My talk given to the American Association of Physicians and Surgeons (AAPS):
For those who have been following this blog closely, much of this information won't be new. But to those who want the entire depth and breath of the corruption of the ABIM/ABMS MOC program summarized in 22 short minutes, this is a "must see." Learn, also, what can be done to disrupt the MOC re-certification cartel in medicine. The video was nicely produced and incorporates my slides into the video.
Tell your colleagues who might not know this story to watch.
Tell your local news reporters to watch.
Tell your state legislators and health care regulators to watch.
Then ask your friends at the IRS, FTC, and DOJ to watch.
After all, it's one amazing story that touches much of the bureaucratic house of medicine.
Thanks-
-Wes
Wednesday, September 28, 2016
Monday, September 26, 2016
Just Dues
She reached into her large canvas bag and handed it to me. “I read about your award, Dr. Fisher, and wanted you to have this to remember it by.”
I was stunned (and a bit embarrassed). “Thank you, Ms. Smith (not her real name).” There in my hands was a beautifully engraved replica of the front-page story in “The Journal,” the local National Naval Medical Center bulletin describing the Young Investigator Award I received from the North American Society of Pacing and Electrophysiology (NASPE) in 1992. Looking back, it was one of my proudest achievements in my young medical career that I can remember. That experience taught me how to do credible research, speak at a scientific session, support my work in a public forum, and write a scientific paper. Ultimately, the award opened important doors for me, like obtaining a fellowship slot at the University of California, San Francisco, one of the most academically productive electrophysiology programs in the country at the time. This plaque still hangs in my office today.
NASPE has since morphed to the Heart Rhythm Society (HRS) to better reflect the organization's more global mission to raise awareness and foster innovation in cardiac rhythm research and management. Cardiac electrophysiologists from around the world attend their annual scientific sessions to learn the latest and greatest innovations in our field. In 2015, HRS had $17M in revenues ($6.6M in registration fees (from Scientific Sessions and board review courses, I assume), $3M from grants, $2.7M from annual meeting exhibits, and $2M from membership dues, representing the largest source of revenues. These revenues were offset by $20M in expenses in FY 2015, somewhat larger than usual due to dissolution of the HRS Foundation which had accumulated a little more than $2M in losses due to lingering administrative overhead expenses. While it touts practicing physician officers, to each of their credit, none of them earned any revenue from their service to HRS in 2015. The CEO of HRS, Mr. James Youngblood, did enjoy a salary of $682,193 for his administrative services in 2015, however. So from what I can gather, MOC educational programs remain important to HRS’s bottom line. No wonder they are reluctant to lose those revenues for the organization! But supporting an illegitimate program that could damage a physician's career just for the revenue stream is wrong.
These past several weeks I received emails requesting renewal of my annual membership fees to HRS, fees I proudly paid every year since I won that NASPE Young Investigator Award. Usually, my administrative assistant would pay the annual fee automatically from my $2500 expense fund I receive from my hospital system. This year, after two years of struggling to have an impact on the MOC debacle and after having an internal debate with myself, I asked her to not pay my dues to both HRS and American College of Cardiology (ACC).
I do not make this decision lightly. I realize that many of my colleagues will think I’m being silly, rigid, or just plain dumb. After all, I won't be able to sit on steering committees for my profession without that membership or the opportunity to chair a scientific session. But most of them also know how strongly I feel about supporting the ABMS MOC program that was born from nothing more than a desire for our cash and is paid to an organization that has participated in blatant tax fraud, accounting irregularities, and strongman tactics that have threatened and intimidated too many unsuspecting and vulnerable physicians without just cause.
This is not to say I do not appreciate the earlier efforts the Heart Rhythm Society to change the MOC system for the better. Efforts like removing the double jeopardy requirement for cardiac electrophysiologists to have to certify in cardiology as a pre-condition to being granted recertification in cardiac electrophysiology, even though you passed the test, for instance, were influenced by their efforts. I also appreciated when they tried to hold sessions at their annual Scientific Sessions debating the need for MOC. But the session held with Dr. Douglas Zipes as MOC protagonist and Dr. Fred Kusumoto as MOC antagonist, allowed the protagonist to dictate the rules, insisting that no discussion of the finances of the ABIM and MOC program would occur, immediately stifling any real debate. Since that time, both the HRS (and their big brothers at the ACC) have increasingly shied away from their original public rebuke of the MOC program. It appears they have acquiesced to MOC's perpetuation, albeit in some as yet undisclosed “modified” form and with a new "blueprint." For this reason, I no longer find myself able to support any organization that allies itself with this scientifically and morally corrupt program.
The MOC re-certification cartel has become a $5.7 billion business enterprise annually in the US alone. It is incredibly divisive to our profession, dividing the bureaucratic in our ranks from those on the front line of patient care. Because this unproven and unwarranted program also threatens physicians’ ability to practice their trade and care for patients, I believe it causes significant harm to our patients by crushing the morale of too many physicians without legitimate cause just so the ABIM, the ABMS, and our own specialty societies can wallow in the MOC program's revenues. Many senior practicing physicians are leaving medicine because of this MOC requirement because they know it's just about the money. The fact that the adverse effects of this program to physicians and their patients have never been independently studied speaks volumes why this MOC program should end immediately.
