As a follow-up of my earlier post on the American Board of Medical Specialties' (ABMS) Maintenance of Certification™(MOC™) program's tax on medical education, I was sent the "approved" responses of two different physicians that were required to answer questions to "earn" ABMS MOC™credits from the Heart Rhythm Society (HRS) Scientific Sessions after the meeting. These responses were "approved" by an HRS "reviewer" so the doctors could apply these points to remain "Board certified" and employed with their hospital systems. Each doctor had to write between 50 and 100 words (no more, no less) in response to questions posed by the ABIM. Despite their different responses, each received the exact same "feedback" that included links to various Heart Rhythm Society, American College of Cardiology, AMA, ABMS and non-governmental organizations' policies and web pages.
(See Physician 1's responses here and Physician 2's responses here.)
Given these canned responses to these physicians feedback, how is this time-consuming, costly, and meaningless "feedback" exercise for "earning" MOC™ points anything but a self-paid advertorial for the HRS, ACC, AMA, ABMS, and other non-governmental organizations?
It is a sad commentary that our own subspecialty societies legitimize this corrupt process despite all that we know about it today.
-Wes
Showing posts with label Heart Rhythm Society. Show all posts
Showing posts with label Heart Rhythm Society. Show all posts
Saturday, May 19, 2018
Saturday, May 12, 2018
Taxing Medical Education with MOC
I just received this in my email in-basket from an attendee at this year's Heart Rhythm Society (HRS) Scientific Sessions:
MOC® is little more than taxation of physicians without representation.
(And we still don't have ABIM's financials from 2017 for the public's review.)
-Wes
I just got back from our annual EP meeting (HRS) which was in Boston. As you can imagine, the entire CME process has been bastardized to monetize the ABIM (American Board of Internal Medicine). After dutifully checking off which sessions I attended and rating the speakers, I noted a few things.Yes. It. Is.
Firstly, all attendees were electronically tracked with RFID tags. Our attendance at the sessions were electronically tracked and automatically noted. A pretty neat feature and designed, I think, to prevent fraudulent CME behavior.
We had to answer a separate ABIM Maintenance of Certification (MOC) section and actually provide prose with a minimum and maximum word count. There was a warning stating that the content of our replies would be reviewed before the ABIM would bless them for the MOC process.
Which begs the question. Under what circumstances does the ABIM have the authority to legitimize or delegitimize my reply to their nonsensical questions? The MOC portion of the CME conversion was more of a sampling of my opinion. Is this the new MOC paradigm: impose an educational tax on our meetings and then also charge a toll on their MOC highway?
This process is not only corrupt and inefficient; it is now surreal and insane.
MOC® is little more than taxation of physicians without representation.
(And we still don't have ABIM's financials from 2017 for the public's review.)
-Wes
Friday, June 24, 2016
Heart Rhythm Society Waffles on MOC
On Thursday (yesterday), I received this notice from the Heart Rhythm Society (HRS) concerning their stance on the American Board of Medical Specialty's (ABMS) Maintenance of Certification (MOC) referendum at the recent AMA House of Delegates meeting held in Chicago:
While the Heart Rhythm Society states the resolutions "are consistent with the HRS concerns and commitment for changes to the MOC program," it appears they do not understand that the House of Delegates overwhemingly resolved to end Maintenence of Certification immediately:
This does not mean studying the ABMS MOC program, it means ending it.
And this certainly does not mean supporting the AMA with our dues when they fail to act in the practicing physicians' best interests either.
Look, it is now abundantly clear that the ABIM did many, many illegal and self-serving activities with our diplomat fees for (at least) the past 27 years. And when they were caught red-handed with their hand lodged in the practicing physician's personal liberty and financial cookie jar, they tried (and continue to try) to cover it up. What they've done is illegal in many fronts. This is not acceptable and none of us need to "change" MOC or perform "another study" on MOC (funded by our dues) to sweep these actions under the rug. MOC just needs to end immediately.
I worry that the HRS leadership doesn't understand how angry practicing physicians are about what has transpired behind our backs as we've struggled to do the yeoman's work of patient care.
Here's the deal: if the HRS wants my dues for another year going forward, move to end MOC now. Put your actions where our money is. Otherwise, I'll save my hard-earned assets for other things besides supporting groups who don't support those of us on the front line of health care who obey the law and prefer to manage our profession ethically and transparently, rather than through political channels using threats and intimidation as their modus operandi.
-Wes
"The American Medical Association (AMA) House of Delegates recently approved resolutions addressing concerns about the American Board of Medical Specialties' (ABMS) MOC program at its annual meeting.I found this notice puzzling.
The resolutions are consistent with the HRS concerns and commitment to advocate for changes to the Maintenance of Certification (MOC) program. HRS currently has a representative in the AMA House of Delegates. To ensure that HRS maintains its seat at the AMA House of Delegates, the Society must demonstrate that 20 percent of the Society’s U.S. physician members are also members of the AMA.
The AMA also approved the commissioning of a study that will evaluate the impact of MOC and Maintenance of Licensure requirements on physicians. This study addresses the heart of the debate and HRS looks forward to the results of this important study."
While the Heart Rhythm Society states the resolutions "are consistent with the HRS concerns and commitment for changes to the MOC program," it appears they do not understand that the House of Delegates overwhemingly resolved to end Maintenence of Certification immediately:
"RESOLVED, That our American Medical Association call for the immediate end of any mandatory, secured recertifying examination by the American Board of Medical Specialties (ABMS) or other certifying organizations as part of the recertification process for all those specialties that still require a secure, high-stakes recertification examination."This does not mean changing the ABMS MOC program, it means ending it.
This does not mean studying the ABMS MOC program, it means ending it.
And this certainly does not mean supporting the AMA with our dues when they fail to act in the practicing physicians' best interests either.
Look, it is now abundantly clear that the ABIM did many, many illegal and self-serving activities with our diplomat fees for (at least) the past 27 years. And when they were caught red-handed with their hand lodged in the practicing physician's personal liberty and financial cookie jar, they tried (and continue to try) to cover it up. What they've done is illegal in many fronts. This is not acceptable and none of us need to "change" MOC or perform "another study" on MOC (funded by our dues) to sweep these actions under the rug. MOC just needs to end immediately.
I worry that the HRS leadership doesn't understand how angry practicing physicians are about what has transpired behind our backs as we've struggled to do the yeoman's work of patient care.
Here's the deal: if the HRS wants my dues for another year going forward, move to end MOC now. Put your actions where our money is. Otherwise, I'll save my hard-earned assets for other things besides supporting groups who don't support those of us on the front line of health care who obey the law and prefer to manage our profession ethically and transparently, rather than through political channels using threats and intimidation as their modus operandi.
-Wes
Monday, October 05, 2015
Heart Rhythm Society and ABMS: Friends for Life
Patients are dropping like flies in Electrophysiology Laboratories across the country. Death and destruction everywhere. Poor quality. Unsafe standards. Pitiful results.
What, you haven't heard?
Clearly this MUST BE THE CASE! That's why it's SO important that the Heart Rhythm Society and the Intersocietal Accreditation Commision (IAC) INSIST (seriously) that EVERY electrophysiology laboratory in the United states have a MEDICAL DIRECTOR certified by the American Board of Medical Specialties. Otherwise, your electrophysiology laboratory will be labeled as "NOT UP TO STANDARDS." And we wouldn't want that now, would we?
I just received this disappointing e-mail from David Haines, MD, president of the "IAC Cardiac Electrophysiology Accreditation" on behalf of the Heart Rhythm Society (who is clearly colluding with the American Board of Medical Specialties to assure regulatory capture of every electrophysiology laboratory in the United States) under the guise of EP laboratory standardization:
I would suggest every electrophysiologist comment on this decision by the Heart Rhythm Society to insist that EP laboratories must meet certain "standards" regulated by yet another unaccountable body to the physician and patient (who the heck is the "Intersocietal Accreditation Commission?") After all, this is ALL about regulatory capture and the money generated for the ABMS and their member boards.
