?
-Wes
PS: Please help support the legal efforts underway to end Maintenance of Certification for all subspecialties by contributing to at https://www.gofundme.com/practicing-physicians-of-america
(Every dollar helps. Please share this video with your colleagues, too.)
Friday, October 25, 2019
A Case Study in the Wrong Way to Fix Clinician Burnout
Asking the system to fix the system in regards to physician and nursing burnout is like asking the fox to watch the henhouse.
They have no clue.
Case in point: the recent article published online before print in the Journal of the American Medical Association (JAMA) (where else?) preaching a "systems-based approach to clinician well-being and provide better patient care."
What "system" is recommending this "approach? None other than the Accreditation Council for Graduate Medical Education comprised of the American Medical Association (AMA), the American Hospital Association (AHA), and the American Board of Medical Specialties (ABMS), among others, with work performed by a committee comprised of friends from Blue Cross Blue Shield.
Most concerning, however, is this report was co-authored by one of the most conflicted authors in the health care business, Christine K. Cassel, MD. Recall that Dr. Cassel failed to disclose her board seats (and income) with Kaiser Hospitals and Health Systems and Premier (the largest health care Group Purchase Organization for the nation's hospitals) while serving as President and CEO of the American Board of Internal Medicine.
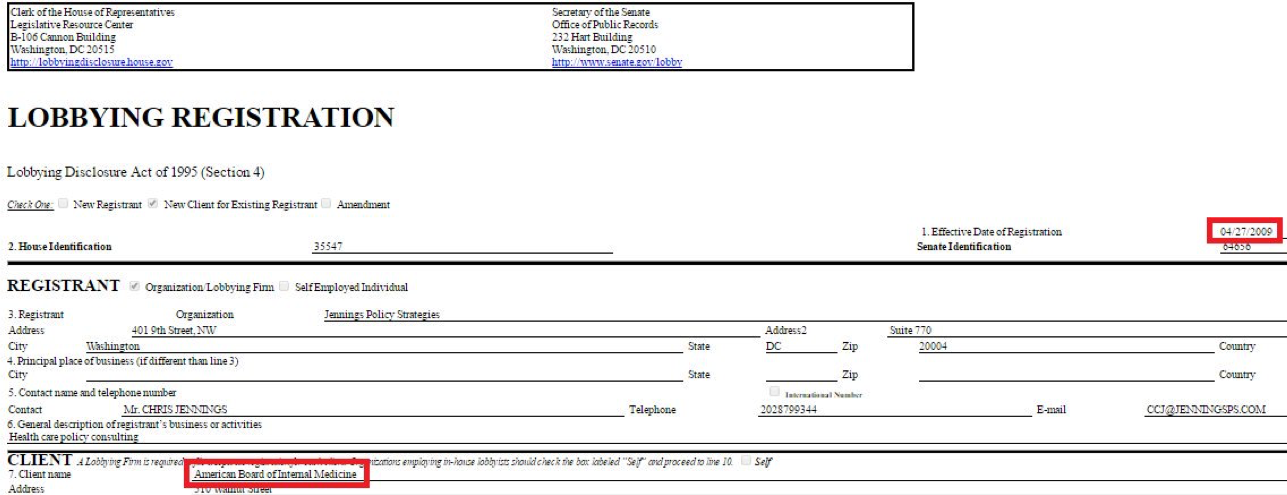
Christine K. Cassel, MD was President and CEO of the ABIM from 2004-2014. During her tenure at the ABIM, Dr. Cassel received a highly influential political appointment on the President's Council of Advisors for Science and Technology under President Obama in April 2009, just before the Affordable Care Act was signed into law in 2010.
The same day she announced that political appointment, the ABIM contracted with Washington lobbying firm Jennings Policy Strategies, Inc. yet never publicly disclosed this relationship. Instead, ABIM tax forms from 2010 listed this firm as hired for "consulting services." It appears to this lay physician that these "services" were in direct violation of IRS regulations concerning lobbying, especially given Dr. Cassel's substantial non-disclosed financial ties to Premier, Inc., one of the nation's largest Group Purchase Organizations for the nation's hospitals. At least one other lobbying firm was retained by ABIM (named Mehlman Castagnetti Rosen Bingel and Thomas, Inc.) until June 30, 2015, and this relationship was never publicly disclosed to ABIM's physician diplomates, the IRS, or the public either.
