The unofficial transcribed 3rd Circuit Appellate Court arguments held 23 Oct 2020 between Mr. Philip Curley (lead attorney representing the physician Plaintiffs) and Ms. Leslie John (representing the American Board of Internal Medicine (ABIM)) are now available for US physician review. The appeal was filed after the 3rd Circuit District Court dismissed the Plaintiffs complaints before discovery because, as Mr. Curley states in those arguments:
"And that's what the district court did here that was incorrect; it concluded that as a matter of law, there could only be one product, and it shouldn't have arrived at that or any other conclusion in our judgment. It arrogated to itself a determination of the ultimate fact issue which is out of the separate products. It was indifferent to our allegations. It improperly weighed evidence. It explicitly made findings. It used those words, and had accepted ABIM's affirmative defenses that are outside of the Complaint. All those are in violation of the proper standards in ruling on a 12(b)(6) motion to dismiss. And we respectfully point out to the Court that this is not a motion where only conclusory recitations of law are pleaded or claims rote elements are simply recited. This is a highly detailed and factual Complaint, and we are entitled to discovery and the right to prove our claim. So we respectfully ask that the district court be reversed."
While I made some earlier observations when only the audio file of the arguments became available, there are a number of other observations that I believe are important from those arguments.
ABIM Never Answers the Question About Forcing or Monopoly Control of Certification
On Page 27 of the transcript, Judge Chagaras asked Ms. John the following question:
"Could I just ask a follow-up there about forcing? How do we conclude that internists aren't forced to buy MOC at this stage in the litigation in light of the allegations that internists can't successfully practice without certification; and isn't the feasibility of practicing without certification ultimately a question of fact?"
Rather than answering the question, Ms. John responds:
"I think you can first look to the facts in this case. So, for instance, Doctor Manalo who never -- who did purchase initial certification and never purchased Maintenance of Certification, I think that certainly shows that his purchase of initial certification was not contingent on the later purchase of Maintenance of Certification. So I think that is one way you can look at it."Recall that in the Amended Complaint, Dr. Manalo has been unable to become employed as a result the fact that he refused to participate in MOC. The judge presses further:
"But, Counsel, what I'm talking about is it may not be so voluntary. If they want to make a living, are they forced to buy your product? You seem to say no, they're not forced to, but is that essentially an issue of fact that's more appropriate for summary judgment?"
And of course, Ms. John forgets the fact that many physicians are grandfathered and don't have to perform MOC, but states:
"I would suggest not because I think when courts look to forcing, they look at what is the situation at the time of the initial purchase, and at the time of the initial purchase here ABIM had a program for certification; and aspects of that program were initially passing your initial Board certification exam, and then that that certification would expire after a set period of time, ten years, without -- unless that diplomate passed subsequent examinations. And so when they up front bought that product, they knew there would be a continuing obligation as part of the certification program that they would have to demonstrate, in fact, that they possess the requisite knowledge to hold themselves out and say, yes, I am ABIM or Board certified. So there is no forcing because there is the knowledge up front at the time of purchase of what certification entails, and that was the periodic demonstration of knowledge."Unfazed, the judge then asks:
But I suppose that the most basic form of your argument is they don't have to go through ABIM to practice?"To which Ms. John answers as only a lawyer can:
"Yes, your Honor. So, for instance, if you look at the Amended Complaint, the Amended Complaint is quite clear that Board certification is not required to practice medicine in the United States. That is simply a function of state boards of medicine that license doctors. You only need a license in your state to practice medicine. Board certification is not required. Board certification is more like the stamp of approval that you can hold yourself out to have special qualifications. Some -- some patients and employers look to that; others do not, but it is not a requirement to practice medicine in any state in the United States, which is a fact that is pled in the Amended Complaint."Fortunately, the judge did not back down, politely recognizing the doublespeak:
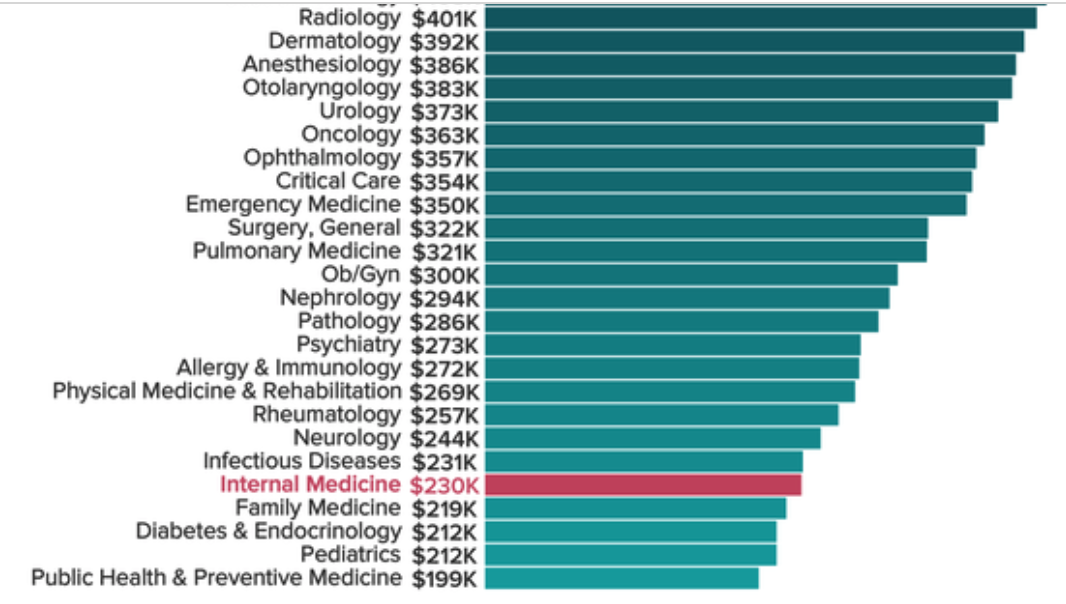
"Well, but I mean this does go to your market power. I mean, yeah, it's true you don't need the ABIM certification, but is it really feasible not to have it in reality? And I think that the allegations, don't they say you -- a lot of places won't let you practice. Your malpractice rates are going to go higher. Reimbursement is going to be an issue. So is it really feasible to practice without certification, and is that something that should be a subject of discovery as opposed to, you know, at this juncture with a motion to dismiss to resolve?We should note that as long ago as 1991, Dr. Benson (the first President of the ABIM) wrote in the Annals of Internal Medicine that certification "is no longer an option for the physician entering the marketplace." A later ABIM President agreed, Dr. Christine Cassel, writing in a climatology journal article in 2008 that "many physicians really feel that board certification is not optional." Finally, the Arthritis Care and Research article from 2019 concluded in no uncertain terms that "Board certification, which started as a voluntary achievement and remains so in theory has become involuntary in practice, making participation in MOC programs mandatory for many if not most physicians in order to maintain employment and clinical privileges, or receive reimbursement."
ABIM is Not a Professional Society
And then there was this exchange from Mr. Curley's final rebuttal statement:
So another fact question that arose from your inquiry was professional society. Is ABIM even a professional society? We don't believe it is, but in any event, there certainly is nothing in the Complaint that speaks to that. That's another example of an affirmative defense that ABIM is trying to raise, standards, professional society, internists aren't keeping up, all sorts of things that can only be resolved after discovery.Given these revelations made from the arguments before the Appellate judges. It is hard for this physician to not be encouraged by what transpired before the Appellant Count judges. I'd love to hear what others think as well.
One thing's for sure: if the Appellate Court refers this case back to the District Court for discovery, Pandora's Box will open for the ABIM and all other member board of the American Board of Medical Specialties.
-Wes