After its initial public humiliation, the American Board of Internal Medicine (ABIM) had to re-group and admit they "got it wrong." But as far as the practicing physician community was concerned, the apology was lukewarm at best. Instead of taking full responsibility for their financial transgressions, the organization continues to deflect and pretend the problem is their Maintenance of Certification (MOC) program. Friday they issued an update asking for more "feedback" as they recruit new "specialty advisers" to appear more clinically relevant. I've had a chance to discuss my concerns with Yul Ejnes, MD, one of their specialty advisors for internal medicine, by phone. After speaking for nearly an hour, it was clear to me that the ABIM is rightfully concerned. It was also clear to me that "specialty advisors" are far down the governance food chain of the ABIM.
The Deeper Problem
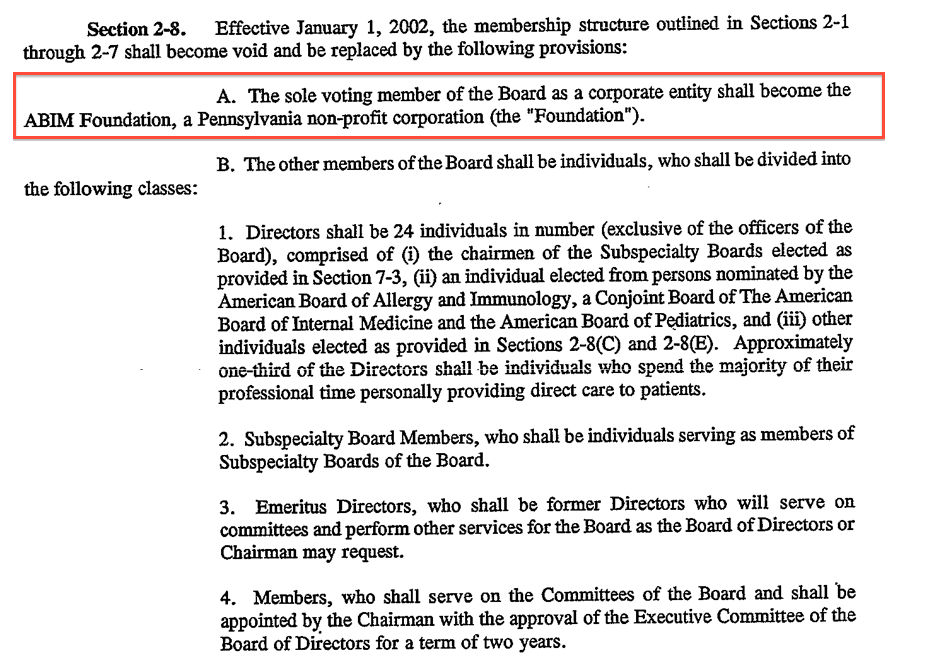
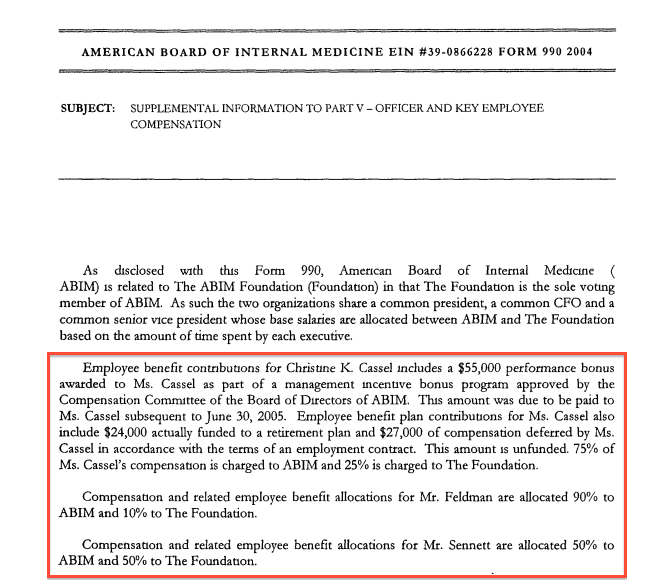
Unfortunately feedback and recruiting efforts won't fix what ails the ABIM and the MOC program in general. There is a much deeper problem. On October 6, 1998, the ABIM, the certification body that overseas approximately one quarter of practicing US physicians, revised their bylaws. Since then, the ABIM has allowed unlimited financial and business conflicts of interest to exist with their board members. One only has to see the effects of those conflicts after Christine Cassel, MD, supposedly a full-time member of the ABIM for 10 years, was forced to divest herself from those long-standing cozy relationships when she transferred jobs to the National Quality Forum, an agency that receives the bulk of its revenues from government contracts. That change also made their own ABIM Foundation the sole voting member of the board as a corporate entity after January 1, 2002, a troubling conflict itself. (Other board members are individuals, but the conduct and management of the affairs of the Board is vested solely in the Board of Directors and the Staff Members of the Board.)
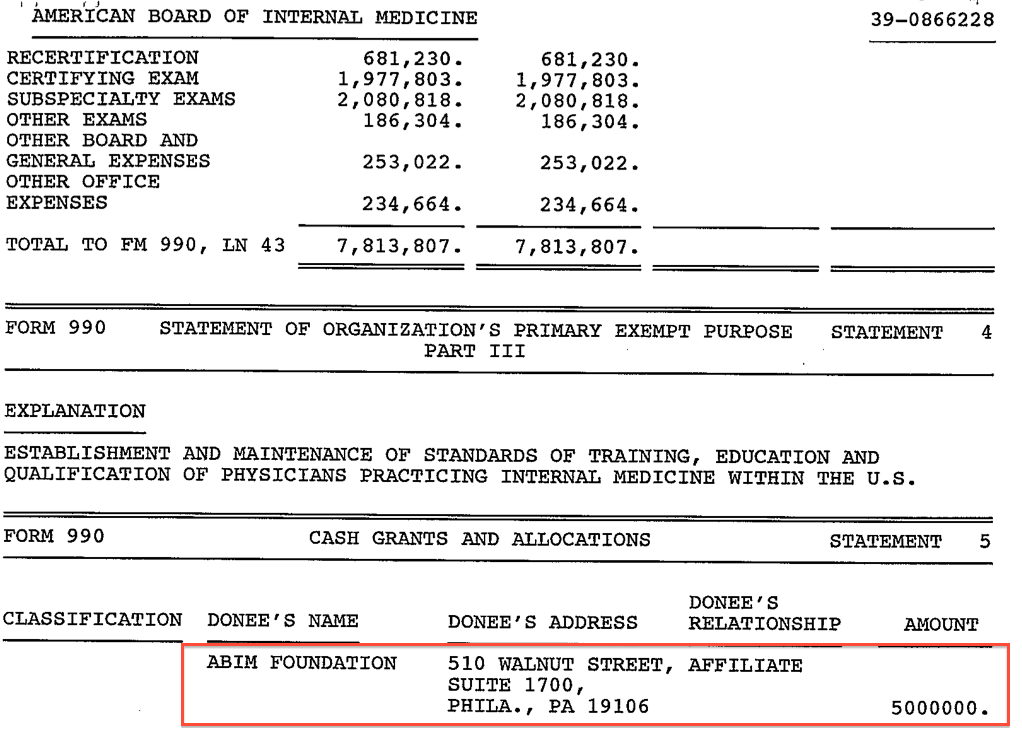
Then, from 1998 through 2007 for reasons that are unclear, the ABIM repeatedly funneled physician testing fees in the form of "grants" to their Foundation to the tune of $30,600,000 (1998 - $5,000,000; 1999 - $5,000,000; 2000 - $3,300,000; 2001 - $1,600,000; 2002 - $1,000,000; 2003 - $1,760,000; 2006 - $7,000,000; 2007 - $6,000,000).