I have no idea if withholding my dues will make a difference in the fight against MOC. Certainly if HRS and ACC change their mind and work to end the MOC program entirely, I’ll be the first to reinstate my dues. But what else can I do in the short term? Keep paying? While I'll lose my subscriptions to the Heart Rhythm Journal and the Journal of the American College of Cardiology, I can search our library for articles I need. Still, I suspect I could lose some of the camaraderie that I have enjoyed in my relationship with HRS over the years, and that will be missed, but it seems like a relatively small price to pay.
My years-long investigation of the ABIM has taken me to places I never fathomed I'd have to go to get to the bottom of this story. It is strange the effect this story has had on me. On one hand, I feel greater connection to more of my peers than ever, yet on the other, I feel a quiet discontent from the House of Medicine's leadership that stands to lose the support of their rank and file as the story unfolds. I suppose I should not be surprised, especially since the MOC program has secretly funded so many for so long. But the stakes appear to be getting higher for all involved.* I just hope that exposing all of the corruption against practicing physicians by those in our own ranks ultimately brings the practice of medicine to a better place.
To offset this ennui, it would be great to have an opporuntity to meet those who might join me in my efforts to stop this program by refusing to pay their society dues. Perhaps we could arrange a trip to Chicago in May, 2017 to hoist a beer together in the epicenter of the ACGME MOC bureaucratic Machine together. It would seem quite apropos and I'd look forward to hosting that event. Let's call it "Lemonade out of MOC lemons."
We need to bring back the integrity of our profession ourselves, one dues payment at a time. It is clearer than ever that no one else will do this for us. It would be quite remarkable if this movement gained steam, but I'm really not holding my breath.
But if it did, it would be nice to at my patient's thoughtful plaque and feel pride in what it means to be a member of a subspecialty medical society again.
-Wes
* I would have posted a picture of my award to accompany this post, but it appears my server may have been hacked. I'll know more in 48 hours as technicians are working to resolve the problem.
I was stunned (and a bit embarrassed). “Thank you, Ms. Smith (not her real name).” There in my hands was a beautifully engraved replica of the front-page story in “The Journal,” the local National Naval Medical Center bulletin describing the Young Investigator Award I received from the North American Society of Pacing and Electrophysiology (NASPE) in 1992. Looking back, it was one of my proudest achievements in my young medical career that I can remember. That experience taught me how to do credible research, speak at a scientific session, support my work in a public forum, and write a scientific paper. Ultimately, the award opened important doors for me, like obtaining a fellowship slot at the University of California, San Francisco, one of the most academically productive electrophysiology programs in the country at the time. This plaque still hangs in my office today.
NASPE has since morphed to the Heart Rhythm Society (HRS) to better reflect the organization's more global mission to raise awareness and foster innovation in cardiac rhythm research and management. Cardiac electrophysiologists from around the world attend their annual scientific sessions to learn the latest and greatest innovations in our field. In 2015, HRS had $17M in revenues ($6.6M in registration fees (from Scientific Sessions and board review courses, I assume), $3M from grants, $2.7M from annual meeting exhibits, and $2M from membership dues, representing the largest source of revenues. These revenues were offset by $20M in expenses in FY 2015, somewhat larger than usual due to dissolution of the HRS Foundation which had accumulated a little more than $2M in losses due to lingering administrative overhead expenses. While it touts practicing physician officers, to each of their credit, none of them earned any revenue from their service to HRS in 2015. The CEO of HRS, Mr. James Youngblood, did enjoy a salary of $682,193 for his administrative services in 2015, however. So from what I can gather, MOC educational programs remain important to HRS’s bottom line. No wonder they are reluctant to lose those revenues for the organization! But supporting an illegitimate program that could damage a physician's career just for the revenue stream is wrong.
These past several weeks I received emails requesting renewal of my annual membership fees to HRS, fees I proudly paid every year since I won that NASPE Young Investigator Award. Usually, my administrative assistant would pay the annual fee automatically from my $2500 expense fund I receive from my hospital system. This year, after two years of struggling to have an impact on the MOC debacle and after having an internal debate with myself, I asked her to not pay my dues to both HRS and American College of Cardiology (ACC).
I do not make this decision lightly. I realize that many of my colleagues will think I’m being silly, rigid, or just plain dumb. After all, I won't be able to sit on steering committees for my profession without that membership or the opportunity to chair a scientific session. But most of them also know how strongly I feel about supporting the ABMS MOC program that was born from nothing more than a desire for our cash and is paid to an organization that has participated in blatant tax fraud, accounting irregularities, and strongman tactics that have threatened and intimidated too many unsuspecting and vulnerable physicians without just cause.
This is not to say I do not appreciate the earlier efforts the Heart Rhythm Society to change the MOC system for the better. Efforts like removing the double jeopardy requirement for cardiac electrophysiologists to have to certify in cardiology as a pre-condition to being granted recertification in cardiac electrophysiology, even though you passed the test, for instance, were influenced by their efforts. I also appreciated when they tried to hold sessions at their annual Scientific Sessions debating the need for MOC. But the session held with Dr. Douglas Zipes as MOC protagonist and Dr. Fred Kusumoto as MOC antagonist, allowed the protagonist to dictate the rules, insisting that no discussion of the finances of the ABIM and MOC program would occur, immediately stifling any real debate. Since that time, both the HRS (and their big brothers at the ACC) have increasingly shied away from their original public rebuke of the MOC program. It appears they have acquiesced to MOC's perpetuation, albeit in some as yet undisclosed “modified” form and with a new "blueprint." For this reason, I no longer find myself able to support any organization that allies itself with this scientifically and morally corrupt program.
