On Wednesday, the American Board of Internal Medicine (ABIM) quietly announced their much-anticipated "modifications" to their Maintenance of Certification program on their blog. As expected, rather than ending the MOC program, ABIM has decided to double down and justify their unproven process using an edited video of Skype sessions from their most fervent (paid) supporters.
The ABIM reportedly conducted invitation-only "listening sessions" accross the nation. On the basis of those sessions and months of focus groups and navel gazing, the ABIM unilaterally decided that an "open-book" examination that physicians must participate in every two years could serve as an "alternate pathway" to "maintain" a physician's (previously lifetime) Board certification. They then had the gall to say these were the changes we requested. They weren't.
In actuality, those "listening sessions"were invitation-only. (Yes, I applied to attend the one here in Chicago but was never granted an "invitation.") Selection bias of diplomates was the order of the day. And as their legal fees mount, ABIM has yet to mention what they plan to charge recertifying physicians for their new "pathway." Rest assured it will be plenty.
By now, practicing physicians understand what MOC is really about. It is NOT about making money, physician ongoing education, assuring physician competency, care quality, or patient safety.
MOC is about the control of physicians.
Control doctors and you control health care delivery. Control doctors and you can shape them to corporate ways. Don't like it, dear doctor? Then leave. We'll find someone else to take your place and your patients.
But replacing experienced physicians is not so easy. It takes years to gain credible experience in medicine. MOC is not about experience, it is about rote memorization and data entry. And what the ABIM doesn't get is referrals are still not always guided by who your employer is, as much as corporations and the government try to make it so with their consolidation attempts. They can "innovate" all the new ideas they want, but doctors are not fooled. Tie MOC to credentials or to insurance company payments if you want, but extortion is extortion, no matter how you color it. Because ABIM has not taken accountability for their serious financial transgressions and strongman tactics used to protect their monopoly, they will remain a pitiful example of corporate greed to practicing physicians (the people they claim to "help") and little else.
The Accreditation Council of Graduate Medical Education (ACCME) and their powerful member groups (The American Board of Medical Specialties, American Medical Association, American Hospital Association, the Council on Medical Subspecialty Societies and American Osteopathic Association) know billions of other reasons MOC is important, too. MOC generates about $2 billion in revenue annually for these organizations when one considers the endless board review classes and registration fees for their members. Condos, limo rides, first class airfare, gym memberships, and multimillion dollar golden parachutes are dependent on this program. All done without proof of value to doctors OR their patients. All done without any assessments of MOC's potential harms. The fact that our bureaucratic academic leadership in medicine will not address the many problems uncovered on this blog's pages and what this means to patient care in America is more even concerning than the ABIM's missteps in my opinion.
Doctors have had it with the outright dishonesty and scandal that has plagued MOC from the beginning, especially when they're dealing with much more important life-and-death issues every day. The only realistic and honorable revision for MOC is to end it, or for every practicing physician to refuse to participate and allow MOC to wallow in it's own avarice and greed.
-Wes
Friday, March 31, 2017
Tuesday, March 21, 2017
Fact Check on ABIM's Director of Investigations
On 9 February 2017, I received a note from the editor of Philadelphia Medicine magazine requesting that I respond to a letter they received from Sidney Baumgarten, Esq, a friend and counsel for Ariel Benjamin Mannes, the American Board of Internal Medicine (ABIM)'s Director of Investigations, whom I had mentioned in their publication dedicated to the ABIM that was released in December, 2016. Yesterday, Mr. Baumgarten's letter and my rebuttal appeared in the Spring 2017 issue (5 Mbytes) of Philadelphia Medicine magazine.
I have reproduced the contents of Mr. Baumgarten's original letter regarding Mr. Mannes and my rebuttal to his letter below:
* * *
Mr. Baumgarten's understanding of Mr. Mannes' background conflicts with publicly available information regarding Mr. Mannes' past. To the best of my knowledge and belief, Mr. Mannes' prior background, responsibilities, "intelligence gathering" tactics, access to ABIM diplomate personal information, law-enforcement connections, and salary at ABIM have never been disclosed to ABIM diplomates despite Mr. Mannes' important public role in the organization. Here is the response I sent to Phildelphia Medicine magazine regarding some of the verifiable facts I have found regarding his history (They requested I limit my response to 500 words):
I take no joy in disclosing the misdeeds of a fellow human being. While the writer of the letter to Philadelphia Medicine magazine seems to be concerned about his "friend and client" and describes his friend's past employment history as a mere "blip," he misses the point that 139 vulnerable physicians (and thousands more who received "letters of concern") had their entire careers threatened by the ABIM's strongman tactics using his "friend and client's" investigation techniques and connections. Those actions resulted in untold personal and professional anxiety, legal fees, and public humiliation before proper due process could occur. In many cases, physicians were forced to undergo ethics training and pay hefty fines to reinstate their board certification on the basis of the ABIM's felonious employee's carefully organized "investigation" so the leadership of the ABIM could maintain their monopoly, power, and lavish executive lifestyles. To then intimidate a person who tries to disclose the truth via a letter to a medical publication is a last-ditch tactic when there is no ground left to stand on.
