He had called the other day to update me up on his condition. He did not sound upset, but resolute. "They offered me peritoneal dialysis," he said, "but I decided against it and figured I'd just let nature take its course. The hospice people are so wonderful - I've got things all set here at home, but I have two questions. What should I do about my warfarin? You know, I just don't want to have a stroke. And what I do about my defibrillator?"
We were colleagues once and grew to be friends later when life's circumstances brought us together. He, a revered senior neurologist and me, a relatively new doctor in town. I could remember overhearing his heated discussions about administrative snafus with colleagues in the hall, or watching a horde of residents and medical students following him into a patient's room to teach at the bedside.
"Of course he didn't want a stroke," I thought.
So we decided to keep the coumadin and let him continue his daily INR checks at home and to turn off just the tachyarrhythmia detections on his biventricular defibrillator.
"I'll come over tomorrow and we'll turn it off," I said.
There was a brief silence, perhaps because of momentary disbelief that I'd do such a thing. Then he proceeded to give me detailed directions and landmarks to watch for on my way over. "I'm sure I can find it," I said thanking him.
So the next afternoon after most of the day's events had finished, I grabbed the programmer and drove to his home. It was an unusually beautiful day - mid 70's, sunny - as if Someone had wanted it that way. There in the yard, was his wife, wearing a large-brimmed hat and holding a hose while pretending to water the shrubs. She came over to greet me: "Thanks so much for coming over," she said, "I know this means so much to him." Then she realized she was still holding the hose. "Oh, I'm so sorry, it's just that someone has to try to keep the place up," she said, voice cracking.
The "place," of course, was beautiful. A majestic grande dame of a house - one I would later learn they had occupied for the past 44 years and bought when they were "just kids on the block." It was meticulousy kept, stately. I entered with his wife and noticed a shadowy figure two rooms away sitting at the edge of a mechanized hospital bed. The bed was placed in what must have been his study with a large bay window with a couch next to it. A reading lamp was over the head of the bed and the walls held books from the floor to ceiling with icons and statues, likely from other, more active time.
"Thanks for coming, Wes," he said, looking up.
"How are you feeling?" I asked, somewhat stupidly.
"Pretty good, considering everything. See? My legs aren't quite so swollen and my abrasions all have eschars on them," he noted as only a doctor could.
"Is there a plug nearby?" and he proceeded to point me the way so I could plug in the programmer to do my job while he explained the device to his wife. The process was quick and I interrogated his defibrillator, then turned off the tachyarrhythmia detections, therapies and now needless alarms. "There, that didn't take long. All done," I said.
There was a moment of silence as I sat with this man whom I known for so long. Like a wise sage and hospitable host, it was clear he wanted to talk for a bit, so I slowed my exit.
"You know, I've always appreciated your frankness about my condition," he said. "You're a lot like me in many ways, I think. You never overstepped, let me have control, to manage things like I wanted to, and I've always appreciated that," he said.
Embarassed by his frankness, I wondered what to say. At a loss for words, I told him how much I enjoyed meeting his family, wife, daughters, and grand-daughters recently in the hospital. He looked puzzled, forgetting. "You know, that day I brought my daughter in your room with them?" His eyes brightened and his smile widened as he remembered.
"Oh, yes! That was wonderful! How fast times flies, doesn't it?" he said.
"You know, I wrote about that day in my blog," I mentioned, ".. and included some pictures of my daughter from 10 years ago - about what she thought about medicine - can I show you?"
"Of course!"
So I showed him the picture and we shared our thoughts about family. Then, to make reading from my iPhone easier, I read him the post I'd written about that day. We talked about family and what they meant to each of us. And then he shared with me another nugget, that he grew to become a writer, too.
"You know, I spent some time and wrote an autobiography for my kids not too long ago - over a hundred pages - about everything I could remember - from my earliest years as a child, about my immigrant father and American mother. My father made it as a successful lawyer - came over from eastern Europe - I even know the ship - I remember the picture of him standing there with his hat..., and I wrote about my family, influential teachers in grade school, fellow professors, and people that I knew throughout the years - everything. You should do that, too, you know. I'm so glad I did. I gave them to my kids and even made some some extra copies - maybe for the grandkids, in case they want it someday..." He looked away to see his wife leave the room, trying not to be noticed as tears filled her eyes once more. She didn't want to him to see her this way.
He stared down at the floor beneath his swollen feet, then continued.
"You know, it was therapeutic for me to write that autobiography. After all, what we do is terribly isolating for the most part. No one understands that. Like you do your procedural stuff and I do my diagnosing. We do most of it all alone, with no one else there. Just the patient and the doctor. Wonderful, to be sure, but isolating. So many memories. I guess it helped me to put some of those feelings and the thoughts I had about those I loved into words. It's hard to capture it all..."
He looked up from the floor and stared in my eyes. "Thank you," he said extending his hand.
I sat motionless for a bit digesting the gravity of his words, lost in them before I saw his hand. Once I noticed, I lept up to shake it and gave him a long hug to his increasingly skeletal frame. It was a brief moment to share together once more and one I now realized I had done too infrequently with other patients in a similar circumstance. Here he was, an incredible man who'd given so much to his family, fellow colleagues and patients, now teaching me once more so much about life as a doctor, about grace, and about real love. Just the two of us, isolated again, but as friends.
With great reluctance I packed things up and found his wife on my way out. "Thank you," she whispered with swollen eyes, "I just don't want him to be in pain."
"He's going to be fine," I told her, "... perfectly fine, especially now. He's such a wonderful guy." She smiled and opened the door.
As I drove away I realized we probably won't see each other again - his remaining time here will be saved for others now. There were so many thoughts, so much to remember, so much still to learn. Perhaps because I'd been through something like this before I was more prepared - it's never easy - but I still felt okay about it all - not sad - confident that we did the right thing...
... together.
-Wes
Showing posts with label teaching. Show all posts
Showing posts with label teaching. Show all posts
Thursday, September 25, 2014
Friday, June 06, 2014
On Mentoring
Recently, I had one of those "proud Daddy" moments: watching my son play in the Chicago Civic Orchestra's last concert of their 95th season. (For those unfamiliar, the Civic Orchestra is the training orchestra of the Chicago Symphony Orchestra.) They played Prokofiev's Symphony No. 5 under the direction of Jaap van Zweden - one of the most amazing conductors I have ever seen (and I later learned, one of my son's favorites). Afterward, we were invited to a reception and I had a chance to meet YoYo Ma who served as an inspiration, role model, and mentor for my son for the past year in his role as creative consultant with the orchestra. What a wonderful guy. He was fun, energetic, complimentary and thoughtful.
Later that night, my encounter with these artists got me thinking about my role as a mentor to young physicians. I teach residents. I teach EP fellows. What are they thinking? Am I doing all I can for them?
So it came as a surprise that I had just been offered to speak at a fellows conference later this year. The conference was sponsored by a major medical device manufacturer in a lovely US city. 100 fellows would be there along with 40 industry personnel. I would be paid well for my travel and speaking time. I'd connect with other contemporaries of mine whom I admire that would also serve as speakers. My topic involved an aspect of social media for physicians.
How could I resist?
And yet, here I am talking about the Health Care Industrial Complex and the Iron Triangle of comprised of Congress, special interests, bureaucracy and how doctors are swept up in their wake. I thought about being a mentor, a teacher, a doctor. I wondered how it might ever change. I wondered if doctors would ever have the courage to push back against the seductive powers of ego and money. Then I realized: probably not. It's how we're groomed for this from the beginning. We're human. So I have no doubt another doctor will be more than happy to serve as my replacement.
And so it goes.
But perhaps I could do what I love again, I could teach for the joy of watching young doctors get excited again, not because I needed to make a buck. Perhaps I could teach those same doctors that we do what we do because it's not about the corporate boondoggle, but about the patient. I could mentor.
So I declined the offer.
After all, I've got other priorities now.
-Wes
Later that night, my encounter with these artists got me thinking about my role as a mentor to young physicians. I teach residents. I teach EP fellows. What are they thinking? Am I doing all I can for them?
So it came as a surprise that I had just been offered to speak at a fellows conference later this year. The conference was sponsored by a major medical device manufacturer in a lovely US city. 100 fellows would be there along with 40 industry personnel. I would be paid well for my travel and speaking time. I'd connect with other contemporaries of mine whom I admire that would also serve as speakers. My topic involved an aspect of social media for physicians.
How could I resist?
And yet, here I am talking about the Health Care Industrial Complex and the Iron Triangle of comprised of Congress, special interests, bureaucracy and how doctors are swept up in their wake. I thought about being a mentor, a teacher, a doctor. I wondered how it might ever change. I wondered if doctors would ever have the courage to push back against the seductive powers of ego and money. Then I realized: probably not. It's how we're groomed for this from the beginning. We're human. So I have no doubt another doctor will be more than happy to serve as my replacement.
And so it goes.
But perhaps I could do what I love again, I could teach for the joy of watching young doctors get excited again, not because I needed to make a buck. Perhaps I could teach those same doctors that we do what we do because it's not about the corporate boondoggle, but about the patient. I could mentor.
So I declined the offer.
After all, I've got other priorities now.
-Wes
Wednesday, January 29, 2014
For Medical Students, It Seems Nothing's Changed
It was a very brief 15 minutes but I had arrived early. There they were, sitting in our conference room, waiting to be interviewed for a residency position at our institution. They had come from far and wide: California, New York, Michigan, for instance - all dressed in their nicest suits or business attire - a 50-50 split of bright women and men. I was to give a lecture as part of my monthly series on EKG interpretation that fell at this time of year. So these applicants could see how faculty interact with residents firsthand, I was asked to give my lecture to a crowded room of residents and the applicants together as part of their visit.
Since I had a few minutes, I introduced myself to the applicants and asked them how things were going. They were very complimentary (of course) and seemed eager to want to talk about something besides why they wanted to come to our institution for residency training. So being a bit subversive (of course) I asked what seemed like a little question: "How much does medical school cost these days?"
Heaven to Betsy, every one responded and shook their head. "It's cost me $75,000 in loans so far this year!" one female residency applicant exclaimed in an embarrassed tone. Most agreed that many of them were astonished at the costs, quoting some with debts of $300,000 to $400,000 for some of their classmates." "How did you do it?" they asked. And I mentioned by 26 years in the Navy and how I couldn't believe my roommate in medical school left with $65,000 debt at the time. They all laughed that I thought that was a lot of money, realizing how much more most of them owed in the present day. "I guess none of you are going into primary care, right?" I said. They laughed nervously, yet didn't really answer.
Medical school costs and the costs of educating America's physicians is in its bubble stage, about to pop. Our finest medical students are accruing huge debts and no one cares. After all, these young doctors were the lucky ones, right? Smart, social, good interpersonal skills, hard-working, driven, and most of all, disciplined. Look how lucky they are!
But when these young doctors look at their first salaries, reality will hit hard. They will realize the next mountain they will have to climb (as if medical school wasn't enough). Tough choices will have to be made. Needless to say, the picture for lower-paid specialties in medicine is particularly grim, yet the reality of fewer residency slots also exists. Depression, already a problem, is likely to increase.