The MOC re-certification cartel has become a $5.7 billion business enterprise annually in the US alone. It is incredibly divisive to our profession, dividing the bureaucratic in our ranks from those on the front line of patient care. Because this unproven and unwarranted program also threatens physicians’ ability to practice their trade and care for patients, I believe it causes significant harm to our patients by crushing the morale of too many physicians without legitimate cause just so the ABIM, the ABMS, and our own specialty societies can wallow in the MOC program's revenues. Many senior practicing physicians are leaving medicine because of this MOC requirement because they know it's just about the money. The fact that the adverse effects of this program to physicians and their patients have never been independently studied speaks volumes why this MOC program should end immediately.
I have no idea if withholding my dues will make a difference in the fight against MOC. Certainly if HRS and ACC change their mind and work to end the MOC program entirely, I’ll be the first to reinstate my dues. But what else can I do in the short term? Keep paying? While I'll lose my subscriptions to the Heart Rhythm Journal and the Journal of the American College of Cardiology, I can search our library for articles I need. Still, I suspect I could lose some of the camaraderie that I have enjoyed in my relationship with HRS over the years, and that will be missed, but it seems like a relatively small price to pay.
My years-long investigation of the ABIM has taken me to places I never fathomed I'd have to go to get to the bottom of this story. It is strange the effect this story has had on me. On one hand, I feel greater connection to more of my peers than ever, yet on the other, I feel a quiet discontent from the House of Medicine's leadership that stands to lose the support of their rank and file as the story unfolds. I suppose I should not be surprised, especially since the MOC program has secretly funded so many for so long. But the stakes appear to be getting higher for all involved.* I just hope that exposing all of the corruption against practicing physicians by those in our own ranks ultimately brings the practice of medicine to a better place.
To offset this ennui, it would be great to have an opporuntity to meet those who might join me in my efforts to stop this program by refusing to pay their society dues. Perhaps we could arrange a trip to Chicago in May, 2017 to hoist a beer together in the epicenter of the ACGME MOC bureaucratic Machine together. It would seem quite apropos and I'd look forward to hosting that event. Let's call it "Lemonade out of MOC lemons."
We need to bring back the integrity of our profession ourselves, one dues payment at a time. It is clearer than ever that no one else will do this for us. It would be quite remarkable if this movement gained steam, but I'm really not holding my breath.
But if it did, it would be nice to at my patient's thoughtful plaque and feel pride in what it means to be a member of a subspecialty medical society again.
-Wes
* I would have posted a picture of my award to accompany this post, but it appears my server may have been hacked. I'll know more in 48 hours as technicians are working to resolve the problem.
Sunday, September 18, 2016
Who Makes Insurance Companies Require MOC?
One of the largest reason physicians must participate in the ABMS Maintenance of Certification (MOC) program is because insurance companies demand it.
At least this is what the NCQA would like us to believe.
Those "evil-doer" insurance companies!
But it is the National Committee for Quality Assurance (NCQA), heavily marketed (video) by the likes of Atul Gwande, MD, that set the rules about which credentialing bodies US insurers can accept. Not surprisingly, the "Department of Health and Human Services (HHS) selected NCQA as an accrediting entity for Qualified Health Plan issuers participating in the Health Insurance Exchange Marketplace."
Who comprises the leadership ranks of the NCQA? Lots of good folks from the ABIM Foundation, the National Quality Forum, American College of Physicians (ACP), the Association of American Medical Colleges, and the insurance industry are members of its board of directors and its leadership team, who else?
And there you have it: a perfectly legal way to monopolize the credentialing process of US physicians, particularly one the ABMS, ACP, and ABIM stand to profit from.
And how much "quality" does the NCQA really require of insurance companies?
Not much:
Sheesh. What an incredible waste of tax dollars.
If this is the hypocritical "quality" that the NCQA assures, we're all in trouble.
