One cardiologist's epiphany.
-Wes
h/t: The Carlat Psychiatry Blog.
Thursday, April 30, 2009
Art in Medicine
Any idea what this is?

-Wes
Answer if you must (spelled backwards): "tneduts lacidem a fo deaH" s'ossaciP olbaP

-Wes
Answer if you must (spelled backwards): "tneduts lacidem a fo deaH" s'ossaciP olbaP
Let This Be Proof
It's been a constant battle in our household between my brother, a neurosurgeon, and me: which is the more important organ, the heart or the brain?
My brother feels the heart is there to nurture the brain. I argue the heart really doesn't need the brain to function for goodness sake, and therefore, due to it's independence, it reigns supreme.
Brotherly love, right?
Thankfully, the folks at Street Anatomy have provided me with the proof I need to settle the score with my brother. It's a piece of contemporary art entitled "Being 20."
So here, bro. This one's for you:

-Wes
My brother feels the heart is there to nurture the brain. I argue the heart really doesn't need the brain to function for goodness sake, and therefore, due to it's independence, it reigns supreme.
Brotherly love, right?
Thankfully, the folks at Street Anatomy have provided me with the proof I need to settle the score with my brother. It's a piece of contemporary art entitled "Being 20."
So here, bro. This one's for you:

-Wes
Wednesday, April 29, 2009
What the President Could Have Done With Photoshop
Think of the money he could have saved:
And to think their griping over doctors getting pens from pharmaceutical companies...
-Wes
h/t: Instapundit.
"I am a graphic designer in Southern California. I spent ten minutes throwing this together this morning, which at my rates equals about 15 dollars. However, I will settle for the thanks of a grateful nation."Compare that to the fuel costs to fill AirForce One and an F-16 fighter for a few hours.
And to think their griping over doctors getting pens from pharmaceutical companies...
-Wes
h/t: Instapundit.
Tuesday, April 28, 2009
17 Pacemakers
Pretty impressive:
His film reminds me of a similar chest x-ray from a former patient who quietly called himself "The Junkyard Dog." Fortunately for this patient, no one will ever know what's inside him - at least until they see his xray...
-Wes
The 17th was implanted March 11 at the Pacemaker and Defibrillator Center at the Saint Barnabas Heart Center at Newark Beth Israel Medical Center.Too bad the picture accompanying the article actually shows him holding biventricular defibrillator, rather than a pacemaker as labeled. His chest xray (seen in the article), although tough to see, shows one left ventricular lead, one right ventricular defibrillator leads, three right ventricular pacing leads and two atrial leads, one of which that has been partially withdrawn to the junction of the right subclavian/superior vena cava junction.
In some ways, Concepcion said he viewed himself as guinea pig growing up, when electrical wires in his chest malfunctioned or battery cells became weak and run down. He was in and out of the hospital every two years, sometimes more frequently, getting outfitted for pacemakers since he was 2 years old.
In the beginning, they weren't built to last long, especially for someone as young as Concepcion. He likes to think he burned them out as a kid, but Concepcion was learning something even more valuable. Each time he was hospitalized in Newark, Concepcion gradually became a part of history for having grown up with the development and evolution of the device.
His film reminds me of a similar chest x-ray from a former patient who quietly called himself "The Junkyard Dog." Fortunately for this patient, no one will ever know what's inside him - at least until they see his xray...
-Wes
Crossroads
 It was a case like so many others, an elderly man who tripped and broke his hip. During his physical examination, a soft murmur was heard so an echocardiogram was ordered. His heart muscle was quite weakened. Cardiologists were contacted, symptoms reviewed, electrocardiograms compared, and soon he was off to surgery to fix his hip.
It was a case like so many others, an elderly man who tripped and broke his hip. During his physical examination, a soft murmur was heard so an echocardiogram was ordered. His heart muscle was quite weakened. Cardiologists were contacted, symptoms reviewed, electrocardiograms compared, and soon he was off to surgery to fix his hip. Rehabilitation was remarkably fruitful – he was weight-bearing quickly and some five days later, he was looking strong enough to consider discharging, shuffling, walker assisted gait and all.
But an abnormality was found before his surgery that must be addressed – to do otherwise would not comply with guidelines for his management: his weaken heart. Mind you he was 78, had been declining physically and mentally over the past several years and did not lose consciousness with this hip fracture, but he was loved by his wife and daughter who were eager see him continue to improve. The hope, if you will, of a better time ahead.
What is a doctor to do in this instance?
From the earliest years, the discipline of medicine requires rigorous study and exhaustive hours of training. By and large, physicians are driven souls, vetted carefully from our formative years of school by exemplary grades, grueling study, competition for residencies, and taxing selection processes. Those that push the norm, strive for excellence, and go above and beyond excel, those that do not, wither. In essence, it’s the epitome of Darwinian selection.
The trend continues when one enters practice as a young doctor. It is, in short, all about productivity: productivity academically, productivity clinically, and productivity economically. That’s the way the ball currently rolls in medicine. And really, that’s the way the patients have benefited in our system, too. Going the extra mile, even when hope seems impossible or the hour is inconvenient has benefited many, many people.
But we are at a critical crossroad in medicine today. Forces are masterfully aligned to impose restrictions or recommendations of care upon the doctor-patient relationship. Just like the patient above who has never had an arrhythmia but has a known weakened heart muscle detected anecdotally after an unrelated fall. Do we treat him, because we “should,” based on guidelines that others in positions of “authority” have vetted and our practice managers have urged, or turn a cheek on our obsessive reliance on “evidence” in favor of “art,” realizing that doing so directly threatens the core of our economic, academic, and clinical productivity-based health care model and exposes us legally?
The only logical resolution to this dilemma is for the doctor is to turn to their patients. But will patients or their families accept anything less than doing everything, just for the common good of the system? Will careful discussion about costs and absolute (rather than relative) risk reduction with preventative measures perceived as responsible or lackadaisical? Can we afford to withhold therapy when our economic survival continually demands more volume, more procedures, and more patients in the system? What incentives exist for doctors to do nothing in the circumstance I have described?
Given the economic, legal, and professional climate in vogue today, there are none. As a new public health care plan is deployed, will we ever be able to achieve cost control in our new system?
At present, it seems unlikely. We have gravitated to models and systems that automate our profound inefficiencies and deem them “highly efficient.” We advertise to load the system more. We leave the cost of the defense of the wrongfully accused to the defendant rather than the plaintiff. All while costs, and volumes, and regulatory infrastructure spiral. Without incentives that reward doing less for both the doctor and the patient, we won’t see any meaningful reduction to health care costs in America irrespective of the ultimate system deployed.
-Wes
Monday, April 27, 2009
Murder She Wrote Part #2: A Heart-Stopping Story
By now it's old news (at least as far as the internet goes). But cutting a pacemaker from someone's chest is no easy feat, especially when a pen knife is used. That's because the pacemaker generator and leads become encased in a fibrous shell that firmly anchors the device in place. This fibrous shell begins to take shape shortly after the pacemaker implant as the body works to isolate the foreign body from the surrounding tissues. The the formation of the typically shimmering scar-like pocket occurs over several months time. When devices are not touched for years, the pocket can even become calcified: a so-called "porcelain pocket" that can be particularly challenging to remove the device when battery changes are needed.
Although I have no idea how long the father's pacemaker had been implanted in this case, I can vouch that its removal late after implant would take considerable effort.
I can only hope he was not successful.
-Wes
Although I have no idea how long the father's pacemaker had been implanted in this case, I can vouch that its removal late after implant would take considerable effort.
I can only hope he was not successful.
-Wes
On Over-priced Specialists
There's a primary care physician (not "provider") shortage.
Yep.
They are underpaid.
Yep.
We should redistribute money from the "rich" specialists and give it to the primary care doctors.
This is being proposed.
Here are some considerations:
#1) Medicare costs are derived from two locations, a doctors fee and a "technical fee." Some examples (estimates only):
A left heart catheterization:
But there will be repercussions with reduced access to specialists. (Funny how we never hear about technical component cuts, but then again, they've got more lobbyists...)
#2) What happens when we pour in more primary care doctors (as is being proposed)?
More primary care doctors find more disease: good for specialists.
More primary care doctors that are paid better find primary care attractive stay in primary care: good for specialists.
More primary care doctors which cost more, both to primary care and to specialists: bad for sustainable model of health care delivery.
Unless, of course, people realize we'll have to eat our spinach and ration the care delivered.
-Wes
Yep.
They are underpaid.
Yep.
We should redistribute money from the "rich" specialists and give it to the primary care doctors.
This is being proposed.
Here are some considerations:
#1) Medicare costs are derived from two locations, a doctors fee and a "technical fee." Some examples (estimates only):
A left heart catheterization:
Doctor fee: $270Open heart surgery:
Hospital fee: $1250
Doctor fee: $2000So, by all means, cut the specialists' portion of the fees to save costs, okay?
Hospital fee: $20,000
But there will be repercussions with reduced access to specialists. (Funny how we never hear about technical component cuts, but then again, they've got more lobbyists...)
#2) What happens when we pour in more primary care doctors (as is being proposed)?
More primary care doctors find more disease: good for specialists.
More primary care doctors that are paid better find primary care attractive stay in primary care: good for specialists.
More primary care doctors which cost more, both to primary care and to specialists: bad for sustainable model of health care delivery.
Unless, of course, people realize we'll have to eat our spinach and ration the care delivered.
-Wes
Saturday, April 25, 2009
Mr. Rogers Does Health Care Reform

Good morning boys and girls. It's so nice to see you again. Yesterday, I enjoyed our show where we learned about a new term called "conflicts of interest" that doctors always seem to have with companies that fund their research. Can you say "conflicts of interest?" Why, that's a very big-boy-and-girl thing to say, isn't it?
It's a beautiful day in this neighborhood
A beautiful day for a neighbor
Would you be mine?
Could you be mine?
 (He hangs his coat in a closet, puts on a cardigan zipper sweater, and removes his dress shoes to put on sneakers, all the while smiling)
(He hangs his coat in a closet, puts on a cardigan zipper sweater, and removes his dress shoes to put on sneakers, all the while smiling)Well, on today's show, we're going to meet our friends who are helping us with health care reform. (stops, pauses) Can you say "Health Care Reform?" Sure. Health - Care - Reform. So let's head over to the Neighborhood of Make-Believe today and see what's happening. Mr. Conductor, can you take us there?