Disclosing facts cannot be defined as "pillorying." In addition to the facts I outlined in my response to Mr. Baumgarten, it appears to me that Mr. Mannes used his experience with the Arora Board Review investigation to promote his test security techniques to the board members of the American Board of Medical Specialties (ABMS) in a course called "Building a Bulletproof Exam Integrity Case: Tools of the Trade" in 2012. Should physicians blindly permit the wanton breach of their civil liberties by individuals with Mr. Mannes' background and connections so other medical certifying boards can also profit using similar techniques?
Mr. Mannes had other conflicts of interest while an employee at ABIM: he worked for the test security firm, Caveon, teaching techniques of "responding to and investigating test-security incidents" to others. Mr. Mannes even created his own corporation, Exam Integrity Services, LLC, in Florida in 2015. How much more profit did Mr. Mannes hope to gain at the expense of ABIM's physician reprisals while working as their employee?
Recently, we have come to learn that the ABIM sued one physician more than two years after the statute of limitations had expired on the 2009 Arora Board Review copyright infringement case that Mr. Mannes investigated under the direction of ABIM officers. The court recently dismissed the claim after the physician (Dr. Salas Rushford) was forced to endure years of stress and expense inflicted by the ABIM. For reasons that are unclear, Mr. Mannes' deposition in that case (for which I serve as an expert witness on behalf of Dr. Salas Rushford) has been kept under seal to the public, yet the deposition of Dr. Salas Rushford has not. Why? It seems the ABIM is an entity that has grown disproportionate authority over physicians without any meaningful accountability or transparency, and which we now see can abuse its power to inflict untold harm against physicians who are trying to serve patients.
How, where, when, and why unaccountable physician certifying bodies can retaliate against or sue physicians by intruding upon their personal property and civil liberties on the basis of an unproven promise of assuring "patient safety and physician quality" is one of society's most delicate and grave decisions. Certainly ABIM knows this but seeks to reduce working physicians' many concerns about their conflicted financial and investigational activities to a name-calling problem. While I admire the cleverness of this strategy, the genie is out of the bottle. Their attempt to make their reality a personal issue against me is deceptive. Tens of thousands of US physicians have my same concerns and want answers from the ABIM and the American Board of Medical Specialties. In addition, an entire state medical society has issued a vote of no confidence against the ABIM at the House of Delegates meeting in Chicago in June 2016, and the entire House of Delegates voted to end Maintenance of Certification (MOC) on the basis of lack of evidence of the need for MOC and the ABIM's financial and strongman actions. Despite this, the leadership of the American Medical Association has still not ended the ABMS Maintenance of Certification (MOC) program. Consequently, practicing physicians are mobilizing nationwide to enact state-level legislation to end the corrupt MOC program that is tied to hospital credentialing and the ability of physicians to receive insurance payments in many states and, therefore, to practice their trade.
French philosopher Foucault's work on power helps us understand why the physician certification industry, and Maintenance of Certification in particular, is so important to the US medical education system and for policy makers today:
It is unacceptable to continue the half-truths and false representations of physician certification (and recertification's) value to our health care system. The ABIM and ABMS must take full accountability for their actions and reform the methods they are willing to employ to assure their revenues at the expense of the personal liberties of practicing physicians and stop using individuals like Mr. Mannes as their strongman and fall guy.
-Wes
I have reproduced the contents of Mr. Baumgarten's original letter regarding Mr. Mannes and my rebuttal to his letter below:
December 27, 2016
Philadelphia Medicine Magazine
c/o Philadelphia County Medical Society
Alan J. Miceli, Editor
2100 Spring Garden St.
Philadelphia PA 19130
Dear Mr. Miceli,
I am writing this letter hoping that you will give it serious consideration and make it available to the members of the Society as well as those who read your publication.
I have been a friend and counsel to Ariel Benjamin Mannes, the Director of Investigations (formerly Test Security) at the American Board of Internal Medicine (ABIM), for many years. I must say, candidly, that with over 50 years of law practice I have never before seen the likes of the repeated attempts by Dr. Westby G. Fisher to malign a person based upon an 11-year old “blip” in his long and successful career of public trust. It is, to be sure, unconscionable, to be using invective to shame the ABIM and, along the way, destroying the career and good name of a very honest, competent person, I know that if a member physician were similarly treated you would be mounting the ramparts to obviate its harm to his/her career.
First, Mr. Mannes was a member of the DC Police Department with a very fine record of service. He had been on a leave of absence and was awaiting reinstatement to duty while working part time at a DC restaurant when the incident in question occurred. That night, Mr. Mannes intervened in an altercation and himself called the police for assistance and was in possession of a legally licensed handgun from Virginia where he lived, but not technically permitted then in DC. His arrest and conviction was solely for illegal possession of the weapon; one felony, not two as Dr. Fisher alleges.
Interestingly, Ben’s employment appeal was won and he was reinstated to the DC Police, and was ordered prior to the incident and was successfully reinstated, our legal view was that he was a de facto police officer at the time of the incident. It should also be noted that the very law Mr. Mannes plead guilty to was later declared unconstitutional by the Supreme Court.