In the past five years, the world of medicine has forever changed for everyone, except medical schools it seems. Their costs and expectations for revenue continues to exceed inflation by a large margin. When will it stop? For our newest trained doctors increasingly saddled with nearly insurmountable debt, the lure of medicine is waning. For those already in the pipeline, the reality of what's coming when the loan bills come due is inevitably going to be turning our best new hope for medicine's future away unless the cost problem is fixed soon.
I am not proposing we make medical school free - that would make things worse in my view. Different, more disruptive ideas that reign in costs will be needed - removing tenured professorial positions and limiting medical school building projects would be a good first step, but admittedly difficult with our entrenched old-school teaching model. Unless we really work to change the cost of educating our next generation physicians I fear that medicine's best hope for the future will quickly dwindle away.
-Wes
Since I had a few minutes, I introduced myself to the applicants and asked them how things were going. They were very complimentary (of course) and seemed eager to want to talk about something besides why they wanted to come to our institution for residency training. So being a bit subversive (of course) I asked what seemed like a little question: "How much does medical school cost these days?"
Heaven to Betsy, every one responded and shook their head. "It's cost me $75,000 in loans so far this year!" one female residency applicant exclaimed in an embarrassed tone. Most agreed that many of them were astonished at the costs, quoting some with debts of $300,000 to $400,000 for some of their classmates." "How did you do it?" they asked. And I mentioned by 26 years in the Navy and how I couldn't believe my roommate in medical school left with $65,000 debt at the time. They all laughed that I thought that was a lot of money, realizing how much more most of them owed in the present day. "I guess none of you are going into primary care, right?" I said. They laughed nervously, yet didn't really answer.
Medical school costs and the costs of educating America's physicians is in its bubble stage, about to pop. Our finest medical students are accruing huge debts and no one cares. After all, these young doctors were the lucky ones, right? Smart, social, good interpersonal skills, hard-working, driven, and most of all, disciplined. Look how lucky they are!
But when these young doctors look at their first salaries, reality will hit hard. They will realize the next mountain they will have to climb (as if medical school wasn't enough). Tough choices will have to be made. Needless to say, the picture for lower-paid specialties in medicine is particularly grim, yet the reality of fewer residency slots also exists. Depression, already a problem, is likely to increase.
In the past five years, the world of medicine has forever changed for everyone, except medical schools it seems. Their costs and expectations for revenue continues to exceed inflation by a large margin. When will it stop? For our newest trained doctors increasingly saddled with nearly insurmountable debt, the lure of medicine is waning. For those already in the pipeline, the reality of what's coming when the loan bills come due is inevitably going to be turning our best new hope for medicine's future away unless the cost problem is fixed soon.
I am not proposing we make medical school free - that would make things worse in my view. Different, more disruptive ideas that reign in costs will be needed - removing tenured professorial positions and limiting medical school building projects would be a good first step, but admittedly difficult with our entrenched old-school teaching model. Unless we really work to change the cost of educating our next generation physicians I fear that medicine's best hope for the future will quickly dwindle away.
-Wes
Tuesday, June 04, 2013
What I'd Tell the Graduating Medical School Class of 2013
Next week I'll be attending our medical school graduation and I wondered what I would tell them if I were chosen to give them a commencement address. This would not be an easy speech to write right now, given all of the uncertainties in health care that lie ahead, but I thought it would be interesting to try. Readers are invited to add their words as well in the comments section.
Dear Graduating Class of 2013 -
I appreciate the opportunity to address such an impressive pool of medical school attendees. From the first day of medical school when you were introduced to your cadaver, you have endured countless lectures and lab hours, physical examination and sensitivity training sessions, and ward rotations under the watchful eye of senior residents and attendings. Today, you will hold something that few people are privileged to sign behind their name: the letters "M.D."
This time in medicine is both a particularly exciting and particularly challenging one for doctors. How you deal with these challenges will determine your staying power in the profession.
During your training and long hours, you carefully cultivated your taste for fine coffee. At first, time allowed for a daily Venti-sized Starbucks mocha latte, but later as you learned the contributions of carbohydrates to your waist line, you switched to "only" black Ethiopian Harrar. Good for you. No doubt your upcoming days of residency will allow you some time to enjoy these delights a bit longer, but rest assured that by the time you call yourself an attending physician, you will be satisfied to drink a late night splash of automated coffee machine chemicals called "Coffee, Black" as you clean up the remaining work load left by residents who have exceeded the work hour restrictions you once enjoyed yourself. With this graduation, your sheltered medical workshop days are quickly coming to a close.
While most of you think this day is about you, realize there are some very important team players that have helped you get to where you are today. First and foremost are members of your family. They have encouraged you, guided you, and likely funded much of your way to this point. And the funding for medical school has been significant. The average medical school costs today, when one includes living expenses, exceeds $200,000. For those of you who did not have family members supporting you, realize that $200,000 of debt obligations translates to $843.21 per month if you plan to pay that loan off over 30 years at a low 3% interest rate. If your interest rate is higher, I feel for you. Yes, Virginia, medical school has become much too expensive.
But there is some good news. For the first time ever, instead of paying in to the health care education system, the health care system will start "giving back" and paying you. Admittedly at a very low rate. But at least it's your first tiny step in the right financial direction. Hopefully by the end of your residency training, the additional clinical experience you gain will finally allow you to make a bit higher salary than the nurse practitioners you work beside.
Fortunately, each of you began life as a medical student-doctor in the Gilded Age of Information Technology. Anything, you were taught, is possible with enough Big Data. But more data is not always better data. More data can confuse and obfuscate. More data might not be important data. And all that data comes at a cost to you: repetetive motion injuries. You see, Big Data is created from the information you will be asked to enter on your keyboard, iPAD, or via mouseclick or Google Glass. And since Big Data must now include a myriad of new procedure and diagnosis codes that you must learn, residency is not only a time to master disease states, but also a time to master your typing and coding skills. What ever you do, don't let Big Data detract from what matters most: your patient.
Your greatest challenge as a newly minted doctor in this Information Age will be to put your cellphone down. Looking up from its glowing screen will let you see your patient's downward stare as they tell you their deepest, personal secrets. If recognized, a trusting doctor-patient relationship will blossom. If missed, a feeling that you don't care may result. Remember that despite what the information technology zealots have been telling you, patients are not digital widgets, but analog, non-linear, feeling creatures who demand respect and intelligence. If you remember this, you will go far.
Many of you will be switching to new cities and new institutions to begin your residency training at a highly-esteemed medical school now that you've "matched." As you work to learn the clinical side of medicine, stay flexible. Fellowship positions are getting harder to come by as cuts to income for specialists continue. So hang on to those cardboard moving boxes - they might be needed sooner than you think. Honing hospitalist skills will probably be a wise choice, too.
And be prepared to have your heart broken. People will die despite your very best efforts. Complications occur, even to the most skilled and most cautious. Administrators will tell you to do things a certain way when you know that way's inefficient, but it pays your salary. People will deny payments for things that you know they shouldn't. A single malpractice lawsuit, even if ultimately found to be unwarranted, will forever change you - not for the better - but for the worse. And your wife and kids will still be affected when you arrive home late after missing your daughter's dance recital even though she says, "That's okay, Dad."
But despite all of these realities, there remain some wonderful aspects of medicine. People still will look up to you. People will still respect what you do and say. People will trust you, confide in you, and appreciate your efforts. You can do amazing things for people if you don't let the system get you down. Get involved in the process. Work to set the needs of your patients before that of the system and you'll usually be rewarded.
Because in the end, this is what really matters.
So go forward, not with an artificial glow about all that you have achieved, but with the stark reality of what lies ahead. These are challenging times for doctors as we increasingly encounter efforts to devalue all we've learned and experienced. Work to make the system better. Stay strong, work hard, and appreciate all you've got.
After all, there's plenty of people who would give anything to be in your shoes.
Good luck and God bless each and every one of you.
-Wes
Dear Graduating Class of 2013 -
I appreciate the opportunity to address such an impressive pool of medical school attendees. From the first day of medical school when you were introduced to your cadaver, you have endured countless lectures and lab hours, physical examination and sensitivity training sessions, and ward rotations under the watchful eye of senior residents and attendings. Today, you will hold something that few people are privileged to sign behind their name: the letters "M.D."
This time in medicine is both a particularly exciting and particularly challenging one for doctors. How you deal with these challenges will determine your staying power in the profession.
During your training and long hours, you carefully cultivated your taste for fine coffee. At first, time allowed for a daily Venti-sized Starbucks mocha latte, but later as you learned the contributions of carbohydrates to your waist line, you switched to "only" black Ethiopian Harrar. Good for you. No doubt your upcoming days of residency will allow you some time to enjoy these delights a bit longer, but rest assured that by the time you call yourself an attending physician, you will be satisfied to drink a late night splash of automated coffee machine chemicals called "Coffee, Black" as you clean up the remaining work load left by residents who have exceeded the work hour restrictions you once enjoyed yourself. With this graduation, your sheltered medical workshop days are quickly coming to a close.
While most of you think this day is about you, realize there are some very important team players that have helped you get to where you are today. First and foremost are members of your family. They have encouraged you, guided you, and likely funded much of your way to this point. And the funding for medical school has been significant. The average medical school costs today, when one includes living expenses, exceeds $200,000. For those of you who did not have family members supporting you, realize that $200,000 of debt obligations translates to $843.21 per month if you plan to pay that loan off over 30 years at a low 3% interest rate. If your interest rate is higher, I feel for you. Yes, Virginia, medical school has become much too expensive.
But there is some good news. For the first time ever, instead of paying in to the health care education system, the health care system will start "giving back" and paying you. Admittedly at a very low rate. But at least it's your first tiny step in the right financial direction. Hopefully by the end of your residency training, the additional clinical experience you gain will finally allow you to make a bit higher salary than the nurse practitioners you work beside.
Fortunately, each of you began life as a medical student-doctor in the Gilded Age of Information Technology. Anything, you were taught, is possible with enough Big Data. But more data is not always better data. More data can confuse and obfuscate. More data might not be important data. And all that data comes at a cost to you: repetetive motion injuries. You see, Big Data is created from the information you will be asked to enter on your keyboard, iPAD, or via mouseclick or Google Glass. And since Big Data must now include a myriad of new procedure and diagnosis codes that you must learn, residency is not only a time to master disease states, but also a time to master your typing and coding skills. What ever you do, don't let Big Data detract from what matters most: your patient.
Your greatest challenge as a newly minted doctor in this Information Age will be to put your cellphone down. Looking up from its glowing screen will let you see your patient's downward stare as they tell you their deepest, personal secrets. If recognized, a trusting doctor-patient relationship will blossom. If missed, a feeling that you don't care may result. Remember that despite what the information technology zealots have been telling you, patients are not digital widgets, but analog, non-linear, feeling creatures who demand respect and intelligence. If you remember this, you will go far.
Many of you will be switching to new cities and new institutions to begin your residency training at a highly-esteemed medical school now that you've "matched." As you work to learn the clinical side of medicine, stay flexible. Fellowship positions are getting harder to come by as cuts to income for specialists continue. So hang on to those cardboard moving boxes - they might be needed sooner than you think. Honing hospitalist skills will probably be a wise choice, too.