(Camera zooms to a small red electric trolley and follows it through a tunnel... *Ding ding* *ding ding*) The scene magically transforms to world like none other, where birds are chirping and the sun always shines: the Neighborhood of Make-Believe.)
 Look who's here! Why it's Mr. McFeely! My, you looks like you've been busy! What are all those letters you're delivering there?
Look who's here! Why it's Mr. McFeely! My, you looks like you've been busy! What are all those letters you're delivering there? Hi, Mr. Rogers! Why, there's a big meeting going on now to help make health care here in the Neighborhood of Make-Believe.
 Gosh, Mr. McFeely. That bag looks so heavy. Why so many letters? Can I help carry it? Are there so many letters because they need more money?Oh, no, Mr. Rogers! Everyone knows pay-to-play only happens in Illinois. That would never happen here in the Neighborhood of Make-Believe. We just want to get everyone's input so we can involve all the stakeholders in the health care reform debate. That way, we know we'll find the right solution and no one will complain about the new plan. Isn't it exciting! But the organizers have to act fast. Grandpere is sick and they want to make sure they get a solution hammered out right away so he'll be able to get coverage if he needs it.Goodness, Mr. McFeely! I understand. That sounds very important. I was wondering if you could help me. I'm looking for conflict of interests here in the Neighborhood of Make-Believe.Sure! Maybe King Friday XIII would know where to find them. Perhaps I could take you to his castle?Gee, Mr. McFeely, that would be swell!
Gosh, Mr. McFeely. That bag looks so heavy. Why so many letters? Can I help carry it? Are there so many letters because they need more money?Oh, no, Mr. Rogers! Everyone knows pay-to-play only happens in Illinois. That would never happen here in the Neighborhood of Make-Believe. We just want to get everyone's input so we can involve all the stakeholders in the health care reform debate. That way, we know we'll find the right solution and no one will complain about the new plan. Isn't it exciting! But the organizers have to act fast. Grandpere is sick and they want to make sure they get a solution hammered out right away so he'll be able to get coverage if he needs it.Goodness, Mr. McFeely! I understand. That sounds very important. I was wondering if you could help me. I'm looking for conflict of interests here in the Neighborhood of Make-Believe.Sure! Maybe King Friday XIII would know where to find them. Perhaps I could take you to his castle?Gee, Mr. McFeely, that would be swell!(camera cuts to a castle where King Friday XIII is meeting with Queen Sara Saturday, Prince Tuesday, Lady Elaine Fairchild, and Daniel Striped Tiger are speaking in hushed tones. King Friday XIII sees them approach.)
 Mr. Rogers, I presume?Correct as always, Your Majesty, King Friday.What brings you to the Neighborhood of Make-Believe? Can't you see we're very busy?I'm sorry King, but I'm looking for conflicts of interest.Here in the Neighborhood of Make-Believe we make sure we are all as pure as the driven snow. After all, we are concerned about the needs of everyone in our neighborhood. That's why we're meeting with everyone in town hall meetings and at Health Care Summits. People need health care and they need it now!Yes, good King. I know Dr. Frogg would want to be a health care helper, too. Is he here?Dr. Frogg and Nurse Nelly have been too busy to come, poor guys. Something about "pay-for-performance" and needing to buy a computer for something called "e-prescribing." Anyway, we'll be sure to let Dr. Frogg know what we decide. So King Friday, you've not seen any conflicts of interest?No, not here in my kingdom!And Queen Sara Saturday, have you seen any conflicts of interest?
Mr. Rogers, I presume?Correct as always, Your Majesty, King Friday.What brings you to the Neighborhood of Make-Believe? Can't you see we're very busy?I'm sorry King, but I'm looking for conflicts of interest.Here in the Neighborhood of Make-Believe we make sure we are all as pure as the driven snow. After all, we are concerned about the needs of everyone in our neighborhood. That's why we're meeting with everyone in town hall meetings and at Health Care Summits. People need health care and they need it now!Yes, good King. I know Dr. Frogg would want to be a health care helper, too. Is he here?Dr. Frogg and Nurse Nelly have been too busy to come, poor guys. Something about "pay-for-performance" and needing to buy a computer for something called "e-prescribing." Anyway, we'll be sure to let Dr. Frogg know what we decide. So King Friday, you've not seen any conflicts of interest?No, not here in my kingdom!And Queen Sara Saturday, have you seen any conflicts of interest? I don't think so, Mr. Rogers. But I really haven't been looking. After all, we've got other very important tasks in front of us. Like deploying electronic medical records and making sure everyone has access to pharmacies!Prince Tuesday, have you seen any conflicts of interest here in the Neighborhood of Make-Believe?
I don't think so, Mr. Rogers. But I really haven't been looking. After all, we've got other very important tasks in front of us. Like deploying electronic medical records and making sure everyone has access to pharmacies!Prince Tuesday, have you seen any conflicts of interest here in the Neighborhood of Make-Believe? No sireeee.And Daniel Striped Tiger, you have seen any either have you?
No sireeee.And Daniel Striped Tiger, you have seen any either have you? Nope. I wouldn't know what one was, Mr. Rogers.
Nope. I wouldn't know what one was, Mr. Rogers.(Turning to Mr. McFeely)
 Gosh, Mr. McFeely, what a busy day! Let's go back now. It seems the only conflicts I have found have been with the doctors working with the drug and medical device companies. So, I guess our search is finished. Thanks everyone!
Gosh, Mr. McFeely, what a busy day! Let's go back now. It seems the only conflicts I have found have been with the doctors working with the drug and medical device companies. So, I guess our search is finished. Thanks everyone!It's such a good feeling to know you're alive.-Wes
It's such a happy feeling
You're growing inside.
And when you wake up ready to say
I think I'll make a snappy new day
It's such a good feeling....
Friday, April 24, 2009
Orthopedic EMR Documentation
The orthopedic physical examination: short, sweet and nearly uninterpretable:
-Wes
Gen: NADOne would think they were on Twitter.
Incision c/d/i
Motor 5/5 pf/df/ehl
Silt @ t/s/s/sp/dp
DP/PT pulses 2+
-Wes
The Ultimate Irony: A Sick Tax to Make Health Care Affordable
Say it ain't so.
But look for cash-strapped legislatures across the country to consider this latest tactic to feed from the Medicare National Bank: in Colorado, held to lower taxes by their self-imposed "Tax Payers Bill of Rights" (or so-called TABOR law enacted in 1992), legislatures have resorted to a "sick tax" cleverly disguised as a hospital fee added without line-item status to hospital bills:
All in the name of making health care more "affordable."
Brilliant.
-Wes
h/t: Walter Olson, editor, Point of Law.
But look for cash-strapped legislatures across the country to consider this latest tactic to feed from the Medicare National Bank: in Colorado, held to lower taxes by their self-imposed "Tax Payers Bill of Rights" (or so-called TABOR law enacted in 1992), legislatures have resorted to a "sick tax" cleverly disguised as a hospital fee added without line-item status to hospital bills:
The state House has passed HB 1293, a tax on sick people. The bill directs hospitals to add a “fee” of up to 5.5 percent on every patient’s bill, keeps the fee secret by prohibiting hospitals from listing it separately, and reimburses hospitals on the basis of what they say their costs are.As Linda Goreman, director of the Health Care Policy Center for the Independence Institute, a Golden-based libertarian think tank points out (pdf):
Those supporting HB 1293 pretend that this is a fee on hospitals. They say hospitals will pay this fee, something that can be true only if hospitals have large pots of surplus funds lying around.
The ultimate irony in all this is that HB 1293’s sponsors upped the ante on their language perversion by claiming that the magic fee that increases the cost of private sector health care to the tune of $600,000,000 a year “makes health care more affordable.” They even named HB 1293 the “Colorado Healthcare Affordability Act.” For this legislature, bigger government and higher fees translates into more affordable living both for it and for its big business friends.Hey, if they can do it to our cable and phone bills, why not hospital bills, too?
If it gets rewarded for its tax into fee prestidigitation and its “affordability” act, voters should expect the future to bring such affordability measures as income taxes transmuted into job privilege fees, increased sales taxes transmuted into transactions fees, and constitutional protections transmuted into therapeutic suggestions.
All in the name of making health care more "affordable."
Brilliant.
-Wes
h/t: Walter Olson, editor, Point of Law.
Thursday, April 23, 2009
Watchman Squeeks By
Watchman, Atritech's new left atrial appendage occlusion device for the treatment of atrial fibrillation stroke risk, squeeked by the FDA's advisory panel on a 7-to-5 vote today:
-Wes
Overall, most panel members felt the sponsor showed the device to be effective, although there were caveats. Many were uncomfortable with the size of the 800-patient study. Others were uncomfortable making a decision about effectiveness with end points such as hemorrhagic stroke, which was included in the primary efficacy end point. They felt a decision on effectiveness was difficult when there were so few hemorrhagic strokes—five in the control arm and one with the Watchman device—while others thought ischemic stroke, which occurred more frequently in the device arm, would have been a more reliable end point.Whether the FDA will approve the lukewarm endorsement remains to be seen, but the first big hurdle for this device has been passed.
Regarding safety, there was also a divergence of opinion. Again, panel members were concerned about assessing the long-term safety of the data given the short-term PROTECT-AF study. Some, including Dr Michael Domanski (National Heart, Lung, and Blood Institute, Bethesda, MD), said it was pretty hard to look at the data and say the device is safe.
"I would think it would be a mistake for the FDA to approve this device," said Domanski.
Still, opinions like this were the minority, and most felt the "devastating" effects of warfarin over time need to be balanced with the increased risks with the device, such as pericardial effusion, device embolization, and thrombus formation on the device. In contrast, warfarin is a lifetime drug that can be difficult to manage, especially in the elderly and frail, many panel members felt.
-Wes
How to Determine a Doctor's Specialty
Want to know what specialty a doctor practices? Just ask that doctor what time their first meeting of the day begins. While not always perfect, it's usually quite telling.
Here's how things play out at our institution:
Here's how things play out at our institution:
If the first morning meeting starts at 06:30 AM - it must be orthopedic surgeons.-Wes
If the first morning meeting starts at 07:00 AM, it must be general surgeons.
If the first morning meeting starts at 07:30 AM, it must be internists.
If the first morning meeting starts at 08:00 AM, it's usually just administrators.