Second, Ben had served with the US Department of Homeland Security on a TSA-led rail inspection team with a security clearance, even on the night of the incident. He had also held roles before moving to DC with the US Federal Protective Service in New York following the first World Trade Center bombing trials and the CAT Eyes program where he trained police instructors on anti-terrorism in multiple jurisdictions. Even after the aforementioned incident he worked as a contractor on homeland security technology initiatives in Los Angeles, Ohio and the Philadelphia region. In multiple instances, Mr. Mannes was able to assist me in my role as Chief of Staff of the Army Division of the New York Guard after 9/11. In fact, his intelligence gathering enabled us in New York to be forewarned of serious threats.
Third, because Ben was a resident of New York for many years, he was able to obtain a Certificate of Relief from Disabilities issued by the State of New York several years ago, which relieved him of any impediments to employment, etc. as a result of his plea and conviction.
Finally, our laws here in New York (where Mr. Mannes’ certificate was issued) prohibit discrimination against a person who has one criminal conviction. It is codified in our Human Rights Law and our Correction Law. Both are designed to prevent the stigma of one arrest from interfering with future employment.
As you can see, the one incident revealed nothing that would even suggest any form of dishonesty of other reason for the ABIM to reject his services. Mr. Mannes’ position was designed with a myriad of checks and balances and his casework, to include the one cited in your publication, have been upheld in courts of law on numerous occasions. Mr. Mannes is a consummate professional, active in the federal and local security community, who has made the appropriate disclosures in both his pre-employment background check at ABIM and the vetting process for appointments he has held since, to include his elected Governorship at Infragard, a public private partnership coordinated by the FBI.
To put it bluntly. Mr. Mannes is being unfairly pilloried to serve Dr. Fisher’s own differences with the ABIM. It is especially unseemly for the member of a highly respected profession to undertake the willful destruction of another human being for his own motives. Mr. Mannes has worked extremely hard over the last 11 years to undo the unfortunate incidents of one night and surely does not deserve to have his family, friends, and colleagues read disparaging, inaccurate things about him in the pages of your publication. I am sure Hippocrates would blush.
Sincerely,
Sidney Baumgarten, Esq.
Former Deputy Mayor, City of New York
Brigadier General, NYG, Retired
Cc: Hoffman Publishing Group
* * *
Mr. Baumgarten's understanding of Mr. Mannes' background conflicts with publicly available information regarding Mr. Mannes' past. To the best of my knowledge and belief, Mr. Mannes' prior background, responsibilities, "intelligence gathering" tactics, access to ABIM diplomate personal information, law-enforcement connections, and salary at ABIM have never been disclosed to ABIM diplomates despite Mr. Mannes' important public role in the organization. Here is the response I sent to Phildelphia Medicine magazine regarding some of the verifiable facts I have found regarding his history (They requested I limit my response to 500 words):
"Contrary to what Sidney Baumgarten, Esq. claims, Ariel Benjamin Mannes does not have a 'fine record of service with the DC police department.' In 2003, Mannes admitted using his access as an officer to obtain Washington reporter Jason Cherkis's personal records and posting the information on a law enforcement website advocating reprisals. The disciplinary board decided unanimously to fire Mannes for conduct unbecoming, but took more than 55 days to notify him.These kinds of threats and attempts to discredit me are a dark example of organized medicine's ethics today. It is also a stark example of the tactics members of the American Board of Internal Medicine (ABIM) will deploy to control the narrative about them.
While on involuntary leave from D.C. Police pending investigation, Mannes began working for the TSA Railroad Division and moonlighted as a bouncer at the “Diva nightclub.” Mannes assaulted a Diva nightclub patron while carrying a loaded unregistered pistol and claiming he was a police officer. Mannes was charged with aggravated assault, impersonating a police officer, and carrying an unregistered firearm.
Per D.C. Court records (felony #006438), Mannes pleaded guilty on December 2005 to two charges from the nightclub incident: (a) impersonating a police officer and (b) carrying an unregistered firearm, and was sentenced to pay fines for each conviction and to probation. He lost his weapon and TSA employment because of this incident.
Police Chief Cathy Lanier was forced to rehire Mannes in November 2008 due solely to the notification issue, but then suspended him. The Department moved again to fire him because of his weapons charge.
Mannes lost his appeal of his two convictions on 10/21/2008, the same year he began working as Director of Test Security for the ABIM.