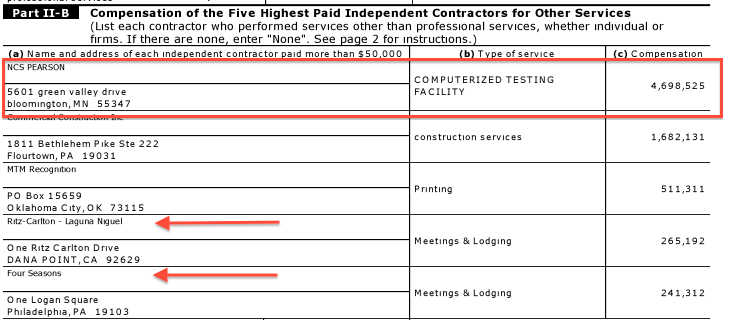
And the ABIM's spending didn't end there. Because the ABIM has no obligation to disclose their relationships to the public or their diplomats they have spent without oversight. In 2007 alone they helped purchase a $2.3 million luxury condominium, and spent $5.2 million to outsource testing centers while they held posh "meetings" at fancy hotels like the Four Seasons, Philadelphia and the Ritz-Carlton, Laguna Niguel. They also occasionally give themselves a bonus. It is this problem of feeding their constituents over their practicing physician consumers that lies at the core of the problems at the ABIM, irrespective of their efforts to change the MOC program.
Ethical Double-Standards
In 2010 while the annual multimillion dollar physician fee transfers were well underway, the ABIM decided to sue five physicians and sanctioned 134 others who allegedly participated in the Arora Board Review Course that allegedly copied paraphrased questions from the ABIM's high-stakes secure examination. Many physician careers were ruined as a result. No doubt many of their patients were affected too. Christine Cassel, MD, the President and CEO of the ABIM at the time, published a press release that admonished the physicians' behavior saying: "Ethics are critical to the practice of medicine and are the foundation
of a successful doctor-patient relationship. We will not tolerate
unethical behavior from physicians seeking board certification" while conveniently failing to mention the physician testing fee fund transfers to their Foundation. Likewise, they've amassed millions for themselves and their political agendas in their Foundation, while demanding that physicians to skimp on necessary tests for their patients in the name of "public good," lest they be labeled "unprofessional."
We can only ponder what the ABIM has to say about their own ethics now.
Next Steps
What the ABIM fails to grasp is that all of the MOC "modifications" in the world won't change these facts. As a result, the ABIM has officially been rendered irrelevant to the practicing physician community. Doctors are moving on and hospitals and insurers will need to adapt. If physicians lose their credentials or ability to practice because of MOC, they will sue. And given these many transgressions, I'm betting they'll win.
It's a new day now. Practicing doctors are watching. Practicing doctors are feeling the squeeze from all the forces that are being placed upon them. So practicing doctors are starting to act. While it is uncertain how far-reaching their actions will become, one thing that is clear is this:
… a sleeping bear has awakened.
-Wes
Monday, March 30, 2015
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Friday, March 27, 2015
Is the Medicare "Doc Fix" Really So Appealing?
It was like magic, a vote was held in the House of Representatives on the Medicare "Doc Fix" and moments later, my inbox was filled with press releases from the American College of Cardiology and the AMA. A few seconds later, a somewhat more tempered press release from AARP arrived, urging more revisions to the bill as it passed to the Senate for approval.
This isn't the first time in history Medicare has changed how it pays physicians. Nor will it be the last. But practicing physicians should be fully aware of what the new bill has in store for us. After all, busy physicians aren't necessarily working on the latest legislative efforts on Capitol Hill.
So it should come as no surprise that working doctors (and the patients they treat) are on the doctor payment menu rather than truly sitting at the legislative negotiating table. From the National Review:
Patients will lose doctors and doctors will lose parts of their careers as this "fix" is enacted.
-Wes
This isn't the first time in history Medicare has changed how it pays physicians. Nor will it be the last. But practicing physicians should be fully aware of what the new bill has in store for us. After all, busy physicians aren't necessarily working on the latest legislative efforts on Capitol Hill.
So it should come as no surprise that working doctors (and the patients they treat) are on the doctor payment menu rather than truly sitting at the legislative negotiating table. From the National Review:
Some Republicans are also enthusiastic about the “reforms” the bill would make to Medicare’s physician-payment system. They shouldn’t be. Today’s system is the result of three decades of technocratic good intentions gone terribly awry. In 1989, Congress adopted the “resource-based relative value scale” as the fundamental building block for determining physician fees. The new system was supposed to accurately assess how much time, effort, and training physicians put into taking care of a patient, and pay them accordingly. The result has been arbitrary and irrational payments that have heavily favored procedure-driven medicine over prevention and primary care.When the federal government is "going to find a way to pay doctors based on quality and value," ask yourself one question: "Value" to whom?
Now we are told that the federal government is going to find a way to pay physicians based on quality and value, using all manner of new technocratic methods to do so. Data will be collected, expert panels convened, and regulations issued, and supposedly that will lead to a better system of physician payments. But there’s no reason to believe the Medicare bureaucracy will be any better in the future than it has been in the past in setting physician fees. The real danger here is that the federal government will use the new authorities provided in the law to become the official arbiter of what constitutes “quality” in physician care. That’s a recipe for getting the exact opposite of what the law’s authors intend.
As to the “reforms” in Medicare, there’s far less there than one might hope. The first provision would only modestly adjust upward the premium payments for a small number of upper-income households. Elderly couples with incomes between $267,000 and $320,000 per year would see their Medicare premiums rise from 50 to 65 percent of the value of their Part B insurance. Couples with incomes above $320,000 but below $428,000 would see their premiums rise from 65 to 75 percent of the implicit total premium for their coverage. What’s important to remember about these kinds of reforms is that the elderly are generally retired. They aren’t working, and many of them are living off their accumulated savings, which they draw on as needed. They don’t have substantial incomes, even if they have substantial assets. So income-tested premiums of the kind envisioned in the SGR deal affect very few people — only 2 percent of all Medicare beneficiaries. And the provision doesn’t become effective until 2018.
Patients will lose doctors and doctors will lose parts of their careers as this "fix" is enacted.
Consider calling your Senator at 1-877-996-4464 and ask them that question: "'Value' to whom?"
If they stumble, even momentarily, ask them to vote "no."
-Wes
Tuesday, March 24, 2015
Money for Nothing
Imagine paying $4,675 for a piece of paper. It would make the days of $436 military hammers look pretty cheap, wouldn't it?
Now imagine that piece of paper comes with a promise of having to pay more for your own good and where time spent acquiring that paper meant nothing. Most rational people would have visions of Bernie Madoff or some other Ponzi scheme.
Yet this is the reality of the American Board of Medical Specialties' Maintenance of Certification (MOC) program for practicing US physicians.
I recently went throughout the Maintenance of Certification process in 2013. I sat for both by Cardiovascular Diseases Certification (that expired in 2013) and Clinical Cardiac Electrophysiology recertification (that expired in 2014) secure examinations in October of 2013. Here's what I got for my cardiovascular recertification fees:
Note that because the cardiovascular certificate was renewed in 2013, it now was extended from 2013 through 2023. The cover letter that came with the new Cardiovascular Disease certificate was also notable for the three references its cited as "proof" of the value of these certificates. The three references were (1) Arch Intern Med 2010; 170(16): 1442-9, (2) Arch Intern Med 2009 (sic - Editor's note: actually 2008) 168: 1396-1403 and (3) JAMA 2005 294(4): 473-81.