Wednesday, April 22, 2009
iElectrophysiology on the iPhone
iThink iT's iNevitable that iElectrophysiology Apps will iNvade the iPhone:
-Wes
Some companies, such as Toumaz.com, are building tiny sensors priced at $10-20 that you can use to track your vitals such as heart rate, and which could be easily connected to a smartphone. A stealthy company called Adigy is working on something similar, but they’ve yet to build a mobile app. Cardionet, of San Diego, is one of the bigger players doing heart rate and rhythm wireless monitoring and says it is building a mobile application. Triage Wireless, backed by Qualcomm Ventures, is one of many that monitors blood sugar levels and other vital signs wirelessly in hospitals and homes, but it hasn’t released a mobile phone version.Up next: pacemaker and defibrillator interrogations.
-Wes
Need a Defibrillator? Call an Electrophysiologist
There is, after all, strength in numbers. From the national ICD Registry:
Reference: "Association of Physician Certification and Outcomes Among Patients Receiving an Implantable Cardioverter-Defibrillator," JAMA Vol. 301 No. 16, April 22/29, 2009.
Of 111,293 ICD (implantable cardiac defibrillator) implantations included in the analysis, 78,857 (70.9%) were performed by electrophysiologists, 24,399 (21.9%) by nonelectrophysiologist cardiologists, 1,862 (1.7%) by thoracic surgeons, and 6,175 (5.5%) by other specialists. Compared with patients whose ICD was implanted by electrophysiologists, patients whose ICD was implanted by either nonelectrophysiologist cardiologists or thoracic surgeons were at increased risk of complications in both unadjusted (electrophysiologists, 3.5% [2743/78 857]; nonelectrophysiologist cardiologists, 4.0% [970/24 399]; thoracic surgeons, 5.8% [108/1862]; P < .001) and adjusted analyses (relative risk [RR] for nonelectrophysiologist cardiologists, 1.11 [95% confidence interval {CI}, 1.01-1.21]; RR for thoracic surgeons, 1.44 [95% CI, 1.15-1.79]).-Wes
Reference: "Association of Physician Certification and Outcomes Among Patients Receiving an Implantable Cardioverter-Defibrillator," JAMA Vol. 301 No. 16, April 22/29, 2009.
Tuesday, April 21, 2009
How Insurance Pre-Approvals Impede Quality Care
When the ache in her lower abdomen became excruciating, the young woman was rushed to a surgery center, where the doctor diagnosed a ruptured appendix.As I read this story, I couldn't help but wonder why our quality advocates were not up in arms with outrage this morning. Why has the Agency for Healthcare Research and Quality (AHRQ) not developed specific quidelines the refuse to pay for such shoddy performance that delays a patient's care? Isn't the delay in therapy because of the medical "requirement" for insurance "pre-approval" dependent on a typed report in a case such as this the ultimate in poor care delivery? What would have happened in this case if the insurance company balked and refused to approve this patient's surgery? Would the doctor have been obligated to refused to do the surgery?
The woman needed an operation—fast. But before the surgeon could wheel her into the operating theater, he had to find out whether the patient's insurance company would pay. That meant paperwork: A report had to be dictated, typed up and submitted to her insurer for approval.
So while the woman waited in agony, her doctor dialed a toll-free number.
The instant he hung up a few minutes later, a digitized recording raced through fiber-optic cables on the Pacific Ocean seabed and into a computer server on the 17th floor of a Manila office tower, where medical school graduate Dinah Barrete was working the graveyard shift.Chicago Tribune, 21 Apr 2009
Of course not.
One of the largest breeches of "quality" patient care in health care today are insurance pre-approvals, especially in the circumstances of true medical emergencies. And it is expensive, too. Why should the doctor have to dictate his note or have it transcribed? What potential harm came to the patient as a result of the delay to her care? Do we know? Might there be other situations like a perforated viscus, depressed skull fracture, septicemia in a patient without a spleen be even more catastrophic if we had to wait for insurance pre-approvals and dictations before treating patients?
Certainly.
I would propose that the decision for surgery rests entirely with the doctor to decide, not some third party as this article suggests.
Let's save a ton of money and get rid of this insurance pre-approval racket and the insurance industry's requirements for a dictated note.
Then maybe we'd start saving real money during health care reform.
-Wes
Monday, April 20, 2009
As Medicare is Set Adrift
The acceptance of Medicare is dwindling amongst primary care doctors in affluent neighborhoods. Case in point: a patient I saw in clinic recently for her arrhythmia said:
Yep. At least for now.
But did I refill her Ambien (sleeping pill) prescription?
No. That I won't do as a heart rhythm specialist.
-Wes
"Would you mind ordering a CBC and all the chemistries I need for my annual physical? My internist no longer takes Medicare."So will subspecialists take up the slack as primary care doctors increasingly abandon the system?
Yep. At least for now.
But did I refill her Ambien (sleeping pill) prescription?
No. That I won't do as a heart rhythm specialist.
-Wes
Sunday, April 19, 2009
Watchman Will Be Watched Thursday
The Pioneer Press reports that Atritech's left atrial appendage "filter," the Watchman device, will be reviewed the FDA advisory panel Thursday.
I appreciate the mention.
-Wes
See also - Dr Wes: "A Big Day for Cardiac Electrophysiology"
I appreciate the mention.
-Wes
See also - Dr Wes: "A Big Day for Cardiac Electrophysiology"
Saturday, April 18, 2009
Humbled
I was humbled by the complexity of her arrhythmia a year ago. She was so sick. Heart failure. Relentless, ventricular tachycardia. No cause was ever found. Back then, I had to resort to a MacGyver moment and patch together a make-shift system to over-drive pace her recurrent ventricular tachycardia. I didn't think she'd make it. But with time, patience, and a bit of luck, she got better. Someone had other plans for her.
At first, I didn't know her except as an arrhythmia. She was a tough case, a bed number, a person on a ventilator. But as she awoke from sedation and her eyes blinked "thank you," I grew to know her. Remarkably, she recovered from what seemed like an impossible situation and for the past year, I came to know her and her husband a bit better: her graciousness, her kindness, her delightful smile, their love for one another and their gratitude for her care.
I continued to see her from time to time in our device clinic. Smiling, joking, moving slowly, gracious, befriending the nurses, amazed at the technology in side of her. For nearly a year since her presentation, she had done so well.
But lately she had become increasingly short of breath. Her cardiologist admitted her and asked me to see her again. I soon discovered that her left ventricular pacing lead had dislodged and wondered if this might be why she struggled. I suggested we might try repositioning it to improve her situation. She seemed relieved a cause had been found. I was reserved for I was uncertain it would help her, but offered to try. But as things would have it, her blood thinner precluded proceeding right away, and despite our best efforts to correct her coagulopathy for surgery, she returned to the ventilator once more.
On the machine, she felt better. At least sitting upright. Her eyes smiled the next morning even as the mechanical tube protruded from her mouth. The nurses marveled at her ability to tolerate the tube without sedation. I returned to her later to explain the situation, the risks, the options available to her, about the uncertain outcome if we proceeded. She nodded understanding, looked to her husband who sat beside her, then looked back and gave a thumbs up as if to say "Let's go for it." We planned to do her revision the following day, opting to keep her on the ventilator for safety's sake. All seemed set.
The next day, she was brought to the laboratory and lifted carefully to the table. As she was situated, she became abruptly short of breath, even when sitting at 45 degrees. Her oxygen was increased, she was allowed to sit up further. Her eyes looked anxious, exhausted, and defeated. It was clear we could not continue. Despite this, she blinked a tender blink of acknowledgement as I told her our problem, and made arrangements to take her back to the intensive care unit. She knew.
Shortly after arrival back in the ICU, she began to improve a bit once more. Her oxygen level climbed and she seemed more comfortable. Her husband was there and she looked at him adoringly, weakened and accepting. She clutched his hand. They talked of options with her, of more diuresis, of doing things to keep her comfortable, but she heard little as she drew the air from the machine and stared into his eyes.
Barely an hour after agreeing to avoiding resuscitate measures, her oxygen levels dropped and her breathing became labored, quickly shallowed, then stopped. Her hand became flaccid and the color drained from her face. Soon the scurrying of humanity left the room and it became eerily quiet as the monitors were turned off, the wires and tubes disconnected. This was not how I knew her, this way. But in the still of moment it was clear that peace had come to yet another remarkable woman I had the privilege to know. In her own way, she taught me creativity, resourcefulness, the value of perseverance, the promise of hope, and the power of kindness.
Imagine: doctor, teacher, and humbled student still.
-Wes
At first, I didn't know her except as an arrhythmia. She was a tough case, a bed number, a person on a ventilator. But as she awoke from sedation and her eyes blinked "thank you," I grew to know her. Remarkably, she recovered from what seemed like an impossible situation and for the past year, I came to know her and her husband a bit better: her graciousness, her kindness, her delightful smile, their love for one another and their gratitude for her care.
I continued to see her from time to time in our device clinic. Smiling, joking, moving slowly, gracious, befriending the nurses, amazed at the technology in side of her. For nearly a year since her presentation, she had done so well.
But lately she had become increasingly short of breath. Her cardiologist admitted her and asked me to see her again. I soon discovered that her left ventricular pacing lead had dislodged and wondered if this might be why she struggled. I suggested we might try repositioning it to improve her situation. She seemed relieved a cause had been found. I was reserved for I was uncertain it would help her, but offered to try. But as things would have it, her blood thinner precluded proceeding right away, and despite our best efforts to correct her coagulopathy for surgery, she returned to the ventilator once more.
On the machine, she felt better. At least sitting upright. Her eyes smiled the next morning even as the mechanical tube protruded from her mouth. The nurses marveled at her ability to tolerate the tube without sedation. I returned to her later to explain the situation, the risks, the options available to her, about the uncertain outcome if we proceeded. She nodded understanding, looked to her husband who sat beside her, then looked back and gave a thumbs up as if to say "Let's go for it." We planned to do her revision the following day, opting to keep her on the ventilator for safety's sake. All seemed set.
The next day, she was brought to the laboratory and lifted carefully to the table. As she was situated, she became abruptly short of breath, even when sitting at 45 degrees. Her oxygen was increased, she was allowed to sit up further. Her eyes looked anxious, exhausted, and defeated. It was clear we could not continue. Despite this, she blinked a tender blink of acknowledgement as I told her our problem, and made arrangements to take her back to the intensive care unit. She knew.
Shortly after arrival back in the ICU, she began to improve a bit once more. Her oxygen level climbed and she seemed more comfortable. Her husband was there and she looked at him adoringly, weakened and accepting. She clutched his hand. They talked of options with her, of more diuresis, of doing things to keep her comfortable, but she heard little as she drew the air from the machine and stared into his eyes.
