Maybe:
Showing posts with label myocardial infarction. Show all posts
Showing posts with label myocardial infarction. Show all posts
Friday, June 21, 2013
Friday, May 31, 2013
How To Simplify Consents
He arrived at the emergency room diaphoretic, hypotensive, and with substernal chest pressure. The patient was brought immediately to an emergency room care area and a stat EKG disclosed classic ST segment elevation in the inferior leads. The cath lab team was immediately summoned as the ER team worked to stabilize the patient. Within minutes, the attending cardiologist was on the scene, reviewed the EKG, examined the patient, and explained to the hoardes of family members with the patient what was taking place. In the interest of being expeditious with his consent process as the team was arriving to take the patient to the cath lab, the attending said:
"There is a 1% risk that anything bad that you can think of could happen with this procedure. If you'd like me to detail those things, I can."
The patient didn't want to hear, and off to the cath lab they went to open the patient's occluded right coronary artery to great relief of the patient and family.
Later, in follow-up, the attending cardiologist was making rounds and asked the patient his occupation.
"I'm a malpractice attorney."
Smiling, the cardiologist immediately asked, "How was my consent?"
"Perfect. Absolutely perfect."
-Wes
"There is a 1% risk that anything bad that you can think of could happen with this procedure. If you'd like me to detail those things, I can."
The patient didn't want to hear, and off to the cath lab they went to open the patient's occluded right coronary artery to great relief of the patient and family.
Later, in follow-up, the attending cardiologist was making rounds and asked the patient his occupation.
"I'm a malpractice attorney."
Smiling, the cardiologist immediately asked, "How was my consent?"
"Perfect. Absolutely perfect."
-Wes
Saturday, September 08, 2012
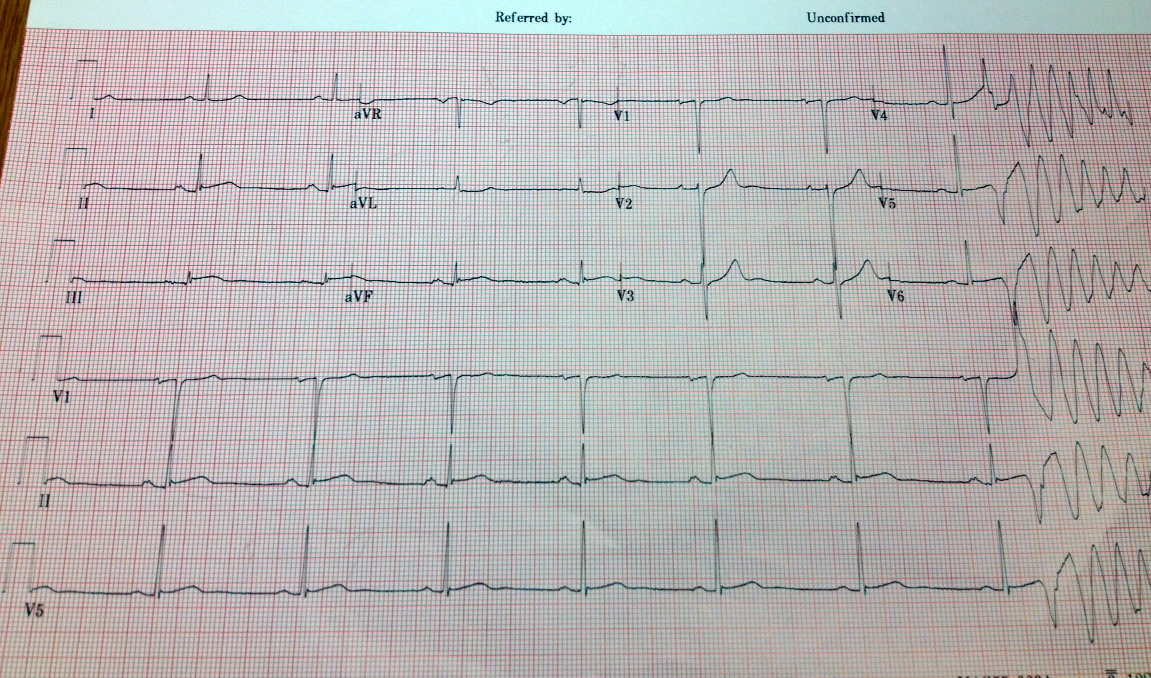
EKG Du Jour #27: Caught in the Act
I've been looking at EKG's for over 20 years and I'm not sure I've ever seen this captured on a 12-lead electrocardiogam outside the EP laboratory.
The patient was admitted with some vague chest discomfort. The initial EKG and troponins were normal, but they decided to admit the patient anyway for observation. Once on the ward after being given some heparin and aspirin, the patient was feeling perfectly fine - wanted to go home - but the second set of troponins returned positive. The first year resident decided to order a second EKG.
