The Facebook–Cambridge Analytica data scandal was a major political scandal in early 2018 when it was revealed that Cambridge Analytica had harvested the personal data of millions of peoples' Facebook profiles without their consent and used it for political advertising purposes. The scandal, first exposed by The Guardian in 2015, revealed that Cambridge Analytica had managed to obtain data on millions of Facebook users in the UK, US, and beyond, made possible through "improper sharing" practices conducted between the "This Is Your Digital Life" Facebook app developer and the company. By giving this third-party app permission to acquire their data, back in 2015, this also gave the app access to information on the user's friends network; this resulted in the data of about 87 million users, the majority of whom had not explicitly given Cambridge Analytica permission to access their data, being collected.
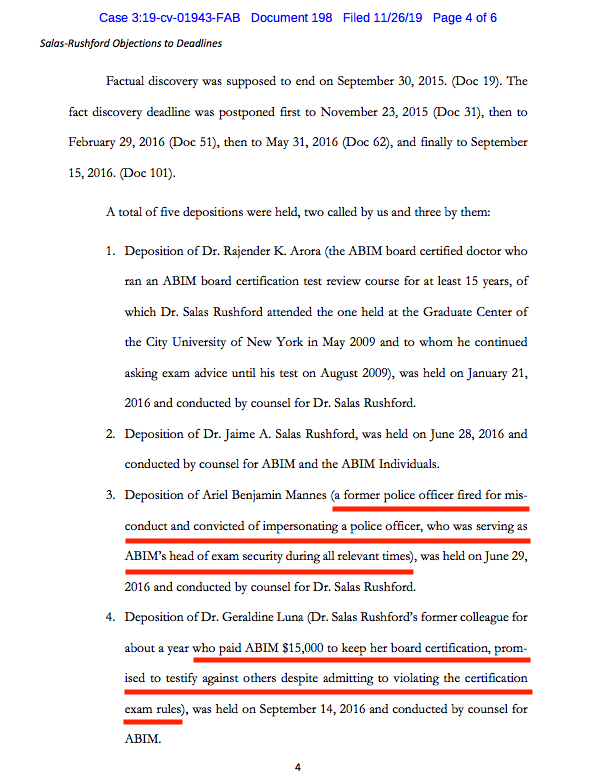
Because patients do not give consent for the use of their data, who better to target for access to sensitive patient-related information than those entrusted with their care? As details come to light about the American Board of Medical Specialties' (ABMS) Maintenance of Certification (MOC) program that has plagued physicians since 1990, many similarities to the Cambridge Analytica data-sharing scandal are appearing. The
adhesion contract that forms the basis for MOC and is increasingly tied to physician hospital privileges and insurance reimbursements, assures this data pipeline remains open:
I also understand that ABIM may use my examination performance, training program evaluations, self evaluations of knowledge and practice assessment, and other information for research purposes, including collaboration with other research investigators and scientific publications."
Unbeknownst to most physicians, the ABMS has been
involved with the sale and sharing of physicians' demographic and sensitive MOC data with third parties for years. Each clinical physician in the United States may see 2000-3000 patient's each annually. Marrying physician data with their patient's data and targeting patient markets becomes possible with physician-specific MOC information. Procedural and pharmaceutical data allows medical suppliers, pharmaceutical companies, device companies, and others virtually unlimited opportunities to sell their products while optimizing most their bottom lines through increased sales and offering rebates to health care facilities (aka,
kickbacks).
Group purchase organizations (GPOs) and Pharmacy Benefit Managers (PBMs) decide what equipment appears on a database for hospitals to purchase. Companies pay those GPOs and PBMs to be on the list. Doctors' equipment choices and pharmaceutical preferences influence that list. Companies want to know what doctors are using and who doctors are seeing. By knowing their patterns and knowing the procedures performed on patients, highly sensitive patient information can be deduced. Registries owned by procedurally-heavy specialty societies (like the American College of Cardiology) are a particularly ripe source of procedural data, particularly when it can be made doctor-specific (where MOC comes in). More data sales occur. Repeated MOC testing and demographic data entries required by physicians assures these physician-specific databases are kept current. Having the President and CEO of the American Board of Internal Medicine on the President's Council of Advisors for Science and Technology
assured uninterrupted marketing access to physicians and their patients.
By using physician information and their patient care information for these corporate purposes, the ABMS/ABIM MOC® product looks more like Cambridge Analytica than a physician education tool and affects far more people's health care than the Cambride Analytica ever did.