Barely an hour after agreeing to avoiding resuscitate measures, her oxygen levels dropped and her breathing became labored, quickly shallowed, then stopped. Her hand became flaccid and the color drained from her face. Soon the scurrying of humanity left the room and it became eerily quiet as the monitors were turned off, the wires and tubes disconnected. This was not how I knew her, this way. But in the still of moment it was clear that peace had come to yet another remarkable woman I had the privilege to know. In her own way, she taught me creativity, resourcefulness, the value of perseverance, the promise of hope, and the power of kindness.
Imagine: doctor, teacher, and humbled student still.
-Wes
Friday, April 17, 2009
Folie à Trois Health Care
I had just spend an hour with the patient and her husband who lived here in Chicago discussing her condition and treatment options. So it was a strange moment when the husband of my patient walked out to me and handed me the phone.
"Can you talk to him?" he asked.
"Who's that?" I asked.
"Dr. Frigamafratz. He's our (concierge) doctor in Baltimore."
"Baltimore? Uh, sure."
I held the phone to my ear.
"Dr. Fisher?", a woman's voice asked.
"Yes?"
"Please hold one second while I get Dr. Frigamafratz on the phone," a lady with a very business-like demeanor said.
I heard static, popping, a voice come and go... then...
"Hello, Dr. Fisher?" (static, hissss, clicks, hisss) "I'm Dr. Frigamafratz. Can you tell me what's going on?"
I told him about the situation, about the fact that those skipped heart beats she had been experiencing and intermittent periods of lightheadedness were likely caused by brief bursts of right ventricular outflow tract tachycardia. About her workup. About her structurally normal heart. About her treatment options and the various options for treatment that I had recommended.
"Uh, yes..." (static...click....hisss) "Well, I see," he said.
Then silence.
"Hello? Hello?" I called.
The pleasant young lady came back on the line. "Yes, Dr. Fisher, I'm here. I'm sorry we must have lost Dr. Frigamafratz. I'd be happy to tell him the situation."
Frustrated and pushed for time, I capitulated and summarized the situation again to the lady on the phone, then handed the phone back to the husband. He thanked me for talking with their concierge doctor and I went on to complete my consult note and forwarded it back to the local referring physician. A while later, I returned to the room to see if my patient and her husband had decided on their course of therapy.
They chose medicines over ablation, much to my surprise given our conversation, but I understood her reluctance and respected her decision.
Later that evening, the patient's internist here in Chicago called me. I learned that our mutual patient had spoken with her concierge doctor, Dr. Frigamafratz, while I was writing my note. The internist was livid. Dr. Frigamafratz had not communicated with the internist about his input to the patient's care. (Doctors reading this know this is basic profesional ethics). I learned that Dr. Frigamafratz was a retired Emergency Room doctor and started this concierge's business to cater to high-end, well-traveled clients. I learned that the pleasant people on the phone were not nurses, but secretaries. Finally, I learned that Dr. Frigamafratz had recommended a therapy to my patient, yet knew nothing about her most recent situation and conducted his entire assessment over the phone without setting eyes on her or examining her.
No wonder the internist was livid.
As we plotted the next steps for our patient's treatment, I reflected on the growing movement for online, mobile, and internet-based physician care and suspect that we can expect more of these "who's on first" experiences in the years to come.
-Wes
"Can you talk to him?" he asked.
"Who's that?" I asked.
"Dr. Frigamafratz. He's our (concierge) doctor in Baltimore."
"Baltimore? Uh, sure."
I held the phone to my ear.
"Dr. Fisher?", a woman's voice asked.
"Yes?"
"Please hold one second while I get Dr. Frigamafratz on the phone," a lady with a very business-like demeanor said.
I heard static, popping, a voice come and go... then...
"Hello, Dr. Fisher?" (static, hissss, clicks, hisss) "I'm Dr. Frigamafratz. Can you tell me what's going on?"
I told him about the situation, about the fact that those skipped heart beats she had been experiencing and intermittent periods of lightheadedness were likely caused by brief bursts of right ventricular outflow tract tachycardia. About her workup. About her structurally normal heart. About her treatment options and the various options for treatment that I had recommended.
"Uh, yes..." (static...click....hisss) "Well, I see," he said.
Then silence.
"Hello? Hello?" I called.
The pleasant young lady came back on the line. "Yes, Dr. Fisher, I'm here. I'm sorry we must have lost Dr. Frigamafratz. I'd be happy to tell him the situation."
Frustrated and pushed for time, I capitulated and summarized the situation again to the lady on the phone, then handed the phone back to the husband. He thanked me for talking with their concierge doctor and I went on to complete my consult note and forwarded it back to the local referring physician. A while later, I returned to the room to see if my patient and her husband had decided on their course of therapy.
They chose medicines over ablation, much to my surprise given our conversation, but I understood her reluctance and respected her decision.
Later that evening, the patient's internist here in Chicago called me. I learned that our mutual patient had spoken with her concierge doctor, Dr. Frigamafratz, while I was writing my note. The internist was livid. Dr. Frigamafratz had not communicated with the internist about his input to the patient's care. (Doctors reading this know this is basic profesional ethics). I learned that Dr. Frigamafratz was a retired Emergency Room doctor and started this concierge's business to cater to high-end, well-traveled clients. I learned that the pleasant people on the phone were not nurses, but secretaries. Finally, I learned that Dr. Frigamafratz had recommended a therapy to my patient, yet knew nothing about her most recent situation and conducted his entire assessment over the phone without setting eyes on her or examining her.
No wonder the internist was livid.
As we plotted the next steps for our patient's treatment, I reflected on the growing movement for online, mobile, and internet-based physician care and suspect that we can expect more of these "who's on first" experiences in the years to come.
-Wes
Wednesday, April 15, 2009
Lawyers Say the Darnedest Things
Last night, I overheard a senior lawyer speaking with my wife, a psychologist:
But this got me thinking. What would we ask as salary for our services priced by the hour? Could we have this conversation with our patients after the dust had settled after an acute illness? If we factor in office expenses, the price of malpractice, account for our level of training and experience, and consider the price point of our attorney colleagues, what hourly wage would we accept? Would we be able to have this conversation, or have our policies and expectations made such a discussion too politically incorrect to broach with our patients?
I have heard others in private practice discuss this topic before while working in Cincinnati. One doctor mentioned to me that he had to bill at least $200 per hour just to cover their office expenses (receptionist, billing staff, office manager, benefits, vacation, utilities, rent, taxes, etc).
Certainly there are many geographic differences in the cost of living and practicing medicine in America. Also, different price-points might be acceptable for an primary care doctor or a specialist and worse, the amount we bill no longer pairs with the amount we can collect. But if each of us had to pick and hourly wage like lawyers, what would we charge if we take all of our expenses and vagaries of our current system into account? Given all of the overhead to health care today, would we have the ability to justify our hourly wage to our patients?
Given that it's likely to far exceed $200 per hour, I suspect none of us could have that conversation any more.
-Wes
"The first thing a lawyer does is discuss how much their services will cost their client. You know, in all my years of going to the doctor, I never once felt I needed to ask how much he cost."I couldn't resist joining in and said, "Well, that's because most know what to tell you, since for any given person, the doctor does not negotiate his own fee, it is negotiated for him by third parties." He nodded acknowledgement.
But this got me thinking. What would we ask as salary for our services priced by the hour? Could we have this conversation with our patients after the dust had settled after an acute illness? If we factor in office expenses, the price of malpractice, account for our level of training and experience, and consider the price point of our attorney colleagues, what hourly wage would we accept? Would we be able to have this conversation, or have our policies and expectations made such a discussion too politically incorrect to broach with our patients?
I have heard others in private practice discuss this topic before while working in Cincinnati. One doctor mentioned to me that he had to bill at least $200 per hour just to cover their office expenses (receptionist, billing staff, office manager, benefits, vacation, utilities, rent, taxes, etc).
Certainly there are many geographic differences in the cost of living and practicing medicine in America. Also, different price-points might be acceptable for an primary care doctor or a specialist and worse, the amount we bill no longer pairs with the amount we can collect. But if each of us had to pick and hourly wage like lawyers, what would we charge if we take all of our expenses and vagaries of our current system into account? Given all of the overhead to health care today, would we have the ability to justify our hourly wage to our patients?
Given that it's likely to far exceed $200 per hour, I suspect none of us could have that conversation any more.
-Wes
Tuesday, April 14, 2009
My Stimulus Package
Found this on my Bloom Stimulator (the device with which I pace - and "stimulate" - the heart during an electrophysiology study) this morning:

Heh. Gotta love those techs...
-Wes

Click image to enlarge
Heh. Gotta love those techs...
-Wes
The Health Information Legacy Problem
 “No one’s talking about the legacy problem with Information Technology systems,” he said.
“No one’s talking about the legacy problem with Information Technology systems,” he said.“What do you mean?” I asked.
“While every one’s talking about developing a fully-integrated nationwide electronic medical record, no one give a damn about the old systems that exist out there. They’re not worth supporting. No one cares about the data they contain, even though for the doctor, they contain critical documentation about patient’s prior health care and are vital documentation to prevent litigation.
He continued, “I was in an eight man group in 1995. We were very cutting-edge. We bought the latest and greatest software that printed out fully legible prescriptions in the patient’s exam room using personalized prescription pads. It organized our clinic visits – helped with scheduling and documentation of the examination – the works. Our first problem was when Windows NT shifted to Windows XP, we found the had to pay for the upgrade because Microsoft stopped supporting the old system. We quickly discovered that the printers we used to print our prescriptions didn’t work. Why? Because printer drivers for our older specialized printers weren’t available for the new operating system. The printers became useless. Who could I pay to develop these drivers?
But it didn’t end there. For other reasons, our group split up. Our eight-man group became four, and eventually over the next several years, two. We simply could no longer afford the maintenance on the fancier medical record system, so we bought a simpler one that was much less expensive to maintain but found that the data from the older system could not be imported into the new system.
What to do?
We couldn’t get rid of the old system for it contained all of the documentation on patients from the recent past. We had to pay to have it maintained while working to re-create patient data on a new system. Eventually, as time went on, fewer and fewer people knew how to support the old system, the hardware became obsolete, and finally I just stopped paying the maintenance fee. I went “naked” without archived medical records. What choice did I have?
So I ask you, when the government decides on a single electronic medical record system that suits their needs and is all-encompassing, what’s going to happen to all the data on the other systems? I bet every one's going to experience the same problems I did.”
