Now imagine that piece of paper comes with a promise of having to pay more for your own good and where time spent acquiring that paper meant nothing. Most rational people would have visions of Bernie Madoff or some other Ponzi scheme.
Yet this is the reality of the American Board of Medical Specialties' Maintenance of Certification (MOC) program for practicing US physicians.
I recently went throughout the Maintenance of Certification process in 2013. I sat for both by Cardiovascular Diseases Certification (that expired in 2013) and Clinical Cardiac Electrophysiology recertification (that expired in 2014) secure examinations in October of 2013. Here's what I got for my cardiovascular recertification fees:
 |
| ABIM Cardiovascular Disease Certificate 2013 - Click to enlarge |
Note that because the cardiovascular certificate was renewed in 2013, it now was extended from 2013 through 2023. The cover letter that came with the new Cardiovascular Disease certificate was also notable for the three references its cited as "proof" of the value of these certificates. The three references were (1) Arch Intern Med 2010; 170(16): 1442-9, (2) Arch Intern Med 2009 (sic - Editor's note: actually 2008) 168: 1396-1403 and (3) JAMA 2005 294(4): 473-81.
Reference (1) concludes that "Publically available characteristics of individual physicians are poor proxies for performance on clinical quality measures." Reference (3) is a cross-sectional retrospective analysis of data on US physician respondents to the 2000-2001 Community Tracking Study linked to Medicare beneficiaries they treated in 2001 that only generated the hypothesis that "profiling practices may help develop tailored interventions that can be directed to sites where the opportunities for quality improvement are greatest."
But the worst reference was Reference (2). This reference is notable in part because of the glaring and inexcusable conflict of interests of every author on the manuscript. Each author was either a paid member of ABIM or an employee of Qualidigm of Middletown, CT, a data analytics firm that does the following according to its website:
Collecting relevant data, turning that data into information, and that information into action, drives almost every Qualidigm initiative and contract.So it appears that Qualidigm's authors (and the purpose of these certificates and entire MOC program) was manufactured not only for the money it creates for these boards, but for insurance company claim denials.
Qualidigm analysts have the qualitative and quantitative knowledge, skills and experience to provide a wide range of services including but not limited to:
- the analysis of claims data from a single source or aggregating claims data from multiple sources;
- the collection, integration and analysis of claims data, administrative data and medical records data;
- the geographic analysis of various types of databases, e.g., claims, medical records;
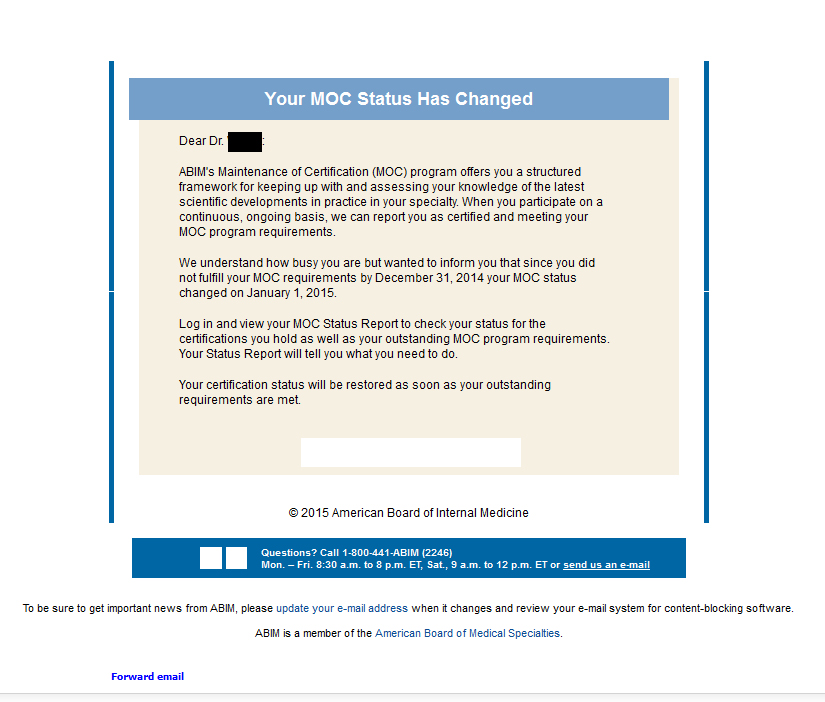
Because my Cardiac Electrophysiology certificate expired in 2014, doctors should be aware of the changes that have occurred to board certificates. I recieved this new certificate after passing by secure examination and countless hours collecting survey data, attending board review courses, and reading enough material to put the Encyclopedia Britannica to shame:
 |
| ABIM Clinical Cardiac Electrophysiology Certificate 2014 - Click to enlarge |
Note the fine print below the words "Clinical Cardiac Electrophysiology:"
"Ongoing certification is contingent upon meeting the requirements of Maintenance of Certification. Please visit www.abim.org to verify certification status."In essense the new 2014 (and later) "Maintenance of Certification" certificates are nothing more than very expensive hyperlinks to the ABIM.org website.
Sorry, but I will never recertify and participate in this Ponzi scheme again.
Ever.
-Wes










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}