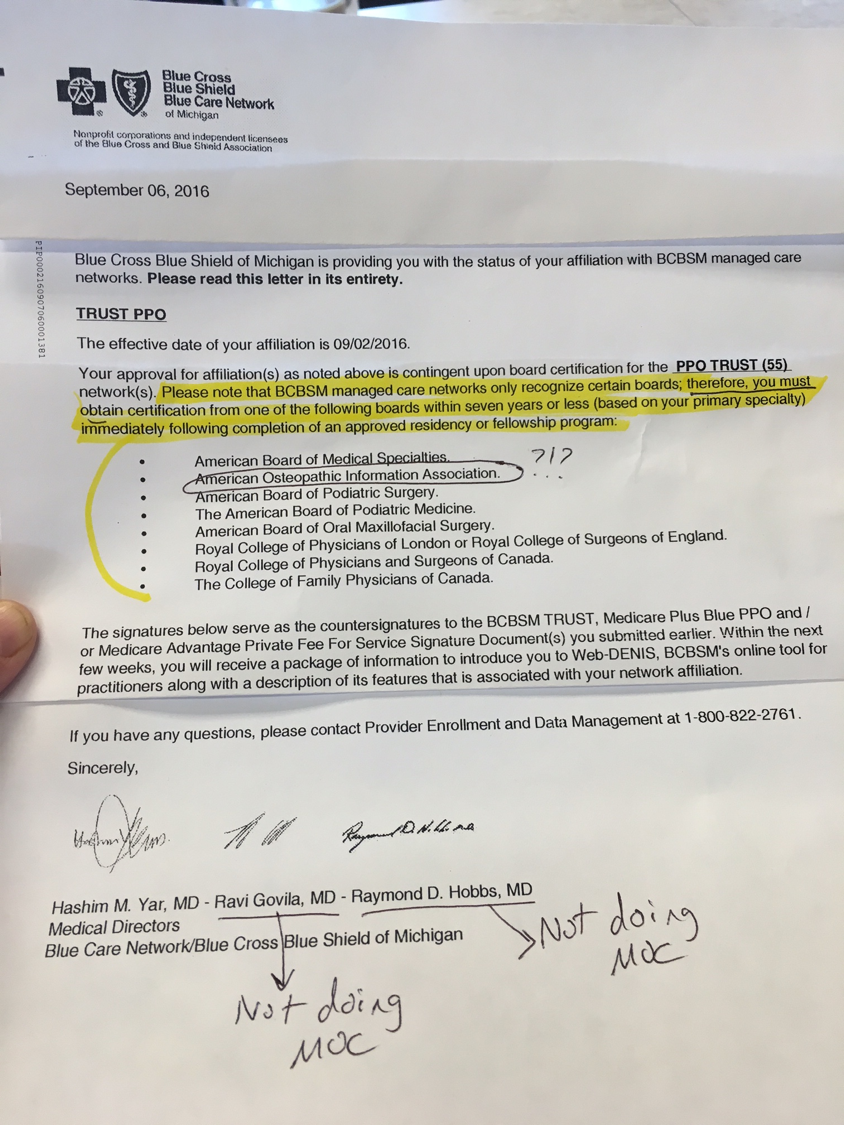
Time for the NCQA to add the National Board of Physicians and Surgeons (NBPAS.org) to that list of accepted credentialing bodies for insurance companies to utilize nationwide. Otherwise, given the number of suits being filed against the AOA (a.k.a., the "American Osteopathic Information Organization" as circled in the letter above) and the ABMS and its member boards these days, the NCQA board members might need an alternative, legitimate credentialing body to add to their list of acceptable credentialing boards in order to keep their jobs.
Just saying'-
-Wes
At least this is what the NCQA would like us to believe.
Those "evil-doer" insurance companies!
But it is the National Committee for Quality Assurance (NCQA), heavily marketed (video) by the likes of Atul Gwande, MD, that set the rules about which credentialing bodies US insurers can accept. Not surprisingly, the "Department of Health and Human Services (HHS) selected NCQA as an accrediting entity for Qualified Health Plan issuers participating in the Health Insurance Exchange Marketplace."
Who comprises the leadership ranks of the NCQA? Lots of good folks from the ABIM Foundation, the National Quality Forum, American College of Physicians (ACP), the Association of American Medical Colleges, and the insurance industry are members of its board of directors and its leadership team, who else?
And there you have it: a perfectly legal way to monopolize the credentialing process of US physicians, particularly one the ABMS, ACP, and ABIM stand to profit from.
And how much "quality" does the NCQA really require of insurance companies?
Not much:
 |
| (Click image to enlarge) |
If this is the hypocritical "quality" that the NCQA assures, we're all in trouble.
Time for the NCQA to add the National Board of Physicians and Surgeons (NBPAS.org) to that list of accepted credentialing bodies for insurance companies to utilize nationwide. Otherwise, given the number of suits being filed against the AOA (a.k.a., the "American Osteopathic Information Organization" as circled in the letter above) and the ABMS and its member boards these days, the NCQA board members might need an alternative, legitimate credentialing body to add to their list of acceptable credentialing boards in order to keep their jobs.
Just saying'-
-Wes
Sunday, September 11, 2016
I'm Thinking Vasodepressor Syncope
Hillary Clinton leaving the 9-11 memorial service:
This just doesn't smack of an abrupt cardiac arrhythmia (usually there's no warning there), but rather hypotension. Perhaps a simple faint. Perhaps a side effect of medications. Whatever it was, there wasn't enough blood pressure to remain vertical unassisted.
Other thoughts? (Please be respectful).
-Wes
There she was, standing in one place for quite a while while feeling poorly, being supported by one or more colleagues (? secret service agents?), when she tries to "walk" and stumbles toward the ground.When you try to roll to Chili's with the squad after Gameday still shitfaced. pic.twitter.com/Pd3AQcJksH
— Old Row (@OldRowOfficial) September 11, 2016
This just doesn't smack of an abrupt cardiac arrhythmia (usually there's no warning there), but rather hypotension. Perhaps a simple faint. Perhaps a side effect of medications. Whatever it was, there wasn't enough blood pressure to remain vertical unassisted.
Other thoughts? (Please be respectful).
-Wes
Thursday, September 08, 2016
A Rebuttal to ABIM President and CEO's Defense of MOC
In August, Medical Economics published an interview with Richard Baron, MD entitled: "The Man Behind MOC Defends the Program Against Critics." Medical Economics then solicited practicing physicians to write a rebuttal. I accepted, but with a warning:
That was August 12, 2016.
I reached out to Medical Economics yesterday to inquire where things stood on the rebuttal and received a phone call a short time later from a more senior editor that they would be unable to publish my work, especially the part that dealt with the ABIM, but would be willing to write about modifications I might suggest for the MOC program. I thanked them for their review but saw no utility in promoting "modifications" to MOC over ending the program entirely. We parted company politely.
Needless to say, I'm frustrated, but this isn't the first time this has happened. (Welcome to the realities of the Medical Industrial Complex!).