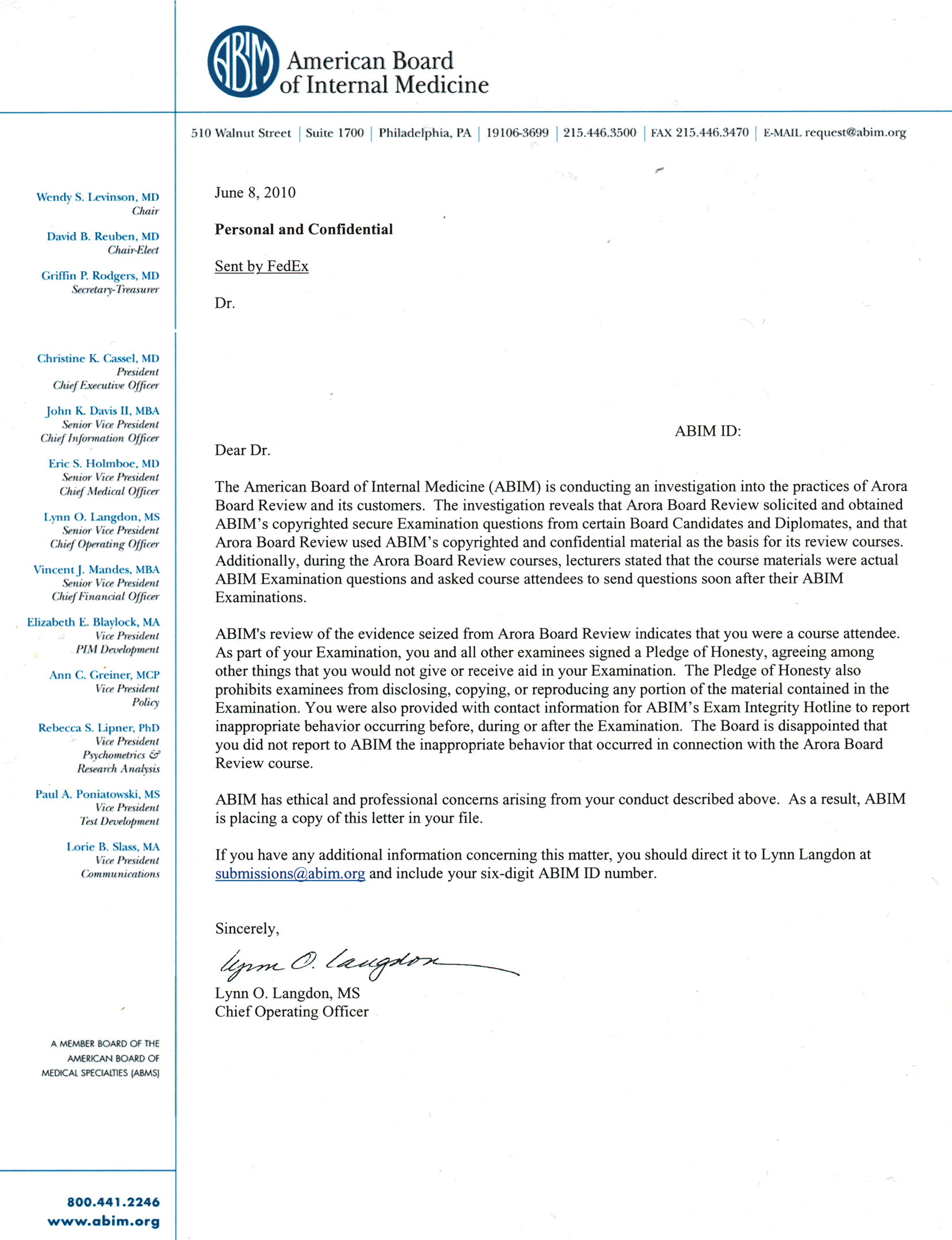
While at the ABIM, Mannes’ declaration before a federal judge was instrumental for the ABIM to obtain a temporary retraining and seizure order in ABIM’s investigation of the Arora Board Review (ABR) course on December 2, 2009. Mannes, ABIM lawyers, and U.S. Marshals seized materials from Dr. Arora’s home days later. Using emails from Arora’s computers, ABIM retaliated against 139 physicians and sued others and then issued a press release June 9, 2010 accusing physicians of unethical "brain dumping" before due process could occur.
In summary, Mannes was disciplined by the D.C. Police for abusing his position of authority to access confidential information to retaliate against an innocent citizen. Such conduct was not acceptable to the DC Police, and yet it appears to be acceptable to ABIM while it falsely accuses physicians of acting unethically. ABIM's double standard should be exposed as long as it continues to harm physicians.
I take no joy in disclosing the misdeeds of a fellow human being. While the writer of the letter to Philadelphia Medicine magazine seems to be concerned about his "friend and client" and describes his friend's past employment history as a mere "blip," he misses the point that 139 vulnerable physicians (and thousands more who received "letters of concern") had their entire careers threatened by the ABIM's strongman tactics using his "friend and client's" investigation techniques and connections. Those actions resulted in untold personal and professional anxiety, legal fees, and public humiliation before proper due process could occur. In many cases, physicians were forced to undergo ethics training and pay hefty fines to reinstate their board certification on the basis of the ABIM's felonious employee's carefully organized "investigation" so the leadership of the ABIM could maintain their monopoly, power, and lavish executive lifestyles. To then intimidate a person who tries to disclose the truth via a letter to a medical publication is a last-ditch tactic when there is no ground left to stand on.
{kind=link}
{kind=link}
Disclosing facts cannot be defined as "pillorying." In addition to the facts I outlined in my response to Mr. Baumgarten, it appears to me that Mr. Mannes used his experience with the Arora Board Review investigation to promote his test security techniques to the board members of the American Board of Medical Specialties (ABMS) in a course called "Building a Bulletproof Exam Integrity Case: Tools of the Trade" in 2012. Should physicians blindly permit the wanton breach of their civil liberties by individuals with Mr. Mannes' background and connections so other medical certifying boards can also profit using similar techniques?