According to a Newsweek reporter, the ABIM used obfuscatory accounting techniques during and after Dr. Cassel's tenure: "I had an easier time figuring out the compensation of officials at Enron, WorldCom and Adelphia—all famous for lying on financial filings—than I did for those at the ABIM, where enormous effort seems to have been taken to make murky what should be crystal clear." The ABIM reportedly paid Dr. Cassel $1.7 million in her final year.
Some things never change: Dr. Cassel once again claimed "no conflicts" in the disclosures to this most recent JAMA article on physician burnout either.
Gaslighting physicians and nurses is not the way to fix burnout.
It would be far better for the members of the ACGME to hold a mirror before themselves to understand how their conflicts of interest have systematically done more to harm our profession over the years. Our current house of Medicine has gleefully created the world's most expensive typing pool with physicians and nurses as little more than data entry clerks clicking away whether home or at work. Our current non-transparent health care system has evolved this way thanks in large part to the AMA's behind-the-scenes business model dependent on licensing its ever-changing "Current Procedural Terminology" (CPT) codes for use by the electronic medical record companies and insurance companies to covertly ration care. At the same time, the ACGME supported and promoted the transition from lifetime ABMS board certification to an unproven and wasteful "continuous board certification" by insisting on lifetime testing and payments from physicians for themselves, the lucrative publishing and testing industries, and a vast network of physician specialty societies without ever examining the harms this extortion has caused physicians and the patients they care for. It is telling there was no mention in the recent JAMA article of the "Maintenance of Certification" (MOC) controversy that has led to multiple ongoing federal class action antitrust and racketeering lawsuits, deprives physicians of personal and family time, and steals any semblance of self-educational autonomy from physicians for the benefit of the ACGME members and their collaborators.
To fix burnout we need doctors and nurses looking up at patients rather than looking down at computer screens. We don't need hand-holding wellness exercises, life coaches, and yoga classes. We especially dont need them right after witnessing the unfortunate death of a child or having a patient die beneath our hands despite our best efforts.
Doctors and nurses are not babies or widgets in an assembly line.We entered into this real-life drama of medicine with eyes wide open knowing full well that medicine and health care can be challenging. Yet much of corporate medicine has taken on its role to push our limits to make the system more "productive" for the system at the expense of its caregivers. Medicine is hard damn work that is both emotionally draining yet exhilarating all at the same time. We take the ultimate responsibility for our patients. The ACGME and their protected bureaucratic workshop do not. We risk falling prey to this exploitation if we fail to expose these many undisclosed conflicts of interest with the authors and "committee" wrote and published this paper in JAMA.
This is not to say I see a day where medicine will occur without the use of computers. But computers and secret sharing of data health care data can have its consequences if patients and physicians are kept in the dark. The depersonalization that computers bring to medicine has a nasty side effect on the care we provide: physicians and nurses need face-to-face, hand-to-hand, and heart-to-heart time with patients and their colleagues, not computers, procedure codes, and recommendations from people who foisted MOC upon us, stood to gain financially from it, but never participated in MOC themselves.
Distrust of our self-imposed corporate overlords is a large part of why we're where we are currently, particularly when they insult us with their self-serving "mission" to have physicians help themselves. What do these physician-bureaucrat posers know what's really happening on the front line of health care today?
Humility at admitting mistakes would go a lot further at curing physician burnout than beating the same corporate drum that wedges itself between what really matters: doctors and nurses caring for patients without the self-appointed, politically- and industry-funded National Academy of Medicine and their cronies telling us how to do our jobs. It would be far better if they took off the chains they bind us with and let us do what we do best.
-Wes
They have no clue.
Case in point: the recent article published online before print in the Journal of the American Medical Association (JAMA) (where else?) preaching a "systems-based approach to clinician well-being and provide better patient care."