-Wes
Image reference: Andrew* on Flickr via a Creative Commons license.
Monday, April 13, 2009
Whose Face Will You See Last?
In a well-written essay, a waiter confronts the frailty of life and asks the question after his became the last face seen by a total stranger.
As a doctor, we often are the last face some people see, I just wonder if we ever stop to think about it as this man did.
-Wes
As a doctor, we often are the last face some people see, I just wonder if we ever stop to think about it as this man did.
-Wes
EchoJournal Launched
Call it YouTube for echocardiography. The guys over a Medgadget have launched EchoJournal:
I wish I had thought of that.
-Wes
PS: I'd be careful to make sure patient identifiers are removed from video loops before uploading, however.
It is a video site, designed to present transthoracic and transesophageal loops for discussion and storage. EchoJournal combines many of the features familiar to users of other video sharing sites, including easy uploading, comments and discussions, and the ability to create communities for your academic department, professional group, or school. The site will be curated by David E. Winchester, MD, a Cardiology Fellow at the University of Florida, who has already uploaded tons of interesting cases, and is ready for many more.Great idea.
I wish I had thought of that.
-Wes
PS: I'd be careful to make sure patient identifiers are removed from video loops before uploading, however.
Sunday, April 12, 2009
How to Deal With Pirates
The US Navy way:
Bravo zulu, gentlemen.
-Wes
The American cargo ship captain held hostage by pirates jumped overboard Sunday from the lifeboat where he was being held, and U.S. Navy SEALs shot and killed three of his four captors, according to a senior U.S. official with knowledge of the situation.Absolutely.
Bravo zulu, gentlemen.
-Wes
What Matters When Choosing A Fellowship Program
It was an unusual week of Intensive Care Unit activity. There was atrial fibrillation, atrial flutter, cardiogenic shock, cor pulmonale and even an occasional atrial tachycardia thrown in for good measure. And while the patient issues were grave, the residents I saw seemed to take it all in stride, for they had just matched in their fellowship positions. Life was good. They were at the top of their game. They had survived Round 1.
-Wes
“So where are you going?” I asked. And they proceeded to tell me, appearing genuinely excited about their upcoming adventures. Hematology/oncology. Dermatology. Pulmonary medicine. Some programs here in Chicago, some far away, but still, they were enthusiastic. It was nice to see.And so, in my carefully-conduced ICU research on three current-day residents accustomed to dot-phrases and instant everything, I’d say the electronic medical record industry is secure.
I watched as they typed their notes – much faster than I could ever imagine. They stopped briefly to answer a text message on their cell phone, then continued. Streaking fingers on keyboards, multi-tasking, opening new windows to search a reference, facile at looking up who was covering infectious disease today by perusing the on-line call schedule. “The operators taught me,” she said. “They got upset I was bothering them for the information all the time.”
And so it went.
Watching this, I couldn’t help but ask: “What would you guys ever do without an electronic record, I mean, have any of you ever entered a paper-based order?”
“Oh, yeah. I’ve done it. But I don’t think I could ever go back. Oh, God, no!”
“Really? What if the computer goes down? Doesn’t it ever worry you that things might grind to a halt? What about new residents who have never seen a paper chart?”
“Oh-my-God! They’d have no clue! I heard Suzie matched at Georgetown, and they still have paper-based records – I mean – I feel so sorry for her. She won’t have a clue. I’d never go to a program with paper records any more. It would suck.”
-Wes
Saturday, April 11, 2009
When Residents Become Vectors
One pediatric resident recently diagnosed with tuberculosis who traveled to three hospitals for her training (including ours) has caused quite a stir.
Ironically, I am due to receive my TB skin test Monday as part of our annual surveillance program.
-Wes
Ironically, I am due to receive my TB skin test Monday as part of our annual surveillance program.
-Wes

Why You Should Be a Doctor
With all the news and challenges in health care today, it's nice to know there's still some pretty compelling reasons to be a doctor today.
But I would caution anyone contemplating the profession solely for the money, better move on to finance.
Oh, wait. Maybe not.
-Wes
But I would caution anyone contemplating the profession solely for the money, better move on to finance.
Oh, wait. Maybe not.
-Wes
Friday, April 10, 2009
Cardiology Fellow Made $250,000 While Moonlighting
Um, it might not be legal:
Court records show Tiano worked at the clinic between 2005 and 2007 while working as a cardiology fellow at Marshall. Tiano earned $250,000 between August 2005 and September 2007, according to the affidavit.-Wes
Tiano's medical license was placed on three years' probation in December 2008, according to the state Board of Medicine.
Tiano was reprimanded by the board in connection with "prescribing, dispensing or administering a prescription drug other than in good faith and in a therapeutic manner in accordance with accepted medical standards, and failing to practice medicine acceptably," according to the order placing his medical license on probation.
I'm a Twit
I've broken down and joined Twitter. You can follow me there at:
http://twitter.com/doctorwes.
If you have no idea what Twitter is, this might help. If you have no interest in 140-character blurbs constantly interrupting you on your cellphone, I understand.
-Wes
http://twitter.com/doctorwes.
If you have no idea what Twitter is, this might help. If you have no interest in 140-character blurbs constantly interrupting you on your cellphone, I understand.
-Wes
When Business Meets Medicine
... business gets squeezed. From the front page story of the Chicago Tribune today entitled "Are Hospitals Passing Off Their Low-Profit Patients?"
Increasingly, doctors find themselves at the crossroads of medicine and business because they are no longer independent, but employed by hospitals run by business people. This business relationship threatens the very fiber of the doctor-patient relationship central to the practice of medicine. Unfortunately, what we're seeing now are the strains created when third party interests and market forces have sufficiently disrupted that relationship.
-Wes
Officials at non-profit hospitals contacted by the Tribune vigorously deny that they steer patients to Stroger's ER and say that they treat everyone who shows up at their hospitals.These are not simple issues. Hospitals, often the largest community employer, struggle to manage staying fiscally sound at a time when the economy has tanked. Liability and regulatory requirements demand a bloated staff of quality assurance, information technology consultants, billing and collection agents, and the like. Competition from surrounding facilities is keen, with every other hospital purchasing the latest robots and technology to stay ahead of their competitors, lest they lose the patients and doctors, the lifeblood of their cash flow, to their rivals. Add to this, the potential to lose their cherished tax exempt status, and one can see the challenges that confront today's hospital administrators.
They defend policies that move some patients out of emergency rooms—known as "triage out"—as reasonable measures to ensure proper care without overburdening ERs.
"Is it unreasonable for hospitals to ask if there are better ways to care for people more efficiently?" asks Howard Peters, senior vice president of governmental affairs for the Illinois Hospital Association.
But some ER doctors are concerned about these policies and what they mean for quality of care for poor patients.
"This is basically legalized patient dumping," said Dr. Jesse Pines, an assistant professor of emergency medicine at the University of Pennsylvania School of Medicine.
Pines also is a member of the American College of Emergency Room Physicians, which recently criticized the University of Chicago Medical Center for plans to send non-urgent patients to other facilities while cutting the number of inpatient beds available to the ER.
The group's members argue that because ERs are staffed and equipped 24 hours a day—regardless of who shows up—the added costs of caring for patients with non-urgent ailments is comparable to a doctor's office visit.
"We have a responsibility to rule out an emergency medical condition," said Dr. Catherine Marco, an ER professor at the University of Toledo and a member of the American College of Emergency Room Physicians' ethics committee. "If we're going that far, why not close the loop? At that point, it's not a labor intensive issue."
Critics of the U. of C. plan questioned whether it was a way for the hospital to avoid caring for indigent and Medicaid patients. Parts of the plan were later put on hold after two national ER physician groups and doctors inside the medical center spoke out against it.
Increasingly, doctors find themselves at the crossroads of medicine and business because they are no longer independent, but employed by hospitals run by business people. This business relationship threatens the very fiber of the doctor-patient relationship central to the practice of medicine. Unfortunately, what we're seeing now are the strains created when third party interests and market forces have sufficiently disrupted that relationship.
-Wes
Gainsharing: Who Gains?
Business people love policies that are "win-win."
And with health care occupying an increasingly important portion of our gross national product, medicine has become big business. So it makes sense that the "stakeholders" in medicine like a good "win-win" scenario, too.
Do a better job, and the patient gets better. "Win-win." Work more efficiently and use less resources so costs are dropped. "Win-win." Do a really good job, meet some quality targets that an insurer has set for a hospital, then maybe the hospital can pass on those bonuses to doctors. Hey, it's a trifecta! "Win-win-win!"
It sounds so good on paper and in theory. In fact, it sounds so good, that even the Office of the Inspector General (OIG) of the United States seems to be warming up to the idea of more gainsharing arrangements.
And gainsharing offers limitless opportunities for marketing to our new health care "consumers." (I think that means "patients," but I'm not always sure.)
Perhaps the best example of the juicy marketing spin regarding gainsharing can be seen at the Geisinger Health System that guarantees coronary bypass outcomes:
Win-win-win!
But there's more:
All on the backs of "gainsharing."
That's right - when they do everything by the book in their "Proven-Care" program, Geisinger achieved (according to the above article) a 0% 30-day post-bypass mortality using their "Proven-Care" methods! Unbelievable!
To which, I say, they must not be treating very sick patients.
I used to have a senior attending who told me that you never want to be cared for by a doctor who had never seen a complication. Complications are why fellows spend so many hours in a catheterization laboratory. They happen. Even in the best of hands. And it's the process of dealing with those complications where fellows do their advanced learning. That's where they learn to deal with the unexpected, the complicated, the unusual, and yes, the sick. As one attending said, "Any moron can sink a Jud." ("Jud" in this case referred to a JL-4, "Judkins-Left-4cm" standard left heart diagnostic catheter that usually finds the left main coronary orifice easily). The implication of his statement was that's is not about doing the easy, routine stuff that really helps the patient (anyone can do that), it's the hard stuff - the stuff that's not automatic, not in the textbook, or not in the algorithm - that shapes us as physicians.
Certainly, there is good that can come from developing an organized, team-approach to health care. When everyone is involved at improving the system, patients benefit (can you say "TQM - Total Quality Management?"). But when that effort is tied financially to outcome incentives, the risk of gaming the system to assure better outcomes can be expected. After all, business ethics are not medical ethics.