Mr. Mannes had other conflicts of interest while an employee at ABIM: he worked for the test security firm, Caveon, teaching techniques of "responding to and investigating test-security incidents" to others. Mr. Mannes even created his own corporation, Exam Integrity Services, LLC, in Florida in 2015. How much more profit did Mr. Mannes hope to gain at the expense of ABIM's physician reprisals while working as their employee?
Recently, we have come to learn that the ABIM sued one physician more than two years after the statute of limitations had expired on the 2009 Arora Board Review copyright infringement case that Mr. Mannes investigated under the direction of ABIM officers. The court recently dismissed the claim after the physician (Dr. Salas Rushford) was forced to endure years of stress and expense inflicted by the ABIM. For reasons that are unclear, Mr. Mannes' deposition in that case (for which I serve as an expert witness on behalf of Dr. Salas Rushford) has been kept under seal to the public, yet the deposition of Dr. Salas Rushford has not. Why? It seems the ABIM is an entity that has grown disproportionate authority over physicians without any meaningful accountability or transparency, and which we now see can abuse its power to inflict untold harm against physicians who are trying to serve patients.
How, where, when, and why unaccountable physician certifying bodies can retaliate against or sue physicians by intruding upon their personal property and civil liberties on the basis of an unproven promise of assuring "patient safety and physician quality" is one of society's most delicate and grave decisions. Certainly ABIM knows this but seeks to reduce working physicians' many concerns about their conflicted financial and investigational activities to a name-calling problem. While I admire the cleverness of this strategy, the genie is out of the bottle. Their attempt to make their reality a personal issue against me is deceptive. Tens of thousands of US physicians have my same concerns and want answers from the ABIM and the American Board of Medical Specialties. In addition, an entire state medical society has issued a vote of no confidence against the ABIM at the House of Delegates meeting in Chicago in June 2016, and the entire House of Delegates voted to end Maintenance of Certification (MOC) on the basis of lack of evidence of the need for MOC and the ABIM's financial and strongman actions. Despite this, the leadership of the American Medical Association has still not ended the ABMS Maintenance of Certification (MOC) program. Consequently, practicing physicians are mobilizing nationwide to enact state-level legislation to end the corrupt MOC program that is tied to hospital credentialing and the ability of physicians to receive insurance payments in many states and, therefore, to practice their trade.
French philosopher Foucault's work on power helps us understand why the physician certification industry, and Maintenance of Certification in particular, is so important to the US medical education system and for policy makers today:
Discipline, according to Foucault’s historical and philosophical analyses, is a form of power that tells people how to act by coaxing them to adjust themselves to what is ‘normal’. It is power in the form of correct training. Discipline does not strike down the subject at whom it is directed, in the way that sovereignty does. Discipline works more subtly, with an exquisite care even, in order to produce obedient people. Foucault famously called the obedient and normal products of discipline ‘docile subjects’.Mr. Baumgarten's letter and the ABIM's strongman actions demonstate how the overreach of our US physician credentialing system can adversely affect the very people they pretend to protect: physicians and their patients. To limit a physicians' ability to think critically and care autonomously for their patients creates dangerous consequences for both caregivers and their patients. Health care administrators and policy makers would be wise to assure physicians continue to be able to speak independently and on behalf of their patients lest they fall prey to the same forces when they become patients themselves.
It is unacceptable to continue the half-truths and false representations of physician certification (and recertification's) value to our health care system. The ABIM and ABMS must take full accountability for their actions and reform the methods they are willing to employ to assure their revenues at the expense of the personal liberties of practicing physicians and stop using individuals like Mr. Mannes as their strongman and fall guy.
-Wes
Friday, March 17, 2017
Federal Judge Dismisses ABIM Copyright Infringement Suit
Yesterday, US District Judge Katherine Hayden dismissed the instant copyright infringement action filed by the American Board of Internal Medicine (ABIM) against defendent Jaime Salas Rushford MD because the action was time-barred by its three-year statute of limitations.
Background
The ruling stems from a December 2009 complaint filed by the ABIM against Rajender K. Arora who conducted a live six-day board review course called the Arora Board Review (ABR) course in May 2009 in Livingston, NJ. Around that time, ABIM discovered test questions on ABR's website that ABIM suspected were copied from its prior examinations. ABIM filed their complaint that Arora, ABR, and an ABR employee, Anise Kachadourian, alleging a scheme through which "ABR unlawfully obtained ABIM's secure examination items by mobilizing course attendees to divuldge contents of the examination to defendents" in violation of federal copyright law. The December 2009 complaint also named 50 John Doe defendents "a presently unknown member of past and/or present candidates for Board Certification who have complied with this requests of defendents Arora and Kachadourian to provide secure, copyrighted examination content to Arora for further dissemination." (Note: the issue of ABIM claiming violations of copyright law are solely those of ABIM and were not addressed by the judge in her opinion, but rather the motion to dismiss was made taking everything the ABIM said was true and giving all the inferences they made in their favor.)