So how how do all these organizations coordinate and connect their MOC data, registries, and corporate databases?
Through a virtually undisclosed tax-exempt AMA-funded private foundation shamelessly called the
Physician Consortium for Performance Improvement (PCPI).
Reportedly formed in 2000 with the help of the AMA, the PCPI Foundation is located just blocks away from the AMA's corporate headquarters in downtown Chicago. The organization
describes itself as follows:
The AMA-convened PCPI, in partnership with its members, has developed more than 350 measures, many of which are used in the Physician Quality Reporting System (PQRS) and Meaningful Use, as well as private health plan payment models. (emphasis mine)
In 2011, American Medical Association staff to the PCPI worked with a group of committed volunteer leaders to launch the NQRN®, a national, multi-stakeholder network of clinical registry stewards and others interested in registries. The NQRN has created tools and educational opportunities and increased the visibility and value of clinical registries as reporting and improvement systems. In 2016 NQRN was merged into the PCPI as a key program. In 2013, the AMA-convened PCPI launched the PCPI Quality Improvement Program to support its members improvement needs beyond measurement.
In 2014, the AMA and AMA-convened PCPI leadership undertook an evaluation to determine the optimal governance structure to meet the growing demand for value-based health care. The result of this evaluation was the adoption of new By-Laws in June 2015, which set the course for the PCPI Foundation (PCPI), an independent organization with an expanded membership.
Not surprisingly, it's Board of Directors is lead by John S. McIntyre, MD of the American Psychiatric Association, who has never participated in MOC and is not required to do so:
The remainder of the Board of Directors include:
- Thomas Granatir, MD, Senior Vice President for Policy and "External Relations" of the ABMS (formerly from Humana)
- Lewis G. Sandy MD, FACP of the UnitedHealth Group
- Non-physician Nancy E. Lundebjerg, MPA of the American Geriatric Society (Vice Chair)
- Non-physician Laura J. Cranston, RPh of the Pharmacy Quality Alliance (Secretary)
- Non-physician Dianne V. Jewell PT, DPT, PhD, FAPTA of the American Physical Therapy Association (Treasurer)
- Larry A. Allen, MD, MHS of the American Heart Association
- Bruce S. Auerbach MD, FAECP of the American College of Emergency Physicians
- Arlene S. Bierman MD, MS of the Agency for Healthcare Research and Quality
- Claire Bradley, MD, MPH who oversees "Quality Improvement"
- Non-physician Carol A Cronin MA, MSW of the Informed Patient Institute
- Non-physician Melissa Danforth of the Leapfrog Group
- E. Scott Ferguson, MD - A radiologist on the AMA Board of Trustees and AMA representative to the National Quality Forum but does not appear to participate in MOC.
- Deeraj Mahajan, MD FACP, CMD, CIC, CHCQM ("Certified Medical Doctor, Certified Infection Control, Certified Health Care Quality Measures") of the Medical Specialty
- Lawyer Melanie G. Phelps JD of the North Carolina Medical Society who previously worked in the Government Affairs Department of Blue Cross Blue Shield
- Non-physician Aisha T. Pittman MPH of Premier, Inc, the largest hospital Group Purchase Organization
- Amir Qaseem MD, PhD, MHA, FACP of the American College of Physicians
- Martha J. Radford, MD FACC, FAHA of the American College of Cardiology
- David Shahian MD of the Society of Thoracic Surgeons
- Computer Scientist Kurt Skifstad, PhD CEO of ArborMetrix, a data analytics company
- Sandra Adamson Fryhofer, MD MACP from the Board of Trustees of the AMA
- Richard D. Zorowitz MD, FAAPMR of the American Academy of Physician Medicine and Rehabilitation
Members get to "access the latest tools and insights on performance measurement, clinical registries, and quality improvement" as well as "influence through representation on the PCPI board, committees, advisory and other, as well as expert panels and task forces."