The EKG technician came dutifully, performed the EKG, and before she knew it, all hell broke loose:
Fortunately, the patient did well after a quite bit of work in the cath lab.
Remember this story. It might just save a life.
-Wes
The patient was admitted with some vague chest discomfort. The initial EKG and troponins were normal, but they decided to admit the patient anyway for observation. Once on the ward after being given some heparin and aspirin, the patient was feeling perfectly fine - wanted to go home - but the second set of troponins returned positive. The first year resident decided to order a second EKG.
The EKG technician came dutifully, performed the EKG, and before she knew it, all hell broke loose:
 |
| Click image to enlarge |
Fortunately, the patient did well after a quite bit of work in the cath lab.
Remember this story. It might just save a life.
-Wes
Monday, February 14, 2011
When A Cardiologist Has a Heart Attack
... the revelations for both the cardiologist and his patients are profound:
The doctor-turned-patient admits he’s faced some challenges in following the advice that he has given cardiac patients all these years.-Wes
“I try to go to the gym several times a week. It’s very difficult to fit that into my schedule,” he said. “I had adjusted my diet years ago, avoiding salt and eating less red meat. Now I’m eating oatmeal for breakfast five days a week.”
Lewin joined the cardiac rehabilitation program at the Ortenzio Heart Center at Holy Spirit, where he often ran into his own patients, who were surprised to see their doctor walking the treadmill.
“Some of them thought I was just coming to exercise,” Lewin said with a laugh. “People would tell me, ‘Gee, I have an appointment to come see you next week.’”
Lewin said his personal experience with cardiac rehab helps him relate better to his patients. “I can identify more now with what they’re going through and the concerns they face,” he said — and the challenge it can be to follow doctor’s orders.
Wednesday, November 03, 2010
How to Vote When You Have a Heart Attack on Election Day
... it can be done, but is harder than you might think:
-Wes
Someone who knew Kopplin and who lived in the same municipality had to print a form from the Internet, take it to the City of Milwaukee Election Commission and testify that he knew Kopplin. Then he had to bring the form to the hospital where Kopplin filled it out and signed it in front of two witnesses. The absentee ballot had to be returned to the commission by 5 p.m. Tuesday. His neighbor couldn't make it and Kopplin's kids don't live in Milwaukee. Kopplin eventually found a friend who is a Milwaukee resident to do the grunt work.This man is a Great American indeed.
"What I had to go through to get a ballot and get it signed and get it turned in by 5, leave it to politicians to come up with this," Kopplin said.
Kopplin received a stent in his heart and is hoping to go home from the hospital on Wednesday.
-Wes
Sunday, October 31, 2010
How Nurses Deal With a Heart Attack
... on one of their own:
-Wes
Although the EKG told a different tale, Glowacki felt well enough to call her husband and explain to him she was having a heart attack.Good idea.
"My fellow employees were just looking at me going, 'You don't look like you're having a heart attack,' " Glowacki said. "I said, 'I don't feel like it,' and they said, 'Get off the cell phone.' "
-Wes
Tuesday, July 20, 2010
Why Every Heart Patient Should Order Pizza
... because the delivery man might just save your life:
Linn's wife says he had just gone into cardiac arrest Friday when the pizza deliveryman knocked on the door of their Colorado home to bring their order. Kami Linn says she opened the door to "some burly-looking dude" and immediately asked for help.-Wes
Monday, June 28, 2010
Why Did Dick Cheney Develop Heart Failure?
Years ago, when I was indoctrinated as a fellow in to American College of Cardiology, Dick Cheney - then a former secretary of state, was the keynote speaker at our commencement ceremony. His keynote speech reflected on what it was like to watch his father die following a massive heart attack, comforted only by morphine, oxygen, bed rest. By then, Mr. Cheney, already a recipient of two bypass operations, made a point to thank the cardiovascular community for helping him.
Many years later, Mr. Cheney's complicated yet remarkable cardiovascular history reads like a social studies timeline - one with heart attacks, arrhythmias, blood clots, and now, congestive heart failure. (Of course, political spin meisters want to make sure we call it "fluid retention" rather than congestive heart failure, since "failure" is not an option when speaking of all things political).
Congestive heart failure is nothing more than an insufficient pumping of blood to meet the body's needs. As a result, the kidneys detect the decreased perfusion pressure and trigger the release of a cascade of hormones to increase the blood pressure to maintain perfusion of the tissues. Some of the hormones help retain fluid in the vascular space. If this fluid becomes too excessive, the fluid can spill into the lung resulting in a sensation of shortness of breath, usually worse when lying flat. One of the main drugs used to fool the kidneys to release the accumulated fluid are diuretics - the most common being furosemide (Lasix).
There are a number of things that may have contributed to the development of Mr. Cheney's heart failure. Since HIPAA knows no bounds with disclosing Mr. Cheney's heart history, we can use this opportunity to tease apart a few possibilities.
First, dead meat don't beat.