Where's the proof that patient care will be improved as a result of such standardization?
Instead, everything (including our "re-certification" expenses) will cost us more and more as the regulatory capture of medicine by the ABMS and the IAC/ and their pals continues unabated.
-Wes
What, you haven't heard?
Clearly this MUST BE THE CASE! That's why it's SO important that the Heart Rhythm Society and the Intersocietal Accreditation Commision (IAC) INSIST (seriously) that EVERY electrophysiology laboratory in the United states have a MEDICAL DIRECTOR certified by the American Board of Medical Specialties. Otherwise, your electrophysiology laboratory will be labeled as "NOT UP TO STANDARDS." And we wouldn't want that now, would we?
I just received this disappointing e-mail from David Haines, MD, president of the "IAC Cardiac Electrophysiology Accreditation" on behalf of the Heart Rhythm Society (who is clearly colluding with the American Board of Medical Specialties to assure regulatory capture of every electrophysiology laboratory in the United States) under the guise of EP laboratory standardization:
Last week, I sent an email discussing the recent partnership between the Heart Rhythm Society, the Intersocietal Accreditation Commission (IAC), and other key stakeholders to develop and operate an EP Lab Accreditation Program. Developed by the IAC Cardiac Electrophysiology Board of Directors, the draft IAC Standards and Guidelines for Cardiac Electrophysiology Accreditation are now available for public comment and I am requesting your assistance on this important initiative. Please review the draft standards and provide feedback to ensure that they meet the expectations and the field’s needs.Don't you get it? The new "Standards" are coming whether you like it or not.
Listed below are the instructions to provide comments. The IAC Comment Form must be completed and submitted electronically by December 1, 2015.
To submit a comment on the proposed IAC Standards:
At the close of the comment period, the IAC Cardiac Electrophysiology Board of Directors will review all submitted comments, consider modifications, and vote on the Standards final approval. The new Standards will be posted to the IAC Cardiac Electrophysiology website and available for download in late 2015.
- Visit the IAC website.
- Click on the proposed Standard you wish to review and/or comment from the menu.
- A window will expand with the description of the Standard and a PDF to view the section of the Standards available for comment.
- Click on the PDF to open it in a separate window for review.
- On the right, fill in your name and provide your comments about the proposed Standards in the boxes provided.
- Push submit.
I would suggest every electrophysiologist comment on this decision by the Heart Rhythm Society to insist that EP laboratories must meet certain "standards" regulated by yet another unaccountable body to the physician and patient (who the heck is the "Intersocietal Accreditation Commission?") After all, this is ALL about regulatory capture and the money generated for the ABMS and their member boards.
Where's the proof that patient care will be improved as a result of such standardization?
Instead, everything (including our "re-certification" expenses) will cost us more and more as the regulatory capture of medicine by the ABMS and the IAC/ and their pals continues unabated.
-Wes
Tuesday, May 12, 2015
EP Lab Activism
Getting ready for the 2015 Heart Rhythm Society Meetings in Boston later this week.

Looking forward to seeing everyone there!
-Wes
Looking forward to seeing everyone there!
-Wes
Saturday, May 02, 2015
Why Electrophysiologists Need to Flood the MOC "Debate" at HRS2015
 |
| Anti-MOC Buttons Click image to order yours |
Doug Zipes, MD will serve as the protagonist of the "debate" and Fred Kusumoto, MD will serve as the antagonist. I am sure the so-called "debate" will be cordial. Both speakers are class acts and I'm sure each will do their best to up-end the other.
But I have many concerns about this "debate," some of which I articulated earlier. Now after reviewing the program format and disclosures for the "debate," I have more concerns.
First of all, the limited time for the debate does not allow time for input from the audience. This is a shame. HRS needs to hear concerns from ALL of their membership. Granted no one wants a shouting fest, but polite and pointed discourse should be encouraged at meetings, not squelched.
Secondly, let's look at the disclosures for this debate, because I think this is important.
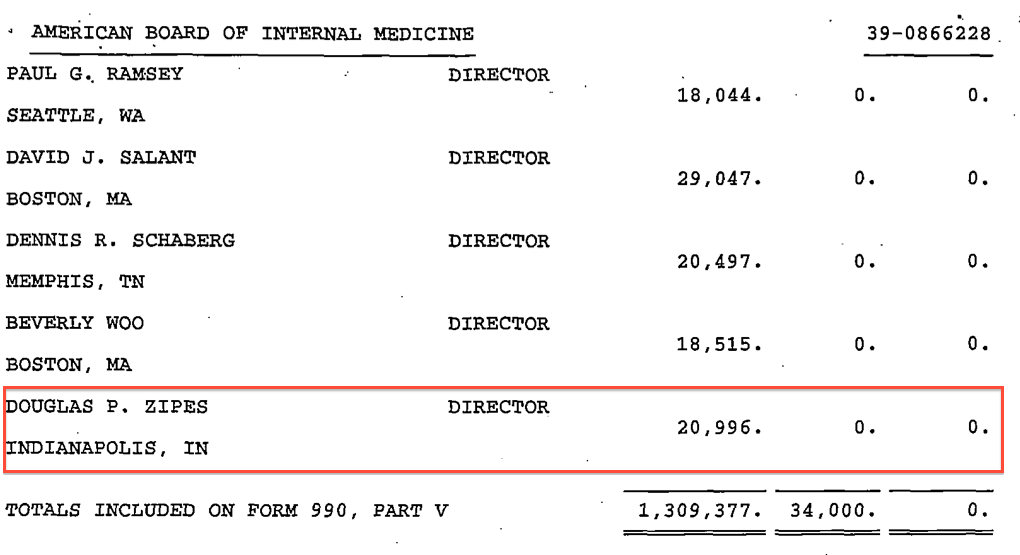
Dr. Zipes lists his disclosures for the MOC "debate" as follows:
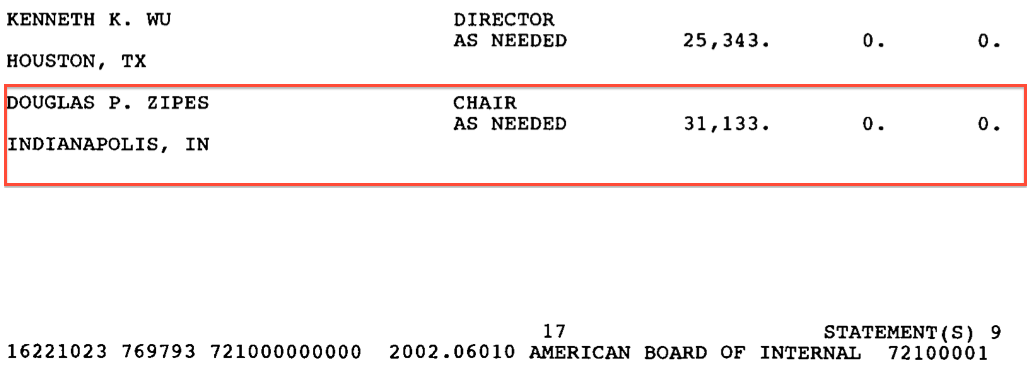
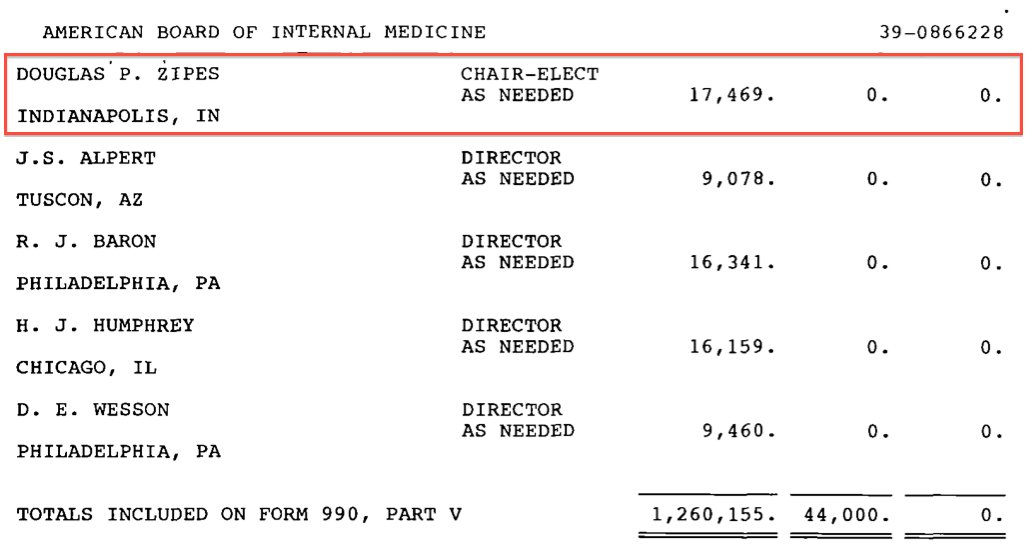
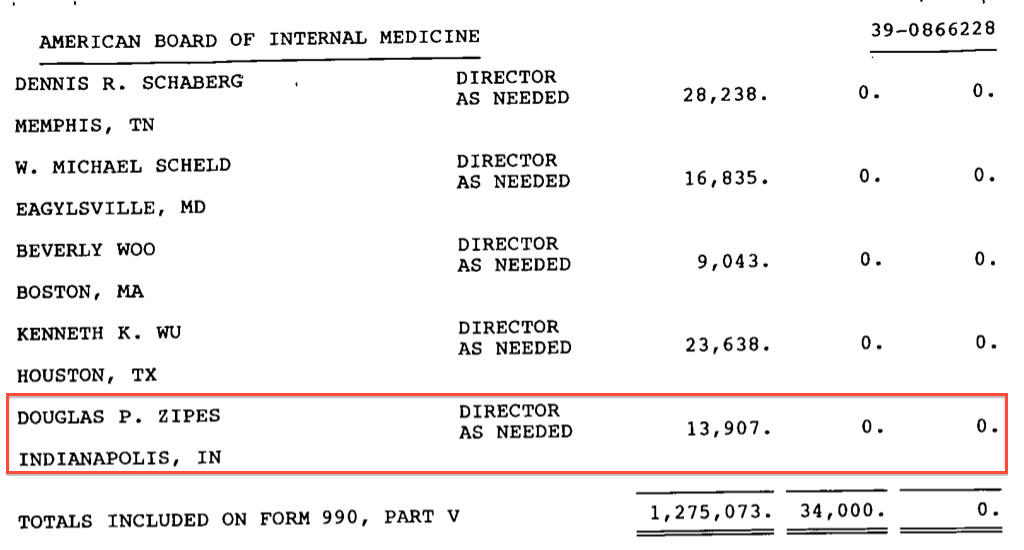