*sigh*
But one of the beauties of social media and the disruptive force of the Internet is that anyone can be their own publisher. Glenn Reynolds famously coined our ability to compete with larger publishing firms "An Army of Davids."
And so, thanks to the wonders of technology, I present my rebuttal to Dr. Baron below.
* * *
After exchanging a series of Twitter direct messages and e-mails with the staff at Medical Economics, much to my surprise they seemed agreeable to publish my piece and promised to move forward with the rebuttal for both print and online versions of Medical Economics. So I signed a "Contributor License Agreement" with UBM LLC, a nearly $2.8 billion owner of Medical Economics (among lots of other throw-away publications) and proceeded to spend the better part of an evening composing my rebuttal and submitted it a few days later.@MedEconomics @DrLaurieG Happy to do so but come with a warning label: I will not mince words.— Westby Fisher, MD (@doctorwes) August 7, 2016
That was August 12, 2016.
I reached out to Medical Economics yesterday to inquire where things stood on the rebuttal and received a phone call a short time later from a more senior editor that they would be unable to publish my work, especially the part that dealt with the ABIM, but would be willing to write about modifications I might suggest for the MOC program. I thanked them for their review but saw no utility in promoting "modifications" to MOC over ending the program entirely. We parted company politely.
Needless to say, I'm frustrated, but this isn't the first time this has happened. (Welcome to the realities of the Medical Industrial Complex!).
*sigh*
But one of the beauties of social media and the disruptive force of the Internet is that anyone can be their own publisher. Glenn Reynolds famously coined our ability to compete with larger publishing firms "An Army of Davids."
And so, thanks to the wonders of technology, I present my rebuttal to Dr. Baron below.
Richard Baron, MD, President and CEO of the American Board of Internal Medicine (ABIM) and the ABIM Foundation, was recently interviewed by Jeff Bendix of Medical Economics and once again attempted to defend the ABIM's Maintenance of Certification (MOC) program by rehashing his usual talking points. Dr. Baron argues that because there is an explosion of medical information out there, doctors should use ABIM recertification metric to prove to themselves, patients, and institutions that they are staying current in medicine. Dr. Baron also seems to believe that taking computerized tests assembled from a database of rehashed test questions every ten years is superior to gaining 10 years of direct patient care experience.
Unfortunately, Dr. Baron and his bureaucratic colleagues at the ABIM seem to have forgotten that practicing physicians are committed to caring for patients, not to supporting Dr. Baron’s retirement fund.
While endlessly promoting their Maintenance of Certification (MOC) program to the public, the truth is that the potential adverse effects of ABIM re-certification on physicians and their patients have never been studied, nor has the American Board of Medical Specialties (ABMS) MOC program ever been shown to improve the quality or safety of patient care (See here, here, and here), especially as it pertains to a physician's specific practice environment. Their form of assessment is, in effect, a one-size-fits-all assessment of a physician's ability to retain facts and take a test, little more. Despite these facts and thanks to heavy lobbying to the medical community by those who stand to profit from the program, practicing physicians certified after 1990 must perform this ritual every 10 years to retain their hospital privileges or be allowed to be providers for many large insurance plans while physicians certified before 1990 do not - a discriminatory practice against younger, more economically vulnerable physicians.
As a triple "Board-certified" physician in good standing who has experienced the transition of the ABIM "Board certification" credential from a voluntary once-in-lifetime designation to a time-limited one, I have experienced first-hand the irrational and humiliating process of re-certification that makes a mockery of the entire health care accreditation process. After spending nearly $10,000 to "maintain" my certifications in cardiovascular diseases and cardiac electrophysiology in 2013 for the third time and having to be scanned, searched, and videotaped to assure my integrity in a PearsonVue testing center, I decided to study the finances, practices, and financial conflicts of interest that have come to define the ABIM and (as I have since learned) much of our physician credentialing system in the United States. Some of my earlier work has already been published. In the financial analysis of the ABIM, I was joined in my effort by Mr. Charles Kroll, a certified public forensic accountant specializing in health care non-profit organization accounting who has donated over 1500 hours of uncompensated time to this review. As our analysis has continued, other physicians have quietly come forward with additional information and personal stories of the impact of an ABIM sanction when the organization targets practicing physicians they feel are cheating while attempting to study for their unproven quality metric. I have reviewed the ABIM's federal Forms 990 from 1997 to the present and other sources including the internet archive (archive.org), IRS Form 1023, Guidestar.org, Brightscope.com, Pacer.gov, and called and emailed Dr. Baron to understand why my fees were so high and better understand why Dr. Baron is able to pay himself $812,000 per year (nearly four times the typical US internist salary) while the ABIM is $50,642,980 in debt according to its most recent Form 990 (line 22, "net assets and fund balances").
By expanding my review to the ABIM Foundation and other member boards of the American Board of Medical Specialties (ABMS) (of which the ABIM has the most physician diplomats), it became obvious that the problems I found at the ABIM were endemic to most of the United States physician credentialing system under the direction of the American Board of Medical Specialties (ABMS). For instance, the American Board of Pediatrics paid a $2.4 million golden parachute to their retiring 20-year veteran President and CEO, James A Stockman, III in 2012, yet still employed him two years later for $793,438 for working just eight hours a work-week: an almost incomprehensible $2066.24 per hour. Worse still, to the best of my knowledge and belief, all of these transgressions appear to have been conveniently ignored by the leadership of US medicine’s associated member organizations of the Accreditation Council of Graduate Medical Education (ACGME), including the American Medical Association, the Association of American Medical Colleges (AAMC), and the Council of Medical Subspecialty Societies (CMSS). The House of Medicine has become deeply divided between the bureaucratic elite of these organizations and those who struggle every day to do the real work of hands-on patient care.