It doesn't help that Mr. Cheney has had many heart attacks in the past. With the progressive loss of healthy muscle cells to to the heavy lifting of contraction, the ejection fraction falls. At first, the heart compensates by recruiting other, non-injured segments of heart muscle to take up the slack, but with each successive heart attack, the reserve heart muscle dwindles. Lose enough muscle and the heart must rely on increasing the rate at which if contracts to increase output, but for hearts already with limited blood flow this might lead to futher shortage of oxygen to the heart muscleto When this happens, the heart rate kicks up just a bit to increase cardiac output. If it kicks up too much, the heart can outstrip it's own oxygen supply, resulting in additional injury to the heart. This is part of the reason medication that slow the heart rate (beta blockers) can be helpful adjuncts to preserving heart muscle function and slowing the progression of worstened heart failure.
Second, Mr. Cheney's atrial fibrillation.
The loss of coordinated pumping of the top chambers (atria) just before the lower pumping chambers (ventricles) can lead to 10-20% drop in effective cardiac output in some patients. The irregularity of the heart's rhythm while in atrial fibrillation also causes a loss of coordinated closing of the normally one-way valves that direct the flow of blood through the heart, further compromising the heart's pumping ability. Rate control of atrial fibrillation or the restoration of normal sinus rhythm in the heart are often important adjuncts to the treatment of atrial fibrillation.
Third, is the presence of Mr. Cheney's defibrillator.
Although we do not know for sure, it would not be surprising if many of Mr. Cheney's heart beats are being supplied by his defibrillator's pacemaker feature. Excessive pacing the right ventricle can cause a dis coordinated beating of the lower pumping chambers, resulting in a subtle, but real, fall in cardiac function during paced heart beats compared to beats that are not paced and normally conducted from the top to bottom heart chambers. At some point in the future, Mr. Cheney might benefit, in appropriate circumstances, by adding extra pacing wire to his existing defibrillator system (so-called biventricular pacing) to re-coordinate the contraction process of his heart chambers above and beyond that which can be achieved with medications alone.
Finally, might he have new portions of heart muscle lacking sufficient oxygen?
Not all coronary arteries that might be partially blocked can be revascularized during surgeries or angioplasties. As a result, some segments of heart muscle might not have enough blood flow to maintain proper function, yet have just enough to survive intact. Many of our medications help lower blood pressure to decrease the work the heart has to perform on a beat-to-beat basis, dilate blood vessels to improve coronary blood flow, and work to decrease the negative affects that excessive adrenaline-like compounds can have on the heart's remaining muscle cells. The very fact that his doctors did not feel further invasive procedures were necessary suggests Mr. Cheney's revacularization options are limited at this point.
So given his current setback, what should we expect regarding his prognosis?
Hard to know. But given what I know about the successful management of heart failure these days, I wouldn't count him out quite yet.
-Wes
Many years later, Mr. Cheney's complicated yet remarkable cardiovascular history reads like a social studies timeline - one with heart attacks, arrhythmias, blood clots, and now, congestive heart failure. (Of course, political spin meisters want to make sure we call it "fluid retention" rather than congestive heart failure, since "failure" is not an option when speaking of all things political).
Congestive heart failure is nothing more than an insufficient pumping of blood to meet the body's needs. As a result, the kidneys detect the decreased perfusion pressure and trigger the release of a cascade of hormones to increase the blood pressure to maintain perfusion of the tissues. Some of the hormones help retain fluid in the vascular space. If this fluid becomes too excessive, the fluid can spill into the lung resulting in a sensation of shortness of breath, usually worse when lying flat. One of the main drugs used to fool the kidneys to release the accumulated fluid are diuretics - the most common being furosemide (Lasix).
There are a number of things that may have contributed to the development of Mr. Cheney's heart failure. Since HIPAA knows no bounds with disclosing Mr. Cheney's heart history, we can use this opportunity to tease apart a few possibilities.
First, dead meat don't beat.
It doesn't help that Mr. Cheney has had many heart attacks in the past. With the progressive loss of healthy muscle cells to to the heavy lifting of contraction, the ejection fraction falls. At first, the heart compensates by recruiting other, non-injured segments of heart muscle to take up the slack, but with each successive heart attack, the reserve heart muscle dwindles. Lose enough muscle and the heart must rely on increasing the rate at which if contracts to increase output, but for hearts already with limited blood flow this might lead to futher shortage of oxygen to the heart muscleto When this happens, the heart rate kicks up just a bit to increase cardiac output. If it kicks up too much, the heart can outstrip it's own oxygen supply, resulting in additional injury to the heart. This is part of the reason medication that slow the heart rate (beta blockers) can be helpful adjuncts to preserving heart muscle function and slowing the progression of worstened heart failure.
Second, Mr. Cheney's atrial fibrillation.