And be prepared to have your heart broken. People will die despite your very best efforts. Complications occur, even to the most skilled and most cautious. Administrators will tell you to do things a certain way when you know that way's inefficient, but it pays your salary. People will deny payments for things that you know they shouldn't. A single malpractice lawsuit, even if ultimately found to be unwarranted, will forever change you - not for the better - but for the worse. And your wife and kids will still be affected when you arrive home late after missing your daughter's dance recital even though she says, "That's okay, Dad."
 |
| An example of a few much-appreciated thank-you notes you'll receive (Click to enlarge) |
Because in the end, this is what really matters.
So go forward, not with an artificial glow about all that you have achieved, but with the stark reality of what lies ahead. These are challenging times for doctors as we increasingly encounter efforts to devalue all we've learned and experienced. Work to make the system better. Stay strong, work hard, and appreciate all you've got.
After all, there's plenty of people who would give anything to be in your shoes.
Good luck and God bless each and every one of you.
-Wes
Friday, May 03, 2013
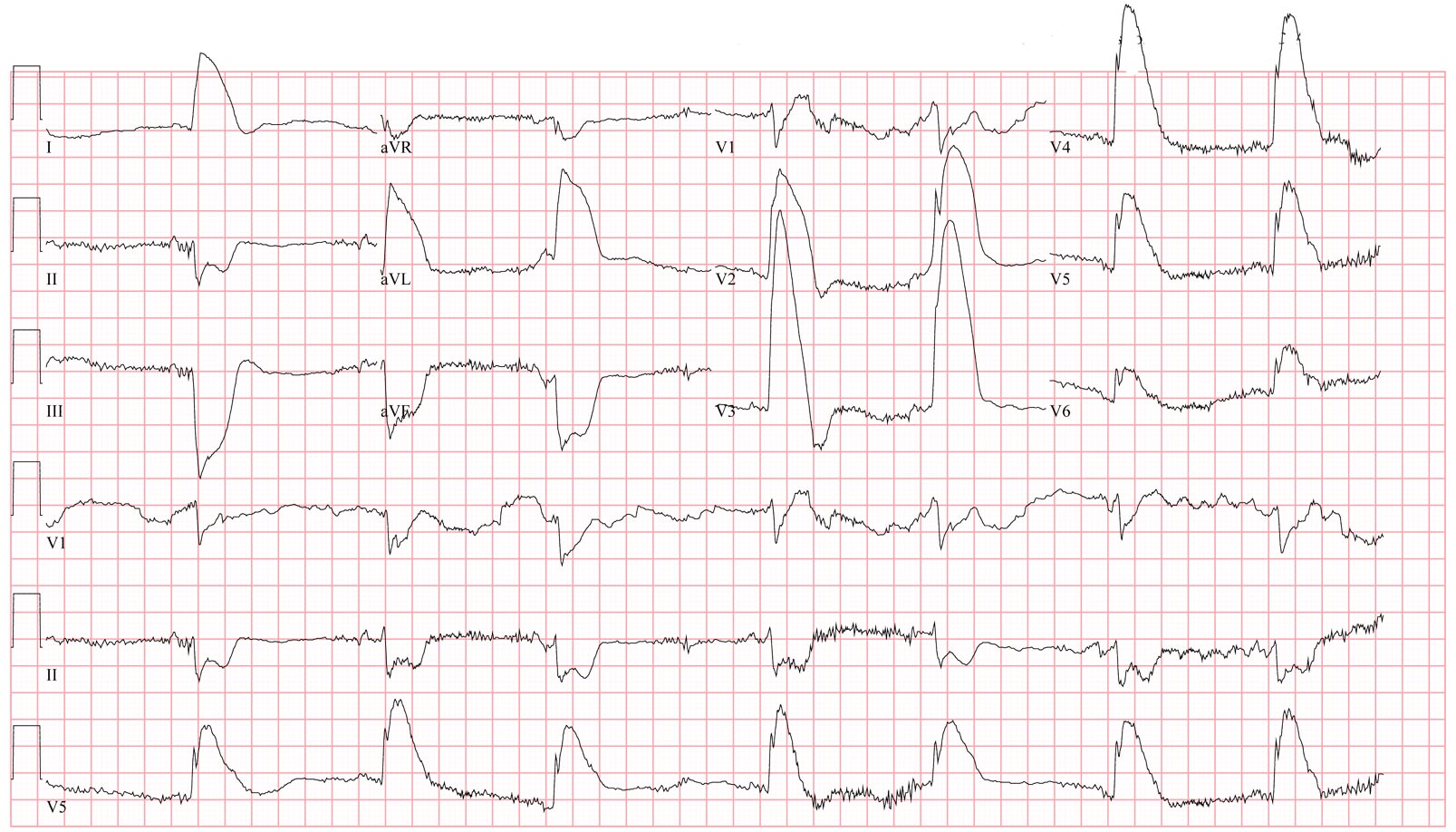
EKG Du Jour #31: A Case of Chest Pain
A 61 year old patient presented to your ER with chest pain, low blood pressure, and this EKG:
Now before you leap to the answer at the link provided below, ask yourself:
(a) What is this?
(b) What could cause this?
(c) How would you manage it?
And when you've really thought about it, click here for the answer but be prepared to describe what you see and what you'd do next.
-Wes
P.S.: (Yeah, I'm giving the answer now because it's Friday)
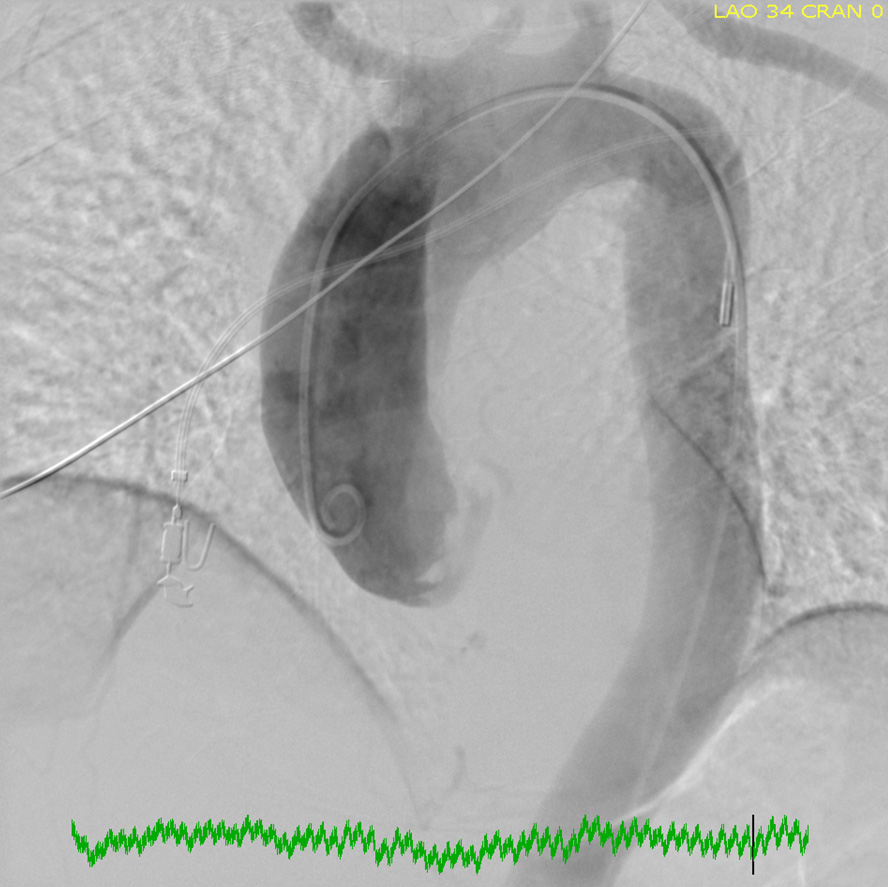
 |
| (Click image to enlarge) |
Now before you leap to the answer at the link provided below, ask yourself:
(a) What is this?
(b) What could cause this?
(c) How would you manage it?
And when you've really thought about it, click here for the answer but be prepared to describe what you see and what you'd do next.
{kind=link}
-Wes
P.S.: (Yeah, I'm giving the answer now because it's Friday)
Sunday, February 24, 2013
How Big Data's Fueling Complacency
"What's the most important finding on this chest x-ray?"
There he was, standing before 5 ICU residents, each peering at a chest film on displayed on the over-sized computer screen.
"Um, the pleural effusion?" whimpered a third-year resident.
"No!" barked the attending.
The others, standing dumbfounded in front of the computer display, searching for another finding but finding none, stood silently.
"Come on, folks! Look!"
And try as they may, no one saw it.
"The name, folks, the name!" the attending said impatiently.
And there it was, a tiny reminder of whose x-ray it was, quietly lurking in tiny print in the upper right corner of the computer screen, unmagnified.
But wait, the name was correct. What the heck was he talking about?
Closer inspection showed another critical piece of information, totally lost on almost everyone standing there: the date of birth of the patient. It was not the same as the patient being discussed. They were looking at the wrong patient's chest x-ray. Never mind that their patient had a chest tube placed on the opposite side that wasn't shown on the displayed chest x-ray. Yet they were already trying to make decisions for care.
***
I recently taught an EKG reading class and had a similar experience to the one above. Since July, I've been teaching the basics of EKG reading at least once a month: rate, rhythm, axis, intervals - you know the drill, right?
But I (once again) asked about the axis of an EKG tracing we were discussing some six months later. A room full of at least twenty residents sat quietly. No one answered.
I kept my composure. I prodded them gently, hoping to hear an answer yet none came. Were they on call? Distracted by their cell phones or pending work? Am I THAT boring?
Still nothing.
So I reviewed how we determine EKG axis, and quickly, a few remembered the concept and gratefully, responded correctly.
But these experiences got me thinking about the effects Big Data is having on our residents today and its tendency to build complacency. Why learn something if you're always spoon-fed it right?
Admittedly, our medical data explosion has prevented us from knowing everything there is to know about anatomy, physiology, pathology, treatment options and the like. There is a role for access to Big Data.
But increasingly the data we feed our residents and medical schools is nothing but printed characters: x-ray reports, EKG interpretations, study results like "ejection fraction:" all limited to the 256 ASCII character set. Residents no longer feel the need to look at the raw image and formulate their own opinion - they'll just look at the printed report. They expect the data to be fed to them in printed format. They expect the reading to be correct. In a way, they're growing up expecting to be spoon fed just the black-and-white answers rather than the brilliant data provided by pictures. Just "google it."
Never mind the computer says "atrial fibrillation" because the original EKG contains noise.
Such an "Big Data-entitled" approach to health care is extremely dangerous, especially if the data upon which decisions are based, are wrong. Residents should never forget two things my father always told me:
"Garbage in, garbage out" and "expect what you inspect."
-Wes
There he was, standing before 5 ICU residents, each peering at a chest film on displayed on the over-sized computer screen.
"Um, the pleural effusion?" whimpered a third-year resident.
"No!" barked the attending.
The others, standing dumbfounded in front of the computer display, searching for another finding but finding none, stood silently.