On the same day that it filed the December 2009 complaint, ABIM successfully obtained an ex parte order from the district court authorizing United States Federal Marshal to "break open and/or forcibly enter" the individual defendents' homes and seize, among other things, all communications with ABR's customers relating to infringement of ABIM's copyrighted examination. This action later led to national headlines in June 2010 that claimed "doctors cheated."
According to the ruling: "As a result of the seizure, ABIM obtained a trove of emails between Arora and various course attendees. The lawsuit against Arora was settled in June, 2010, and according to counsel, ABIM began instituting action against individual physicians whom ABIM deemed complicit with Arora and ABR. According to the complaint eventually filed in court, ABIM identified Jaime Salas Rushford in January 2012 as one of ABR's alledgedly complicit customers, when it linked him to an e-correspondence about August 2009 exam questions that was sent from the email address "padrinojr@yahoo.com." Salas allegedly began compiling detailed ABIM examination content that he got from colleagues who sat for the examination leading up to his own examination date 20 August 2009 and sent it to Arora using the padrinojr@yahoo.com email address."
ABIM then waited until October 2014 to file the current action against him in October 2014, even though they knew the identity of Salas Rushford in January 2012, eight months before the three-year statute of limitations for their action against Arora ended. (ABIM argued that the three-year statute of limitations did not begin until January 2012 when the identified Salas Rushford as the owner of the padrinojr@yahoo.com email address.) In fact, the judge noted "ABIM made an intentional decision not to bring suit against Salas within the applicable limitations period when the alledged facts clearly show it was capable of doing so." Judge Hayden goes on to say that "this lawsuit against Salas is a coda to the main thrust of ABIM's litigation efforts, apparently born of a second look at the decision ABIM made not to sue Salas when his name popped up in January 2012."
At the time Salas Rushford was sued by ABIM in 2014, he filed a counterclaim, not only against ABIM, but against Richard Baron, MD, Christine Cassel, MD, Lynn O. Langdon, Eric Holmbie, MD, and members of an alleged ABIM "Hearing Panel" comprised of David Coleman, MD, Joan M. Von Feldt, MD, and Naomi O'Grady, MD. He also included ABIM's insurance companies and Pearson Education Inc. in the counterclaim. That counterclaim now proceeds.
Implications
The implications of the decision by the Judge Hayden yesterday are signficiant for a large portion of practicing US physicians and for the the financial solvency of the ABIM. According to its most recently-available Fiscal Year 2015 federal tax forms, the ABIM has a deficit of $50,642,980. Currently, their website lists the ABIM's FY 2016 expenses at $62.5 million, $2.5 million more than their federal tax form disclosed for fiscal year 2015. Legal expenses are signficiantly contributing to these expenses, not just "strategic non-capitalized spending on infrastructure upgrades in anticipation of the launch of a new MOC assessment in 2018" as ABIM claims on its website.
How much higher can these expenses be allowed to go? Who shoulders these expenses?
Physicians do.
From 2000 to 2014, the cost of board certification has increased 244% (16.3%/year) from $795 to $1940 for general internists and 257% (17.2%/yr) from $995 to $2560 for specialists. This year, candidates sitting for their initial board certification in cardiac electrophysiology had to pay $2830 to register for their examination.
If things continue the way they are, the countersuit by Salas Rushford will be the least of the ABIM's legal and financial concerns as doctors come together to act collectively on their own behalf.
-Wes
Disclaimer: I serve as an expert witness for Jaime Salas Rushford, MD and am a co-founder of Practicing Physicians of America, a physician advocacy organization.
Background
The ruling stems from a December 2009 complaint filed by the ABIM against Rajender K. Arora who conducted a live six-day board review course called the Arora Board Review (ABR) course in May 2009 in Livingston, NJ. Around that time, ABIM discovered test questions on ABR's website that ABIM suspected were copied from its prior examinations. ABIM filed their complaint that Arora, ABR, and an ABR employee, Anise Kachadourian, alleging a scheme through which "ABR unlawfully obtained ABIM's secure examination items by mobilizing course attendees to divuldge contents of the examination to defendents" in violation of federal copyright law. The December 2009 complaint also named 50 John Doe defendents "a presently unknown member of past and/or present candidates for Board Certification who have complied with this requests of defendents Arora and Kachadourian to provide secure, copyrighted examination content to Arora for further dissemination." (Note: the issue of ABIM claiming violations of copyright law are solely those of ABIM and were not addressed by the judge in her opinion, but rather the motion to dismiss was made taking everything the ABIM said was true and giving all the inferences they made in their favor.)
On the same day that it filed the December 2009 complaint, ABIM successfully obtained an ex parte order from the district court authorizing United States Federal Marshal to "break open and/or forcibly enter" the individual defendents' homes and seize, among other things, all communications with ABR's customers relating to infringement of ABIM's copyrighted examination. This action later led to national headlines in June 2010 that claimed "doctors cheated."
According to the ruling: "As a result of the seizure, ABIM obtained a trove of emails between Arora and various course attendees. The lawsuit against Arora was settled in June, 2010, and according to counsel, ABIM began instituting action against individual physicians whom ABIM deemed complicit with Arora and ABR. According to the complaint eventually filed in court, ABIM identified Jaime Salas Rushford in January 2012 as one of ABR's alledgedly complicit customers, when it linked him to an e-correspondence about August 2009 exam questions that was sent from the email address "padrinojr@yahoo.com." Salas allegedly began compiling detailed ABIM examination content that he got from colleagues who sat for the examination leading up to his own examination date 20 August 2009 and sent it to Arora using the padrinojr@yahoo.com email address."