The loss of coordinated pumping of the top chambers (atria) just before the lower pumping chambers (ventricles) can lead to 10-20% drop in effective cardiac output in some patients. The irregularity of the heart's rhythm while in atrial fibrillation also causes a loss of coordinated closing of the normally one-way valves that direct the flow of blood through the heart, further compromising the heart's pumping ability. Rate control of atrial fibrillation or the restoration of normal sinus rhythm in the heart are often important adjuncts to the treatment of atrial fibrillation.
Third, is the presence of Mr. Cheney's defibrillator.
Although we do not know for sure, it would not be surprising if many of Mr. Cheney's heart beats are being supplied by his defibrillator's pacemaker feature. Excessive pacing the right ventricle can cause a dis coordinated beating of the lower pumping chambers, resulting in a subtle, but real, fall in cardiac function during paced heart beats compared to beats that are not paced and normally conducted from the top to bottom heart chambers. At some point in the future, Mr. Cheney might benefit, in appropriate circumstances, by adding extra pacing wire to his existing defibrillator system (so-called biventricular pacing) to re-coordinate the contraction process of his heart chambers above and beyond that which can be achieved with medications alone.
Finally, might he have new portions of heart muscle lacking sufficient oxygen?
Not all coronary arteries that might be partially blocked can be revascularized during surgeries or angioplasties. As a result, some segments of heart muscle might not have enough blood flow to maintain proper function, yet have just enough to survive intact. Many of our medications help lower blood pressure to decrease the work the heart has to perform on a beat-to-beat basis, dilate blood vessels to improve coronary blood flow, and work to decrease the negative affects that excessive adrenaline-like compounds can have on the heart's remaining muscle cells. The very fact that his doctors did not feel further invasive procedures were necessary suggests Mr. Cheney's revacularization options are limited at this point.
So given his current setback, what should we expect regarding his prognosis?
Hard to know. But given what I know about the successful management of heart failure these days, I wouldn't count him out quite yet.
-Wes
Wednesday, June 16, 2010
Saturday, April 24, 2010
The Costs of a Heart Attack
Quite a bit, according to some:
-Wes
Reference: The WISE Study:
Shaw LJ, Merz CNB, Pepine CJ, et al. The Economic Burden of Angina in Women With Suspected Ischemic Heart Disease: Results From the National Institutes of Health-National Heart, Lung, and Blood Institute-Sponsored Women's Ischemia Syndrome Evaluation. Circulation. August 29, 2006 2006;114(9):894-904.
According to an article from the National Business Group on Health, the average total (editor's note: lifetime) cost of a severe heart attack–including direct and indirect costs–is about $1 million. Direct (lifetime) costs include charges for hospitals, doctors and prescription drugs, while the indirect costs include lost productivity and time away from work. The average (lifetime) cost of a less severe heart attack is about $760,000. Amortized over 20 years, that’s $50,000 per year for a severe heart attack and $38,000 per year for a less severe heart attack.I'm all for maintaining a healthy lifestyle, but before we get all hot and bothered about performing more testing to "prevent" a heart attack as a means to save health care costs going forward, remember the lessons we learned from the Tim Russert fallout.
-Wes
Reference: The WISE Study:
Shaw LJ, Merz CNB, Pepine CJ, et al. The Economic Burden of Angina in Women With Suspected Ischemic Heart Disease: Results From the National Institutes of Health-National Heart, Lung, and Blood Institute-Sponsored Women's Ischemia Syndrome Evaluation. Circulation. August 29, 2006 2006;114(9):894-904.
Could a Heart Attack During A Trial Help a Defendent in Court?
Perhaps:
Assistant U.S. Attorney Christopher Graveline wrote in a motion that after the judge told the jury about the heart attack “many jurors in their body language and facial expressions, rightly expressed concern for Mr. Cicchetti.” The prosecutor said the government did not object to the judge telling the jury about the heart attack because it assumed that Cicchetti would be prosecuted later before a different jury.-Wes
“It is only natural for the jury to feel sympathy for Mr. Cicchetti’s condition and this sympathy may well play into its consideration of the evidence against Mr. Cicchetti especially in light of his defense that he is a sick harmless older man who is only guilty of loving motorcycles and cocaine.”
“The government believes that allowing Mr. Cicchetti to continue in absentia would prejudice its ability to have a fair hearing and that there would be a high probability that an extrinsic factor, i.e. the defendant’s health, could affect the jury’s decision rather than the evidence presented in court.”
Friday, February 26, 2010
Don't Abandon Manual Blood Pressure Cuffs
... they might help preserve myocardium:
-Wes
Reference:
Bøtker HE at al. "Remote ischaemic conditioning before hospital admission, as a complement to angioplasty, and effect on myocardial salvage in patients with acute myocardial infarction: a randomised trial" Lancet 27 February 2010 375: 727-734.