"Come on, folks! Look!"
And try as they may, no one saw it.
"The name, folks, the name!" the attending said impatiently.
And there it was, a tiny reminder of whose x-ray it was, quietly lurking in tiny print in the upper right corner of the computer screen, unmagnified.
But wait, the name was correct. What the heck was he talking about?
Closer inspection showed another critical piece of information, totally lost on almost everyone standing there: the date of birth of the patient. It was not the same as the patient being discussed. They were looking at the wrong patient's chest x-ray. Never mind that their patient had a chest tube placed on the opposite side that wasn't shown on the displayed chest x-ray. Yet they were already trying to make decisions for care.
***
I recently taught an EKG reading class and had a similar experience to the one above. Since July, I've been teaching the basics of EKG reading at least once a month: rate, rhythm, axis, intervals - you know the drill, right?
But I (once again) asked about the axis of an EKG tracing we were discussing some six months later. A room full of at least twenty residents sat quietly. No one answered.
I kept my composure. I prodded them gently, hoping to hear an answer yet none came. Were they on call? Distracted by their cell phones or pending work? Am I THAT boring?
Still nothing.
So I reviewed how we determine EKG axis, and quickly, a few remembered the concept and gratefully, responded correctly.
But these experiences got me thinking about the effects Big Data is having on our residents today and its tendency to build complacency. Why learn something if you're always spoon-fed it right?
Admittedly, our medical data explosion has prevented us from knowing everything there is to know about anatomy, physiology, pathology, treatment options and the like. There is a role for access to Big Data.
But increasingly the data we feed our residents and medical schools is nothing but printed characters: x-ray reports, EKG interpretations, study results like "ejection fraction:" all limited to the 256 ASCII character set. Residents no longer feel the need to look at the raw image and formulate their own opinion - they'll just look at the printed report. They expect the data to be fed to them in printed format. They expect the reading to be correct. In a way, they're growing up expecting to be spoon fed just the black-and-white answers rather than the brilliant data provided by pictures. Just "google it."
Never mind the computer says "atrial fibrillation" because the original EKG contains noise.
Such an "Big Data-entitled" approach to health care is extremely dangerous, especially if the data upon which decisions are based, are wrong. Residents should never forget two things my father always told me:
"Garbage in, garbage out" and "expect what you inspect."
-Wes
Wednesday, September 12, 2012
The Irony of Why EKG Class Was Cancelled
I look forward to teaching our housestaff the basics of EKGs each year. Moments where I can leap from worker-bee clinician to the quiet confines of a lecture hall is rejuvenating. Seeing eyes widen as they grasp basic insights to the wealth of information contained in biologic signals even more so. So I carve some time at the beginning of each year with the chief residents to commit to this endeavor far in advance.
This year, I arrived a little early for my lecture with a stack of EKG’s, ready to bring down the screen, load the Powerpoint presentation, and collect my thoughts. Unlike most lecture days, the lecture hall door was closed when I arrived. I quietly cracked the door and peered in: there, in their new, carefully pressed white coats, was a sea of residents. I was elated, expecting that attendance at this lecture would be especially high since I already had a captive audience.
So I closed the door quietly and paced in the halls waiting for the lecture before mine to conclude.
The nearby secretaries noticed me and politely said hello and I, in turn, smiled and acknowledged their greeting. I grabbed a quick cup of coffee from the coffee pot and sipped the nectar in my quiet moment of reverie before class.
But something was askew. The secretaries seemed a bit uncomfortable.
“Doctor Fisher? Oh, I’m so sorry, the lecture hall is being used today for our annual Transitional Residency program review. Let me see if I can find another lecture hall for you.”
She logged on her computer and scanned the available spaces. She clicked and clicked and clicked.
“Well, there is a room on the fifth floor…. Um, maybe not. I see there’s only 15 chairs in there… Let me keep trying.”
“Thanks so much,” I said.
About this time, the doors from my previously-arranged lecture hall opened and a sea of smiling residents poured out from the room. Some headed to the washroom, others checking their beepers. Others appeared to be heading back to the wards. I was puzzled.
I glanced in the lecture hall to see several well-dressed women sitting before a pile of 3-ring binders full of papers, one of which was opened. They chatted with each other, occasionally giggling, but very professionally so. There behind them was a tray of uneaten donuts and other treats and a coffee dispenser neatly arranged on a tray behind them. Boy, those looked tasty! I smiled as I thought to myself: “No wonder their attendance was so good.”
A few moments later, one of the Chief Residents came to me with his tail between his legs and apologized profusely. “I’m SO sorry, Dr. Fisher, we forgot to call you about this change of schedule!”
The poor guy. Sent with full flak jacket in place to take the hit. But I knew exactly how he felt as he tried to keep all the various clinical and administrative scheduling balls in the air.
“No problem,” I said. “We’ll do this another time.”
But as I walked back to my office, I couldn’t help but wonder what we’re creating as housestaff are corralled before bureaucrats who ask them how their residency is going while their own residency's EKG training was silently sabotaged.
It’s kind of like those uneaten donuts behind those well-dressed ladies: food for thought.
-Wes
This year, I arrived a little early for my lecture with a stack of EKG’s, ready to bring down the screen, load the Powerpoint presentation, and collect my thoughts. Unlike most lecture days, the lecture hall door was closed when I arrived. I quietly cracked the door and peered in: there, in their new, carefully pressed white coats, was a sea of residents. I was elated, expecting that attendance at this lecture would be especially high since I already had a captive audience.
So I closed the door quietly and paced in the halls waiting for the lecture before mine to conclude.
The nearby secretaries noticed me and politely said hello and I, in turn, smiled and acknowledged their greeting. I grabbed a quick cup of coffee from the coffee pot and sipped the nectar in my quiet moment of reverie before class.
But something was askew. The secretaries seemed a bit uncomfortable.
“Doctor Fisher? Oh, I’m so sorry, the lecture hall is being used today for our annual Transitional Residency program review. Let me see if I can find another lecture hall for you.”
She logged on her computer and scanned the available spaces. She clicked and clicked and clicked.
“Well, there is a room on the fifth floor…. Um, maybe not. I see there’s only 15 chairs in there… Let me keep trying.”
“Thanks so much,” I said.
About this time, the doors from my previously-arranged lecture hall opened and a sea of smiling residents poured out from the room. Some headed to the washroom, others checking their beepers. Others appeared to be heading back to the wards. I was puzzled.
I glanced in the lecture hall to see several well-dressed women sitting before a pile of 3-ring binders full of papers, one of which was opened. They chatted with each other, occasionally giggling, but very professionally so. There behind them was a tray of uneaten donuts and other treats and a coffee dispenser neatly arranged on a tray behind them. Boy, those looked tasty! I smiled as I thought to myself: “No wonder their attendance was so good.”
A few moments later, one of the Chief Residents came to me with his tail between his legs and apologized profusely. “I’m SO sorry, Dr. Fisher, we forgot to call you about this change of schedule!”
The poor guy. Sent with full flak jacket in place to take the hit. But I knew exactly how he felt as he tried to keep all the various clinical and administrative scheduling balls in the air.
“No problem,” I said. “We’ll do this another time.”
But as I walked back to my office, I couldn’t help but wonder what we’re creating as housestaff are corralled before bureaucrats who ask them how their residency is going while their own residency's EKG training was silently sabotaged.
It’s kind of like those uneaten donuts behind those well-dressed ladies: food for thought.
-Wes
Tuesday, June 28, 2011
For Interns: Ten Rules to Go By
He sat in a crisp white coat, staring at a computer screen, note cards in his lap. Occasionally, I noted him jot a note to himself as he compiled his list. A nurse sat next to him, pounding feverishly on the keyboard as she recorded her nurse’s note. He tentatively moved his mouse, then clicked, still staring.
I recall my first day in clinical medicine: no computer, an ER rotation, a white board filled with names and abbreviated medical problems next to them with little magnetic color-coded labels nearby. Room 1: Head trauma. Room 2: Abscess. Room 3: UTI, Room 4: Rash.
I got room 2. It was the biggest, bad-est infected sebaceous cyst on a guy’s back a newly minted doctor had ever seen. Can you say “softball?” “See one, do one,” they told me. And off I went.
Much in medicine has changed since then, but much remains the same. Medicine is miraculous, terrifying, then rewarding all at once. Fortunately, there’s a method within the madness that can serve to preserve and protect those who first start out. Every doctor has had the fortune to learn from those who passed before them as begin their journey to refine their title of “doctor” (literally, “teacher.”)
I thought it would be interesting to put a few of the “Rules of the Road for Medicine” down on paper (with the help of friends on Twitter) for interns and residents as they embark on their own incredible journey ahead. The list is not exhaustive, but hopefully can serve as a resource for our new doctors as they head off to meet their clinical challenges ahead.
Rule #1: Treat every patient like your mother
Obey this rule and you’ll do the right thing more often than not. If it means staying late, do it. If it means going the extra mile, do it. If people disagree as to a specific approach to care, ask yourself “What would my mother want?” Then go that direction. Be kind. Be respectful. Wear clean clothes, brush your teeth, comb your hair, and look your best. (Note: @DrElizabethLee was quick to remind me that kids are not always kind and respectful, so their age might require a slightly more top-down, “parental” approach.)
Rule #2: There are an infinite number of ways to get screwed
That’s right – not a thousand, not a million, not ten billion – but an infinite number of ways… Check and recheck. If you’re not sure, check it again. Somewhere out there, born 20 years or so ago, there is a person whose sole mission in life is to thwart your efforts to protect your patient. It usually is not intentional, mind you, but it happens. Like the nurse who feeds the patient breakfast when they’re NPO after midnight, or the orderly who accidentally trips and pulls out the IV or better yet, the pacemaker wires. Oh yeah, it happens. So double-tape where single-tape might do. Communicate. Involve the team. If you’ve got a better idea, say so. If someone else has a better idea, defer to them. Park your ego at the door and work to avoid the errors. Everyone will benefit if you do.
Surgeons always emphasize this point, but it extends far beyond the obvious. Consider it shorthand for “do the physical.” Trust no one except yourself and what you see, hear, and feel. More often than not, you’ll be rewarded with the satisfaction of finding something no one else has, simply because you made the effort to lift the covers and do the exam.
So research, research, research. Don’t be cocky. Humility is paramount since there’s nothing like the vagaries of medicine and individual circumstances and personalities to take the wind out of your sail. No single person (or website) has all the answers. Attend the lectures while you still can: you’ll never be spoon-fed like that again. Remember: the learning never ends. (h/t @sonodoc99 and @shartiga)
Rule #5: Your family is your anchor
Spend time with them. Make them a priority. Surprise your spouse or significant other with flowers, or better yet, carry-out. If safe to do so, leave work to attend the kids’ assemblies at school or their sports games and return later if you still have work to do. Do this and they might even help with your laundry once in a while. (h/t @DoctorNatasha)
Rule #6: It’s okay to say “I don’t know”
… just be sure to add “… but I’ll look it up.” More often than not, someone else might have an idea, so bring in the cavalry. Use the phone and call the expert – even if he or she is in another state or country. Still, if the answer remains elusive, it really is okay to say you really don’t know what to do. Sometime there is nothing you can do. And once in a while when all other options have been exhausted, don’t forget to ask the patient or family for their help to see if they have another idea that you haven’t tried. (h/t: @kevinmd)
Rule #7: If you screw up, say you’re sorry.