What "system" is recommending this "approach? None other than the Accreditation Council for Graduate Medical Education comprised of the American Medical Association (AMA), the American Hospital Association (AHA), and the American Board of Medical Specialties (ABMS), among others, with work performed by a committee comprised of friends from Blue Cross Blue Shield.
Most concerning, however, is this report was co-authored by one of the most conflicted authors in the health care business, Christine K. Cassel, MD. Recall that Dr. Cassel failed to disclose her board seats (and income) with Kaiser Hospitals and Health Systems and Premier (the largest health care Group Purchase Organization for the nation's hospitals) while serving as President and CEO of the American Board of Internal Medicine.
Christine K. Cassel, MD was President and CEO of the ABIM from 2004-2014. During her tenure at the ABIM, Dr. Cassel received a highly influential political appointment on the President's Council of Advisors for Science and Technology under President Obama in April 2009, just before the Affordable Care Act was signed into law in 2010.
The same day she announced that political appointment, the ABIM contracted with Washington lobbying firm Jennings Policy Strategies, Inc. yet never publicly disclosed this relationship. Instead, ABIM tax forms from 2010 listed this firm as hired for "consulting services." It appears to this lay physician that these "services" were in direct violation of IRS regulations concerning lobbying, especially given Dr. Cassel's substantial non-disclosed financial ties to Premier, Inc., one of the nation's largest Group Purchase Organizations for the nation's hospitals. At least one other lobbying firm was retained by ABIM (named Mehlman Castagnetti Rosen Bingel and Thomas, Inc.) until June 30, 2015, and this relationship was never publicly disclosed to ABIM's physician diplomates, the IRS, or the public either.
{kind=link}
According to a Newsweek reporter, the ABIM used obfuscatory accounting techniques during and after Dr. Cassel's tenure: "I had an easier time figuring out the compensation of officials at Enron, WorldCom and Adelphia—all famous for lying on financial filings—than I did for those at the ABIM, where enormous effort seems to have been taken to make murky what should be crystal clear." The ABIM reportedly paid Dr. Cassel $1.7 million in her final year.
Some things never change: Dr. Cassel once again claimed "no conflicts" in the disclosures to this most recent JAMA article on physician burnout either.
Gaslighting physicians and nurses is not the way to fix burnout.
It would be far better for the members of the ACGME to hold a mirror before themselves to understand how their conflicts of interest have systematically done more to harm our profession over the years. Our current house of Medicine has gleefully created the world's most expensive typing pool with physicians and nurses as little more than data entry clerks clicking away whether home or at work. Our current non-transparent health care system has evolved this way thanks in large part to the AMA's behind-the-scenes business model dependent on licensing its ever-changing "Current Procedural Terminology" (CPT) codes for use by the electronic medical record companies and insurance companies to covertly ration care. At the same time, the ACGME supported and promoted the transition from lifetime ABMS board certification to an unproven and wasteful "continuous board certification" by insisting on lifetime testing and payments from physicians for themselves, the lucrative publishing and testing industries, and a vast network of physician specialty societies without ever examining the harms this extortion has caused physicians and the patients they care for. It is telling there was no mention in the recent JAMA article of the "Maintenance of Certification" (MOC) controversy that has led to multiple ongoing federal class action antitrust and racketeering lawsuits, deprives physicians of personal and family time, and steals any semblance of self-educational autonomy from physicians for the benefit of the ACGME members and their collaborators.
To fix burnout we need doctors and nurses looking up at patients rather than looking down at computer screens. We don't need hand-holding wellness exercises, life coaches, and yoga classes. We especially dont need them right after witnessing the unfortunate death of a child or having a patient die beneath our hands despite our best efforts.
Doctors and nurses are not babies or widgets in an assembly line.We entered into this real-life drama of medicine with eyes wide open knowing full well that medicine and health care can be challenging. Yet much of corporate medicine has taken on its role to push our limits to make the system more "productive" for the system at the expense of its caregivers. Medicine is hard damn work that is both emotionally draining yet exhilarating all at the same time. We take the ultimate responsibility for our patients. The ACGME and their protected bureaucratic workshop do not. We risk falling prey to this exploitation if we fail to expose these many undisclosed conflicts of interest with the authors and "committee" wrote and published this paper in JAMA.