333 consecutive adult patients with a suspected first acute myocardial infarction were randomly assigned in a 1:1 ratio by computerised block randomisation to receive primary percutaneous coronary intervention with (n=166 patients) versus without (n=167) remote conditioning (intermittent arm ischaemia through four cycles of 5-min inflation and 5-min deflation of a blood-pressure cuff). Allocation was concealed with opaque sealed envelopes. Patients received remote conditioning during transport to hospital, and primary percutaneous coronary intervention in hospital. The primary endpoint was myocardial salvage index at 30 days after primary percutaneous coronary intervention, measured by myocardial perfusion imaging as the proportion of the area at risk salvaged by treatment; analysis was per protocol.Hey, lose blood flow to an arm to save a heart. Works for me.
...
Median salvage index was 0·75 (IQR 0·50—0·93, n=73) in the remote conditioning group versus 0·55 (0·35—0·88, n=69) in the control group, with median difference of 0·10 (95% CI 0·01—0·22; p=0·0333); mean salvage index was 0·69 (SD 0·27) versus 0·57 (0·26), with mean difference of 0·12 (95% CI 0·01—0·21; p=0·0333).
Interpretation
Remote ischaemic conditioning before hospital admission increases myocardial salvage, and has a favourable safety profile. Our findings merit a larger trial to establish the effect of remote conditioning on clinical outcomes.
-Wes
Reference:
Bøtker HE at al. "Remote ischaemic conditioning before hospital admission, as a complement to angioplasty, and effect on myocardial salvage in patients with acute myocardial infarction: a randomised trial" Lancet 27 February 2010 375: 727-734.
Wednesday, March 11, 2009
Strange Twist to the Work-up of Heart Attack
Bizarre. I guess when we're working up chest pain in the young patient, we should inquire about bullet holes in the side of the house.
-Wes
-Wes
Sunday, August 24, 2008
What Your Heart Attack Might Be Like
The Brits showed this ad from the patient's perspective:
Although one would hope the symptoms wouldn't get to this extreme, the ad makes the point that heart attacks aren't really just about chest pain: but also chest or arm tightness or a discomfort, dizziness, shortness of breath, nausea, vomiting, sweating, and the like.
But back pain, especially between the scapula, was not mentioned, nor was incessant burping typical with some inferior myocardial infarctions (lower wall heart attacks).
Not only are people unfamiliar with the more common symptoms of heart attacks, but there's a tremendous amount of denial when they happen to one of us. Worse yet, many people I have seen were ashamed to call the ambulance because they didn't like the idea of flashing lights and sirens in front of their residence.
And one more thing to consider: if a friend wants to call an ambulance for you, let them. Remember they are objective observers, and might just save your life even despite yourself.
-Wes
Although one would hope the symptoms wouldn't get to this extreme, the ad makes the point that heart attacks aren't really just about chest pain: but also chest or arm tightness or a discomfort, dizziness, shortness of breath, nausea, vomiting, sweating, and the like.
But back pain, especially between the scapula, was not mentioned, nor was incessant burping typical with some inferior myocardial infarctions (lower wall heart attacks).
Not only are people unfamiliar with the more common symptoms of heart attacks, but there's a tremendous amount of denial when they happen to one of us. Worse yet, many people I have seen were ashamed to call the ambulance because they didn't like the idea of flashing lights and sirens in front of their residence.
And one more thing to consider: if a friend wants to call an ambulance for you, let them. Remember they are objective observers, and might just save your life even despite yourself.
-Wes
Tuesday, June 17, 2008
The Tim Russert Fallout
It’s hard for me not to sit amazed at the job medicine has done convincing people we can control heart attacks. One only needs to review the many news stories regarding news journalist Tim Russert's untimely death to see the public fallout of our efforts to "educate" the populace about "screening tests" used to "prevent" the likelihood of having a heart attack. You see, with Mr. Russert's death, those tests have suffered a huge public relations nightmare.
Cholesterol screening and statins: dead in the water.
CT scanning for detection of plague to prevent heart attack: harpooned.
Stress testing to assure you're protected against the Big One: pulverized.
Not one damn thing predicted (or prevented) Mr. Russert's death.
Oh sure, there's plenty of others who want to jump right in to promote the next great lifestyle modification, rather than those damn cholesterol drugs as a way to save your life, provided of course, you buy their book. Or those who promise reduced mortality if everyone just got an ultrasound of their carotid arteries, even though this test still can't predict acute plaque rupture and the onset of a heart attack like Mr. Russert's.
You see, the entire industrial complex of healthcare technology and innovation was shaken, not because Mr. Russert was a nice guy and great journalist, but rather because they will have to explain why their technology isn't worth a damn at predicting heart attacks.
Welcome, my friends, to the world of real-life medicine rather than marketing.
-Wes
Cholesterol screening and statins: dead in the water.
CT scanning for detection of plague to prevent heart attack: harpooned.
Stress testing to assure you're protected against the Big One: pulverized.
Not one damn thing predicted (or prevented) Mr. Russert's death.