Douglas P. Zipes, MD, FHRS. Krannert Institute of Cardiology, Indianapolis, INNo where in his current disclosures does Dr. Zipes mention his long relationship with ABIM as a paid "Director," "Chair-Elect," and "Chair" of the organization. Here is what Dr. Zipes earned from the ABIM between July 1, 1998-Jun 30, 2003:
Disclosures
D.P. Zipes: E - Royalty Income; 3; Elsevier. I - Research Grants; 1; Medtronic, Inc.
Abstract
There is no abstract associated with this presentation.
FY 2003 $31,133 as "Chair"
{kind=link}
FY 2002 $17,469 as "Chair-Elect"
{kind=link}
FY 2001 $13,907 as "Director"
{kind=link}
FY 2000 $20,996 as "Director"
{kind=link}
FY 1999 $30,484 as "Director"
{kind=link}
No doubt Dr. Zipes has good friends at the ABIM and will find it easy to take the "protagonist" role in the "debate," but is he the right person for a non-biased recommendation for endorsement of the ABIM's MOC program by the Heart Rhythm Society?
We should recall that Christine Cassel, MD was the acting President and CEO of the ABIM and the ABIM Foundation during the time Dr. Zipes' had his appointments there. Dr. Cassel now is President and CEO of the National Quality Forum (NQF), a non-profit organization called a "consensus-based entity" that sets quality metrics that soon will influence how physicians are paid. The NQF has close ties to the ABIM and derives most of its revenue from the Center for Medicare and Medicaid Services (CMS) by way of government grants. Recall that the current President and CEO of the ABIM, Richard Baron, MD worked for the National Quality Forum before coming to the ABIM and may have been slated for a leadership role there as evidenced by a screen shot I captured from the National Quality Forum's website in July 5, 2014 (the web page is no longer present). Also realize that the National Quality Forum continues to employ Ms. Cassel who was responsible for (1) the repeated piecemeal funneling of $30.6 million of our physician testing fees to the ABIM Foundation (and that purchase of the now infamous $2.3 million luxury condominium), (2) the creation and write-off of $3 million dollars for the now defunct "Institute of Clinical Evaluation" created by the Foundation, and (3) the non-disclosure of grants the ABIM Foundation received from the Josiah Macy Jr. Foundation and the "Institute of Medicine as a Profession," a non-profit created by George Soros and his Open Society Institute. Needless to say, Dr. Zipes' conflicts are very significant in light of this interplay of money and politically-connected individuals and organizations.
{kind=link}
Let's now look at Dr. Kusumoto's published conflicts of interest for this "debate:"
Fred M. Kusumoto, MD, FHRS. Mayo Clinic, Jacksonville, FL(I did not see Dr. Kusumoto's name on any of the ABIM's Form 990 tax disclosure forms either. )
Disclosures
F.M. Kusumoto: None.
Abstract
There is no abstract associated with this presentation.
The Heart Rhythm Society must make a clear choice after the upcoming scientific sessions. They can side with the working community of cardiac electrophysiologists or they can side with continuing their support of government grants, cronyism, and an increasingly political agenda that promises cash flow from the government. Which will they choose?
So let's show up with a sea of buttons and other bling and make it clear that the HRS's endorsement of MOC must go. All of it.
To promote the anti-MOC movement, I have created a section of my MedTees.com website specifically to purchase anti-MOC bling. All proceeds I receive (about 1-5% of the prices) will go to the ABIM's competitor, NBPAS.org instead. The rest of the costs go to the manufacturer of the bling, Cafepress.com, including the high shipping prices (sorry, out of my control).
If you'd like to get a FREE 2.25" Anti-MOC button from me before the "debate" session at HRS2015, I will have a hundred of them to distribute(limit one per doctor - I paid for them myself), so get there early.
I look forward to seeing everyone at the meeting.
-Wes
Friday, January 16, 2015
Grass Roots: It's Time To Take Action on MOC
As many long-term readers of this blog are aware, because of concerns over its coercive nature, I have been investigating the American Board of Medical Specialties (ABMS) Maintenance of Certification (MOC) program implemented in large part by the American Board of Internal Medicine (ABIM) since studying for my third round of re-certification. As part of that investigation, I have uncovered what appears to be a carefully crafted propaganda campaign using poor scientific methods, non-practicing authors from think-tanks, the veterinary profession, and the ABMS/ABIM hierarchy to serve as "evidence" of the program's legitimacy, as well as much more troubling financial dealings of the ABIM and the ABIM Foundation.