This is not to say I see a day where medicine will occur without the use of computers. But computers and secret sharing of data health care data can have its consequences if patients and physicians are kept in the dark. The depersonalization that computers bring to medicine has a nasty side effect on the care we provide: physicians and nurses need face-to-face, hand-to-hand, and heart-to-heart time with patients and their colleagues, not computers, procedure codes, and recommendations from people who foisted MOC upon us, stood to gain financially from it, but never participated in MOC themselves.
Distrust of our self-imposed corporate overlords is a large part of why we're where we are currently, particularly when they insult us with their self-serving "mission" to have physicians help themselves. What do these physician-bureaucrat posers know what's really happening on the front line of health care today?
Humility at admitting mistakes would go a lot further at curing physician burnout than beating the same corporate drum that wedges itself between what really matters: doctors and nurses caring for patients without the self-appointed, politically- and industry-funded National Academy of Medicine and their cronies telling us how to do our jobs. It would be far better if they took off the chains they bind us with and let us do what we do best.
-Wes
Saturday, October 12, 2019
Plaintiffs to Appeal ABIM Class-Action Lawsuit in Full
With the time to amend the earlier class action antitrust and racketeering lawsuit against the American Board of Internal Medicine (ABIM) past, this statement was issued by C. Phillip Curley, the Plaintiffs' lead attorney:
-Wes
Physicians wishing to support the plaintiffs in this unprecedented action are encouraged to contribute here.
“Plaintiffs plan to appeal in full the dismissal of their case. While we respect the district court, we believe it was wrong at this early stage of the litigation to dismiss Plaintiff’s case and deprive them of their day in court. Plaintiffs look forward to the vindication of their claims on appeal.”ABIM may have thought they won this case on dismissal, but it looks the plaintiffs' claims will get a second more critical review of the case with the 3rd Circuit Court of Appeals.
-Wes
Physicians wishing to support the plaintiffs in this unprecedented action are encouraged to contribute here.
Saturday, October 05, 2019
You Know There's a Problem with MOC When...
... yet another antitrust lawsuit is filed against ANOTHER American Board of Medical Specialties' member board. This time, the American Board of Orthopaedic Surgery joined the antitrust litigation fray on September 11, 2019.
Look for those Maintenance of Certification® (MOC®) fees to continue to skyrocket as the certification cartel extracts more fees from workingstiffs doctors to help pay their mounting legal bills.
-Wes
PS: Want to help with this David vs Goliath battle to help end MOC®? Click here.
Look for those Maintenance of Certification® (MOC®) fees to continue to skyrocket as the certification cartel extracts more fees from working
-Wes
PS: Want to help with this David vs Goliath battle to help end MOC®? Click here.
Wednesday, October 02, 2019
Why Working Physicians Deserve Their Day in Court
Ask any physician who shares 24-hour call with his colleagues: what time is the worst time to get called into the hospital? Most will tell you just before midnight.
That's because you miss out on those most precious first few hours of deep sleep needed for the next day.
For me, the call this particular evening came at 10:47 PM. Seventy-nine years old. Complete heart block. Wide complex escape rhythm at 34. Started to feel poorly early that morning. Stable blood pressure: 134/60.
A decision was needed.
So, I pulled my head off the pillow, glanced at the clock, grabbed by cellphone, and stumbled toward the other bedroom where the home computer rests. Giggling the mouse, the 45,000 watt screen light illuminated, blinding me as I struggled to type in the cellphone-derived time-sensitive passcode needed to log into EPIC alongside my username and password. I entered by username and password again (once is not enough, I guess), then found the particular hospital (I cover four at night when on call), then the Emergency Room patient list, then the room, and there it was: just as advertised, but with the dreaded one-triage note entry in the chart that basically just noted the time the patient arrived. That is the tell-tale sign that no real decision-making is needed for the ER staff. Just "call EP" (aka, me.)
The decision: pacemaker now or pacemaker later?