After writing about by re-credentialing experience in 2013 on my blog, Dr. Wes (http://drwes.blogspot.com), my dive into the corrupt finances of the ABIM began in earnest 16 Dec 2014 with my article entitled "The ABIM Foundation, Choosing Wisely®, and the $2.3 Million Condominium." Since that time, a partial list of my ongoing investigation has uncovered the following:
- The ABIM Foundation, which was flush with over $47 million in cash when it was supposedly "created" in Iowa in 1999 (as disclosed on its tax forms from 2008 through 2013), was actually secretly created on October 17, 1989, in Pennsylvania. It has since been determined (and later acknowledged by the ABIM on their revised website) that the organization was funded by making multiple (undisclosed) transfers of ABIM diplomat fees from the ABIM (IRS Form 990's for the Foundation are unavailable for review because the ABIM had the IRS remove available tax forms after it changed the name of their Foundation from the "American Board of Internal Medicine Foundation" to the ABIM Foundation in 1999). Additional revenues were transferred from the ABIM from 1999 through 2007, culminating in the purchase of a $2.3 million luxury condominium complete with a chauffeur-driven Mercedes S-class town car in December of 2007. It remains unclear why a 501(c)(3) non-profit testing agency would purchase a condominium as an "investment" or for housing ABIM staff and directors when other cheaper options for housing exist in the Philadelphia area. The list of names of those who actually used the ABIM Foundation's condominium has never been publicly disclosed.
- One independent peer reviewed cost analysis of Maintenance of Certification has demonstrated the average cost for an internist to re-certify is $23,607 (95% CI, $5,380 to $66,383) and cost US physicians $5.7 billion in 2015. Despite all of these facts, the ABIM and ABMS managed to lobby Congress to have MOC included in the Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) as a physician quality measure even though 501(c)(3) organizations like the ABIM should have lost their tax-exempt status when they covertly participated in this activity, according to federal law.
- ABIM's own published Maintenance of Certification pass rates from 2000-2014 have demonstrated 13.2% of physician first-time test-takers failed their examination with large and inconsistent year-to-year pass rate volatility raising significant concerns of how the pass rate cut-off point is determined each year and the ABIM's motives for testing.
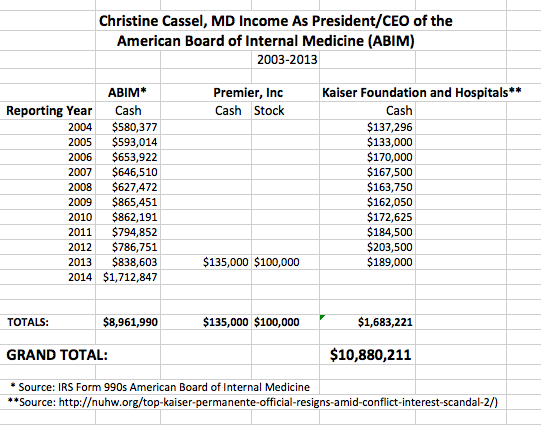
- Christine Cassel, MD, the former President and CEO of the ABIM and its Foundation from 2004-2014 earned over $8.9 million dollars over 11 years she worked at the ABIM for 35 hours per week and never disclosed her financial conflicts of interest while she simultaneously served on the boards of Premier, Inc., and Kaiser Hospital Health Plans until these relationships were disclosed after she left the ABIM to serve at the National Quality Forum. Despite these ethical lapses, Dr. Cassel still describes herself as a medical ethics "expert" and still serves as a consultant to the highest office in the land: the U.S. President's Council of Advisors on Science and Technology (PCAST) without Maintaining her own Certification status.
- The ABIM showers their executives with lavish perks on the backs of their physician diplomat fees. For instance, ABIM paid for spousal travel fees for Dr. Cassel for the ten-year duration of her term, even as residents and fellows struggle with the high fees for their certification while having record medical education debt.
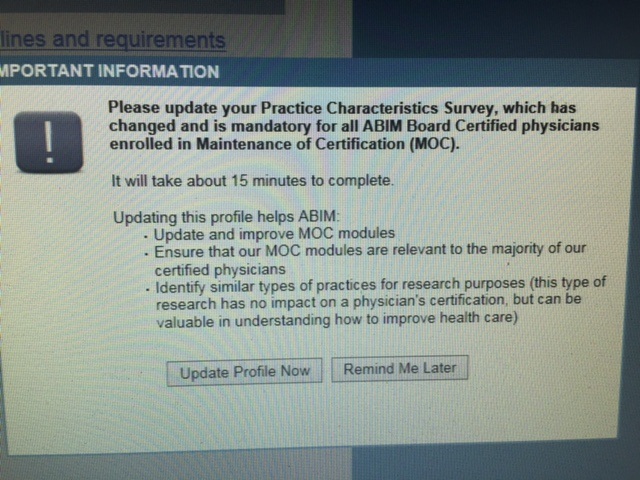
- The ABIM website registration requirements and registration agreement used for their MOC program, ABIM and the ABIM Foundation routinely conduct "research" on physicians and their practices without a research protocol, Investigational Review Board review, or informed consent in violation of FDA and Health and Human Services Protection of Human Subject statutes. Note that the enrollment agreement (no longer found on the current ABIM website) stated: "I understand that the ABIM may use my examination performance, training program evaluations, self-evaluations of knowledge and practice performance, and other information for research purposes, including collaboration with other research investigators and scientific publications." There is no mistaking the ABIM was (and still is) conducting "research" on their diplomats for their benefit.