I brought these concerns to the leadership at the Heart Rhythm Society via an email left on their website on 2 January 2015 that included a link to my investigation of the ABIM's tax records. The Heart Rhythm Society's office as closed at that time (they returned 5 January 2015), but I never received a response to that email initially. So I called the Heart Rhythm Society on the 14th of January and asked to speak with Mr. James Youngblood, their President and CEO, about my concerns regarding the ABIM. I seems he was unavailable at the time but I was assured they had found the email and that I would receive a response "in 24-48 hours." Yesterday I received the email and this is what he said:
I would ask that Heart Rhythm Society members who agree with this petition to sign it and designate their membership status with the Heart Rhythm Society in the "Notes" section and then send it on to your colleagues.
It is time we send a strong message to our professional organizations that we demand more than words in response to our deep concerns with the ABMS/ABIM MOC program.
Thank you -
-Wes
I brought these concerns to the leadership at the Heart Rhythm Society via an email left on their website on 2 January 2015 that included a link to my investigation of the ABIM's tax records. The Heart Rhythm Society's office as closed at that time (they returned 5 January 2015), but I never received a response to that email initially. So I called the Heart Rhythm Society on the 14th of January and asked to speak with Mr. James Youngblood, their President and CEO, about my concerns regarding the ABIM. I seems he was unavailable at the time but I was assured they had found the email and that I would receive a response "in 24-48 hours." Yesterday I received the email and this is what he said:
"Sorry for the delay in responding to your email request. We appreciate the information you shared and your opinion in this matter. Regarding your follow-up voice message inquiring about what the HRS offers in support of ABIM-MOC, HRS provides the opportunity for members to earn up to 42 MOC medical knowledge points on a complementary basis. (Opportunity for MOC points expires 10/15/15)It seems the very public outcry by practicing physicians over the entire ABMS/ABIM-MOC program is being met with little action despite the evidence of its corrosive effects on our profession of medicine. Therefore, I have decided to begin a grass roots effort to ask my own professional medical society, the Heart Rhythm Society, to immediately cease their promotion and marketing of the ABMS/ABIM MOC program and instead to turn their considerable resources to removing the corrupt ABMS MOC program from the Affordable Care Act. To that end, I am now circulating a petition for Heart Rhythm Society members (and other interested practicing physicians) to sign to send a clear message to our society's leadership that we need more than words, we need action, to stop the use of this unproven and unethical MOC program that has been foisted without evidence of its effectiveness for improving patient care upon practicing US physicians. Anything less is unacceptable, given what we now know about the program.
We have extensive additional information provided at http://www.hrsonline.org/Education-Meetings/Maintenance-of-Certification#16575
We have provided ongoing feedback to the ABIM around our concerns with their approach to the MOC program. We will continue that dialogue.
With regard to an financial concerns with ABIM, we will continue to monitor the situation closely and inform our members should any action be required.
Thanks, J
James H. Youngblood
Chief Executive Officer
Heart Rhythm Society
NEW ADDRESS:
1325 G St. NW, Suite 400
Washington, DC 20005
(Phone numbers redacted)
www.HRSonline.org
I would ask that Heart Rhythm Society members who agree with this petition to sign it and designate their membership status with the Heart Rhythm Society in the "Notes" section and then send it on to your colleagues.
It is time we send a strong message to our professional organizations that we demand more than words in response to our deep concerns with the ABMS/ABIM MOC program.
Thank you -
-Wes
Tuesday, January 13, 2015
Some Thoughts on the National Board of Physicians and Surgeons
I admire Paul Tierstein, MD's honest attempt to create a greatly simplified alternative to the ABMS's Maintenance of Certification® (MOC) program called the National Board of Physicians and Surgeons (NBPAS). I hope he's successful, but I sense there will be large headwinds for the effort ahead.
Here's why.
The Affordable Care Act (ACA) modified Sections 1848(k) and 1848(m) of the Social Security Act which defines how CMS pays physicians for their services. Section (k) is the section that defines how a "Quality Reporting System" is to be set up (with subsection (4) requiring the "Use of Registry-based Reporting") and Section (m) defining physician incentive payments physicians might receive if quality reporting occurs properly. (Sadly, those CMS incentive payments do not cover the cost of participating in MOC for most of us.)*
Section (k) was modified by the ACA to include the ABMS MOC program as a "physician registry." The registry was "defined" as requiring all four parts of the MOC program created by the ABMS, including the much-maligned "practice improvement modules" that have been described by the physician community as overly time-consuming, irrelevant and may even violate federal research statutes regarding the study of physicians, their practices, and patients.
Unfortunately the new NBPAS does not address these requirements of the our new health care law, leaving the creation of the NBPAS to look like a Rand Paul moment all over again with physicians signing up for something that, legislatively, means nothing.
Welcome to the concept of "regulatory capture."
Physicians should realize that special interests and their lobbyists (including the US hospital, pharmaceutical, survey companies, and insurance lobbying groups) were highly influential in the creation of our new health care law. They are also very good at politics. It is unlikely that these entities want to see MOC go away, irrespective of how corrupt the system has become. There's just too much money involved. Even our own specialty societies use the MOC program's educational requirements to coerce physicians to take their educational courses to "earn MOC points" to help pad their bottom lines as physician attendance (and corporate sponsorship) at scientific sessions has dwindled over the past years.
But what's more important to our patients in the long run? Time for their needs or time for test-taking and survey collection? Is it more important to satisfy government requirements or address the real needs of our patients? Certainly continuing education of physicians is needed, but irrelevant work for an unaccountable third-party organization so they can measure us rather than help us is not.
Physicians need to take the stick, but we can't do this alone since we care for patients. So we need to ask this question: will our specialty societies commit to supporting practicing physicians or the new bureaucratic divide? (They can't do both.) Will they truly step up to the plate and commit their considerable staff, dollars, pager-less hours, lobbying and legislative efforts to help remove the corrupt MOC program from the Affordable Care Act or allow practicing physicians - their members - to wallow in the corrupt status quo as they are coerced to participate in MOC?
I remain pessimistic that creating another "board" will fix the current deep-seated problems with the ABMS MOC construct with ABMS as the mothership directing a flotilla of 24 member boards. In my view the only way to truly "change" MOC is to have a coordinated effort from all specialty societies to insist our legislators remove the portion of our new health care law that requires we participate in a "physician registry" that robs not only practicing physicians, but patient care itself.
HRS and ACC, are you on board?
-Wes
*Addendum 2/12/2015:
It should be noted that the payment incentives offered 2012-2104 from CMS for participation in MOC ended January 1, 2015, but that MOC participation will still be used as a physician quality reporting metric.
Here's why.
The Affordable Care Act (ACA) modified Sections 1848(k) and 1848(m) of the Social Security Act which defines how CMS pays physicians for their services. Section (k) is the section that defines how a "Quality Reporting System" is to be set up (with subsection (4) requiring the "Use of Registry-based Reporting") and Section (m) defining physician incentive payments physicians might receive if quality reporting occurs properly. (Sadly, those CMS incentive payments do not cover the cost of participating in MOC for most of us.)*
Section (k) was modified by the ACA to include the ABMS MOC program as a "physician registry." The registry was "defined" as requiring all four parts of the MOC program created by the ABMS, including the much-maligned "practice improvement modules" that have been described by the physician community as overly time-consuming, irrelevant and may even violate federal research statutes regarding the study of physicians, their practices, and patients.
Unfortunately the new NBPAS does not address these requirements of the our new health care law, leaving the creation of the NBPAS to look like a Rand Paul moment all over again with physicians signing up for something that, legislatively, means nothing.