The mind does strange things with little sleep, but the decision at that time of night was mine and mine alone. No one else was there. No one else in medicine has this much responsibility. No nurse practitioner, medical administrator, or bureaucrat could make this call, but there I was: dead tired with my mind playing tricks on me. I would hear my inner-self rationalizing with the rapid-fire voices dancing in my head:
After a few hours sleep I woke, knowing I did the right thing. But reflecting back to that brief moment of decision-making the night before, I wondered to myself. Could things have gone differently?
Which brings me to the point of this blog post.
For the past five years, there has been tremendous uproar about the payments and unproven requirements of the Maintenance of (Board) Certification (MOC) mandate for US physicians created out of thin air by the American Board of Internal Medicine (ABIM) and marketed by the American Board of Medical Specialties (ABMS) to fund their bloated salaries, lobbying activities, and for-profit corporate subsidiaries that sell data. Thanks in part to the ACA law that includes the MOC mandate as a "quality" metric included by their lobbying, MOC's payments and needless exercises have became mandatory for employed physicians without their knowledge or consent. And with every passing day, the programs and exercises are promised to be easier, faster, less intrusive, because these bureaucrats continuously claim to know what's best for working physicians on the front-line of 24-hour patient care. They wallow in a sense of schadenfreude as they wield their undeserved power over their working colleagues, purposely naive to the most dangerous side effect their unwarranted and potentially illegal actions risk creating.
Longtime readers know that at least five different antitrust lawsuits have been filed against various non-profit entities that comprise the ABMS member boards in regards to MOC. The largest member board of that consortium is the ABIM, who recently breathed a partial sigh of relief when a Pennsylvania judge dismissed most of the claims of anti-trust tying, monopolization, racketeering, fraud, and unjust enrichment brought by four working internists. While the monopolization, fraud, and racketeering claims remain unresolved at this time, we should note that there might be significant consequences if working physicians don't get their day in court, and it's not what most people expect.
Not having an unbiased judgement in court before a jury of one's peers in these untested legal waters risks the development of US physician apathy.
Too many examples of lying, cheating, and stealing physicians' certification fees for political and economic purposes have occurred since MOC was mandated by the ABMS member boards in 1990. From the quiet movement of nearly $70 million from the ABIM to the secretly created ABIM Foundation from 1990-2007 in the name of "Choosing Wisely," the falsification of tax forms, holding political and corporate appointments while serving as the President and CEO of the ABIM, performing undisclosed lobbying, transferring funds to the Cayman Islands, and using felonious strongmen to invade doctors' houses with Federal Marshals and lawyers, were all accomplished just so their monopoly and partnership with insurers, hospitals, and medical specialty societies could flourish. By quashing the chance for justice against these actions, the courts risk irreparably damaging the integrity of the entire US medical profession and crushing the souls of those who make huge sacrifices on behalf of their patients every day.
This whole ABMS MOC fiasco, especially with the recent opinion to dismiss doctors claims of impropriety against this racket of monied tax-exempt corporations so broadly, risks making doctors apathetic. Could such apathy lead to less-than ideal decision-making in the wee hours of the morning?
I wonder.
For the sake of our profession and our patients, it's time to make sure working physicians get their day in court.
-Wes
That's because you miss out on those most precious first few hours of deep sleep needed for the next day.
For me, the call this particular evening came at 10:47 PM. Seventy-nine years old. Complete heart block. Wide complex escape rhythm at 34. Started to feel poorly early that morning. Stable blood pressure: 134/60.
A decision was needed.
So, I pulled my head off the pillow, glanced at the clock, grabbed by cellphone, and stumbled toward the other bedroom where the home computer rests. Giggling the mouse, the 45,000 watt screen light illuminated, blinding me as I struggled to type in the cellphone-derived time-sensitive passcode needed to log into EPIC alongside my username and password. I entered by username and password again (once is not enough, I guess), then found the particular hospital (I cover four at night when on call), then the Emergency Room patient list, then the room, and there it was: just as advertised, but with the dreaded one-triage note entry in the chart that basically just noted the time the patient arrived. That is the tell-tale sign that no real decision-making is needed for the ER staff. Just "call EP" (aka, me.)
The decision: pacemaker now or pacemaker later?