Lots has been written on this, and certainly there’s an appropriate time and place for doing so, but take the time to offer your apologies if a mistake occurs. Work to make sure the mistake doesn’t happen again and realize there is an important bond that forms when a doctor sticks with his or her patient through thick and thin. (h/t: @kevinmd)
Rule #8 – Play nice
Nurses, respiratory technicians, physical therapists, nurse practitioners, dietary personnel, pharmacists, and the EMT's/paramedics are your friends – keep them that way. Be respectful, appreciate their skills, and use their expertise. Most important, before you try to lie down on call, ask the covering nurse(s) if there’s anything they need before you retire. It might just save you a page. (h/t: @rlbates)
Rule #9 – Crazy people get sick, too
So be sure to attend to rules #1, #2, and #3. (h/t: @InpatientMed
Rule #10 – Do the dirty work
All you have to do is help with nurse with a digital disimpaction, enema, or cleanup of a dirty bed and you’ll be an instant hero. Word travels fast. After all, believe it or not, you are not above the others. You are part of a team: just one member with a bit more responsibility at times. By helping, you’ll be helped. By caring, you’ll be cared for. And sometimes, your new patients or colleagues might even bring you cookies.
-Wes
10:20PM CST Addendum: The corollary to Rule #3 was added and edits to Rule #8 made to include EMT's and paramedics. Thanks to all those who have contributed to this post! (Keep 'em coming!)
I recall my first day in clinical medicine: no computer, an ER rotation, a white board filled with names and abbreviated medical problems next to them with little magnetic color-coded labels nearby. Room 1: Head trauma. Room 2: Abscess. Room 3: UTI, Room 4: Rash.
I got room 2. It was the biggest, bad-est infected sebaceous cyst on a guy’s back a newly minted doctor had ever seen. Can you say “softball?” “See one, do one,” they told me. And off I went.
Much in medicine has changed since then, but much remains the same. Medicine is miraculous, terrifying, then rewarding all at once. Fortunately, there’s a method within the madness that can serve to preserve and protect those who first start out. Every doctor has had the fortune to learn from those who passed before them as begin their journey to refine their title of “doctor” (literally, “teacher.”)
I thought it would be interesting to put a few of the “Rules of the Road for Medicine” down on paper (with the help of friends on Twitter) for interns and residents as they embark on their own incredible journey ahead. The list is not exhaustive, but hopefully can serve as a resource for our new doctors as they head off to meet their clinical challenges ahead.
Rule #1: Treat every patient like your mother
Obey this rule and you’ll do the right thing more often than not. If it means staying late, do it. If it means going the extra mile, do it. If people disagree as to a specific approach to care, ask yourself “What would my mother want?” Then go that direction. Be kind. Be respectful. Wear clean clothes, brush your teeth, comb your hair, and look your best. (Note: @DrElizabethLee was quick to remind me that kids are not always kind and respectful, so their age might require a slightly more top-down, “parental” approach.)
Rule #2: There are an infinite number of ways to get screwed
That’s right – not a thousand, not a million, not ten billion – but an infinite number of ways… Check and recheck. If you’re not sure, check it again. Somewhere out there, born 20 years or so ago, there is a person whose sole mission in life is to thwart your efforts to protect your patient. It usually is not intentional, mind you, but it happens. Like the nurse who feeds the patient breakfast when they’re NPO after midnight, or the orderly who accidentally trips and pulls out the IV or better yet, the pacemaker wires. Oh yeah, it happens. So double-tape where single-tape might do. Communicate. Involve the team. If you’ve got a better idea, say so. If someone else has a better idea, defer to them. Park your ego at the door and work to avoid the errors. Everyone will benefit if you do.
- Corollary: “If there’s a test for it, just get the test.” (h/t: @gruntdoc)Rule #3: Do the rectal.
Surgeons always emphasize this point, but it extends far beyond the obvious. Consider it shorthand for “do the physical.” Trust no one except yourself and what you see, hear, and feel. More often than not, you’ll be rewarded with the satisfaction of finding something no one else has, simply because you made the effort to lift the covers and do the exam.
- Corollary: Believe none of what your hear, half of what you see, all of what you do. (h/t: Benjamin Franklin via @MGKatz036)Rule #4: Medicine is like life – no “always” and no “nevers”
So research, research, research. Don’t be cocky. Humility is paramount since there’s nothing like the vagaries of medicine and individual circumstances and personalities to take the wind out of your sail. No single person (or website) has all the answers. Attend the lectures while you still can: you’ll never be spoon-fed like that again. Remember: the learning never ends. (h/t @sonodoc99 and @shartiga)
Rule #5: Your family is your anchor
Spend time with them. Make them a priority. Surprise your spouse or significant other with flowers, or better yet, carry-out. If safe to do so, leave work to attend the kids’ assemblies at school or their sports games and return later if you still have work to do. Do this and they might even help with your laundry once in a while. (h/t @DoctorNatasha)
Rule #6: It’s okay to say “I don’t know”
… just be sure to add “… but I’ll look it up.” More often than not, someone else might have an idea, so bring in the cavalry. Use the phone and call the expert – even if he or she is in another state or country. Still, if the answer remains elusive, it really is okay to say you really don’t know what to do. Sometime there is nothing you can do. And once in a while when all other options have been exhausted, don’t forget to ask the patient or family for their help to see if they have another idea that you haven’t tried. (h/t: @kevinmd)
Rule #7: If you screw up, say you’re sorry.
Lots has been written on this, and certainly there’s an appropriate time and place for doing so, but take the time to offer your apologies if a mistake occurs. Work to make sure the mistake doesn’t happen again and realize there is an important bond that forms when a doctor sticks with his or her patient through thick and thin. (h/t: @kevinmd)
Rule #8 – Play nice
Nurses, respiratory technicians, physical therapists, nurse practitioners, dietary personnel, pharmacists, and the EMT's/paramedics are your friends – keep them that way. Be respectful, appreciate their skills, and use their expertise. Most important, before you try to lie down on call, ask the covering nurse(s) if there’s anything they need before you retire. It might just save you a page. (h/t: @rlbates)
Rule #9 – Crazy people get sick, too
So be sure to attend to rules #1, #2, and #3. (h/t: @InpatientMed
Rule #10 – Do the dirty work
All you have to do is help with nurse with a digital disimpaction, enema, or cleanup of a dirty bed and you’ll be an instant hero. Word travels fast. After all, believe it or not, you are not above the others. You are part of a team: just one member with a bit more responsibility at times. By helping, you’ll be helped. By caring, you’ll be cared for. And sometimes, your new patients or colleagues might even bring you cookies.
-Wes
10:20PM CST Addendum: The corollary to Rule #3 was added and edits to Rule #8 made to include EMT's and paramedics. Thanks to all those who have contributed to this post! (Keep 'em coming!)
Tuesday, April 05, 2011
Lessons
It was one of those lectures you never forget.
Years ago, in my first year of medical school, we took our first of many amazing classes: human anatomy. There you were, day 1, all bright-eyed and bushy-tailed, walking to the basement of the hospital with your assigned fellow-students after a rousing introductory lecture into the anatomy lab.
There, in a huge well-lit room, stood a sea of steel tables covered in thick plastic bags with their most unusual contents: human cadavers.
Your first job?
To remove the bag as a team.
No one can forget that day, or that semester for that matter, as a medical student. The smell of formaldehyde that pierces your nostrils and permeates every pore of your hands while seemingly flavoring your lunchtime meals. The smell was your identifier as you stood in the lunch line: you were a first-year.
It would be easy to write about those days in the lab, but this is a story outside the lab that stuck with me through all of these years in the every-Friday lecture called “Clinical Correlations.” In that lecture we would apply the anatomy we had learned from our careful dissections earlier in the week to other clinical scenarios. The class was conducted by a brilliant radiologist. He shared his vast library of carefully-categorized radiographs with us in class and pointed to a spot on the radiographs while asking: “What’s this?” Or as we learned more disease processes that affected anatomy: “What disease might cause this?”
Very cool.
One Friday late in the year after we had completed the laborious task of dissecting the entire abdominal contents, he brought in a series of “unknown” radiographs. He would have us compete to see who could answer correctly first: winner got a trinket; losers (incorrect answers) got public humiliation and laughs from their peers. It was always a very lively class.
Little did we know what he had in store for us.
Up went the first radiograph, a pause, then: “The kid swallowed a penny!” someone would shout. “No, a quarter,” he would answer, “… but close enough.”
Then another. People stared for a while, couldn’t recognize what it was but we all knew it was something mechanical, there, in the projection of the ascending colon. Um, could it be? Yes, another foreign body that had migrated there with the switch turned on. We call cringed, amazed that he had seen such a thing. (We were young).
Then finally, as if we had not had enough, a final flat plate of the abdomen. I think I saw it first, and started laughing. He looked at me with eyes that could have pierced the thick hide of a water buffalo. He didn’t crack a smile at all. Suddenly, another female classmate blurted out, “Oh my goodness, is that a lightbulb?”
He replied to our amusement, “Yes it is: a 60-watt bulb, wide end first, in a 40-watt rectum.” By now the entire class was howling while simultaneously turning to each other and cringing. But he looked serious.
“I’d like to say something to you as future physicians,” he said above the din of laughter. Things quieted a bit as he spoke. “You will see things in your careers that are far stranger than this,” he continued, “and you must forever remember that you are dealing with a real person in real need.” Silence. “This was a situation that required the utmost discretion to manage: can you imagine what would happen to that patient if the bulb broke?” We considered the horrible consequences. “How would you handle this?”
Suddenly, the entire class felt impotent, struggling to imagine themselves in such a scenario. We quickly realized the joke was on us. We were clueless as our minds whirled to find a solution. No one could.
In the end he described the general anesthesia, the delivery forceps, and the team approach required to manage such a challenging situation and closed with these words:
“Guys, no matter how weird, how repulsive, how funny, or how crazy a situation might seem, when you see that person you MUST speak with them as though it’s the fifth case like that you’ve seen that day and respect the person’s dignity no matter what. Don’t ever forget that.”
I never have.
-Wes
Years ago, in my first year of medical school, we took our first of many amazing classes: human anatomy. There you were, day 1, all bright-eyed and bushy-tailed, walking to the basement of the hospital with your assigned fellow-students after a rousing introductory lecture into the anatomy lab.
There, in a huge well-lit room, stood a sea of steel tables covered in thick plastic bags with their most unusual contents: human cadavers.
Your first job?
To remove the bag as a team.
No one can forget that day, or that semester for that matter, as a medical student. The smell of formaldehyde that pierces your nostrils and permeates every pore of your hands while seemingly flavoring your lunchtime meals. The smell was your identifier as you stood in the lunch line: you were a first-year.