As a case in point, when we see perfect mortality scores as a result of "gainsharing" arrangements we must ask ourselves, what has been sacrificed in the name of outcome perfection? Which patients were excluded? Will only insured patients have an opportunity to participate in such a program because they are effectively "pre-screened?" Where are the sickest being shunted? What kind of health care system are we striving for - one that treats the "kinda sick" but not the "real sick?" Do we really want to reward perfect mortality scores at the expense of ignoring the benefits that occur to our patients from calculated risk-taking, even some outcomes may be less than perfect?
Who gains then?
-Wes
And with health care occupying an increasingly important portion of our gross national product, medicine has become big business. So it makes sense that the "stakeholders" in medicine like a good "win-win" scenario, too.
Do a better job, and the patient gets better. "Win-win." Work more efficiently and use less resources so costs are dropped. "Win-win." Do a really good job, meet some quality targets that an insurer has set for a hospital, then maybe the hospital can pass on those bonuses to doctors. Hey, it's a trifecta! "Win-win-win!"
It sounds so good on paper and in theory. In fact, it sounds so good, that even the Office of the Inspector General (OIG) of the United States seems to be warming up to the idea of more gainsharing arrangements.
And gainsharing offers limitless opportunities for marketing to our new health care "consumers." (I think that means "patients," but I'm not always sure.)
Perhaps the best example of the juicy marketing spin regarding gainsharing can be seen at the Geisinger Health System that guarantees coronary bypass outcomes:
"Mimicking the appliance company that advertised its products’ reliability, the health system devised a 90-day warranty on elective heart surgery, promising to get it right the first time, for a flat fee. If complications arise or the patient returns to the hospital, Geisinger bears the additional cost."Simply brilliant. Who wouldn't want that, right?
Win-win-win!
But there's more:
"The venture has paid off. Heart patients have fared measurably better, and the health system has cut its bypass surgery costs by 15 percent. Today, Geisinger has extended the program to half a dozen other procedures, and initiatives such as the counter-intuitive experiment in Pennsylvania coal country are now at the heart of efforts in Washington to refashion how care is delivered across the United States."See? Utopia. Right here in the good 'ol U.S.A.
All on the backs of "gainsharing."
That's right - when they do everything by the book in their "Proven-Care" program, Geisinger achieved (according to the above article) a 0% 30-day post-bypass mortality using their "Proven-Care" methods! Unbelievable!
To which, I say, they must not be treating very sick patients.
I used to have a senior attending who told me that you never want to be cared for by a doctor who had never seen a complication. Complications are why fellows spend so many hours in a catheterization laboratory. They happen. Even in the best of hands. And it's the process of dealing with those complications where fellows do their advanced learning. That's where they learn to deal with the unexpected, the complicated, the unusual, and yes, the sick. As one attending said, "Any moron can sink a Jud." ("Jud" in this case referred to a JL-4, "Judkins-Left-4cm" standard left heart diagnostic catheter that usually finds the left main coronary orifice easily). The implication of his statement was that's is not about doing the easy, routine stuff that really helps the patient (anyone can do that), it's the hard stuff - the stuff that's not automatic, not in the textbook, or not in the algorithm - that shapes us as physicians.
Certainly, there is good that can come from developing an organized, team-approach to health care. When everyone is involved at improving the system, patients benefit (can you say "TQM - Total Quality Management?"). But when that effort is tied financially to outcome incentives, the risk of gaming the system to assure better outcomes can be expected. After all, business ethics are not medical ethics.
As a case in point, when we see perfect mortality scores as a result of "gainsharing" arrangements we must ask ourselves, what has been sacrificed in the name of outcome perfection? Which patients were excluded? Will only insured patients have an opportunity to participate in such a program because they are effectively "pre-screened?" Where are the sickest being shunted? What kind of health care system are we striving for - one that treats the "kinda sick" but not the "real sick?" Do we really want to reward perfect mortality scores at the expense of ignoring the benefits that occur to our patients from calculated risk-taking, even some outcomes may be less than perfect?
Who gains then?
-Wes
Thursday, April 09, 2009
Bogus Medical Board Certification Targets Immigrant Physicians
In October 2007, I wrote a post about a fraudulent board certification scheme that I researched after being sent an application for "certification" in the bogus American Academy of Cardiology spearheaded by a "Reverend A. Lasko, MD" or "Reverend K. Lasko, MD" - I wasn't sure. Later, I was subpoenaed by this man to appear before his lawyer in a suit between he and his sister (I was not a party to the suit). The subpoena insisted I bring down my blog post and identify the the URLs of those who commented. After fighting to have the subpoena quashed, the subpoena was rendered "moot" after the suit was dismissed.
Since that time, the American Board of Internal Medicine has been busy tracking Mr. Lasko's whereabouts. Today, the Connecticut Attorney General's Office offered this press release verifying Mr. Lasko's identity and alias's used for his scam:
I sincerely hope they catch this guy. After all, I've got some serious legal fees I need repaid.
-Wes
Since that time, the American Board of Internal Medicine has been busy tracking Mr. Lasko's whereabouts. Today, the Connecticut Attorney General's Office offered this press release verifying Mr. Lasko's identity and alias's used for his scam:
"Blumenthal's office has learned that an out-of-state individual known as Keith Alan Lasko -- who also uses the names K. Lasko, Keith Ferrari, K. Ferrari, and KA James Windsor -- has sold phony certifications to doctors in a variety of medical specialties in exchange for submitting only basic information and a substantial fee.Bottom line: buyer beware.
At least 130 more complaints have been reported, including at least one in Connecticut.
Lasko's alleged scheme particularly targets foreign-born or foreign-taught doctors who may be unaware of the proper certification process.
"Real and recognized medical board certifications require rigorous examination and education -- not simply payment for a piece of paper," Blumenthal said. "This scheme deceives patients and medical professionals, and endangers lives -- misleading consumers into believing that their physicians possess a level of expertise that they lack.
"This alleged con artist used false names -- for himself and for fictitious medical boards whose fake certificates he sold. Doctors face potential legal action if they misrepresent their credentials with phony certificates. These specialty-seeking doctors who paid substantial sums -- $500 or higher -- were typically foreign born or foreign educated, and now should know better."
I sincerely hope they catch this guy. After all, I've got some serious legal fees I need repaid.
-Wes
If You Can't Beat 'Em...
... join 'em.
At least that seems to be the trend:
-Wes
At least that seems to be the trend:
"The Iowa Heart Center, which is one of the country’s largest groups of cardiology doctors, is considering a merger with Mercy Medical Center in Des Moines. Dr. Bill Wickemeyer, president of Iowa Heart’s board, said the group’s doctors would continue serving patients at all current locations, including hospitals controlled by Mercy’s rival, Iowa Health-Des Moines. He said his practice wanted to emulate places like the Mayo Clinic and the Cleveland Clinic, where specialists work for a large, up-to-date hospital.If you want to belly-up to the ongoing, tenuous government health care trough, the ever-expanding bureaucratic requisites leave cardiologists with no other choice.
“This model seems to be the most successful as we look around the country,” Wickemeyer said.
Iowa Heart has 54 physicians."
-Wes
Guy Humor
Somehow, I found this very funny when I came across it:
h/t: Boing Boing via Instapundit.
"The drive to bring good manners back to football has reached new heights after a referee issued a yellow card to a player for "breaking wind" as a penalty (shot) was being taken."-Wes
h/t: Boing Boing via Instapundit.
Wednesday, April 08, 2009
The Challenge of Medical Device Advisories
It was a routine pacemaker implant yesterday. No big deal, really.
But there's always one point of a surgical procedure that grabs the doctor's gonads, and for device implants, it's usually gaining access to the blood vessel where the leads for a pacemaker or defibrillator are to be implanted. You see, poke too deeply, you might hit the patient's lung. Poke a half a centimeter higher toward the patient's head, you might hit the high-pressure artery rather than the low pressure vein and bleeding will compress the target vein, making it very difficult to cannulate. Don't poke deeply enough, you never get in the vessel. That's the way these procedures go. (I've already mentioned that I cheat and use a vascular ultrasound device to find the vessel. I mean, why stress, right?)
But yesterday, I encountered a "new" challenge: not being able to advance a guidewire into the vessel after I had entered it with a needle.
"What the....?" This was certainly not something I had encountered before. And that's when the rep who was in the lab said: "I wonder if that's one of those recalled SafeSheaths."
"What recalled SafeSheaths?"
"I'm not sure, but I think there was a problem that sometimes the needle hub was not aligned properly and people couldn't pass a guidewire into the vein."
"Seriously? Well that sucks," I said.
So I had to pull out the carefully placed needle and try a new one. Fortunately, the rest of the procedure went fine. But I stopped briefly later to see what existed on the Internet about this problem, and sure enough, I found this little pdf document about the problem posted way back in September, 2008. I was unaware of this problem.
I wonder, how many other advisories am I unaware of? What responsibility to distributors of medical products have to their customers? What responsibility to the manufacturers have? What did I miss?
Because all of the FDA warnings and advisories and recalls don't mean a thing if the information is not received by the end users. Unfortunately, I suspect this will always be a challenge, irrespective of the amount of money we pour into oversight bodies. Maybe, just maybe, placing information like this in the blog-o-sphere will help out another device implanter caught unaware.
-Wes
But there's always one point of a surgical procedure that grabs the doctor's gonads, and for device implants, it's usually gaining access to the blood vessel where the leads for a pacemaker or defibrillator are to be implanted. You see, poke too deeply, you might hit the patient's lung. Poke a half a centimeter higher toward the patient's head, you might hit the high-pressure artery rather than the low pressure vein and bleeding will compress the target vein, making it very difficult to cannulate. Don't poke deeply enough, you never get in the vessel. That's the way these procedures go. (I've already mentioned that I cheat and use a vascular ultrasound device to find the vessel. I mean, why stress, right?)
But yesterday, I encountered a "new" challenge: not being able to advance a guidewire into the vessel after I had entered it with a needle.
"What the....?" This was certainly not something I had encountered before. And that's when the rep who was in the lab said: "I wonder if that's one of those recalled SafeSheaths."
"What recalled SafeSheaths?"
"I'm not sure, but I think there was a problem that sometimes the needle hub was not aligned properly and people couldn't pass a guidewire into the vein."
"Seriously? Well that sucks," I said.
So I had to pull out the carefully placed needle and try a new one. Fortunately, the rest of the procedure went fine. But I stopped briefly later to see what existed on the Internet about this problem, and sure enough, I found this little pdf document about the problem posted way back in September, 2008. I was unaware of this problem.
I wonder, how many other advisories am I unaware of? What responsibility to distributors of medical products have to their customers? What responsibility to the manufacturers have? What did I miss?