Welcome to the concept of "regulatory capture."
 |
| Screenshot of Heart Rhythm Society webpage |
But what's more important to our patients in the long run? Time for their needs or time for test-taking and survey collection? Is it more important to satisfy government requirements or address the real needs of our patients? Certainly continuing education of physicians is needed, but irrelevant work for an unaccountable third-party organization so they can measure us rather than help us is not.
 |
| A second Heart Rhythm Society webpage devoted to MOC |
I remain pessimistic that creating another "board" will fix the current deep-seated problems with the ABMS MOC construct with ABMS as the mothership directing a flotilla of 24 member boards. In my view the only way to truly "change" MOC is to have a coordinated effort from all specialty societies to insist our legislators remove the portion of our new health care law that requires we participate in a "physician registry" that robs not only practicing physicians, but patient care itself.
HRS and ACC, are you on board?
-Wes
*Addendum 2/12/2015:
It should be noted that the payment incentives offered 2012-2104 from CMS for participation in MOC ended January 1, 2015, but that MOC participation will still be used as a physician quality reporting metric.
Monday, September 23, 2013
Reviewing the 2013 EP Board Review Course
This past week I sat for my third board review course in anticipation of my upcoming third EP board recertification. It was a well attended event of about 150-160 electrophysiologists, some from as far away as Alaska. That, I suppose, is one of the attractions of having this course in a city like Chicago: it's a major central airport hub and has plenty to see and do for those hearty and financially solvent enough to spend the evenings out at a nice restaurant or club. For me, a native of the Chicago area, I was lucky enough to stay in my own home and just had to brave the traffic and $35-a-day parking fees. Others from out of town bore a much larger expense in terms of lost days from work, hotel and transportation fees. The meeting was held at the Marriott Renaissance Hotel on 1 Wacker Drive in Chicago, just a few blocks from Michigan Avenue's shopping district downtown - not the cheapest hotel in Chicago, nor the most expensive. Perhaps it was held there for the comfort of the rooms, the size of the lecture hall, or a need to provide a central Chicago location, but given the amount of time we spent in the lecture room and the social life of most serious electrophysiologists I know, I wondered why it wasn't held somewhere less expensive. After all, cost remains a huge concern (if not overriding one) for doctors attending these courses.
The course began Thursday afternoon at 1pm and went until 8:30 pm Thursday, 7:45am-5:30 pm Friday and Saturday, and concluded Sunday with a rushed morning review of pacing principles from 07:45 am to 12:30pm. (Completing the course on time was critical for those who had to catch planes home on Sunday)
I paid the extra money for attending a maintenance of certification test session before the main session began to earn a few points. This clearly was not worth the extra money in my view, as it was just an extra Workshop that included a bunch of typical board-style questions with the answers in the back of the book. My recommendation would be to save your money and take the online versions that come with one's recertification fee. It just seemed to be another cash cow for the ABIM and HRS.
The course materials were printed, and the majority of doctors polled (75%) preferred their materials this way, despite the Heart Rhythm Society (HRS) clearly leaning to providing the material electronically on a thumb drive. They also offered (with a $1300 discount if you attended the session) the full lectures (with audio and slides) to members who wanted to cough up even more money so they could review the materials at another time. (I passed).
The main course was taught by established names in EP and the Heart Rhythm Society: Ken Ellenbogen, N.A. Mark Estes, David Haines, Fred Morady, William Stevenson, among others. These are guys that taught me, they've been doing it a while, and they're good at what they do. As such, the lectures were paired down to the essential principles and generally well-organized with good audiovisuals and sound, but were peppered the same pimp items that you'll still have to memorize despite our new era of Google. I suppose having these things pass your cortex once so the recognition of these syndromes might be realized in one's practice, but in this era of Google whether memorization is really necessary is another matter.
But did I learn anything? Okay, I have to admit I did. New things I learned included a few pearls about Early Repolarization Syndrome (and is probably fair game for boards), the genetics of plenty of obscure diseases, and about how many ways a doctor can get pimped on a cleverly written examination. Given these realizations, I hope my chances for passing my board certification were improved as a result of attending this course. We'll see.
It was kind of sad (yet psychologically affirming) to see Sonny Jackman, an icon of accessory pathway ablation and EP, in the audience with me. It was particularly entertaining when he had to hop up and explain a tracing to the audience on behalf of the lecturer (truly a highlight). But I also wondered why Dr. Jackman was there. Sadly, I knew the answer: he's no different than the rest of us now and understands that it won't be long before the bureaucratic machine called medicine will require passing an irrelavent test to practice medicine.
It was this last issue that was most relevant and prescient. Mark Estes (someone who has sat on the test-writing committee in the past) tried to explain how the ABIM decides how many recertifying doctors ultimately pass their examination. "This is a sensitive and unpopular issue for EPs in practice," he said quietly. You could see people agreeing. But as he explained how the ABIM determines how many recertifying EPs pass the recertification exam he admitted, "I really have no idea how they decide." He continued, "But when we look at the trend line for the percent passing from prior years, you can see that last year's percentage was down a bit." He then showed the trend line.
Think about that. No one has an idea what consitutes the criteria for a "passing" grade for recertification, yet here we are spending too much money on a process that has little to no proven patient care benefit in terms of quality care. This non-transparent scoring criteria adds to the problems with recertification in my view, since it would not be difficult to think that granting of a passing grade for re-certification could be used against certain subspecialites for any number of obscure reasons (eg., the desire to downsize the specialty, political differences, etc.) One only has to consider how the IRS was used against non-profit political organizations to get my paranoid drift in the era of medical cost conservation here. Perhaps this is a bit overdramatic, but it makes you wonder, doesn't it?
So I'm back in the salt mine of everyday practice now. Hopefully the course helped and will prove itself valuable for me in the future. Honestly, every effort was made to make the sessions tolerable and informative, I just wish I understood why the re-certifiers needed to be there. But I'm trying to cope with the reality of the times and I just hope the ABIM won't decide not to pass me for what I've said here.
-Wes
The course began Thursday afternoon at 1pm and went until 8:30 pm Thursday, 7:45am-5:30 pm Friday and Saturday, and concluded Sunday with a rushed morning review of pacing principles from 07:45 am to 12:30pm. (Completing the course on time was critical for those who had to catch planes home on Sunday)
I paid the extra money for attending a maintenance of certification test session before the main session began to earn a few points. This clearly was not worth the extra money in my view, as it was just an extra Workshop that included a bunch of typical board-style questions with the answers in the back of the book. My recommendation would be to save your money and take the online versions that come with one's recertification fee. It just seemed to be another cash cow for the ABIM and HRS.
The course materials were printed, and the majority of doctors polled (75%) preferred their materials this way, despite the Heart Rhythm Society (HRS) clearly leaning to providing the material electronically on a thumb drive. They also offered (with a $1300 discount if you attended the session) the full lectures (with audio and slides) to members who wanted to cough up even more money so they could review the materials at another time. (I passed).
The main course was taught by established names in EP and the Heart Rhythm Society: Ken Ellenbogen, N.A. Mark Estes, David Haines, Fred Morady, William Stevenson, among others. These are guys that taught me, they've been doing it a while, and they're good at what they do. As such, the lectures were paired down to the essential principles and generally well-organized with good audiovisuals and sound, but were peppered the same pimp items that you'll still have to memorize despite our new era of Google. I suppose having these things pass your cortex once so the recognition of these syndromes might be realized in one's practice, but in this era of Google whether memorization is really necessary is another matter.
But did I learn anything? Okay, I have to admit I did. New things I learned included a few pearls about Early Repolarization Syndrome (and is probably fair game for boards), the genetics of plenty of obscure diseases, and about how many ways a doctor can get pimped on a cleverly written examination. Given these realizations, I hope my chances for passing my board certification were improved as a result of attending this course. We'll see.