It would be easy to write about those days in the lab, but this is a story outside the lab that stuck with me through all of these years in the every-Friday lecture called “Clinical Correlations.” In that lecture we would apply the anatomy we had learned from our careful dissections earlier in the week to other clinical scenarios. The class was conducted by a brilliant radiologist. He shared his vast library of carefully-categorized radiographs with us in class and pointed to a spot on the radiographs while asking: “What’s this?” Or as we learned more disease processes that affected anatomy: “What disease might cause this?”
Very cool.
One Friday late in the year after we had completed the laborious task of dissecting the entire abdominal contents, he brought in a series of “unknown” radiographs. He would have us compete to see who could answer correctly first: winner got a trinket; losers (incorrect answers) got public humiliation and laughs from their peers. It was always a very lively class.
Little did we know what he had in store for us.
Up went the first radiograph, a pause, then: “The kid swallowed a penny!” someone would shout. “No, a quarter,” he would answer, “… but close enough.”
Then another. People stared for a while, couldn’t recognize what it was but we all knew it was something mechanical, there, in the projection of the ascending colon. Um, could it be? Yes, another foreign body that had migrated there with the switch turned on. We call cringed, amazed that he had seen such a thing. (We were young).
Then finally, as if we had not had enough, a final flat plate of the abdomen. I think I saw it first, and started laughing. He looked at me with eyes that could have pierced the thick hide of a water buffalo. He didn’t crack a smile at all. Suddenly, another female classmate blurted out, “Oh my goodness, is that a lightbulb?”
He replied to our amusement, “Yes it is: a 60-watt bulb, wide end first, in a 40-watt rectum.” By now the entire class was howling while simultaneously turning to each other and cringing. But he looked serious.
“I’d like to say something to you as future physicians,” he said above the din of laughter. Things quieted a bit as he spoke. “You will see things in your careers that are far stranger than this,” he continued, “and you must forever remember that you are dealing with a real person in real need.” Silence. “This was a situation that required the utmost discretion to manage: can you imagine what would happen to that patient if the bulb broke?” We considered the horrible consequences. “How would you handle this?”
Suddenly, the entire class felt impotent, struggling to imagine themselves in such a scenario. We quickly realized the joke was on us. We were clueless as our minds whirled to find a solution. No one could.
In the end he described the general anesthesia, the delivery forceps, and the team approach required to manage such a challenging situation and closed with these words:
“Guys, no matter how weird, how repulsive, how funny, or how crazy a situation might seem, when you see that person you MUST speak with them as though it’s the fifth case like that you’ve seen that day and respect the person’s dignity no matter what. Don’t ever forget that.”
I never have.
-Wes
Friday, January 28, 2011
Social Media and the Challenge of Overcoming Intellectual Complacency
They lined the walls in a warm room as far from the central table as possible. They had come to learn about EKG's. Residents of at varying years of training sat amongst the interns, much the same way as the Democrats sat amongst the Republican's at the recent presidential State-of-the-Union address: cordial - not too aloof.
I was fortunate to be the lucky guy to teach them that day. I have always enjoyed this opportunity and generally the lectures seem to be well-received and attended. This was lecture toward the latter part of the year, so things were not the chip-shot tracings that most learn in ACLS. Still, we always harken back to the fundamentals of reading tracings to help us understand new concepts, but I encountered a strange silence when I discussed the EKG's of patients with pacemakers:
"We all hear the phrase "He's got a DDD pacemaker," right?
They all uniformly nodded they'd heard the phrase, so I asked further:
"What do the letters in the term 'DDD pacemaker' mean?"
Silence overcame the room.
Perhaps I had caught them off guard. Many of their eyes fell to the floor. Some smiled but failed to answer. Some were clearly unnerved by the question as they shifted in their seats. A cough could be heard in the corner - it might as well have been a pin dropping. In the back right-hand corner a pager sounded. Everyone turned to the lucky contestant who was saved by the beep. Finally, somewhere toward the opposite corner of the room came a faint suggestion:
"Isn't one of them mean which chamber is paced?"
Relieved, you could see a few heads nodding now.
"Which letter of the three represents that?"
Again, the room fell silent.
Needless to say, we moved on from there after a quick basic review of pacing terminology, but his got me thinking: where have we failed to teach our medical students and residents such fairly basic clinical concepts and vernacular we use every day? Are we spending too much time on the Krebs cycle and not enough time on clinically relevant concepts in medical school and internship? How do we get them to remember?
So I had an idea: what if I used social media?
We all know that every medical student and resident (and doctor and patient, for that matter) has a cell phone. Might we use Twitter to try to teach small snippets of information to our trainees? Obviously they would have to have a Twitter account. Also, not all concepts lend themselves to this appraoch very well, but it might be worth a trial.
Soooooo, look for an occassional Electrophysiology Quiz via Twitter from yours truly. (Others with ideas for ultra-short cardiac electrophysiology quizes are welcome to join in the fun, just use the hashtag '#epquiz' in your tweet.)
Soon, there might be an entire library of fun questions and answers for all to enjoy on Twitter that are easy to catalog! And who knows? Maybe some of our more engaged students, interns, and residents on social media just might remember a thing or two while contributing to the fun.
-Wes
I was fortunate to be the lucky guy to teach them that day. I have always enjoyed this opportunity and generally the lectures seem to be well-received and attended. This was lecture toward the latter part of the year, so things were not the chip-shot tracings that most learn in ACLS. Still, we always harken back to the fundamentals of reading tracings to help us understand new concepts, but I encountered a strange silence when I discussed the EKG's of patients with pacemakers:
"We all hear the phrase "He's got a DDD pacemaker," right?
They all uniformly nodded they'd heard the phrase, so I asked further:
"What do the letters in the term 'DDD pacemaker' mean?"
Silence overcame the room.
Perhaps I had caught them off guard. Many of their eyes fell to the floor. Some smiled but failed to answer. Some were clearly unnerved by the question as they shifted in their seats. A cough could be heard in the corner - it might as well have been a pin dropping. In the back right-hand corner a pager sounded. Everyone turned to the lucky contestant who was saved by the beep. Finally, somewhere toward the opposite corner of the room came a faint suggestion:
"Isn't one of them mean which chamber is paced?"
Relieved, you could see a few heads nodding now.
"Which letter of the three represents that?"
Again, the room fell silent.
Needless to say, we moved on from there after a quick basic review of pacing terminology, but his got me thinking: where have we failed to teach our medical students and residents such fairly basic clinical concepts and vernacular we use every day? Are we spending too much time on the Krebs cycle and not enough time on clinically relevant concepts in medical school and internship? How do we get them to remember?
So I had an idea: what if I used social media?
We all know that every medical student and resident (and doctor and patient, for that matter) has a cell phone. Might we use Twitter to try to teach small snippets of information to our trainees? Obviously they would have to have a Twitter account. Also, not all concepts lend themselves to this appraoch very well, but it might be worth a trial.
Soooooo, look for an occassional Electrophysiology Quiz via Twitter from yours truly. (Others with ideas for ultra-short cardiac electrophysiology quizes are welcome to join in the fun, just use the hashtag '#epquiz' in your tweet.)
Soon, there might be an entire library of fun questions and answers for all to enjoy on Twitter that are easy to catalog! And who knows? Maybe some of our more engaged students, interns, and residents on social media just might remember a thing or two while contributing to the fun.
-Wes
Sunday, January 16, 2011
First Diagnosis
They lived in a high-rise apartment complex - five stories - maybe 40 apartments in all. It was neatly kept, had a functional elevator, but was hardly a place you'd want to bring your mother to view. Probably the best word for it: functional. But he didn't care - he was a first year medical student. One bedroom, bath, kitchenette, 5th floor. "Penthouse suite," he'd call it.
He rarely interacted with his neighbors, except to exchange a courteous "Good morning" with them as he closed his door to attend the morning's lecture or perhaps an occasional "'night" as he unlocked his door upon returning home. But she lived three doors down - a charmer, frail, maybe eighty, wearing galoshes, and a hint of a flowered skirt beneath her undersized long winter coat. "Nice to have a 'doctor' on the floor," she beamed as she fumbled for her keys.
"Not quite yet," he'd say in return, but she never heard him. Hearing aides, schmearing aides. Damned if she'd ever wear them.
And so it went: a rare exchange of pleasantries, but not much more. Human anatomy, cytology, and human physiology were really what mattered to him at the moment. School was all consuming and he was doing well this first semester. The formula he had imagined to become a doctor was founded on an unswerving work ethic that he'd learned though college and studying for the MCAT's: read, memorize, regurgitate. Read, memorize, regurgitate.
Nothing to it.
Lather, rinse, repeat.
To her, she was focused on her son. He was moving in with her. "He needs a place to stay," she'd tell him. "Lost his job." And so, the groceries in her pull cart were unusually heavy this day as the student arrived home. She asked for help, and he obliged.
Her apartment was like his, but filled with pictures - some adorning the wall, some of the hall table, most on the refrigerator. A black and white with a young couple at the wedding. "Was that your husband?" "Yes," she replied, "... died of cancer of the stomach." He wished he knew more about cancer of the stomach, but said "I'm sorry" instead. And there, on the refrigerator was the picture of a massive man hugging to her frail body. "That's Tommy, my son," as she pointed to the picture. "He's all I've got now. It'll be good to have him home from the hospital."
"Hospital?"
"Well, not really a hospital, rehab. He's got's lots of problems, but his biggest one is drinking. He's had a tough go. Diabetes. Sleep apnea. You know." He really didn't know, but they made short work of emptying the grocery bags. "Thanks so much for your help."
He returned to his apartment down the hall and was glad he still had time to study for there seemed to be no end to the things he didn't know about. "How am I going to learn about all of this?" he wondered.
Weeks passed and the student caught glimpses of the large man. Simply put, he was huge, particularly when you compared him to her. But he was seen helping her with the even larger load of groceries and soft drinks on more than one occasion. The hallway was always the place for pleasantries, after all. Only later, behind closed doors, did he occasionally hear the shouting: "You've got to get help!" she'd plea. "I'm not giving you more money, dammit." Another expletive, a slammed door, then the elevator arriving to usher someone downstairs. A few hours later: pounding on the door, "I'm sorry, Ma. You gotta let me in." The door would creak open, then close.
And so it went. Her game face would be on each time she saw her 'doctor' in the hall. A gentle smile, a tacit signal that she was okay. He was too shy, too ignorant, too embarrassed to inquire about how it was going. He knew. "Good night," he'd say.
Until the day the medical student made his first diagnosis.
The early morning pounding at the door, the panicked face, the tears, the "Please come, quick!", the terror, "I've called 911," were not there in his textbooks.
Nor was the pallid face, the glassy half-opened eyes staring up, the crimson under-surface of his shirtless chest.
"My God! He'd been out most of the night, " she explained. "Just laid on the floor in the back hall and said he was exhausted. Wanted some breakfast. Didn't think about it... I kept cooking. The stove fan. I never heard him. We were out of eggs, so I went to get some. I came back and I called to him, he didn't answer."
She stopped and turned to the young doctor-to-be, searching his face, tears flowing, "Is he.... is he... ", her voice cracked, "... dead?"