Because all of the FDA warnings and advisories and recalls don't mean a thing if the information is not received by the end users. Unfortunately, I suspect this will always be a challenge, irrespective of the amount of money we pour into oversight bodies. Maybe, just maybe, placing information like this in the blog-o-sphere will help out another device implanter caught unaware.
-Wes
On Sprint Fidelis Lead Extraction
The New York Times published an article in their business section (interesting location to put such an article, but I digress) about extracting the Medtronic's advisory Sprint Fidelis defibrillator "cable" recently. (Note to their editors, it's actually a "defibrillator lead" containing multiple wires, not a "cable.") The article quotes some of the best and brightest in the lead extraction field - all of whom are truly experts at the task. It is interesting to note the differences in management style that these guys display: some (Wilkoff) would re-use the lead when it comes times for generator change, while others advise removing the lead at the time of a defibrillator generator (battery) change. There is little mention about placing a new lead next to the old one. Instead, the article suggests that "leaving it in place can make it more difficult to remove later, because of in-grown tissue."
No, that is not the reason to have the lead extracted. On the contrary, that's a reason to leave the lead in place so you can avoid the potential risk of tearing one of the great vessels and bleeding to death during the extraction procedure. After 6 months most of these leads have their "ingrowth" of tissue well-established. The "ingrowth" is not like a cancer that continues to grow. It can become more dense and even calcified over time, however, and the amount of ingrowth varies patient to patient.
Most experienced explanters look for certain characteristics on any lead that needs to be extracted to determine the potential difficulties they might encounter. Leads with more shocking coils are usually more difficult to extract because the coils often become adherent to tissue. Also, leads that passivly fix to the heart by scar formation tend to be harder to extract compared to those that actively screw into the heart muscle (and can have the screw retracted before removal). These are some of the bigger factors to explain why some of these leads come out more easily than others.
Admittedly, sometimes the lead must be extracted because the blood vessel into which the original lead was inserted became completely occluded and a new lead simply cannot be placed next to the old one without removing the old one first. Sometimes there's a desire not to implant a new device from the opposite chest area because of anatomic issues, like a prior mastectomy. Or maybe the lead has become infected, then it MUST be removed because, like a splinter festering in your foot, the infection will never resolve unless the lead is removed in its entirety. These reasons I'd buy as reasons to consider lead extraction. Also, patient preference of anxiety influences the decision to remove the lead, sometimes despite the doctor's best attempts at suggesting alternatives. There will always be a few of these.
But if it is at all possible to place a new lead at the time of battery change, that's seems like a reasonable compromise to me that avoids most future issues with the advisory lead. Certainly, Dr. Wilcoff thinks that the fracture rate is low enough that he'd just re-use it. While this conservative approach might make sense in most instances, is more difficult to justify when a patient is pacemaker-dependent and must have a normally functioning lead at all times for their heart to beat. In these cases, placement of a new lead, especially at the time of device battery change when the risk of infection is unavoidable, might warrant a more aggressive approach to avoid a potentially fatal complication should the lead later fracture. But what to do if the implant vessel is completely occluded and no room exists to place a new lead in such a pacemaker-dependent patient? This is where the toughest clinical issue lies: do you implant a whole new system from the contra-lateral side or just a pace-sense lead and then tunnel the lead to the same side as the others? Or do you extract the lead to make room for a new one? Given the risks involved with extraction, it's hard to know if the "cure" is worse than the disease.
What is certain is that patients with this lead should discuss all of these potential eventualities with their cardiologist or electrophysiololgist before any surgery takes place to develop a game plan should any of these challenges be encountered during routine device battery-change surgeries.
-Wes
No, that is not the reason to have the lead extracted. On the contrary, that's a reason to leave the lead in place so you can avoid the potential risk of tearing one of the great vessels and bleeding to death during the extraction procedure. After 6 months most of these leads have their "ingrowth" of tissue well-established. The "ingrowth" is not like a cancer that continues to grow. It can become more dense and even calcified over time, however, and the amount of ingrowth varies patient to patient.
Most experienced explanters look for certain characteristics on any lead that needs to be extracted to determine the potential difficulties they might encounter. Leads with more shocking coils are usually more difficult to extract because the coils often become adherent to tissue. Also, leads that passivly fix to the heart by scar formation tend to be harder to extract compared to those that actively screw into the heart muscle (and can have the screw retracted before removal). These are some of the bigger factors to explain why some of these leads come out more easily than others.
Admittedly, sometimes the lead must be extracted because the blood vessel into which the original lead was inserted became completely occluded and a new lead simply cannot be placed next to the old one without removing the old one first. Sometimes there's a desire not to implant a new device from the opposite chest area because of anatomic issues, like a prior mastectomy. Or maybe the lead has become infected, then it MUST be removed because, like a splinter festering in your foot, the infection will never resolve unless the lead is removed in its entirety. These reasons I'd buy as reasons to consider lead extraction. Also, patient preference of anxiety influences the decision to remove the lead, sometimes despite the doctor's best attempts at suggesting alternatives. There will always be a few of these.
But if it is at all possible to place a new lead at the time of battery change, that's seems like a reasonable compromise to me that avoids most future issues with the advisory lead. Certainly, Dr. Wilcoff thinks that the fracture rate is low enough that he'd just re-use it. While this conservative approach might make sense in most instances, is more difficult to justify when a patient is pacemaker-dependent and must have a normally functioning lead at all times for their heart to beat. In these cases, placement of a new lead, especially at the time of device battery change when the risk of infection is unavoidable, might warrant a more aggressive approach to avoid a potentially fatal complication should the lead later fracture. But what to do if the implant vessel is completely occluded and no room exists to place a new lead in such a pacemaker-dependent patient? This is where the toughest clinical issue lies: do you implant a whole new system from the contra-lateral side or just a pace-sense lead and then tunnel the lead to the same side as the others? Or do you extract the lead to make room for a new one? Given the risks involved with extraction, it's hard to know if the "cure" is worse than the disease.
What is certain is that patients with this lead should discuss all of these potential eventualities with their cardiologist or electrophysiololgist before any surgery takes place to develop a game plan should any of these challenges be encountered during routine device battery-change surgeries.
-Wes
Tuesday, April 07, 2009
What Health Care Reform Might Look Like
... if Rahm Emanuel's brother, Ezekiel, has his way. His book describes the use of a Federal Health Board and a VAT tax but:
-Wes
"Some were put off by proposals in his book, including a plan to scrap Medicare, Medicaid and employer-based health insurance in favor of vouchers that people could use to purchase coverage."Hey, at least he's trying... and a physician on the "team," no less...
-Wes
EKG Du Jour #15: What's Inside?
Here's a recent pacemaker interrogation showing a simultaneous surface EKG (top tracing), right atrial marker channel (center tracing) and right atrial electrogram (bottom tracing) from a patient who underwent aortic valve replacement over 30 years ago and later mitral valve replacement about 6 years ago. He has had multiple bouts of symptomatic atrial flutter that have responded to electrical cardioversion. His echocardiogram has demonstrated a nearly 7-centimeter left atrium, among other things. He was now fairly asymptomatic at the time of this recording:

How does one explain what's seen?
-Wes
hat tip: Alan D. Kogan, MD for supplying the tracing.
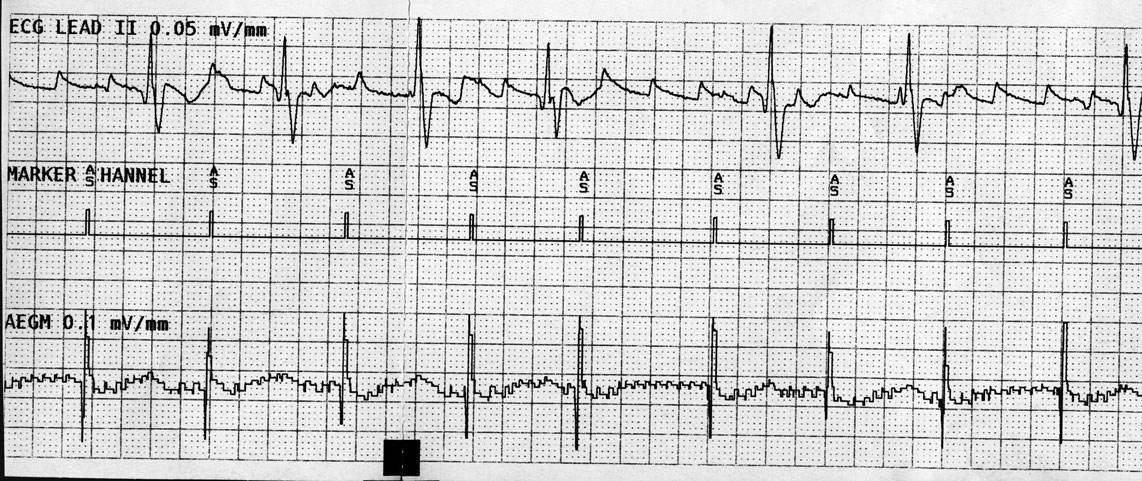
Click image to enlarge
How does one explain what's seen?
-Wes
hat tip: Alan D. Kogan, MD for supplying the tracing.
Sunday, April 05, 2009
The Anesthetists Hymn
Another great song from two well-known UK doctors, Adam Kay and Suman Biswas, also known as the Amateur Transplants:
(See the live version performed here).
-Wes
(See the live version performed here).
-Wes
Saturday, April 04, 2009
The Wonders of Electronics
E-prescribing.
The envy of Washington.
The envy of IT departments.
But occassionly, the scourge of doctors and patients.
Why?
No paper trail. No proof. Just lost electrons when a prescription fails to go through.
When it works, it's great: a script flies at the speed of light (literally) to a local pharmacy near you. One set up to receive the little electrons and it pops up on Mr. Pharmacist's work cue. Presto!
But when it fails, doctors become the impotent bad guys:
I sat and looked at the order verification screen before me. Wonderdrug. 10mg tablets. YourLocalPharmacy in YourTown. E-Script. Order confirmation number. All correct. Seemingly sent.
And yet, nothing. Vapor. Into the electronic ether. I felt like the the young apprentice sitting before the zen master:
The envy of Washington.
The envy of IT departments.
But occassionly, the scourge of doctors and patients.
Why?
No paper trail. No proof. Just lost electrons when a prescription fails to go through.
When it works, it's great: a script flies at the speed of light (literally) to a local pharmacy near you. One set up to receive the little electrons and it pops up on Mr. Pharmacist's work cue. Presto!