Reference (1) concludes that "Publically available characteristics of individual physicians are poor proxies for performance on clinical quality measures." Reference (3) is a cross-sectional retrospective analysis of data on US physician respondents to the 2000-2001 Community Tracking Study linked to Medicare beneficiaries they treated in 2001 that only generated the hypothesis that "profiling practices may help develop tailored interventions that can be directed to sites where the opportunities for quality improvement are greatest."
But the worst reference was Reference (2). This reference is notable in part because of the glaring and inexcusable conflict of interests of every author on the manuscript. Each author was either a paid member of ABIM or an employee of Qualidigm of Middletown, CT, a data analytics firm that does the following according to its website:
Because my Cardiac Electrophysiology certificate expired in 2014, doctors should be aware of the changes that have occurred to board certificates. I recieved this new certificate after passing by secure examination and countless hours collecting survey data, attending board review courses, and reading enough material to put the Encyclopedia Britannica to shame:
Note the fine print below the words "Clinical Cardiac Electrophysiology:"
Sorry, but I will never recertify and participate in this Ponzi scheme again.
Ever.
-Wes
Now imagine that piece of paper comes with a promise of having to pay more for your own good and where time spent acquiring that paper meant nothing. Most rational people would have visions of Bernie Madoff or some other Ponzi scheme.
Yet this is the reality of the American Board of Medical Specialties' Maintenance of Certification (MOC) program for practicing US physicians.
I recently went throughout the Maintenance of Certification process in 2013. I sat for both by Cardiovascular Diseases Certification (that expired in 2013) and Clinical Cardiac Electrophysiology recertification (that expired in 2014) secure examinations in October of 2013. Here's what I got for my cardiovascular recertification fees:
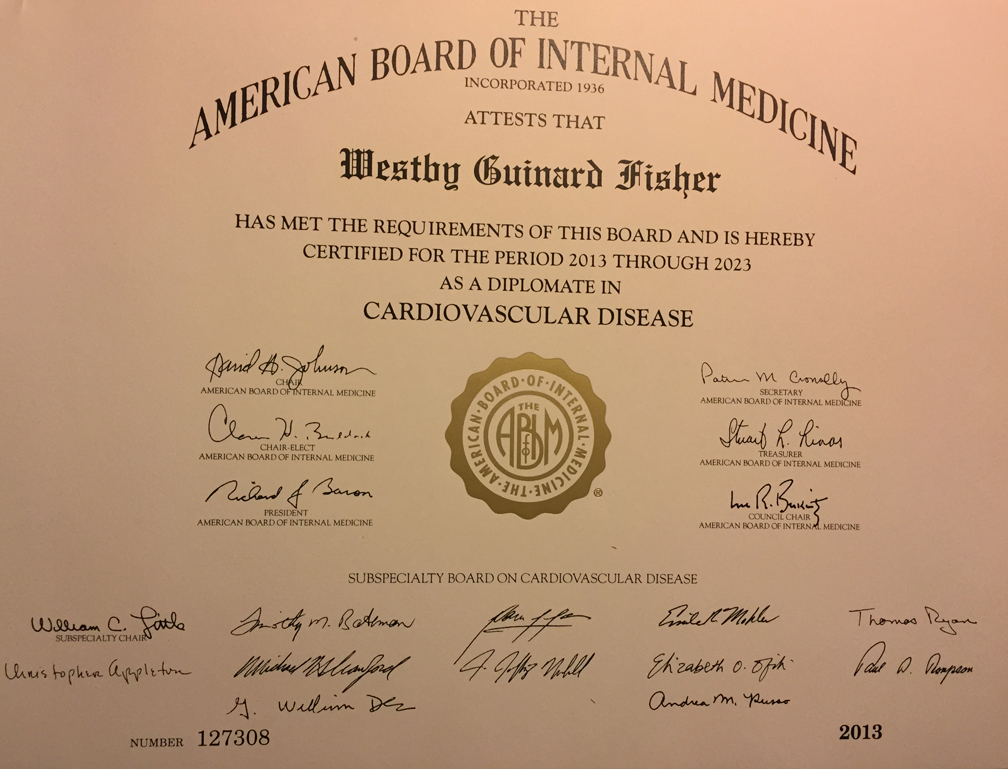 |
| ABIM Cardiovascular Disease Certificate 2013 - Click to enlarge |
Note that because the cardiovascular certificate was renewed in 2013, it now was extended from 2013 through 2023. The cover letter that came with the new Cardiovascular Disease certificate was also notable for the three references its cited as "proof" of the value of these certificates. The three references were (1) Arch Intern Med 2010; 170(16): 1442-9, (2) Arch Intern Med 2009 (sic - Editor's note: actually 2008) 168: 1396-1403 and (3) JAMA 2005 294(4): 473-81.
Reference (1) concludes that "Publically available characteristics of individual physicians are poor proxies for performance on clinical quality measures." Reference (3) is a cross-sectional retrospective analysis of data on US physician respondents to the 2000-2001 Community Tracking Study linked to Medicare beneficiaries they treated in 2001 that only generated the hypothesis that "profiling practices may help develop tailored interventions that can be directed to sites where the opportunities for quality improvement are greatest."
But the worst reference was Reference (2). This reference is notable in part because of the glaring and inexcusable conflict of interests of every author on the manuscript. Each author was either a paid member of ABIM or an employee of Qualidigm of Middletown, CT, a data analytics firm that does the following according to its website:
Collecting relevant data, turning that data into information, and that information into action, drives almost every Qualidigm initiative and contract.So it appears that Qualidigm's authors (and the purpose of these certificates and entire MOC program) was manufactured not only for the money it creates for these boards, but for insurance company claim denials.