Oh sure, there's plenty of others who want to jump right in to promote the next great lifestyle modification, rather than those damn cholesterol drugs as a way to save your life, provided of course, you buy their book. Or those who promise reduced mortality if everyone just got an ultrasound of their carotid arteries, even though this test still can't predict acute plaque rupture and the onset of a heart attack like Mr. Russert's.
You see, the entire industrial complex of healthcare technology and innovation was shaken, not because Mr. Russert was a nice guy and great journalist, but rather because they will have to explain why their technology isn't worth a damn at predicting heart attacks.
Welcome, my friends, to the world of real-life medicine rather than marketing.
-Wes
Thursday, January 31, 2008
Go Red?
Also, zillions of nice "events" are planned for this day - each with tons of sponsors' paraphernalia - all sprinkled about the audience to raise awareness of heart disease, tune-ups, floor tile, and cutlery while corporations add to their marketing budgets. The conflicts that this bling brings to the event reminds me of the conflicts inherent to "free lunches" provided at Grand Rounds sponsored by drug companies.
Take for instance, Merck. They're one of the "Proud National Sponsors" of the Go Red for Women campaign.
But they're also interested in the controvertial promotion of Gardasil for women to prevent cervical cancer. Merck also sells Vioxx, Vytorin, and Zetia - several drugs without such great press lately in their quest to prevent heart disease.
Other corporate sponsors' motivations are less clear - like Jiffy Lube, Diet Coke, Campbell's Soup, Cutco, Brighton, Clairol Professional, Hamilton Beach, Flooring America, Starkist, Del Monte, Swanson's and RiteAid pharmacies. I mean, its so touchy feely and the women's purchasing power so important that corporations have jumped on this feel-good campaign like a tick on a bloodhound. Where exactly are their heart health motivations? In assuring sodium loading, cutlery, or toxic chemical exposures to women?
Or is this campaign really about funding research for the prevention of women's heart disease?
If so, can anyone point me to studies funded by this endeavor? Or does it just go to the general operating budget of the American Heart Association or NIMH for their big comfy corporate furniture, officer salaries, or office appointments? It's just not clear where all the money goes.
Maybe it goes for all those nice red dress pins or the Heart Checkup website? Seems like a heck of a lot of dough for that.
Yes, I'm jaded. I admit it. But I remember grocery store Green Stamps - that cute marketing invention of grocery store chains of the 1950's and 1960's that proported to help people save money if they just saved more stamps, yet actually made money for the sponsors because people never redeemed them. So I am skeptical of corporate marketing bonanzas like the Go Red Campaign that have yet to demonstrate tangible benefits to reducing women's heart disease while exacting considerable costs to our society.
So if you see me in red tomorrow, remember that I hope my red sweater raises awareness of the need for women to have a better appreciation of their heart health. I just hope it doesn't also advocate for the red budgets of families unable to afford healthcare and medications in America.
-Wes
Friday, October 26, 2007
A New Adventure
Today I'll be starting to contribute to MedPageToday's new physicians' blog from time to time. The blog kicks off today. There's a number of us physician bloggers contributing to this endeavor, so stop by and check it out.
Today's topic: my perspectives on the new heart attack definition.
-Wes
Today's topic: my perspectives on the new heart attack definition.
-Wes
Monday, October 22, 2007
Silent MI's Fair Game for Vioxx Suits?
If you never felt your MI but took Vioxx, could you sue Merck anyway and get free medical monitoring anyway? Well, maybe:
-Wes
Traditionally, New Jersey law has covered medical monitoring for people exposed to toxic chemicals. But lawyers point out that monitoring also has been allowed in some pharmaceutical cases, such as one several years ago involving the diet drug combo Fen-Phen.Pharmalot has the story.
“It makes logical sense that you should have the ability for medical monitoring,” says E. Drew Britcher, a past president of the American Trial Lawyers Association-New Jersey, which filed a “friend of the court” brief. “The question is whether or not you get a heart condition from a medication as opposed to getting cancer from a chemical. It’s still the same concept. … This should be a remedy available.”
-Wes
Monday, August 20, 2007
Guidelines: Not for Doctors Anymore
My printer nearly burned up printing the nearly 160-page guidelines of the American College of Cardiology for management of unstable angina and non-Q wave myocardial infarctions (heart attacks).
While these "guidelines" are helpful and contain the latest in evidence-based research to justify the recommendations, they now exceed the length of chapters of our classic textbooks of medicine for their specific problem. It was interesting to note that these guidelines dwarf the classic chapter in Braunwald's Heart Disease (7th ed.) with its chapter on the same information that spans just 30 pages.
These guidelines are now being written more for regulators, I'm afraid, than doctors.
-Wes
References: Cannon CP and Braunwald E. "Chapter 49, Unstable Angina and Non-ST Elevation Myocardial Infarction" in Zipes DP, Libby P, Bonow RO, Bruanwald E (eds.), Braunwald's Heart Disease - A Textbook of Cardiovascular Medicine, 7th ed., pp 1243-1273.