But when it fails, doctors become the impotent bad guys:
"Hey doc, you never sent my script."
"Uh, yes, Mr. Jones, I did. I sent it to YourLocalPharmacy in YourTown yesterday. I even have the order number."
"Doc, I was at YourLocalPharmacy and he said you never sent it. He didn't have any scripts with my name. Nothing. Nada. You sure you sent it off?"
"Yes, Mr. Jones, I'm looking at the order right now. I never received an e-mail that it failed to deliver, like it's supposed to if that happens, but I'll call the Pharmacist at YourLocalPharmacy in YourTown and find out what's up."
"Thanks, Doc."
* brrriinnnnggggg bbbbrrrriinngggg *
* Click *
"Hello. Welcome to YourLocalPharmacy where you can get all your meds at a moments notice! If you're a calling about a new prescription, press 1. If you're a doctor or a doctor's office calling, press 2..."
*2*
"Just a moment please..." ("Tie a yellow ribbon 'round the old oak tree" plays in the background...)
"This is Sally the pharmacy assistant, may I help you?"
"Yes Sally, this is Doctor Fisher and I'm inquiring about a prescription on Mr. SomeDude that I wrote as an e-prescription yesterday for 10 mg tablets of Wonderdrug, and he says you never received it..."
"Just a moment, doctor..."
(... it's been two long years, will you still want me...)
"This is Joe the Pharmacist..."
"Yes, Joe, this is Doctor Fisher and I'm calling about my prescription on Mr. SomeDude that I sent yesterday as an e-prescription for 10 mg tablets of Wonderdrug and he was told you never received it..."
"What was the last name?"
"SomeDude..."
"One second..."
(...stay on the bus, forget about us, put the blame on meeeee...)
"I'm sorry, we don't have anything for a Mr. SomeDude here at our pharmacy..."
"Would you like the order confirmation number that I have on my handy dandy EMR screen that says it was sent to you yesterday about 12:45 PM - yep, sent to YourLocalPharmacy in YourTown on 3 April."
"We don't use order numbers here... Wait, let me check one other place. One second..."
"Now the whole damn bus is cheering, and I can't believe I seeeee, a hundred yellow ribbons round the ole oak tree..."
"Hello, Dr. Fisher?"
"Yes?"
"We don't have any scripts here for Mr. SomeDude. I checked both our systems and don't see anything for him here.... Maybe our staff hit a delete key or something. Sometimes that happens you know. I just don't see it... What did you want to give him again? I'll just take the verbal and have it ready for him..."
"Its for sixty 10-milligram pills of WonderDrug with two refills. The sig is one to two tablets every six hours as needed for what he really needs it for."
"Okay, I'll have it ready for him..."
I sat and looked at the order verification screen before me. Wonderdrug. 10mg tablets. YourLocalPharmacy in YourTown. E-Script. Order confirmation number. All correct. Seemingly sent.
And yet, nothing. Vapor. Into the electronic ether. I felt like the the young apprentice sitting before the zen master:
Apprentice: "Master, if a tree falls in the forest and no one hears it, does it make a sound?"-Wes
Zen Master: "No, Grasshopper... but the squirrel it lands on does."

Friday, April 03, 2009
Heading Home on Friday
It's amazing what comes to the lab just for a few pacemaker implants these days...

-Wes
Click to enlarge
-Wes
Thursday, April 02, 2009
Digoxin: Another Generic Drug Recalled
First it was digitek, then generic Toprol ER, now it's digoxin from Caraco Pharmaceuticals.
Caraco Digoxin 0.125 mg is a scored round biconvex yellow tablet imprinted with “437” and Caraco Digoxin 0.25 mg is a scored round biconvex white tablet imprinted with “441.”
Fortunately, alternate generic suppliers of digoxin exist and include Actavis Totawa, Smithkline Beecham, Jerome Stevens, and West Ward.
-Wes
Reference: The FDA's electronic "Orange Book" containing Approved Drug Products With Therapeutic Equivalence Evaluations.
Caraco Digoxin 0.125 mg is a scored round biconvex yellow tablet imprinted with “437” and Caraco Digoxin 0.25 mg is a scored round biconvex white tablet imprinted with “441.”
Fortunately, alternate generic suppliers of digoxin exist and include Actavis Totawa, Smithkline Beecham, Jerome Stevens, and West Ward.
-Wes
Reference: The FDA's electronic "Orange Book" containing Approved Drug Products With Therapeutic Equivalence Evaluations.
Wednesday, April 01, 2009
The Challenge of Readmissions
Today in the New York Times, we learned of the hopes of the politico in Washington DC to idealize the problem of readmissions to hospitals as a cost saving measure for Medicare and Medicaid. While this is a laudible goal, the challenges of readmissions to hospitals is not as simple as the pundits might suggest. Take for instance, these 9 patients who visited ER's 2,678 times between 2003 and 2008.
When we see data like this, I wonder how much government bureaucracy poured into hospital mandates will really address the underlying societal challenges we have before us.
-Wes
h/t: A faithful reader.
When we see data like this, I wonder how much government bureaucracy poured into hospital mandates will really address the underlying societal challenges we have before us.
-Wes
h/t: A faithful reader.
Could Hospital Rankings Hurt Patients?
There's now evidence hospital ranking schemes might adversely affect some patients:
"Recent studies in Massachusetts and nationally suggest that cardiologists may be turning away more high-risk patients as an unintended consequence of public reporting, Resnic said. In a paper published in the Journal of the American College of Cardiology last month, Resnic and his coauthors reported that in 2005, the proportion of patients undergoing angioplasty in Massachusetts for cardiogenic shock - a life-threatening condition caused by poor heart function - dropped to 1.3 percent, from 2.3 percent in 2003, the year the state began publicly reporting angioplasty death rates. Since then, the rate has been level, he said."-Wes
The Cost of Fainting
What it will cost after you faint in a public space? Kirk Nielsen, of Miller-McCune.com, explains:
Read on.
-Wes
"I was afraid, I thought I might be dying, I was thinking about my deductible. The number '$2,500' flashed through my mind. Or was that my maximum 'out of pocket'?How much did the workup "cost?" How much did the insurer pay? How much did the patient end up paying for the ambulance ride and the care he received?
I knew for sure that I was enrolled in a $129-per-month emergency and hospitalization plan with Blue Cross Blue Shield of Florida. Like everyone, I'd heard that a trip to an emergency room could cost several grand.
'I can't afford that,' I muttered.
'Now isn't the time to worry about money,' my sister responded, slightly scolding.
Then my eyes rolled upward into my skull as I blacked out again, my chin dropping to the top of my chest and the rest of me still just sitting there."
Read on.
-Wes
Measure Twice, Cut Once
It is interesting to note that Kathleen Sebelius, named as U.S. health secretary by President Barack Obama, decided to "measure twice" her tax obligations over the past three years before proceeding to Senatorial confirmation and, gosh, found some errors that needed to be corrected.
Wasn't Ms. Sebelius just advocating for a 51-vote edge instead of the usual 60-votes needed for passage of the health care reform bill to assure its passage? Why wouldn't they want to give the same meticulois attention to our nation's health care proposals and carefully vet them? Wouldn't it be better to measure twice, and cut once?
Just asking.
-Wes
Wasn't Ms. Sebelius just advocating for a 51-vote edge instead of the usual 60-votes needed for passage of the health care reform bill to assure its passage? Why wouldn't they want to give the same meticulois attention to our nation's health care proposals and carefully vet them? Wouldn't it be better to measure twice, and cut once?
Just asking.
-Wes
The Problems With Medical E-mail
Ask a business executive what they think about corporate e-mail, they'll tell you: "I love it! It's so efficient!"
As any nurse practitioner what they think about secure patient e-mail, they'll tell you: "I hate it. It's so inefficient."
So why the difference?
Perhaps because corporate e-mail is often one-way transmissions of information (broadcasting) so the information can often be ignored. We do not have the luxury of ignoring e-mails in medicine. These e-mails are always two-way, very personal communications, often about significant patient concerns. For nurses and doctors, there is a remarkable efficency in punching 10 munbers on a phone and speaking with the patient directly, or if they're not there, leaving a message acknowledging that you tried to connect. With e-mail, typing much more to compose an e-mail is just not as efficient as the spoken word and invariably takes much longer to craft a response that is accurate and grammatically correct.
Further, e-mail lacks the subtlties of the emotion conveyed with the spoken word. You can't hear the tremulous nature of the patient's voice or the patient's rapid breathing in the background. Worse, responses in e-mails might be misconstrued by the patient. Defusing such concerns quickly is impossible by back-and-forth e-mail communication. Finally, if the doctor or nurse has the caps-lock key depressed, IT MIGHT BE PERCEIVED THAT YOU ARE SHOUTING AT THEM!
Certainly, electronic communication has its advantages at times. Simple, quick questions that are reaffirmation of appointment times, clarifications, or reminders can be efficiently managed to everyone's satisfaction in medicine, but to look to e-mail as the way to cut office clerical staff as a means of cost-cutting, is missing the forest for the trees.
-Wes
As any nurse practitioner what they think about secure patient e-mail, they'll tell you: "I hate it. It's so inefficient."
So why the difference?
Perhaps because corporate e-mail is often one-way transmissions of information (broadcasting) so the information can often be ignored. We do not have the luxury of ignoring e-mails in medicine. These e-mails are always two-way, very personal communications, often about significant patient concerns. For nurses and doctors, there is a remarkable efficency in punching 10 munbers on a phone and speaking with the patient directly, or if they're not there, leaving a message acknowledging that you tried to connect. With e-mail, typing much more to compose an e-mail is just not as efficient as the spoken word and invariably takes much longer to craft a response that is accurate and grammatically correct.
Further, e-mail lacks the subtlties of the emotion conveyed with the spoken word. You can't hear the tremulous nature of the patient's voice or the patient's rapid breathing in the background. Worse, responses in e-mails might be misconstrued by the patient. Defusing such concerns quickly is impossible by back-and-forth e-mail communication. Finally, if the doctor or nurse has the caps-lock key depressed, IT MIGHT BE PERCEIVED THAT YOU ARE SHOUTING AT THEM!
Certainly, electronic communication has its advantages at times. Simple, quick questions that are reaffirmation of appointment times, clarifications, or reminders can be efficiently managed to everyone's satisfaction in medicine, but to look to e-mail as the way to cut office clerical staff as a means of cost-cutting, is missing the forest for the trees.
-Wes
Subscribe to:
Posts (Atom)