- Robert Wachter, MD, former President of the ABIM Foundation, earned stock options from the IPC Hospitalist Company while serving at the ABIM Foundation. While it is unclear what role Dr. Wachter played at IPC Hospitalist Company, the company remains under federal investigation for Medicare fraud.
- From 2010-2014, the ABIM paid a little-known company to the practicing physician community, CECity, $5,568,538 for their services. Just before leaving ABIM, Dr. Christine Cassel received $130,000 in cash and $100,000 in stock from Premier, Inc, that then announced its purchase of CECity for $400 million a short time later on August 4, 2015.
- The ABMS plans to sell physician certification data to a multitude of parties at ABMSSolutions.com and offer subscriptions to its CertiFACTS Online product (video). Funny how Dr. Baron and his colleagues at the ABMS fail to disclose this fact to major medical journals and Medical Economics when they are interviewed or publish their articles promoting the need for physician re-certification.
- Since 1 January 2014, to facilitate the coverup of its operations and to limit transparency, the ABIM no longer permits archived webpages to be stored on a regular basis on the Wayback Machine at archive.org as seen by the absence of archived webpages after that date.
These are just a small sampling of the serious problems that have been uncovered by careful review of the ABIM's actions, ongoing cover-ups, and propaganda inherent to the ABMS MOC program that Dr. Baron supports. Legal fees (all paid by ABIM diplomats) are mounting against the ABIM and the ABMS member boards as they attempt to defend an antitrust lawsuit brought against them, attempt to sanction even more physicians, and have more threats legal action from the Pennsylvania Medical Society’s recent announcement of a vote of no confidence against the organization at the AMA House of Delegates Meeting in June of this year.
Practicing US physicians don't need any more propaganda from Dr. Baron in Medical Economics promoting the ABIM's Maintenance of Certification program, we need a careful independent audit of their finances and a thorough investigation of the ABIM and their collaborating organizations by appropriate authorities to end this unjustified, highly corrupt, and conflicted ABMS MOC program nationwide.
Westby G. Fisher, MD
Director, Cardiac Electrophysiology,
NorthShore University HealthSystem, Evanston, Illinois
Clinical Associate Professor of Medicine
Pritzker School of Medicine
University of Chicago
{kind=link}
{kind=link}
Monday, September 05, 2016
How the ABMS MOC Program Threatens Major Medical Journal Integrity
They are two of the most prestigious academic journal's in the United States: the New England Journal of Medicine (NEJM) and the Journal of the American Medical Association (JAMA). Both have published extensively on the American Board of Medical Specialties' (ABMS) Maintenance of Certification (MOC) program. Both have clear rules requiring full disclosure of conflicts of interest: the NEJM has its Integrity Safeguards and JAMA, like the NEJM, follow the conflict of interest disclosure recommendations (pdf) of the International Committee of Medical Journal Editors.
But what happens when authors who are widely published in these journals fail to disclose financial relationships that are more than de minimus? Are articles retracted? Are authors sanctioned? Or are conflicts that also benefit the bottom line of one of these medical journals just ignored?
Take, for instance, this article that was recently published in the NEJM: "Maintenance of Certification 2.0 — Strong Start, Continued Evolution" written by Mira B. Irons, MD and Lois M. Nora, MD. The disclosures of the authors reveal that "Dr. Irons reports being employed by the American Board of Medical Specialties" and "Dr. Nora reports being an employee of the American Board of Medical Specialties, and being a coauthor on work describing the American Board of Medical Specialties Maintenance of Certification program." In another correspondence, Drs Norris and Nora, both of the ABMS, disclosed "Dr. Norris reports being on the board and Dr. Nora reports being the president and chief executive officer of the ABMS. No other potential conflict of interest relevant to this letter was reported." In JAMA in August 2015 entitled "American Board of Internal Medicine and Maintenance of Certification Standards," a similar disclosure only lists Dr. Nora's affiliation with the American Board of Medical Specialties.