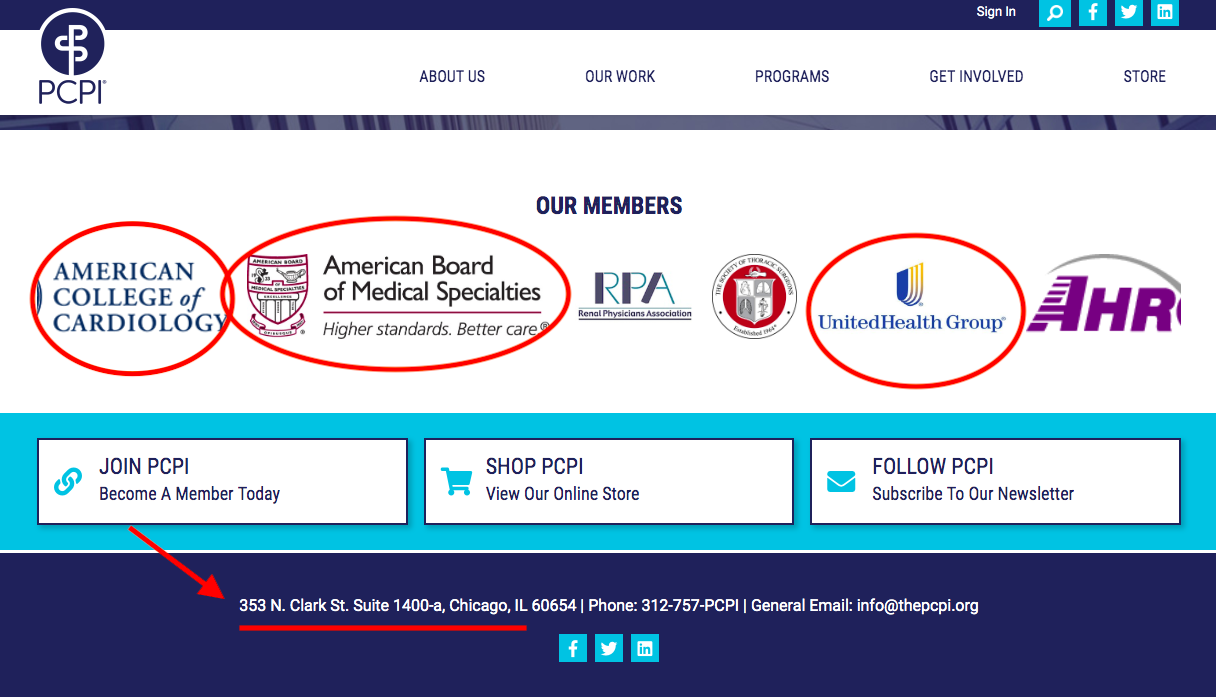
Members of this organization, according to the revolving banner on the PCPI website, include:
AvaMed,
FigMD (MOC data collectors), AMA, ACP, ACC, ABMS, Informed Patient Institute, CMSS, Am Society of Clinical Oncology, The American Health Quality Association, Am College of Occupational Medicine,
Primaris (A healthcare consulting and data abstraction company), American Academy Foot and Ankle Orthopedics Society,
UnitedHealth Group (Market cap: $262B), The Society of Thoracic Surgeons, Pharmacy Quality Alliance, American Gastroenterology Association, Health Care Services Platform, American Optometric Association, Academy of Nutrition and Dietetics, American Heart Association, American College of Radiology, and on, and on...
It's handsomely paid CEO and Executive Director, Kevin Donnelly, is a non-physician, too. Here's their latest
2017 IRS filing that confirms a cool $2.78M contribution from the AMA to the PCPI and contains this explanation why the organization is not a true public "charity" after all:
The organization is filing this 990PF after the extended due date of November 15, 2018 (extension was for Form 990). Upon completion of schedule it was determined that the public support test had not been met for the second year. Research into IRS code and regulations was done to determine the next steps, which took the organization past the due date. The organization did not intentionally disregard the filing requirement, but rather, took time to ensure that that (sic) the appropriate filings were being made. Going forward, now that the requirements are understood, all 990PF filings will be timely. Additionally the organization properly extended the 2018 return as fling a Form 990PF.
I'm sensing some BS here, but I'll leave that to my readers (and the IRS) to decide.
Are UnitedHealth, Humana, Blue Cross Blue Shield, Premier, AvaMed (and all the medical device companies they represent), FigMD, and Primaris really about "quality" or their own bottom line?
Is there any wonder, then, that when a physician
points out certain conflicts to medical editors of the Journal of the American Medical Association (JAMA) or the New England Journal of Medicine (owned by the Massachusetts Medical Society), he can't get a straight answer and is referred by the conflicted party to IRS tax filings?
One thing's for sure, to the best of my knowledge and belief, these multiple organizations are colluding with each other for their own best interests ("covert rationing" - a concept
coined by the prescient Dr. Richard Fogoros) and using our physician MOC® data to drive their bottom lines while hiding behind non-profit tax law and the ruse of assuring the public it's all in the name of "quality."
-Wes








{kind=link}
{kind=link}