It was kind of sad (yet psychologically affirming) to see Sonny Jackman, an icon of accessory pathway ablation and EP, in the audience with me. It was particularly entertaining when he had to hop up and explain a tracing to the audience on behalf of the lecturer (truly a highlight). But I also wondered why Dr. Jackman was there. Sadly, I knew the answer: he's no different than the rest of us now and understands that it won't be long before the bureaucratic machine called medicine will require passing an irrelavent test to practice medicine.
It was this last issue that was most relevant and prescient. Mark Estes (someone who has sat on the test-writing committee in the past) tried to explain how the ABIM decides how many recertifying doctors ultimately pass their examination. "This is a sensitive and unpopular issue for EPs in practice," he said quietly. You could see people agreeing. But as he explained how the ABIM determines how many recertifying EPs pass the recertification exam he admitted, "I really have no idea how they decide." He continued, "But when we look at the trend line for the percent passing from prior years, you can see that last year's percentage was down a bit." He then showed the trend line.
Think about that. No one has an idea what consitutes the criteria for a "passing" grade for recertification, yet here we are spending too much money on a process that has little to no proven patient care benefit in terms of quality care. This non-transparent scoring criteria adds to the problems with recertification in my view, since it would not be difficult to think that granting of a passing grade for re-certification could be used against certain subspecialites for any number of obscure reasons (eg., the desire to downsize the specialty, political differences, etc.) One only has to consider how the IRS was used against non-profit political organizations to get my paranoid drift in the era of medical cost conservation here. Perhaps this is a bit overdramatic, but it makes you wonder, doesn't it?
So I'm back in the salt mine of everyday practice now. Hopefully the course helped and will prove itself valuable for me in the future. Honestly, every effort was made to make the sessions tolerable and informative, I just wish I understood why the re-certifiers needed to be there. But I'm trying to cope with the reality of the times and I just hope the ABIM won't decide not to pass me for what I've said here.
-Wes
Thursday, May 30, 2013
A Critical Review of the Insurance Claim Denial Process
"If you can speak what you will never hear,
if you can write what you will never read,
you have done rare things."
-Henry David Thoreau
"Doctor, how much longer?"
The case had gone smoothly, but the challenges of mapping the infrequent skipped beats that signified the initiating sequence to the tachycardia was getting more difficult. "Could it be left sided?" I wondered. "Anterior or posterior? I've tried the posterolateral area and that timing was late. Clearly anteromedial was earlier. All the darn beats look so similar with pace-mapping."
I had been working for an hour and a half without effect when I had an idea: "Maybe the 3D mapping system would help."
And so, I deployed a highly sophisticated three-dimensional (3D) electroanatomical (EAM) mapping system that sped her successful ablation. She was relieved. That is until the bill arrived and the 3D EAM mapping was denied by her insurance carrier.
***
On December 19, 2012, I wrote about the insurance denial for this case. I was surprised that a denial for payment was made for a portion of a ventricular tachycardia (VT) ablation procedure that was commonplace in my field: three-dimensional (3D) electroanatomic mapping. Worse, I was even more surprised that the denial came from an unknown physician who lacked training in my field and appeared to be nothing more than a foot-soldier of a Cigna insurance company medical coverage policy. Such a denial had never happened to one of my patients before.
Since that blog post was written many months ago, my administrative staff and I have been enduring the appeal. Here's how it's gone.
Shortly after my piece was published, I was notified that someone at Cigna had called our hospital and inquired if they were aware of my blog post. They were. My workplace has graciously permitted me to have this blog since 2005, provided I clearly state the views in that blog are my own, which they are.
Second, I learned that the individual who sent the original coverage denial letter to me was not our local Cigna "regional" medical director. After my post was published, my local medical director from Cigna wanted to talk and explain the proper way that claim denials should handled. A telephone conference was arranged between myself and my the medical director (a local pediatrician from a local academic center which will go un-named) along with another non-medical representative of the local regional office of Cigna. I offered them the opportunity to publish a rebuttal to my post at this site if they desired, but they declined the offer. Instead, I was asked to contact them via e-mail or phone before going public with my concerns about their decision on a blog - "we have a set way of handling disagreements with policy decisions" I was told. Was this because Cigna's leadership didn't want the bad press or was it a polite way of saying "cease and desist?" I wasn't sure.
So, in the interest obtaining a reversal of my patient's claim denial as easily as possible, I complied. I sent them my first rebuttal in writing and communicated with them via email as requested. My rebuttal went something like this:
Cigna's original denial letter, dated 1 March 2012 stated:
Since that blog post was written many months ago, my administrative staff and I have been enduring the appeal. Here's how it's gone.
Shortly after my piece was published, I was notified that someone at Cigna had called our hospital and inquired if they were aware of my blog post. They were. My workplace has graciously permitted me to have this blog since 2005, provided I clearly state the views in that blog are my own, which they are.
Second, I learned that the individual who sent the original coverage denial letter to me was not our local Cigna "regional" medical director. After my post was published, my local medical director from Cigna wanted to talk and explain the proper way that claim denials should handled. A telephone conference was arranged between myself and my the medical director (a local pediatrician from a local academic center which will go un-named) along with another non-medical representative of the local regional office of Cigna. I offered them the opportunity to publish a rebuttal to my post at this site if they desired, but they declined the offer. Instead, I was asked to contact them via e-mail or phone before going public with my concerns about their decision on a blog - "we have a set way of handling disagreements with policy decisions" I was told. Was this because Cigna's leadership didn't want the bad press or was it a polite way of saying "cease and desist?" I wasn't sure.
So, in the interest obtaining a reversal of my patient's claim denial as easily as possible, I complied. I sent them my first rebuttal in writing and communicated with them via email as requested. My rebuttal went something like this:
Cigna's original denial letter, dated 1 March 2012 stated:
"Use of an intracardiac electrophysiological 3-dimensional mapping system in the diagnosis, treatment, or management of ventricular arrhythmias or any other condition because there is insufficient scientific evidence to support its use does not meet Cigna guidelines for coverage because it is considered experimental, investigational, and/or unproven (E/I/U)."Cigna's 2012-2013 Medical Coverage Policy regarding 3D electroanatomic mapping systems for VT ablation (which I have copied on my own server, lest it disappear) stated:
The authors state, "although not yet established as requisite or "core" equipment for the EP laboratory, these and other emerging technologies have had, and will continue to have, a major impact on the practice of cardiac arrhythmia management. It is also anticipated that additional new technologies will be developed at ever faster rates in the future" (Tracy, et al., 2006). There has been no update to this statement since 2006.Baloney. The EHRA/HRS Expert Consensus statement on VT ablation was subsequently published in in 2009 and that document specifically addresses the use of 3D EAM for VT ablation. It said:
Technological advances have been critical to the development of the field and will continue to play an important role in improving outcomes. The evaluation of new technologies has generally been based on uncontrolled series. There is limited head-to-head comparison of different technologies. Although new technologies generally increase the cost of a procedure when they are introduced, the costs may be justified if they improve outcomes.
...
The focal VT origin can be identified from activation and/or pace mapping.4,381,385,410 Systematic point-by-point activation mapping is the initial preferred technique.233,234,385,409 Some investigators use three-dimensional EAM systems to assist in relating the anatomy to the mapping data.4,124,125,233,381,385,428–430
Wrong.
Two MORE submissions for higher-order reviews and over four months later, the verdict was handed down: my patient had exhausted all avenues of appeal for the claim. The insurance company would not pay this portion of my patient's bill, no matter what.