The mind does strange things with little sleep, but the decision at that time of night was mine and mine alone. No one else was there. No one else in medicine has this much responsibility. No nurse practitioner, medical administrator, or bureaucrat could make this call, but there I was: dead tired with my mind playing tricks on me. I would hear my inner-self rationalizing with the rapid-fire voices dancing in my head:
"Really, now?" ("Yeah, now")So the pacemaker representative and the rest of the team were called as I drove to see the patient (none are happy, but they understood). I placed a temporary pacing wire for backup (thank goodness), implanted the pacemaker, spoke with the grateful family, then drove home for my head to finally meet my lonely pillow at 2 AM. Thankfully without another interruption that morning.
"His blood pressure is stable, and the ER doctor says he looks fine, maybe this can wait until the morning?" (But that nice escape rhythm could quit, the pacer pads might not work, and you'll have to scramble those 10 miles up the road to make it in time.")
"The rep on call lives far away." (Too bad.)
"The staff will be spent, too. They are overstretched and need their sleep." (But this is why we're on call.)
"Maybe just a temp wire, then pacer in the morning daylight hours? (I have to drive there anyway. The temp wire might dislodge, then the patient has NO rhythm... )
"Dude, just do it. It'll save time in the long run and let you sleep without worrying."
After a few hours sleep I woke, knowing I did the right thing. But reflecting back to that brief moment of decision-making the night before, I wondered to myself. Could things have gone differently?
Which brings me to the point of this blog post.
For the past five years, there has been tremendous uproar about the payments and unproven requirements of the Maintenance of (Board) Certification (MOC) mandate for US physicians created out of thin air by the American Board of Internal Medicine (ABIM) and marketed by the American Board of Medical Specialties (ABMS) to fund their bloated salaries, lobbying activities, and for-profit corporate subsidiaries that sell data. Thanks in part to the ACA law that includes the MOC mandate as a "quality" metric included by their lobbying, MOC's payments and needless exercises have became mandatory for employed physicians without their knowledge or consent. And with every passing day, the programs and exercises are promised to be easier, faster, less intrusive, because these bureaucrats continuously claim to know what's best for working physicians on the front-line of 24-hour patient care. They wallow in a sense of schadenfreude as they wield their undeserved power over their working colleagues, purposely naive to the most dangerous side effect their unwarranted and potentially illegal actions risk creating.
Longtime readers know that at least five different antitrust lawsuits have been filed against various non-profit entities that comprise the ABMS member boards in regards to MOC. The largest member board of that consortium is the ABIM, who recently breathed a partial sigh of relief when a Pennsylvania judge dismissed most of the claims of anti-trust tying, monopolization, racketeering, fraud, and unjust enrichment brought by four working internists. While the monopolization, fraud, and racketeering claims remain unresolved at this time, we should note that there might be significant consequences if working physicians don't get their day in court, and it's not what most people expect.
Not having an unbiased judgement in court before a jury of one's peers in these untested legal waters risks the development of US physician apathy.
Too many examples of lying, cheating, and stealing physicians' certification fees for political and economic purposes have occurred since MOC was mandated by the ABMS member boards in 1990. From the quiet movement of nearly $70 million from the ABIM to the secretly created ABIM Foundation from 1990-2007 in the name of "Choosing Wisely," the falsification of tax forms, holding political and corporate appointments while serving as the President and CEO of the ABIM, performing undisclosed lobbying, transferring funds to the Cayman Islands, and using felonious strongmen to invade doctors' houses with Federal Marshals and lawyers, were all accomplished just so their monopoly and partnership with insurers, hospitals, and medical specialty societies could flourish. By quashing the chance for justice against these actions, the courts risk irreparably damaging the integrity of the entire US medical profession and crushing the souls of those who make huge sacrifices on behalf of their patients every day.
This whole ABMS MOC fiasco, especially with the recent opinion to dismiss doctors claims of impropriety against this racket of monied tax-exempt corporations so broadly, risks making doctors apathetic. Could such apathy lead to less-than ideal decision-making in the wee hours of the morning?
I wonder.
For the sake of our profession and our patients, it's time to make sure working physicians get their day in court.
-Wes
Subscribe to:
Comments (Atom)