While these "guidelines" are helpful and contain the latest in evidence-based research to justify the recommendations, they now exceed the length of chapters of our classic textbooks of medicine for their specific problem. It was interesting to note that these guidelines dwarf the classic chapter in Braunwald's Heart Disease (7th ed.) with its chapter on the same information that spans just 30 pages.
These guidelines are now being written more for regulators, I'm afraid, than doctors.
-Wes
References: Cannon CP and Braunwald E. "Chapter 49, Unstable Angina and Non-ST Elevation Myocardial Infarction" in Zipes DP, Libby P, Bonow RO, Bruanwald E (eds.), Braunwald's Heart Disease - A Textbook of Cardiovascular Medicine, 7th ed., pp 1243-1273.
Friday, August 03, 2007
Feeding the Beast
I want to be the first to go on record and say that a 90-minute door-to-balloon time for the treatment of an Acute Coronary Syndrome is not good enough.
After all, there are two important studies that appeared in Circulation this week (here and here) that have demonstrated that maybe half of the patients can achieve the 90-minute goal if we just devote enough resources! The Wall Street Journal even noted how cleaning staff can be diverted to help transport patients in smaller, outlying health care facilities:
Here’s how it will work:
When Charlie gets chest pain at 3AM, we’re gonna set up a system whereby he’ll just lift his cell phone, punch and hold “5” on the keypad (it’s the central number, and dialing just one number will save 30 seconds!), and activate the Emergency Chest Pain System (ECPS).
 The ECPS will be a well-coordinated team of specialized health care professionals devoted to saving lives 24/7/365. State-of-the-art telecommunications will permit live, continuous monitoring of transport operations from Emergency Rooms of each of the designated Centralized Chest Pain Centers (CCPC). Even Charlie’s cell phone will transmit his continuous EKG on a Specialized Medical Frequency (SMF) to the CCPC in real-time. The ECPS will have a Centralized Coordination Center (CCC) that will help determine which resources we should bring to bear to save Charlie’s life. The CCC will have at its disposal decision-support software that will have live feeds from GPS, weather, and ground transportation monitoring systems specially-developed to streamline patient flow from the street to the Emergency Room.
The ECPS will be a well-coordinated team of specialized health care professionals devoted to saving lives 24/7/365. State-of-the-art telecommunications will permit live, continuous monitoring of transport operations from Emergency Rooms of each of the designated Centralized Chest Pain Centers (CCPC). Even Charlie’s cell phone will transmit his continuous EKG on a Specialized Medical Frequency (SMF) to the CCPC in real-time. The ECPS will have a Centralized Coordination Center (CCC) that will help determine which resources we should bring to bear to save Charlie’s life. The CCC will have at its disposal decision-support software that will have live feeds from GPS, weather, and ground transportation monitoring systems specially-developed to streamline patient flow from the street to the Emergency Room.
 Should there be a tie-up of traffic on I-94, then the CCC will determine the location where Charlie’s cell phone originates from and re-route the response team from the ground to the air. A specially designed Sikorsky jet helicopter that we have designated for this purpose equipped with the latest medical technology and defibrillators. Never mind that you can't hear a blood pressure on the helo. It's time that matters! The Sikorsky will also permit twice the range as conventional medical helicopters because it is equipped with jet engine technology. Charlie can just walk out his door and the Sikorsky will come to him! (Time saved – 45 minutes!). Oh, and don’t worry if there might be inclement weather, our team of crack professionals will have specially-designed helo’s equipped with the latest infrared and night vision systems to tackle any weather!
Should there be a tie-up of traffic on I-94, then the CCC will determine the location where Charlie’s cell phone originates from and re-route the response team from the ground to the air. A specially designed Sikorsky jet helicopter that we have designated for this purpose equipped with the latest medical technology and defibrillators. Never mind that you can't hear a blood pressure on the helo. It's time that matters! The Sikorsky will also permit twice the range as conventional medical helicopters because it is equipped with jet engine technology. Charlie can just walk out his door and the Sikorsky will come to him! (Time saved – 45 minutes!). Oh, and don’t worry if there might be inclement weather, our team of crack professionals will have specially-designed helo’s equipped with the latest infrared and night vision systems to tackle any weather!
Next, we’ll need to clear the airspace. Once the ECPS is activated, the government air-traffic control system will be notified by the CCC to clear the airspace to provide the most direct flight path between Charlie and the CCPC. Time saved (10 minutes).
Once Charlie arrives at the CCPC, specially-designed transport tubes will ascend from the CCPC to meet the Sikrorsky hovering overhead, and apply high, continuous suction to expedite Charlie’s transport into the Angiography Suite at the CCPC. Money will be saved here because people will no longer be needed to transport Charlie from the aircraft to the catheterization laboratory. (Time saved - 10 minutes)
There, our well-trained and ever-attentivegnomes doctors who will now be living at the facility around the clock (time saved - 30 minutes) to support the expedited care, will perform the necessary catheterization procedure to open Charlie’s artery.