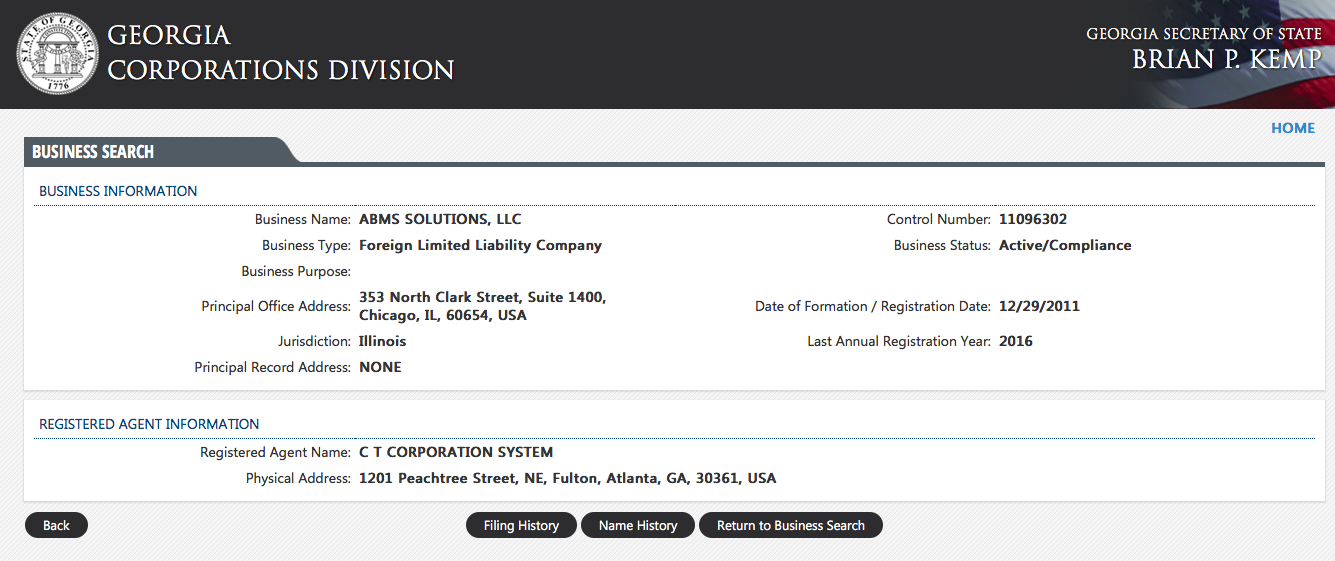
What was never publicly disclosed by either of these major medical journals was the authors' significant financial relationship with the Georgia-registered Foreign Limited Liability Corporation, ABMS Solutions, LLC (Control number 11096304), whose office address exactly matches that of the American Board of Medical Specialties in Chicago, IL. Furthermore, Dr. Nora, as President and CEO of the ABMS, never mentions the congressional lobbying the ABMS conducted with members of the Congressional Energy and Commerce Committee to solidify their MOC program as a "quality" standard for "800,000 licensed US physicians," to assure virtually unlimited funding of their organization through the sale of primary source verification of physician certification status to third parties via ABMS Solutions, LLC.
It is no secret that the New England Journal of Medicine also earns money for the sale of educational products for the ABMS Maintenance of Certification program through their 'NEJM Knowledge+' educational product. This relationship makes the NEJM's response more economically difficult for them. But if the NEJM and JAMA fail to actively address the failure of ABMS authors to publicly disclose their multiple significant financial conflicts with the ABMS MOC program at the time they submitted their manuscripts, they risk compromising their own integrity with the entire international medical community.
-Wes
P.S.: I contacted the New England Journal of Medicine letter editor to make them aware of these conflicts. They are currently evaluating the situation.
11:05 CST 9/6/2016 - Link to the Georgia corporate registration fixed.
Addendum: For follow-up of the letters I sent to JAMA and New England of Journal Medicine regarding the perceived ABMS conflicts, click here.
But what happens when authors who are widely published in these journals fail to disclose financial relationships that are more than de minimus? Are articles retracted? Are authors sanctioned? Or are conflicts that also benefit the bottom line of one of these medical journals just ignored?
Take, for instance, this article that was recently published in the NEJM: "Maintenance of Certification 2.0 — Strong Start, Continued Evolution" written by Mira B. Irons, MD and Lois M. Nora, MD. The disclosures of the authors reveal that "Dr. Irons reports being employed by the American Board of Medical Specialties" and "Dr. Nora reports being an employee of the American Board of Medical Specialties, and being a coauthor on work describing the American Board of Medical Specialties Maintenance of Certification program." In another correspondence, Drs Norris and Nora, both of the ABMS, disclosed "Dr. Norris reports being on the board and Dr. Nora reports being the president and chief executive officer of the ABMS. No other potential conflict of interest relevant to this letter was reported." In JAMA in August 2015 entitled "American Board of Internal Medicine and Maintenance of Certification Standards," a similar disclosure only lists Dr. Nora's affiliation with the American Board of Medical Specialties.
What was never publicly disclosed by either of these major medical journals was the authors' significant financial relationship with the Georgia-registered Foreign Limited Liability Corporation, ABMS Solutions, LLC (Control number 11096304), whose office address exactly matches that of the American Board of Medical Specialties in Chicago, IL. Furthermore, Dr. Nora, as President and CEO of the ABMS, never mentions the congressional lobbying the ABMS conducted with members of the Congressional Energy and Commerce Committee to solidify their MOC program as a "quality" standard for "800,000 licensed US physicians," to assure virtually unlimited funding of their organization through the sale of primary source verification of physician certification status to third parties via ABMS Solutions, LLC.
{kind=link}
It is no secret that the New England Journal of Medicine also earns money for the sale of educational products for the ABMS Maintenance of Certification program through their 'NEJM Knowledge+' educational product. This relationship makes the NEJM's response more economically difficult for them. But if the NEJM and JAMA fail to actively address the failure of ABMS authors to publicly disclose their multiple significant financial conflicts with the ABMS MOC program at the time they submitted their manuscripts, they risk compromising their own integrity with the entire international medical community.
-Wes
P.S.: I contacted the New England Journal of Medicine letter editor to make them aware of these conflicts. They are currently evaluating the situation.
11:05 CST 9/6/2016 - Link to the Georgia corporate registration fixed.
Addendum: For follow-up of the letters I sent to JAMA and New England of Journal Medicine regarding the perceived ABMS conflicts, click here.
Subscribe to:
Posts (Atom)