ABIM then waited until October 2014 to file the current action against him in October 2014, even though they knew the identity of Salas Rushford in January 2012, eight months before the three-year statute of limitations for their action against Arora ended. (ABIM argued that the three-year statute of limitations did not begin until January 2012 when the identified Salas Rushford as the owner of the padrinojr@yahoo.com email address.) In fact, the judge noted "ABIM made an intentional decision not to bring suit against Salas within the applicable limitations period when the alledged facts clearly show it was capable of doing so." Judge Hayden goes on to say that "this lawsuit against Salas is a coda to the main thrust of ABIM's litigation efforts, apparently born of a second look at the decision ABIM made not to sue Salas when his name popped up in January 2012."
At the time Salas Rushford was sued by ABIM in 2014, he filed a counterclaim, not only against ABIM, but against Richard Baron, MD, Christine Cassel, MD, Lynn O. Langdon, Eric Holmbie, MD, and members of an alleged ABIM "Hearing Panel" comprised of David Coleman, MD, Joan M. Von Feldt, MD, and Naomi O'Grady, MD. He also included ABIM's insurance companies and Pearson Education Inc. in the counterclaim. That counterclaim now proceeds.
Implications
The implications of the decision by the Judge Hayden yesterday are signficiant for a large portion of practicing US physicians and for the the financial solvency of the ABIM. According to its most recently-available Fiscal Year 2015 federal tax forms, the ABIM has a deficit of $50,642,980. Currently, their website lists the ABIM's FY 2016 expenses at $62.5 million, $2.5 million more than their federal tax form disclosed for fiscal year 2015. Legal expenses are signficiantly contributing to these expenses, not just "strategic non-capitalized spending on infrastructure upgrades in anticipation of the launch of a new MOC assessment in 2018" as ABIM claims on its website.
How much higher can these expenses be allowed to go? Who shoulders these expenses?
Physicians do.
From 2000 to 2014, the cost of board certification has increased 244% (16.3%/year) from $795 to $1940 for general internists and 257% (17.2%/yr) from $995 to $2560 for specialists. This year, candidates sitting for their initial board certification in cardiac electrophysiology had to pay $2830 to register for their examination.
If things continue the way they are, the countersuit by Salas Rushford will be the least of the ABIM's legal and financial concerns as doctors come together to act collectively on their own behalf.
-Wes
Disclaimer: I serve as an expert witness for Jaime Salas Rushford, MD and am a co-founder of Practicing Physicians of America, a physician advocacy organization.
Sunday, March 05, 2017
MOCA-Peds and Its Conflicts of Interest
The pediatric Maintenance of Certification (MOC) propaganda machine rolls on - this week in the JAMA Pediatrics.
These authors need to understand the days of pulling the wool over working physicians' eyes by publishing opinion pieces in journals sponsored by the AMA that has refused to end MOC despite recommendations made by their own House of Delegates are over. These continued efforts to justify MOC without acknowledging the programs many flaws and financial conflicts of interest must end. While physicians who chose to continue to work have little choice but to participate in MOC currently, efforts are underway across the nation to end MOC for all subspecialties on the basis of its discriminatory practice against younger physicians and because its adverse effects on physicians and their patients have never been studied (or even acknowledged) by these organizations that profit from the program without legitimate independent oversight.
-Wes
Lewis R. First, MD, MS, David A Gremse, MD, and Joseph W. St. Geme, III, MD join forces to publish their opinion piece entitled "Maintenance of Certification - A Prescription for Improved Child Health" in JAMA Pediatrics on 27 Feb 2017. The only conflicts of interests they disclose to the public are their various associations with their institutions and various professional medical organizations with which they have been affiliated with over the years. As is typical for many of the JAMA publications published by the American Medical Association (AMA), they failed to disclose their ties to the pharmaceutical industry or the fact that annual Maintenance of Certification (MOC) revenues almost matches that of initial certification for the American Board of Pediatrics (ABP) every year.
Lewis R. First, MD, MS advertises himself as restricting this practice to inpatients only on his University of Vermont website. Such a practice is hardly representative to the vast majority of pediatricians in the U.S. who primarily care for outpatients. It would not be surprising, then, that the hours required to participate in MOC would seem trivial to one who works in a sheltered inpatient workshop. He never mentions that he "won" the Joseph St. Geme Jr. Leadership award created in the honor of the father of his co-author, Joseph St. Geme III, MD, by the Academic Pediatric Association, American Academy of Pediatrics, American Pediatric Society, the Association of Medical School Pediatric Department Chairs (AMSPDC), the Association of Pediatric Program Chairs and the Society for Pediatric Research. To his credit, Dr. First does disclose the fact that the is chair of the AMSPDC Education Committee, member of the ABP Research Advisory Committee, member of the AMSPDC Planning Committee, editor of Pediatrics, and past chair of the National Board of Medical Examiners, so his enthusiasm for lifelong repeated testing of physicians is at least understandable as part of the vast network of Accreditation Council of Graduate Medical Education (ACGME) certification member organizations' fixation with lifelong testing and revenue generation.