Parsing Truths
When deciding what therapies are effective for our field, who should set the requirements for the level of evidence required to determine effectiveness of any therapy, EP societies or the insurance industry? While it is true that prospective randomized trials comparing mapping techniques head-to-head for localizing ventricular arrhythmias have not been done, we should also understand that such a study will never be performed. Why? First, who would pay for such a study to be conducted? The utility of 3D mapping for SVT has been demonstrated and proven effective, in large part because of the greater safety (and greater likelihood of obtaining FDA approval) when supraventricular rhythms are studied compared to ventricular arrhythmias. Second, because the occurrence of the arrhythmia (in this case RVOT VT) is relatively rare, a compelling reason for industry (or government) to fund such a study doesn't exist.
But like SVT ablation, there are three real advantages to these 3D mapping systems for VT ablation that has been repeatedly demonstrated in the literature: (1) catheters can be returned to prior locations accurately whether the arrhythmia is occurring in a location or not, (2) real reductions in fluoroscopy times can be achieved and (3) certain 3D EAM systems that use mathematical algorithms (non-contact balloon mapping) can localize the origin of an arrhythmia using a single heart beat. For the rare patient (like mine) that has infrequent arrhythmias, how would a randomized trial be constructed in hopes of proving the utility of such a technology over conventional mapping by point-to-point techniques? Would such a trial be even ethical to conduct? So, just because a prospective trial has not been performed to demonstrate the utility of a technology in rare circumstances, does this mean electrophysiologists should never utilize such a technology to achieve a successful ablation outcome when other means fail even though such a technology has been shown to be effective in single-center studies? According to Cigna's policy statement, the answer to this question is "yes."
Too bad insurers never have to speak with patients when an ablation fails.
One Last Try
Because I did not want to take "no" for an answer, I asked my administrative staff to see if they could obtain the name of the Cigna "external" reviewer. We had been assured that the case was externally reviewed by an electrophysiologist. We were given the name of an individual but were surprised to find that the physician was a paid employee of Cigna with credentials as an internist and general cardiologist with a nuclear medicine background. To me, it seemed Cigna "external" review was actually an "internal" review performed by a paid employee of different regional office of Cigna (hence "external" to our region) who was a general cardiologist, not a cardiac electrophysiologist.
I brought this concern to the attention of my local medical director of Cigna by e-mail. In that email I also expressed my concerns about the long time each review had taken. I asked him to examine both issues, since I felt my patient had not received a fair and unbiased claim review. Also, while my patient had received a final denial letter, I never received a notification of their final determination for coverage. After some delay, the director promised to look into my concerns and contacted me by phone later in the week as promised.
In our subsequent discussion, it appeared the director felt the timeliness of their reviews was satisfactory, despite a timeline that stretched over fourteen months for this entire process. In regards to my concerns over who reviewed my patient's claim denial, he claimed there were two "internal" Cigna reviewers and reviewers "external" to Cigna who supported the denial. Of the external reviewers, the director claimed one was board-certified in internal medicine and interventional cardiology and the other external reviewer was board-certified in internal medicine, cardiology and cardiac electrophysiology. He refused to disclose either of the external reviewers' names. When asked, the director stated that the electrophysiologist was in active practice. I reiterated that I still felt the EHRA/HRS Expert Consensus statement suggested the 3D-mapping falls well within the standard of care. Surely they should reconsider. But despite my pleas for reconsideration, no reversal was forthcoming.
I hung up the phone.
Amazingly, there is little else I can do for my patient's insurance payment denial now. Here I am, a non-anonymous board-certified cardiac electrophysiologist with over twenty years experience who was caught in a challenging case with my patient and am now being told by a pediatrician from an insurance company that there's no merit to my concerns about an unfair denial for coverage of the 3D mapping portion of my patient's claim. I am dumbfounded, confused, and heartbroken for my patient.
So what have I learned?
1) In Cigna's case, some insurance coverage decisions disregard current standards of care and up-to-date expert consensus statements in lieu of poorly-updated corporate medical coverage policies.
2) Specific challenges I encountered with my patient's RVOT VT ablation case had no bearing on Cigna's decision.
3) Physician reviewers often do not hold expertise in the specialty areas they are asked to review. Because they are first and foremost paid employees of the insurer, they turn to corporate medical coverage directives for guidance, even though they are woefully lag current medical practice. As health care dollars get tighter and medicine becomes increasingly codified, significant conflicts of interest will continue to rise for a fair and impartial review of payment denials.
4) If the insurance company claims to have an individual of the same specialty externally review a case, physician providers are not notified of the basis for the denial nor given the names of the reviewers, limiting one's ability to verify the reviewer's credentials or to understand the rationale for the denial. As a result, there is no transparency to the process, nor opportunity for learning or system improvement. To me, this practice should not be condoned. Health care requires continuous quality improvement. More importantly, health care requires trust of all those who touch the field, especially when the care provided, no matter how seemingly far removed, impacts a patient's physical or socioeconomic well-being.
5) Cardiac electrophysiologists should be aware that both Cigna (here) and Aetna insurance companies (here) in Illinois now have coverage policies that may opt to deny payment for three-dimensional electroanatomic mapping for VT ablation because they claim they are experimental procedures for this indication based on their outdated internal review of the literature.
6) When confronted about the obsolete nature of their medical coverage policy, Cigna refused to take this into consideration and still refused to overturn by patient's payment denial. Instead, the medical director only promised to include the EHRA/HRS document I sent them in their next annual review of their corporate medical coverage policy for 3D mapping scheduled for 2013-2014.
7) There are technologies that have certain niche benefits for patients, but because they are not "proven" beneficial by randomized trials, in some cases they are no longer be paid for by insurers.
8) My patient will now has four months from the date of her final denial letter to ask for an state-directed independent external review of the Cigna's coverage decision via the Illinois Insurance Fairness Act as her only remaining avenue for recourse.
So now what?
As I reflect on this case, I used this sophisticated mapping technology because I felt I needed it to improve my patient's outcome and safety. I wonder what this denial of coverage does to the relationship with my patient. Has trust been eroded? As I look forward, how I will perform my next RVOT VT ablation? What do I say to the next patient with a similar arrhythmia? Should I warn all my future patients requiring VT ablation that some of the technology we routinely use to expedite their procedure might not be paid for by their insurer because of a paucity of prospective randomized trials exist (and never will)? Will I have to avoid the use of this technology knowing my patient may have to pay for it because a pediatrician or a general cardiologist who knows nothing about my field might not approve its use? Can I afford to devote this amount of time for wrestling future insurance payment denials that surface?
These are not minor concerns.
So there's the current status of this long, arduous months-long insurance denial review process for just one patient, critically reviewed. It would be easy to make this post a screed against one insurer, and while I have to say that the way this claim denial process was handled was poor at best, we should recall that other insurers have similar policies. It is in the interest of insurers to make the payment denial/review process as difficult as possible for patients and providers. It is also in insurers' best interest to keep out-of-date medical coverage policies in place that consider new technologies "experimental." Better yet, it is even better for insurers to claim niche technologies are "unproven" despite evidence to the contrary and should therefore never be paid. Finally, it is in insurers' best interest to perform internal reviews by uninformed physician reviewers of another subspecialty rather than peer-to-peer independent reviews.
What will it take to change this system?
Maybe we should start with the truth.
-Wes
Thursday, May 09, 2013
Former President Bill Clinton Kicks off Heart Rhythm Society Meeting
While the above title is true, I admit that it was used more for garnering readership than suggesting that former U.S. President Bill Clinton had any real news to share with the world's pool of heart rhythm specialists. Oh how we hoped he would tell us about his pacemaker or implantable defibrillator that he had installed but, alas, it was not to be.
But the man can still draw a crowd. The large auditorium was filled by just about everyone that attended the conference it seemed, and he received a standing ovation upon entry. He seemed relaxed, but often glanced down a bit toward the floor when he spoke on occasion as he gauged the audience and weighed his commentary. For the first part of his talk, he stood behind the podium with teleprompters at its side, but unlike other presidents we know, those seemed more for those introducing the former president, rather than the former president himself.
