At first with the beta release of the device it just so cool to see your EKG in real time: just tap the app, put your hands in the device's over-sized electrodes on the specialized iPhone case and *bam* there it was - your heart's realtime EKG displayed right before your eyes.
Then a new software upgrade to the app came quite a bit later after the device's FDA approval. You had to enter a name before the app would proceed to the EKG screen.
Okay, makes sense. Don't want to confuse data.
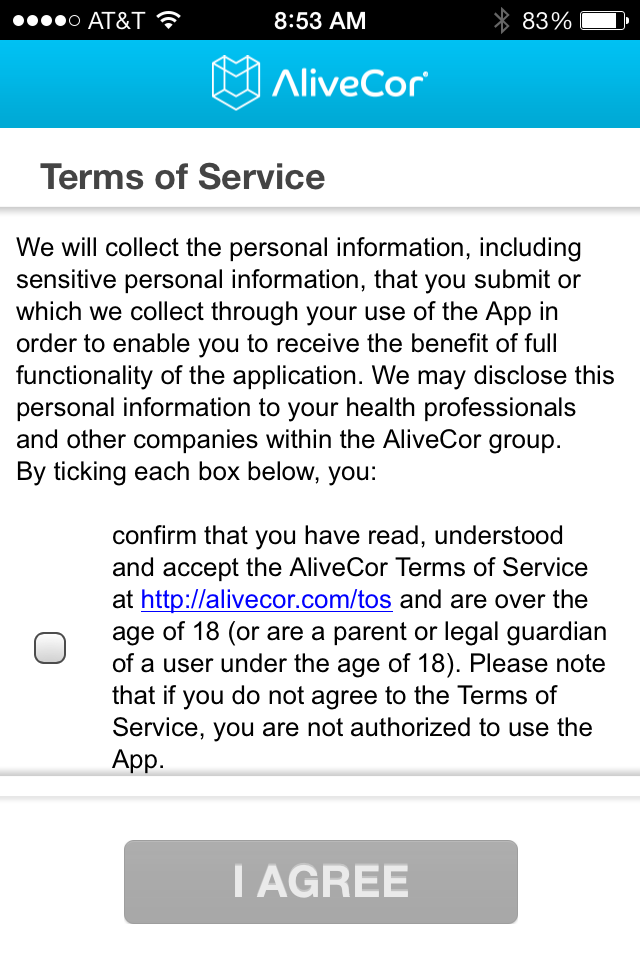 | ||
| Screenshot of Alivecor EKG app software (click image to enlarge) |
Welcome to the mobile health care privacy surrender. After all, these days if it's mobile, it's Big Data.
We've seen it with Google tracking their customers. We've seen it with Apple's Terms of Service agreement, too. And just like the big internet giants, the money in medical apps is not the app, but the data they produce. Alivecor has to develop a business model and nowhere in the world is there bigger business than health data, especially your personal data.
My purpose here is not to bash Alivecor. On the contrary, I think they are leaders in moving forward in the mobile health care app arena that might be a viable business entity. But I think patients should be aware of what we're surrendering each time we use any health care app that deals with anything medical and click "I Agree" to the app's broad "Terms of Service" that surrenders one's "sensitive personal information."
Perhaps people won't care about their privacy any more. Perhaps so much about us is already available on the internet, that we've already unwittingly surrendered our souls. We want our iPhone or Galaxy visuals and we want them now. So we agree. But given the implications of what this might mean to a future insurance premiums or health care marketing tactics, shouldn't we at least wonder?
One of the most important abstracts at the recent American Heart Association this year was this little gem entitled "Do ICDs Prevent Hip Fractures or Are Physicians Selecting Appropriate Candidates for ICDs?" (thanks to John Mandrola MD, for pointing me to this). The abstract underscores the pitfalls of observational comparative effectiveness research - the cornerstone for the latest internet promise of Big Data. Believe it or not, correlation does not equal causation.
And yet increasingly we see Big Data analysis revered and marketed as scientific gospel. Even our own FDA has used bench data over clinical data to specify pill dosages using this extrapolation, for instance.
Big data is becoming a means to justify the ends.
Think about that the next time you click on "I agree" and then see next month's higher insurance premium.
-Wes





{kind=link}