Qualidigm analysts have the qualitative and quantitative knowledge, skills and experience to provide a wide range of services including but not limited to:
- the analysis of claims data from a single source or aggregating claims data from multiple sources;
- the collection, integration and analysis of claims data, administrative data and medical records data;
- the geographic analysis of various types of databases, e.g., claims, medical records;
Because my Cardiac Electrophysiology certificate expired in 2014, doctors should be aware of the changes that have occurred to board certificates. I recieved this new certificate after passing by secure examination and countless hours collecting survey data, attending board review courses, and reading enough material to put the Encyclopedia Britannica to shame:
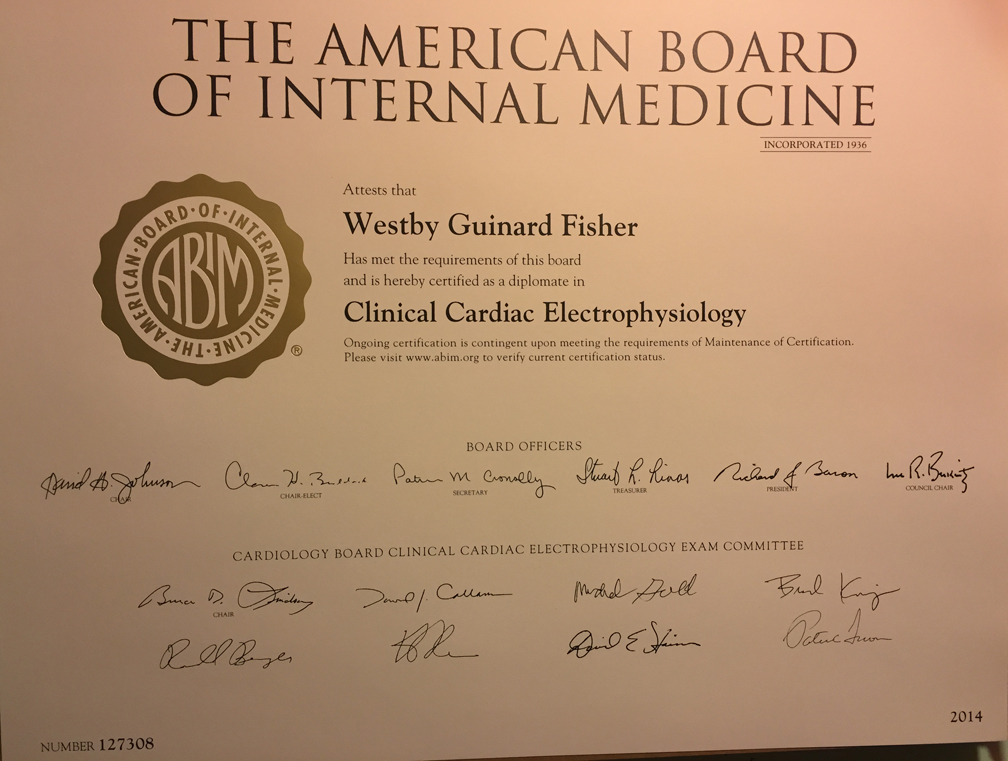 |
| ABIM Clinical Cardiac Electrophysiology Certificate 2014 - Click to enlarge |
Note the fine print below the words "Clinical Cardiac Electrophysiology:"
"Ongoing certification is contingent upon meeting the requirements of Maintenance of Certification. Please visit www.abim.org to verify certification status."In essense the new 2014 (and later) "Maintenance of Certification" certificates are nothing more than very expensive hyperlinks to the ABIM.org website.
Sorry, but I will never recertify and participate in this Ponzi scheme again.
Ever.
-Wes
Friday, March 20, 2015
Heart Rhythm Society and MOC: It's Not About the Doctors
 |
| Dr. Fogel |
From Dr. Fogel's announcement, it appears the Heart Rhythm Society is carefully choosing its words so as not to seem too adversarial to the ABIM by recommending (1) the removal of the requirement of being dual-MOC certified in BOTH cardiology and cardiac electrophysiology, (2) permanently ridding electrophysiologists of having to perform the busy-work of "practice improvement modules" and (3) "continuing the discussion" at a later time.
While Dr. Fogel's statement is pleasant and forthright, those are not exactly fighting words.
Dr. Fogel also announced a "debate" on MOC that will take place at the Heart Rhythm Society Scientific Sessions being held in Boston in May of this year. It will be moderated by Mike Gold, MD with Doug Zipes, MD as the pro-MOC advocate and Fred Kusumoto, MD taking the contrary argument. I'm sure the session will be well-attended and, who knows, maybe a few carefully-selected questions will be hand-picked from the audience! But will the "debate" do anything? No.
 |
| MOC Debaters? |

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Please note that the ABIM still has not publicly posted their 2014 Form 990 (due Feb 17, 2015). It is clear they want to wait as long as possible to do so. But even with an extension, the form must be filed by May 15, 2015, the day before the 2015 HRS Scientific Sessions end. It's very hard to have a "debate" on MOC when all the facts on the finances of the ABIM remain cloaked in secrecy, too.
Physicians should remember that just because the 0.5% incentive payment from Medicare to physicians who participated in the MOC ended 1 Jan 2014, it doesn't mean the coercive practice has gone away. Through their many political supporters, the ABMS made sure that MOC remained a component of the Medicare Physician Quality Reporting System (PQRS) as a part of the Center for Medicare and Medicaid Services (CMS) "Physician Compare" initiative. The majority of US physicians are now employed by hospitals eager to compete for a growing number of newly-insured patients. As such, hospitals are increasingly requiring physicians to participate in MOC as a condition for gaining credentials in their hospital. By even pretending to side with any form of MOC, the Heart Rhythm Society tactically agrees that MOC may continue to coerce money from their own physician consumers for the their benefit and that of ABMS's constituents.
Let's be clear: MOC is not a doctor issue, it's a political issue.
It is remarkable that the US government is now the only government in the world that officially requires repeated "re-certification" of physicians for them to practice medicine. Thanks to MOC, it is also the only government in the world that acts as imprimatur to an unproven pay-to-play scheme.
Doctors are done playing this game. It's time for HRS to stop the faux debating and start aggressively acting on behalf of their membership.
The time to end MOC as a faux physician quality measure - all of it - is now.
-Wes
Sunday, March 15, 2015
Live Video Feeds at Medical Conferences
Am I Big Brother?
The explosion of social media in our society, and at medical meetings in particular, is changing how our society, and medical professionals in particular, work and interact. There is potential for tremendous good: social media to market, to promote, to communicate rapidly, to effect change.
But the social media story is not always one of roses.
My talk at the 2015 American College of Cardiology Scientific Sessions referenced a factoid that I am not smart enough to completely verify, but I suspect isn't too far off the mark: that in January of 2014 there were 7,095,476,818 people in the world and 6,572,950,124 (93%) of them had mobile phones.
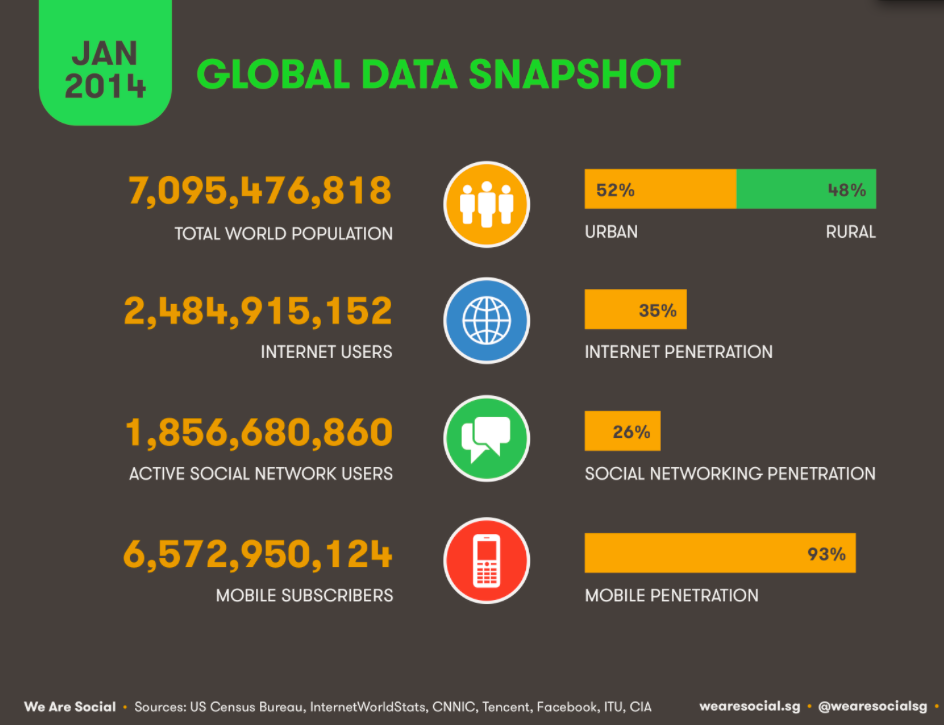{kind=link}
Think about that.
Everyone has a camera with them. Everyone at meetings (especially scientific sessions far away from the office) is shooting pictures of abstracts, friends, selfies, drug company displays … whatever - despite a policy to the contrary.