David A Gremse, MD disclosed that he is chair of the department of pediatrics at South Alabama University, chair-elect of the ABP, member of the AMSPDC Planning Committee, and past member of the AMSDPC Board of Directors. He failed to mention that he was secretary-treasurer of the ABP and a pediatric gastroenterologist.
Finally Joseph W. St. Geme III, MD discloses he is chair of the department of pediatrics at the Children's Hospital of Philadelphia and the University of Pennsylvania, associate chair of the AMSPDC Research Committee, immediate past chair of the ABP (often with first class travel from the ABP) and Dr. St. Geme failed to mention his advisory role with PureTech Health, a "cross-disciplinary biopharmaceutical company."
Why mention these conflicts? Because their article is filled with misinformation.
First, board certification for pediatricians in America is no longer "voluntary"as these authors claim. It is disingenuous for them to claim board certification is "voluntary" when the next sentence they note "Hospitals increasingly require board certification for medical staff privileges credentialing bodies and payers often require board certification for participation in provider networks and for reimbursement."
Two "Quality Improvement" projects are mentioned by the authors that they claim can be used to justify Maintenance of Certification to all general pediatricians in the United States. These studies were less than robust and filled with uncontrolled endpoints. For instance, one involved a QI project with the "ImproveCareNow Collaborative" funded by many pharmaceutical companies and the American Board of Pediatrics Foundation that actually admitted in their paper:
First, board certification for pediatricians in America is no longer "voluntary"as these authors claim. It is disingenuous for them to claim board certification is "voluntary" when the next sentence they note "Hospitals increasingly require board certification for medical staff privileges credentialing bodies and payers often require board certification for participation in provider networks and for reimbursement."
Two "Quality Improvement" projects are mentioned by the authors that they claim can be used to justify Maintenance of Certification to all general pediatricians in the United States. These studies were less than robust and filled with uncontrolled endpoints. For instance, one involved a QI project with the "ImproveCareNow Collaborative" funded by many pharmaceutical companies and the American Board of Pediatrics Foundation that actually admitted in their paper:
'Third, improvements in outcome occurring over time could have taken place independent of changes in care delivery as part of the network. No external comparator group was available to help with this determination. However, not all centers showed improvement, and the improvement we observed took place over a relatively short period of time during which no new therapies were introduced into routine clinical practice. Finally, the processes we measured may not be directly responsible for the observed improvement in remission."In fiscal year 2015 (from the 2014 IRS Form 990) - the latest tax form the public can review - the American Board of Pediatrics earned $10,644,504 from the Maintenance of Certification program while their senior executives enjoyed first class airfare and paid spousal travel fees. They paid their former President and CEO who worked only 8 hours per week, James Stockman, III, MD, $793,991 - more money than their current highest paid employees, Executive Vice President of Credentialing and Exam Administration ($675,055) and President and CEO ($624.001). By comparison, one source cites the current median pediatrician salary in the US in 2017 as $187,376. Might these facts be more important to explain the authors' enthusiasm for promoting MOC than the flawed studies they cite regarding MOC's importance to patient care?
These authors need to understand the days of pulling the wool over working physicians' eyes by publishing opinion pieces in journals sponsored by the AMA that has refused to end MOC despite recommendations made by their own House of Delegates are over. These continued efforts to justify MOC without acknowledging the programs many flaws and financial conflicts of interest must end. While physicians who chose to continue to work have little choice but to participate in MOC currently, efforts are underway across the nation to end MOC for all subspecialties on the basis of its discriminatory practice against younger physicians and because its adverse effects on physicians and their patients have never been studied (or even acknowledged) by these organizations that profit from the program without legitimate independent oversight.
-Wes
Saturday, March 04, 2017
TeamHealth: Medicine's "Big Short"

Remember how he played Elvis and sang "Your Hospitalist Song" at Mandalay Casino while serving on the board of IPC The Hospitalist Company in 2014?
Remember how Dr Wachter pivoted to "love" as a quality measure in the New York Times after leaving the American Board of Internal Medicine (ABIM) and after he quietly earned $210,586 in income, stock, and options with IPC Hospitalist Company in 2014, a portion of which was shared with his institution?
Remember how IPC Hospitalist was being investigated by the DOJ for Medicare fraud?
Remember how IPC Hospitalist Company was acquired by TeamHealth for a hefty profit anyway?
The DOJ's investigation completed and TeamHealth had a $60M judgement levied against it.
I went to look what happened to TeamHealth's stock price at the time of that announcement, but was surprised to see that TeamHealth had disappeared from the New York Stock Exchange.
It seems TeamHealth had been purchased by The Blackstone Group and became a private company just before the judgement was handed down.
* poof *
IPC Hospitalist Company. TeamHealth. All gone. All forgotten.
Welcome to US Medicine's mini-version of "The Big Short."
-Wes
More here: http://fortune.com/2016/10/31/blackstone-teamhealth-merger/
Subscribe to:
Posts (Atom)