What did you say? His EKG only showed T wave inversion? Well, we’ll cath him anyway, just to be sure!
After all, the Beast is hungry.
-Wes
After all, there are two important studies that appeared in Circulation this week (here and here) that have demonstrated that maybe half of the patients can achieve the 90-minute goal if we just devote enough resources! The Wall Street Journal even noted how cleaning staff can be diverted to help transport patients in smaller, outlying health care facilities:
When a Level 1 heart case is declared, everyone has a specific job to do. One rural hospital assigns its cleaning lady to help push the stretcher to the helicopter. "Level 1 is all you have to say," says David Larson, an emergency-room doctor at Ridgeview Medical Center who helped develop the protocol. "You're all on the same page right off the bat."I still think we can do better. I think we should have, say, 30-minute door-to-balloon times! We could save many, many more lives if we just focus, people!
Here’s how it will work:
When Charlie gets chest pain at 3AM, we’re gonna set up a system whereby he’ll just lift his cell phone, punch and hold “5” on the keypad (it’s the central number, and dialing just one number will save 30 seconds!), and activate the Emergency Chest Pain System (ECPS).
 The ECPS will be a well-coordinated team of specialized health care professionals devoted to saving lives 24/7/365. State-of-the-art telecommunications will permit live, continuous monitoring of transport operations from Emergency Rooms of each of the designated Centralized Chest Pain Centers (CCPC). Even Charlie’s cell phone will transmit his continuous EKG on a Specialized Medical Frequency (SMF) to the CCPC in real-time. The ECPS will have a Centralized Coordination Center (CCC) that will help determine which resources we should bring to bear to save Charlie’s life. The CCC will have at its disposal decision-support software that will have live feeds from GPS, weather, and ground transportation monitoring systems specially-developed to streamline patient flow from the street to the Emergency Room.
The ECPS will be a well-coordinated team of specialized health care professionals devoted to saving lives 24/7/365. State-of-the-art telecommunications will permit live, continuous monitoring of transport operations from Emergency Rooms of each of the designated Centralized Chest Pain Centers (CCPC). Even Charlie’s cell phone will transmit his continuous EKG on a Specialized Medical Frequency (SMF) to the CCPC in real-time. The ECPS will have a Centralized Coordination Center (CCC) that will help determine which resources we should bring to bear to save Charlie’s life. The CCC will have at its disposal decision-support software that will have live feeds from GPS, weather, and ground transportation monitoring systems specially-developed to streamline patient flow from the street to the Emergency Room. Should there be a tie-up of traffic on I-94, then the CCC will determine the location where Charlie’s cell phone originates from and re-route the response team from the ground to the air. A specially designed Sikorsky jet helicopter that we have designated for this purpose equipped with the latest medical technology and defibrillators. Never mind that you can't hear a blood pressure on the helo. It's time that matters! The Sikorsky will also permit twice the range as conventional medical helicopters because it is equipped with jet engine technology. Charlie can just walk out his door and the Sikorsky will come to him! (Time saved – 45 minutes!). Oh, and don’t worry if there might be inclement weather, our team of crack professionals will have specially-designed helo’s equipped with the latest infrared and night vision systems to tackle any weather!
Should there be a tie-up of traffic on I-94, then the CCC will determine the location where Charlie’s cell phone originates from and re-route the response team from the ground to the air. A specially designed Sikorsky jet helicopter that we have designated for this purpose equipped with the latest medical technology and defibrillators. Never mind that you can't hear a blood pressure on the helo. It's time that matters! The Sikorsky will also permit twice the range as conventional medical helicopters because it is equipped with jet engine technology. Charlie can just walk out his door and the Sikorsky will come to him! (Time saved – 45 minutes!). Oh, and don’t worry if there might be inclement weather, our team of crack professionals will have specially-designed helo’s equipped with the latest infrared and night vision systems to tackle any weather!Next, we’ll need to clear the airspace. Once the ECPS is activated, the government air-traffic control system will be notified by the CCC to clear the airspace to provide the most direct flight path between Charlie and the CCPC. Time saved (10 minutes).
Once Charlie arrives at the CCPC, specially-designed transport tubes will ascend from the CCPC to meet the Sikrorsky hovering overhead, and apply high, continuous suction to expedite Charlie’s transport into the Angiography Suite at the CCPC. Money will be saved here because people will no longer be needed to transport Charlie from the aircraft to the catheterization laboratory. (Time saved - 10 minutes)
There, our well-trained and ever-attentive
What did you say? His EKG only showed T wave inversion? Well, we’ll cath him anyway, just to be sure!
After all, the Beast is hungry.
-Wes
Subscribe to:
Comments (Atom)