{kind=link}
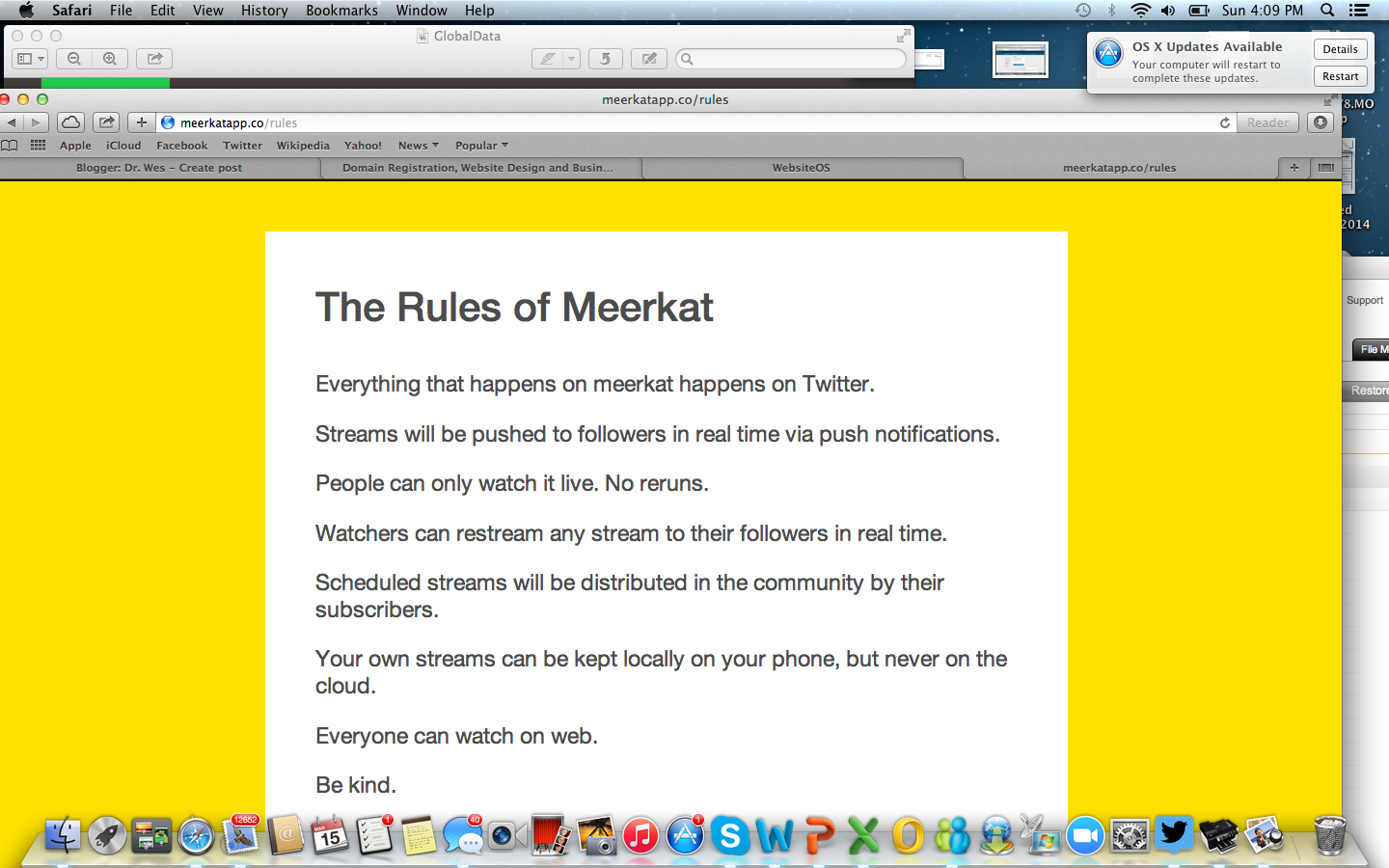
And now, there's even live streaming video on Twitter. I experimented with one of these yesterday called Meerkat. (Twitter recently announced a partnership with competing live video feed service called Periscope, so this feature is here to stay). For $1.99 I downloaded the Meerkat app to my cell phone, linked my Twitter account, and my ability to transform any experience into a live video feed transmitted instantly to the world was complete. There are some "rules" associated with Meerkat. Yet even with these rules, I found it disquieting that I held Big Brother's camera in my hand, if only for a few minutes. Those videos might not be on the "cloud" by policy, but how do I know where else they're stored, or used.
{kind=link}
There is a remarkable power, subversiveness, and wonder in the simplicity of this new technology to send live video feeds from a mobile phone. It is both novel and "cool." But I still deleted the video that I sent from the ACC meeting yesterday from my iPhone this morning after I thought about things. Perhaps I'm being overly cautious because videos can still be taken at meetings and uploaded to YouTube for the world to share. But somehow this live feed was different - so instantaneous, so uncontrollable.
And as a doctor, I don't want to become an agent for Big Brother.
-Wes
Friday, March 13, 2015
Scientific Meetings Are Becoming MOC Training Sessions
Tomorrow marks the beginning of the 2015 American College of Cardiology (ACC) Scientific Sessions in San Diego, CA. This morning I was struck by the "Schedule At-a-Glance" sent to registrants participating in these sessions:
Using Photoshop, I decided to rearrange the schedule in a linear graph format day-by-day instead:
As we can clearly see, the time devoted to Maintenance of Certification Study Sessions exceeds that of other collegial scientific and learning opportunities.
Does the American College of Cardiology really value the development of physician test-taking skills for the American Board of Medical Specialties Maintenance of Certification® program over the sharing of innovative ideas and scientific content at our largest world-wide cardiology meeting?
It would appear the largest purpose of our national meetings has changed to quelling the fear and implications of failing the ABMS MOC secure examination. I wonder what cardiovascular physicians and patients are losing as a result of this coercive and corrupt program being foisted upon us.