He didn't have the heart to tell her he'd never seen someone dead before. How do you do this? Breathing? None. He sure looks dead. He went to his side and checked for a pulse. That cool, unmistakable almost gray-white skin had none and highlighted the coal-black widely dilated pupils that didn't move. He remembered the term "livor mortis" and returned to her quivering frame. An ambulance could be heard in the distance coming closer. Time stopped for a minute and he cupped her head gently against his shoulder as he whispered in her ear.
"Yes."
She knew, but she needed to hear it from someone else. She looked up from his shoulder at her son as she regained her composure and used her bent fingers to wipe away the tears from her cheek.
"Maybe now Tommy can rest in peace. Thank you, doctor."
-Wes
He rarely interacted with his neighbors, except to exchange a courteous "Good morning" with them as he closed his door to attend the morning's lecture or perhaps an occasional "'night" as he unlocked his door upon returning home. But she lived three doors down - a charmer, frail, maybe eighty, wearing galoshes, and a hint of a flowered skirt beneath her undersized long winter coat. "Nice to have a 'doctor' on the floor," she beamed as she fumbled for her keys.
"Not quite yet," he'd say in return, but she never heard him. Hearing aides, schmearing aides. Damned if she'd ever wear them.
And so it went: a rare exchange of pleasantries, but not much more. Human anatomy, cytology, and human physiology were really what mattered to him at the moment. School was all consuming and he was doing well this first semester. The formula he had imagined to become a doctor was founded on an unswerving work ethic that he'd learned though college and studying for the MCAT's: read, memorize, regurgitate. Read, memorize, regurgitate.
Nothing to it.
Lather, rinse, repeat.
To her, she was focused on her son. He was moving in with her. "He needs a place to stay," she'd tell him. "Lost his job." And so, the groceries in her pull cart were unusually heavy this day as the student arrived home. She asked for help, and he obliged.
Her apartment was like his, but filled with pictures - some adorning the wall, some of the hall table, most on the refrigerator. A black and white with a young couple at the wedding. "Was that your husband?" "Yes," she replied, "... died of cancer of the stomach." He wished he knew more about cancer of the stomach, but said "I'm sorry" instead. And there, on the refrigerator was the picture of a massive man hugging to her frail body. "That's Tommy, my son," as she pointed to the picture. "He's all I've got now. It'll be good to have him home from the hospital."
"Hospital?"
"Well, not really a hospital, rehab. He's got's lots of problems, but his biggest one is drinking. He's had a tough go. Diabetes. Sleep apnea. You know." He really didn't know, but they made short work of emptying the grocery bags. "Thanks so much for your help."
He returned to his apartment down the hall and was glad he still had time to study for there seemed to be no end to the things he didn't know about. "How am I going to learn about all of this?" he wondered.
Weeks passed and the student caught glimpses of the large man. Simply put, he was huge, particularly when you compared him to her. But he was seen helping her with the even larger load of groceries and soft drinks on more than one occasion. The hallway was always the place for pleasantries, after all. Only later, behind closed doors, did he occasionally hear the shouting: "You've got to get help!" she'd plea. "I'm not giving you more money, dammit." Another expletive, a slammed door, then the elevator arriving to usher someone downstairs. A few hours later: pounding on the door, "I'm sorry, Ma. You gotta let me in." The door would creak open, then close.
And so it went. Her game face would be on each time she saw her 'doctor' in the hall. A gentle smile, a tacit signal that she was okay. He was too shy, too ignorant, too embarrassed to inquire about how it was going. He knew. "Good night," he'd say.
Until the day the medical student made his first diagnosis.
The early morning pounding at the door, the panicked face, the tears, the "Please come, quick!", the terror, "I've called 911," were not there in his textbooks.
Nor was the pallid face, the glassy half-opened eyes staring up, the crimson under-surface of his shirtless chest.
"My God! He'd been out most of the night, " she explained. "Just laid on the floor in the back hall and said he was exhausted. Wanted some breakfast. Didn't think about it... I kept cooking. The stove fan. I never heard him. We were out of eggs, so I went to get some. I came back and I called to him, he didn't answer."
She stopped and turned to the young doctor-to-be, searching his face, tears flowing, "Is he.... is he... ", her voice cracked, "... dead?"
He didn't have the heart to tell her he'd never seen someone dead before. How do you do this? Breathing? None. He sure looks dead. He went to his side and checked for a pulse. That cool, unmistakable almost gray-white skin had none and highlighted the coal-black widely dilated pupils that didn't move. He remembered the term "livor mortis" and returned to her quivering frame. An ambulance could be heard in the distance coming closer. Time stopped for a minute and he cupped her head gently against his shoulder as he whispered in her ear.
"Yes."
She knew, but she needed to hear it from someone else. She looked up from his shoulder at her son as she regained her composure and used her bent fingers to wipe away the tears from her cheek.
"Maybe now Tommy can rest in peace. Thank you, doctor."
-Wes
Monday, September 20, 2010
Medicine: From Altruism to Cynicism… and Almost Back
“I’ve always wanted to help people.”
“How can the brachial plexus be exactly the same for every person?"
“Why do they put microbiology, pharmachology, and pathology in the same semester?”
“Physical diagnosis is so frickin’ cool! Look what you can see if you know what you’re looking for!”
“She didn’t want to see me; she wants to talk to the attending.”
“Why? He was so young, 2 kids, nice wife. Worse, he was my age!”
“People are idiots. He blew his whole hand off and for what?"
“What do you mean I didn’t get paid? I spent two hours with that guy!”
"I can't believe she set fire to their trailer with the baby there..."
“Since when did that ICD-9 code have to be paired with that CPT code?”
“Why is it the nurse always wakes me at 1 AM so the patient can have a sleeping pill?”
“Screw it. Tylenol, Ambien, milk of magnesia are now standard meds in my admission orders.”
“What do you mean there are no blood pressure cuffs on the wards?”
“They charged the patient how much for that surgery?”
“Stethoscopes are worthless. Get an echo.”
“With chest pain, all roads lead to cath.”
"E-mail, too?"
“Volume. Need more volume. Have you talked with PR?”
“I can't stand this EMR."
“Why aren’t we being asked to do more research for those guys?”
“It’ll be every third weekend for a while now that we’ve added another hospital to the mix.”
“Mom’s got a mass – looks like the pancreas.”
“I hear they’re doing some amazing research. And they've got a helluva surgeon.”
“I can’t believe what they can do these days. They technology is amazing.”
“Why she losing so much weight?”
“I hate that she has to run around all over the place for another appointment.”
"Here, let me help you with that door."
“I can’t believe she made it through! The team was… frankly… amazing.”
“We spent Christmas together, I'm glad we had that time together. I miss her.”
"I have no idea how I'd be able to do medicine without that EMR."
“The key is to not only look at the lines of the page that represent the heart’s activity, it’s to use deductive reasoning to make a diagnosis.”
"I've never felt so good. Thanks, doc."
“Dude, medicine is so cool.”
-Wes
“How can the brachial plexus be exactly the same for every person?"
“Why do they put microbiology, pharmachology, and pathology in the same semester?”
“Physical diagnosis is so frickin’ cool! Look what you can see if you know what you’re looking for!”
“She didn’t want to see me; she wants to talk to the attending.”
“Why? He was so young, 2 kids, nice wife. Worse, he was my age!”
“People are idiots. He blew his whole hand off and for what?"
“What do you mean I didn’t get paid? I spent two hours with that guy!”
"I can't believe she set fire to their trailer with the baby there..."
“Since when did that ICD-9 code have to be paired with that CPT code?”
“Why is it the nurse always wakes me at 1 AM so the patient can have a sleeping pill?”
“Screw it. Tylenol, Ambien, milk of magnesia are now standard meds in my admission orders.”
“What do you mean there are no blood pressure cuffs on the wards?”
“They charged the patient how much for that surgery?”
“Stethoscopes are worthless. Get an echo.”
“With chest pain, all roads lead to cath.”
"E-mail, too?"
“Volume. Need more volume. Have you talked with PR?”
“I can't stand this EMR."
“Why aren’t we being asked to do more research for those guys?”
“It’ll be every third weekend for a while now that we’ve added another hospital to the mix.”
“Mom’s got a mass – looks like the pancreas.”
“I hear they’re doing some amazing research. And they've got a helluva surgeon.”
“I can’t believe what they can do these days. They technology is amazing.”
“Why she losing so much weight?”
“I hate that she has to run around all over the place for another appointment.”
"Here, let me help you with that door."
“I can’t believe she made it through! The team was… frankly… amazing.”
“We spent Christmas together, I'm glad we had that time together. I miss her.”
"I have no idea how I'd be able to do medicine without that EMR."
“The key is to not only look at the lines of the page that represent the heart’s activity, it’s to use deductive reasoning to make a diagnosis.”
"I've never felt so good. Thanks, doc."
“Dude, medicine is so cool.”
-Wes
Wednesday, June 02, 2010
End-of-the-year Lectures

Some things never change - like sitting in the back of the lecture hall.
I just wonder if they know how good they've got it.
-Wes
Monday, August 10, 2009
The Med Student's Pockets: Then and Now
In case you've forgotten what medical students' pockets looked like:
This was then:

And this is now:

-Wes
This was then:

And this is now:

-Wes
Metamorphosis
It’s the kind of thing you don’t expect.
It starts with a bit of reluctance, peppered with a reservation, knowing that things will take a bit longer this day.
And there you are, contemplating the day ahead, when a soft voice interrupts the reverie:
“Uh, are you Dr. Fisher?”
You turn and see not a colleague, but a stranger, a young stranger much more fit than you, smiling. You admire the crispness of their lab coat, the gleam in their eye, the enthusiasm that seems to exude from their pores. Not that anything has happened, mind you, but still, for a brief moment, you see yourself in the same place many years ago. Eager, anxious, awestruck and clueless, all blended together in a complicated emotional goulash.
Years ago it was you, entering a different lab. You knew no one, knew nothing and barely had an idea how to tie a facemask so your chin was not permanently touching your chest. Surrounded by instruments and tech-speak you watched. You had no idea how in the hell you’d ever be able to do this, but never dared to admit it.
But time passed.
Slowly, gradually, carefully, your mentor introduced you to your new home away from home. See one, do one. Bit by tiny bit. Hundreds of hours, thousands of anecdotes. Each meant to shape you, scare you, and guide you. “Here, feel what 1500 psi feel like in your hand” as the pigtail spewed contrast in my palm. “How many cc’s are in that catheter?” “This is the image intensifier.” “Gotta hold longer.” Tons of iterations, plenty of mistakes. “It’s okay to make a mistake once,” they’d say, “but not twice.” Papers. Research. Presentations. Fewer inefficiencies. You taught the first- and second-years, but still were the student.
And then they said you were done.
But you quickly realized you hadn’t even started. Going alone is different. Very different. So you learned some more. You kept watching, absorbing, getting faster, safer, yet always losing sleep over tough cases. Again and again and again. Soon you realize you're growing weary, growing old.
Until in the din of a back room a fresh face walks in and asks who you are.
And suddenly you realize it's good to slow down again, if for just a moment, since the student is the teacher in more ways than one.
It starts with a bit of reluctance, peppered with a reservation, knowing that things will take a bit longer this day.
And there you are, contemplating the day ahead, when a soft voice interrupts the reverie:
“Uh, are you Dr. Fisher?”