-Wes
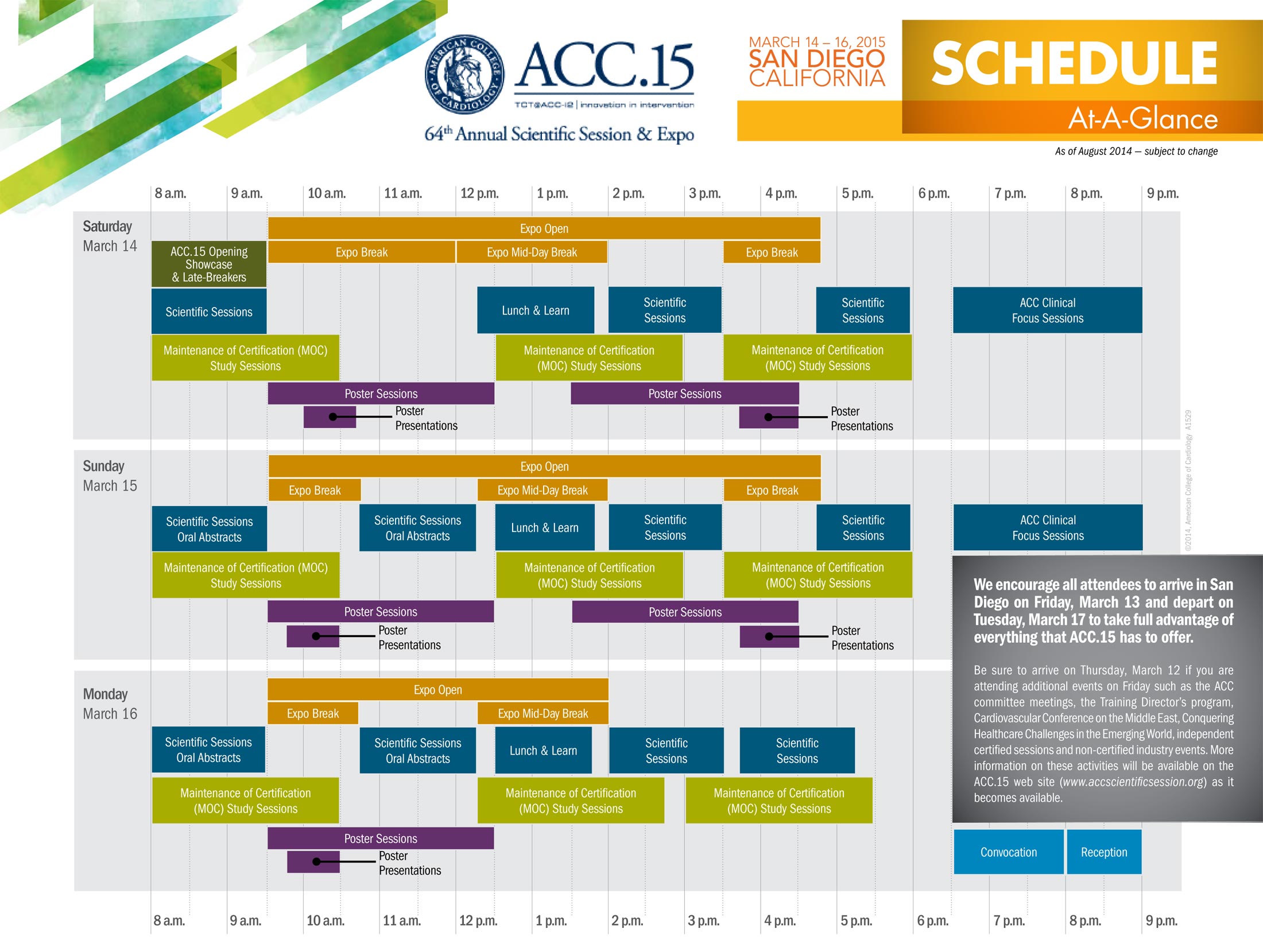 |
| ACC.15 Schedule at a Glance - Click to enlarge |
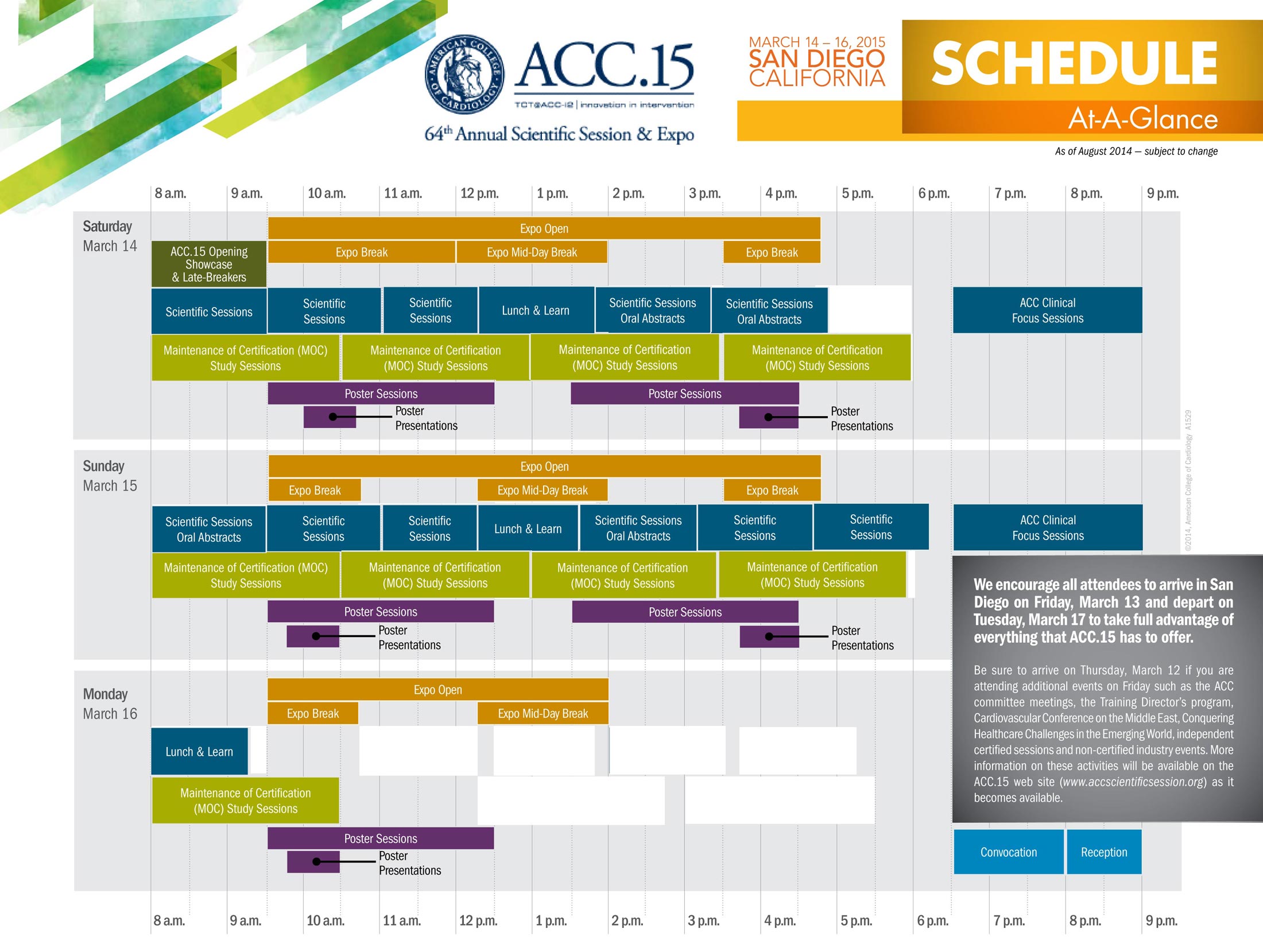 |
| ACC.15 Schedule Rearranged in Graphical Format - Click to enlarge |
As we can clearly see, the time devoted to Maintenance of Certification Study Sessions exceeds that of other collegial scientific and learning opportunities.
Does the American College of Cardiology really value the development of physician test-taking skills for the American Board of Medical Specialties Maintenance of Certification® program over the sharing of innovative ideas and scientific content at our largest world-wide cardiology meeting?
It would appear the largest purpose of our national meetings has changed to quelling the fear and implications of failing the ABMS MOC secure examination. I wonder what cardiovascular physicians and patients are losing as a result of this coercive and corrupt program being foisted upon us.
-Wes
Tuesday, March 10, 2015
Physician Civil War or Revolution?
Today, Kurt Eichenwald published a report in Newsweek on the American Board of Internal Medicine (ABIM) scandal entitled "The Ugly Civil War in American Medicine." Here's a small exerpt:
What the American Board of Medical Specialties and their member boards (like the ABIM) don't realize is that America's practicing physicians are sick and tired of funding organizations that serve as little more than job boards for non-practicing physicians looking for their next career.
-Wes
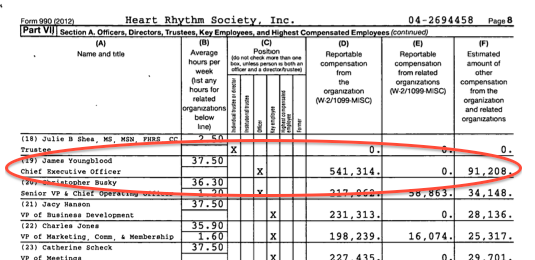
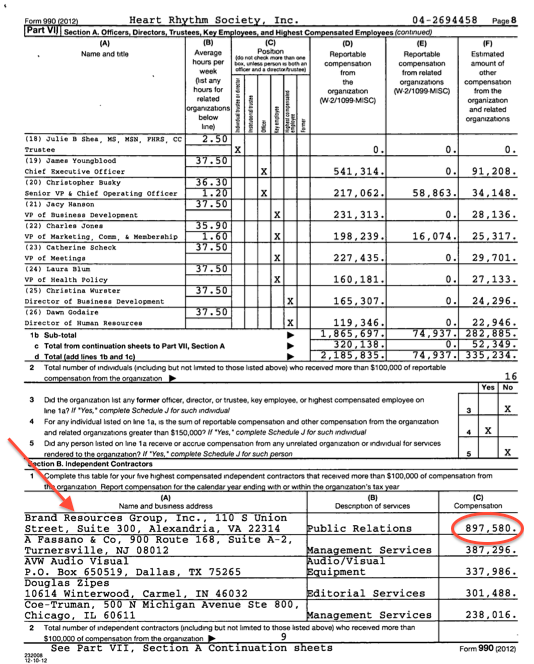
Slass says the suggestion that the ABIM is “purposefully failing candidates on their exams to generate more revenue is flat-out wrong.” Maybe so, but according to the Form 990s filed with the Internal Revenue Service, in 2001—just as the earliest round of new-test standard was kicking in, the ABIM brought in $16 million in revenue. Its total compensation for all of its top officers and directors was $1.3 million. The highest paid officer received about $230,000 a year. Two others made about $200,000, and the starting salary below that was less than $150,000. Printing was its largest contractor expense. That was followed by legal fees of $106,000.Be sure to read the whole thing.
Twelve years later? ABIM is showering cash on its top executives—including some officers earning more than $400,000 a year. In the tax period ending June 2013—the latest data available—ABIM brought in $55 million in revenue. Its highest paid officer made more than $800,000 a year from ABIM and related ventures. The total pay for ABIM’s top officers quadrupled. Its largest contractor expense went to the same law firm it was using a decade earlier, but the amounts charged were 20 times more.
And there is another organization called the ABIM Foundation that does...well, it’s not quite clear what it does. Its website reads like a lot of mumbo-jumbo. The Foundation conducts surveys on how “organizational leaders have advanced professionalism among practicing physicians.” And it is very proud of its “Choosing Wisely” program, an initiative “to help providers and patients engage in conversations to reduce overuse of tests and procedures,” with pamphlets, videos and other means.
Doesn’t sound like much, until you crack open the 990s. This organization is loaded. In the tax year ended 2013, it brought in $20 million—not from contributions, not from selling a product, not for providing a service. No, the foundation earned $20 million on the $74 million in assets it holds.
The foundation racked up $5.2 million in expenses, which—other than $245,000 it gave to the ABIM—was divided into two categories: compensation and “other.” Who is getting all this compensation? The very same people who are top earners at the ABIM. Deep in the filings, it says the foundation spends $1.9 million in “program and project expenses,” with no explanation what the programs and projects are.
There are some expenditures, though, that are easy to understand: The foundation spends $153,439 a year on at least one condominium. And it picks up the tab so the spouse of the top-officer can fly along on business trips for free.
What the American Board of Medical Specialties and their member boards (like the ABIM) don't realize is that America's practicing physicians are sick and tired of funding organizations that serve as little more than job boards for non-practicing physicians looking for their next career.
-Wes
Where Will Social Media Be in Five Years?
Where will social media be in five years? Will it be dead? Will it be thriving? What will it look like?
This was just one question posed to me as a speaker in this topic for the 2015 American College of Cardiology Scientific Sessions in San Diego this upcoming weekend. Here are some of my thoughts and I'd love to hear what others think (I need CONTENT people!) since I'm really not an expert:
Your thoughts?
-Wes
This was just one question posed to me as a speaker in this topic for the 2015 American College of Cardiology Scientific Sessions in San Diego this upcoming weekend. Here are some of my thoughts and I'd love to hear what others think (I need CONTENT people!) since I'm really not an expert:
- The word "social" in "social media" will disappear.
- The term "rectangle deficiency" (aka, misplaced cellphone) will achieve DSM-V status.
- True privacy will be the "new black" for medicine (as will actually looking at the patient).
- Text messaging will overwhelmingly replace paging for day-to-day patient care.
- Research will increasingly recruit patients via this channel.
- Credible content on social media will be recognized and even encouraged by academic institutions.
- US physician attendance at Scientific sessions will further dwindle due to costs while subsidized overseas physician attendance will grow.
- The Apple iWatch will be so, well, yesterday...
Your thoughts?
-Wes
Sunday, March 08, 2015
Medscape Issues a Non-Private Privacy Update
With physicians increasingly turning to news aggregators to keep up with medical news and developments, physicians' eyes have become Big Business.
So has sharing their information.
Medscape (a division of WebMD) recently sent all of its registered users an update of their "privacy" policy (By the way, check to see if a "cookie" considers you already "logged on" when you view this policy webpage).
Here's my summary take:
Nothing physicians do with Medscape/theHeart.org/WebMD websites is private and, in fact, our data (including license information) is being shared with just about anyone willing to pay for the data.
Medscape, ironically the same institution charged with managing continuing medical education for the Health and Human Services HIPAA policy, wants to collect physician license information from "third parties," track what doctors are viewing and interacting with on their website, then share this data to anyone willing to pay them a pretty penny. In fact, we should take special notice of the section entitled "Disclosure of Your Information to Third Parties."
I was particularly interested in the the Companies and People Who Work For Us subsection:
Privacy? What privacy?
-Wes
h/t Mr. Larry Husten
So has sharing their information.
Medscape (a division of WebMD) recently sent all of its registered users an update of their "privacy" policy (By the way, check to see if a "cookie" considers you already "logged on" when you view this policy webpage).
Here's my summary take:
Nothing physicians do with Medscape/theHeart.org/WebMD websites is private and, in fact, our data (including license information) is being shared with just about anyone willing to pay for the data.
Medscape, ironically the same institution charged with managing continuing medical education for the Health and Human Services HIPAA policy, wants to collect physician license information from "third parties," track what doctors are viewing and interacting with on their website, then share this data to anyone willing to pay them a pretty penny. In fact, we should take special notice of the section entitled "Disclosure of Your Information to Third Parties."
I was particularly interested in the the Companies and People Who Work For Us subsection:
In addition, if you are a healthcare professional, we may request that a third party validate your licensure status and other information against available databases of healthcare professionals. In order to provide these services, we may provide these other companies with Personal Information we maintain about users of our Services. We require that all such companies agree that they will limit their use of your Personal Information to fulfilling their responsibilities to us. (Emphasis mine)Such a friendly two-way give and take of our information! (Remember that practice information you were recently asked to supply to the American Board of Internal Medicine?)
Privacy? What privacy?