You turn and see not a colleague, but a stranger, a young stranger much more fit than you, smiling. You admire the crispness of their lab coat, the gleam in their eye, the enthusiasm that seems to exude from their pores. Not that anything has happened, mind you, but still, for a brief moment, you see yourself in the same place many years ago. Eager, anxious, awestruck and clueless, all blended together in a complicated emotional goulash.
Years ago it was you, entering a different lab. You knew no one, knew nothing and barely had an idea how to tie a facemask so your chin was not permanently touching your chest. Surrounded by instruments and tech-speak you watched. You had no idea how in the hell you’d ever be able to do this, but never dared to admit it.
But time passed.
Slowly, gradually, carefully, your mentor introduced you to your new home away from home. See one, do one. Bit by tiny bit. Hundreds of hours, thousands of anecdotes. Each meant to shape you, scare you, and guide you. “Here, feel what 1500 psi feel like in your hand” as the pigtail spewed contrast in my palm. “How many cc’s are in that catheter?” “This is the image intensifier.” “Gotta hold longer.” Tons of iterations, plenty of mistakes. “It’s okay to make a mistake once,” they’d say, “but not twice.” Papers. Research. Presentations. Fewer inefficiencies. You taught the first- and second-years, but still were the student.
And then they said you were done.
But you quickly realized you hadn’t even started. Going alone is different. Very different. So you learned some more. You kept watching, absorbing, getting faster, safer, yet always losing sleep over tough cases. Again and again and again. Soon you realize you're growing weary, growing old.
Until in the din of a back room a fresh face walks in and asks who you are.
And suddenly you realize it's good to slow down again, if for just a moment, since the student is the teacher in more ways than one.
Monday, April 13, 2009
EchoJournal Launched
Call it YouTube for echocardiography. The guys over a Medgadget have launched EchoJournal:
I wish I had thought of that.
-Wes
PS: I'd be careful to make sure patient identifiers are removed from video loops before uploading, however.
It is a video site, designed to present transthoracic and transesophageal loops for discussion and storage. EchoJournal combines many of the features familiar to users of other video sharing sites, including easy uploading, comments and discussions, and the ability to create communities for your academic department, professional group, or school. The site will be curated by David E. Winchester, MD, a Cardiology Fellow at the University of Florida, who has already uploaded tons of interesting cases, and is ready for many more.Great idea.
I wish I had thought of that.
-Wes
PS: I'd be careful to make sure patient identifiers are removed from video loops before uploading, however.
Monday, July 28, 2008
Making 'Em Look Good
It’s the beginning of the academic medical school year, and a new flock of energetic medical students has arrived. It is evident as they eagerly call the attending to “notify” them of a sick case that was “coming to the ward” having never seen the patient.
It was no biggie, this time. Things were handled. But it was clear during the late-night phone conversation that the medical student hadn’t seen the patient, wasn’t aware of the entire medical history, and was sent as the “messenger.”
Well, we don’t shoot the messenger.
But there’s also an important principle that should be followed when communicating with different members of the medical team involved in a patient’s care:
Make ‘em look good.
If you are a medical student, make your resident look good on rounds. Know the history, medications, lab results, and the patient’s chief complaint that day. If you do, he’ll make sure you look good.
If you’re a resident, make your fellow look good on rounds. Teach the students. Check the patient yourself if needed. Give the fellow the pertinent items to be addressed that day, and make sure they happen. If you do, your fellow will make you look good.
If you’re a fellow, make your attending look good on rounds. Guide the resident. Come prepared, having communicated with the team, understand the next plan of action, and implement it. If you do, your attending will make you look good.
If you’re an attending, make sure the nurse looks good. Point out the good things he or she did overnight, guide them on the items that need attention, and listen to their concerns. If you do, your nurse will make you look good.
If you’re a nurse, make sure the patient looks good. Respond to their calls, check the medications not once but twice, ask why the dinner tray arrived late, and help brush the patient's hair and teeth. If you do, the patient will make sure the whole hospital looks good.
Simple, effective.
That’s the way it works.
Best of luck to all of you.
-Wes
It was no biggie, this time. Things were handled. But it was clear during the late-night phone conversation that the medical student hadn’t seen the patient, wasn’t aware of the entire medical history, and was sent as the “messenger.”
Well, we don’t shoot the messenger.
But there’s also an important principle that should be followed when communicating with different members of the medical team involved in a patient’s care:
Make ‘em look good.
If you are a medical student, make your resident look good on rounds. Know the history, medications, lab results, and the patient’s chief complaint that day. If you do, he’ll make sure you look good.
If you’re a resident, make your fellow look good on rounds. Teach the students. Check the patient yourself if needed. Give the fellow the pertinent items to be addressed that day, and make sure they happen. If you do, your fellow will make you look good.
If you’re a fellow, make your attending look good on rounds. Guide the resident. Come prepared, having communicated with the team, understand the next plan of action, and implement it. If you do, your attending will make you look good.
If you’re an attending, make sure the nurse looks good. Point out the good things he or she did overnight, guide them on the items that need attention, and listen to their concerns. If you do, your nurse will make you look good.
If you’re a nurse, make sure the patient looks good. Respond to their calls, check the medications not once but twice, ask why the dinner tray arrived late, and help brush the patient's hair and teeth. If you do, the patient will make sure the whole hospital looks good.
Simple, effective.
That’s the way it works.
Best of luck to all of you.
-Wes
Thursday, July 24, 2008
Change of Shift is Up With Great Content
Kim over at Emergiblog once again hosts Change of Shift - the best of the nursing blog-o-sphere this week. In it, I found this hilarious depiction of a German doctor's clever way to dance his way in to teaching arrhythmias. Be sure to check out atrial fibrillation and the successful defibrillation:
Enjoy!
-Wes
Enjoy!
-Wes
Friday, July 11, 2008
Medical Instruction: Dying on the Vine
It's happening more and more:
Then, after being slapped by residency-review committees about their deficiencies and threatened with a sudden drop in federally-mandated funds for teaching, hospitals jump to action:
-Wes
The program to train cardiologists at Los Angeles County-USC Medical Center has been stripped of its national accreditation by the Accreditation Council for Graduate Medical Education. The decision marks the first time a residency or fellowship program at the facility has lost accreditation. The council faulted the program for "insufficient teaching time by the faculty."It's really not unexpected, though. Clinical faculty at medical schools are increasingly pressured to maintain "productivity" standards based on Medicare's RVU system, while rarely being compensated for the time spent teaching students. As a result, training programs suffer.
Then, after being slapped by residency-review committees about their deficiencies and threatened with a sudden drop in federally-mandated funds for teaching, hospitals jump to action:
County-USC hopes to fix the problems and have the 21-year-old cardiology program recertified before June 30, 2009, when the accreditation is to be withdrawn.Teaching subsidies must flow more consistently to the people doing the teaching and not to support the training program "overhead:"
A main argument for reducing IME payments is supported by data demonstrating that teaching hospitals have substantially higher margins on their Medicare business than other hospitals. In 1999, inpatient Medicare margins for all hospitals were, on average, 11.9 percent. For major teaching hospitals this figure was 22.3 percent versus 11.6 percent for other teaching hospitals, and 6.5 percent for non-teaching hospitals.Only when such transparency is evident to the instructors will there be a long-term incentive to maintain most clinical training programs.
Finally, some point out that the logic of providing support for the social mission of teaching hospitals under Medicare IME is not rational, and that it is a "disguised" payment that should be more transparent. This argument suggests that these types of payment mechanisms provide little accountability for the funds provided for the social missions of teaching hospitals.
-Wes
Wednesday, April 30, 2008
Where Have All The Residents Gone?
Last night - a code - complete heart block. I was called it to place a temporary pacing wire in the ICU. Little time. Stress. Need to prepare the field. Gloves, does anyone have gloves? Could we prep the area? You have the central line kit? Could I get another set of hands?
Then I realized something. The residents who had so carefully run the initial code and get the patient to the ICU had vanished. Why? Don't they want to learn how to start a central line, or at least see one placed? Where are they?
After the dust settled, I came to realize what had happened.
So to them and the medical teachers everywhere, I dedicate my parody of Pete Seeger and Joe Hickerson's "Where Have All the Flowers Gone" popularized by Peter, Paul and Mary and Joan Baez:
Where Have All the Residents Gone?
Where have all the residents gone, long time passing?
Where have all the residents gone, long time ago?
Where have all the residents gone?
They’ve gone to the keyboards everyone.
When will they ever learn?
When will they ever learn?
Where have all the keyboards gone, long time passing?
Where have all the keyboards gone, long time ago?
Where have all the keyboards gone?
They’re now in the hospitals everyone.
When will they ever learn?
When will they ever learn?
Where have all the hospitals gone, long time passing?
Where have all the hospitals gone, long time ago?
Where have all the hospitals gone?
They’ve gone to the hospitalists, everyone.
When will they ever learn?
When will they ever learn?
Where have all the hospitalists gone, long time passing?
Where have all the hospitalists gone, long time ago?
Where have all the hospitalists gone?
Consulting the specialists, everyone.
When will they ever learn?
When will they ever learn?
Where have all the specialists gone, long time passing?
Where have all the specialists gone, long time ago.
Where have all the specialists gone?
They’re planning retirement, everyone.
When will they ever learn?
When will they ever learn?
Where have all the retirees gone, long time passing?
Where have all the retirees gone, long time ago?
Where have all the retirees gone?
They’re treated by residents, everyone.
When will they ever learn?
When will they ever learn?
-Wes
Then I realized something. The residents who had so carefully run the initial code and get the patient to the ICU had vanished. Why? Don't they want to learn how to start a central line, or at least see one placed? Where are they?
After the dust settled, I came to realize what had happened.
So to them and the medical teachers everywhere, I dedicate my parody of Pete Seeger and Joe Hickerson's "Where Have All the Flowers Gone" popularized by Peter, Paul and Mary and Joan Baez:
Where have all the residents gone, long time passing?
Where have all the residents gone, long time ago?
Where have all the residents gone?
They’ve gone to the keyboards everyone.
When will they ever learn?
When will they ever learn?
Where have all the keyboards gone, long time passing?
Where have all the keyboards gone, long time ago?
Where have all the keyboards gone?
They’re now in the hospitals everyone.
When will they ever learn?
When will they ever learn?
Where have all the hospitals gone, long time passing?
Where have all the hospitals gone, long time ago?
Where have all the hospitals gone?
They’ve gone to the hospitalists, everyone.
When will they ever learn?
When will they ever learn?
Where have all the hospitalists gone, long time passing?
Where have all the hospitalists gone, long time ago?
Where have all the hospitalists gone?
Consulting the specialists, everyone.
When will they ever learn?
When will they ever learn?
Where have all the specialists gone, long time passing?
Where have all the specialists gone, long time ago.
Where have all the specialists gone?
They’re planning retirement, everyone.
When will they ever learn?
When will they ever learn?
Where have all the retirees gone, long time passing?
Where have all the retirees gone, long time ago?
Where have all the retirees gone?
They’re treated by residents, everyone.
When will they ever learn?
When will they ever learn?
-Wes
Subscribe to:
Comments (Atom)