-Wes
h/t Mr. Larry Husten
Tuesday, March 03, 2015
Why the IRS Should Investigate the ABIM and Its Foundation
This morning, I woke to this remarkable comment to Dr. Robert Centor from Charles Koo, MD on Dr. Centor's blog, Medical Rants. I republish it here for all to read for it precisely and professionally articulates what many of us have been trying to say to the public about the corrosive nature of the ABIM scandal that has erupted over the ABMS Maintenance of Certification program:
-Wes
It's time the IRS takes notice.Dr. Centor, In an email to me regarding the ABIM and the ABIM Foundation financial behavior, Dr. Baron stated in the email that the ABIM has never had any inappropriate financial behavior. (I can send you the email from Rich Baron if you would like to read it yourself) Is that so? Myself and folks like Dr. Fisher, Dr. Cutler and legions of other hard working clinicians take great issue with a group of aloof administrator physicians spending vast amounts of money on themselves via Mercedes Limo Service, Condos, and "retreats" to the Four Seasons. Is it appropriate to pool the fees from graduating housestaff and hard working clinicians so they can reward themselves with nauseatingly gaudy creature comforts? How can an organization designed and run by non-clinicians tell the rest of us to "Choose Wisely" and to embrace cost efficiency/austerity while making themselves multi-millionaires off the sweat equity of the everyday clinician and graduating house staff? Would you trust such an organization? Dr. Fisher's point is very, very well taken. More so since the ABIM and the ABIM Foundation are both registered "non-profit" organizations. In essence, the American Taxpayer is subsidizing their operational status and their capital budget when in fact the ABIM is totally, hugely, and utterly profitable. That hypocrisy has never been fully addressed by Dr. Baron or any other ABIM representative. Can you trust an clinical regulatory organization that is utterly devoid of any contemporary clinicians? Dr. Cutler pointed out that Dr. Zeke Emanuel is "not certified" by the ABIM continues to be "not certified" and yet remains as a leader for ABIM Assessment 2020. According to the 2012 Medicare database, Dr. Krumholz has no patient E/M contacts and read a handful of echos. Yet he is another leader of ABIM Assessment 2020. Isn't the lack of inclusion of active, high volume clinicians into the structure of the ABIM and the ABIM Foundation patently wrong? And yet you trust and "hope" this clubby cadre of "ethical" non-clinical physicians will magically do the right thing when it is clear they been doing it wrong for almost a decade. The irony of this oxymoronic situation is troubling and sickening. Even more ironic and more sickening is the ABIM's driving point- that their mission is somehow a product of pure altruism and promoting honesty and integrity to its Diplomates. If that were to be true, the ABIM leaders should immediately vow to take an oath of fiscal modesty and financial mediocrity. Do you think the ABIM leaders would ever take a significant pay cut and promise never to abuse the money from an impoverished senior resident on Mercedes limo service? When you look at your residents at Morning Report, can you honestly and whole heartedly tell all these young folks that your friends at the ABIM are doing them right? Do you think the ABIM has the courage to set aside their own financial interests and to show leadership when they are apt to state their financial misbehavior were inherited? How cowardly is the ABIM to place all the blame on Christine Cassel? Would you have to courage to ask the ABIM and the ABIM Foundation to take such an oath of modesty and fiscal/financial mediocrity? Or is your sense of cronyism clouding your judgment? In the end, we have a growing schism between those who are placing their bets on a sclerotic ABIM whose leadership has failed its Diplomates and those who welcome change, competition and Darwinian evolutionary forces in Medicine. The loss of trust and faith in the ABIM cannot be ignored by their leaders and the proof in the pudding will be when the Diplomates who are sick and tired of the ABIM selling them out will defund this organization and turn to more responsible organizations willing to document their lifelong learning without pricing in a condo, a limo, a retreat to the Four Season, and massive salaries for themselves. At low tide, everyone will find out who is swimming naked.
-Wes
Sunday, March 01, 2015
New York Times Shamefully Panders to Aetna's Management Style
In this morning's New York Times, David Gelles, writes a gushing piece on how Aetna is using meditation and mindfulness to "reshape his company's future."
Much of the article idealizes the management approach of Aetna's 58 year-old CEO, Mark T. Bertolini, and tugs at the heart strings of America by focusing on his near-death experience after an unfortunate ski accident he suffered in 2004. The crux of the article focused on how Mr. Bertolini became "enamored with yoga's intellectual and cultural history," and how "Mr. Bertolini found that difficult thoughts and emotions became easier to manage" with mindfulness techniques. He later expanded these practices to the rest of his employees on a voluntary basis, using metrics of heart rate variability and cortisol level measurement ("common measures of anxiety") to assess the efficacy of his programs to his company's bottom line. Most remarkable, Mr. Gelles implies that "productivity gains" and cost savings were attributed, in part, to his practices. In fact, if it weren't for these practices, we are told, he might "not have been inspired to act on his impulse" to raise their lowest paid employees salaries from $12 an hour to $16 dollars an hour as the "latest phase of Mr. Bertolini's grand experiment."
It is remarkable that any reporter, much less one from the New York Times, would attribute Aetna's windfall to mindfulness and meditation practices without even mentioning the impact that our new health care law and its higher premiums and co-pays has had to Aetna's bottom line. It doesn't take much digging to find in Aetna's own 2014 Investor Conference data that health care premiums have increased four times faster than inflation, employee costs are rising 50% faster than employer costs, and average deductibles to patients have increased over 50% in the past five years. Nor did Mr. Gelles even deem it important to mention that Mr. Bertolini made over $30 million dollars in compensation and benefits in just one year (2013) on the backs of Aetna's own customers as well.
There his a mindfulness practice called "Mettā" where practitioners chant "May I be healthy. May I be happy. May I be well. May I be free from harm." Maybe Aetna and Mr. Gelles should practice a little "Mettā" on behalf of Aetna's customers rather than just for Aetna's bottom line.
-Wes
Much of the article idealizes the management approach of Aetna's 58 year-old CEO, Mark T. Bertolini, and tugs at the heart strings of America by focusing on his near-death experience after an unfortunate ski accident he suffered in 2004. The crux of the article focused on how Mr. Bertolini became "enamored with yoga's intellectual and cultural history," and how "Mr. Bertolini found that difficult thoughts and emotions became easier to manage" with mindfulness techniques. He later expanded these practices to the rest of his employees on a voluntary basis, using metrics of heart rate variability and cortisol level measurement ("common measures of anxiety") to assess the efficacy of his programs to his company's bottom line. Most remarkable, Mr. Gelles implies that "productivity gains" and cost savings were attributed, in part, to his practices. In fact, if it weren't for these practices, we are told, he might "not have been inspired to act on his impulse" to raise their lowest paid employees salaries from $12 an hour to $16 dollars an hour as the "latest phase of Mr. Bertolini's grand experiment."
It is remarkable that any reporter, much less one from the New York Times, would attribute Aetna's windfall to mindfulness and meditation practices without even mentioning the impact that our new health care law and its higher premiums and co-pays has had to Aetna's bottom line. It doesn't take much digging to find in Aetna's own 2014 Investor Conference data that health care premiums have increased four times faster than inflation, employee costs are rising 50% faster than employer costs, and average deductibles to patients have increased over 50% in the past five years. Nor did Mr. Gelles even deem it important to mention that Mr. Bertolini made over $30 million dollars in compensation and benefits in just one year (2013) on the backs of Aetna's own customers as well.
There his a mindfulness practice called "Mettā" where practitioners chant "May I be healthy. May I be happy. May I be well. May I be free from harm." Maybe Aetna and Mr. Gelles should practice a little "Mettā" on behalf of Aetna's customers rather than just for Aetna's bottom line.
-Wes
Subscribe to:
Posts (Atom)