Mr. Clinton was politely received by what could have been a viper's den of cardiac subspecialists. He's a gifted speaker and many of us were impressed by the depth and breadth of humanitarian efforts taken on by his Clinton Foundation following his stint in the White House. It was interesting to hear about all of the places hes been and the work his organization has done and at the outset. After the polished introductory video of the Clinton Foundation's excellent work was shown to the audience of political neophytes, many of whom had never seen a president before, it was clear no one was going to kill the baby seal. This was to be the Bill Show and sadly, there was never a single mention of the support team behind his foundation.
Still, there were moments in his speech that were captivating, especially the part where he described his own post-bypass ordeal of being told that he had fluid around his heart after his heart surgery and how he had to return to the operating room to have "my chest cracked open again" to manage it. We got a glimpse at his real fears and his real appreciation for his doctors and the technologies that cared for him. We heard how he ignored his chest tightness that occurred at rest after his bypass operation and how foolish he felt in retrospect after receiving two stents to a "badly mangled artery." Then we heard about how all of this lead his efforts to change his own dietary habits and to work with PepsiCo to develop policy for school kids to lower caloric intake of sugary drinks: "We found a way to change the system without having to take it down. That's what we need to do."
But his efforts to circle back to health care reform were disjointed much of the time as he waxed back and forth from his experience in Rowanda building clinics and providing logistics to the US, and then to comparing the relatively small Netherlands' health care system to the US's system, leaving many doctors wondering when he was going to say anything of real substance. Still, he tried to make the point about a "systems approach" and paying for "performance" rather than "procedures" as a partial way to fix things. He seemed to yearn for a simpler system than the one we've got. When asked point blank if his perspective on health care had changed since having his expensive care, he masterfully deflected the question by saying "I have a deeply personal regard for the American health care system, but we're limp at preventing errors." No doubt doctors who worked so hard on his behalf appreciated that comment.
Overall, most people I spoke with after the event seemed generally pleased with Mr. Clinton's performance, especially when he admitted the limitations of the Affordable Care Act (ACA). They liked his quip about how 99.5% of people's DNA are identical, yet we spend so much time focused on making sure others know the differences in the remaining 0.5% of their genome. It was clear he was a master at reaching across the aisle and he opined for a more collaborative approach to resolving our nation's health care problems. When asked whether he thought the ACA (Affordable Care Act) would fix what's wrong with America's health care system, he said honestly "Maybe. Maybe not." But he stuck with the partisan narrative of error management, paying by "performance" rather than procedures and asking doctors to do their part to fix the system, seemingly unaware of the 30% drop in RVU payments that took hold 1 January 2013 and the 2% Medicare payments to physicians that recently affected many members of his audience. It seems he felt doctors needed to do more, but many doctors wondered silently how much more we can take.
It was clear the Europeans I spoke with after the talk loved his speech. But they were also quick to point out another little fact: Mr, Clinton's appearance fee is somewhere in the order of $250,000. A quick fact check showed that was a gross understatement: it's closer to $500,000 or more. If this is the price we've paid for this hour of entertainment it's no wonder our health care's cost crisis is such a mess.
And if so, maybe Mr. Clinton should do his part for health care reform, too, and stay home.
And if so, maybe Mr. Clinton should do his part for health care reform, too, and stay home.
-Wes
Wednesday, May 08, 2013
HRS2013 Pre-meeting Reflections
This morning I sit quietly in my hotel room, contemplating the day ahead at the 2013 Heart Rhythm Society Scientific Sessions in Denver. Emotions clash.
On one hand, it will be great to see old friends an colleagues, to be spoon-fed information, and to relax. On the other hand, I find myself in an electrophysiologic angst: how I can spend the time upbeat knowing that the relative value of the work that heart rhythm specialists do was cut at least 30% on 1 January 2013, thanks to new billing codes that bundled multiple codes into one?
Can I afford to be here?
I do not say this lightly. Our first quarter's pay this year compared to last year was recently disclosed and the results were striking. Guys like me who have devoted years to our training, stood at bedsides for countless hours, and endured training that finally ended at age 36 (counting a brief two-year hiatus for a general medical officer stint as an ER physician for the US Navy), got a whopping 30% cut from CMS for the much of the procedure work we do, stealthy cloaked in codes.
It is real. It has happened. And its effects are being felt by many, real time, even now, at #HRS2013.
I realize in these economic times that many professions are feeling similar pressures. I am not here to lament nor ask for pity, but rather to describe. In many ways, I am lucky: lucky to have good friends, a fascinating skill, and wonderful colleagues and support staff to work with. But I wonder, how all of this will change things.
Certainly, we tabled our plans to hire another EP. No wonder EP fellows are finding it tough to get a job. Hospitals are not hiring. Wards are being consolidated. Pennies are being pinched, and so are staff. Patients are waiting more to see guys like me. Attendance at continuing education conferences is falling. While the effect on physician care "quality" are probably uncertain at best, but it is becoming quite obvious that "innovation" in my field of medicine as we've known it is stagnating or moving overseas.
It is all change - I get that - part of the Great Experiment of our nation's health care reformation project that is moving fast and furious to places unknown. But change is difficult. It shakes things up. Anxiety and restlessness at times like these can consume a psyche or, in ideal circumstances, lead to something new, something liberating, something better.
So off I go to the 2013 Heart Rhythm Scientific Sessions, hoping to keep my chin up, my ear to the ground, and my eyes open.
You never know what you might learn.
-Wes
Sunday, May 05, 2013
Physician Blogger Insights On Social Media
A recent e-mail exchange between myself (WGF) and fellow-physician bloggers John M. Mandrola MD (JMM), Edward J Schloss MD (EJS) and Ves Dimov MD (VDMD) resulted in some interesting insights about how physicians are using social media tools today. The following is a lightly edited version of the thread (used with permission). It began with an e-mail from Dr. Mandrola:
* * *
* * *
* * *
* * *
For those attending the 2013 Heart Rhythm Society Scientific Sessions in Denver, CO next week, Drs. Schloss, Mandrola and myself (as well as Robert Coffield, Esq. of the Health Care Law Blog fame) will be speaking at the Rhythm Theatre at 3:15pm on 10 May 2013 on Physicians in Social Media.
Hope to see you there!
-Wes
PS: For doctors considering the leap to social media, here's a basic Twitter Primer.
JMM: "In prep for our Social Media session at HRS2103. I was just wondering…
Do you guys keep a list of favorites on Twitter? I have lists--but they aren't very effective logistically. I was wondering if I designed a list--say the Mandrola-twenty--of folks I did not want to miss, I might be able to use a column on TweetDeck. Right now, I follow 350 people--and it's unwieldy. But yet I have trouble parsing because I'll look at an acct and say to myself, "this one's pretty good; I don't want to unfollow." Also, I find TweetDeck sometimes intrusive. I use the reg Twitter app and often post with Hootsuite--because it allows me to link to 4 social networks at once--LinkedIn, FB, Twitter etc.
What Twitter app do you all use on Computer? On smartphone?
Do you have thoughts on Facebook (FB)? I see from the WSJ they are making a comeback so to speak. For a while there, I thought they might be dead.
Do you agree that Twitter seems more amendable to professional needs--the sort we all use it for: things like links, communication with colleagues, filtering of important medical news. I tend to use FB, the little that I do, for real life things like family, in-real-life friends and cycling stuff, for instance. I wonder whether this is a correct distinction, as most of the major journals and medical society have a FB presence. And likewise, Twitter has plenty of willy-nilly stuff like Hollywood, Athletes etc. The young people I know use Twitter more like I use FB."
EJS: "I also use Twitter almost strictly for professional stuff, especially my posts. I follow a few non-professional accounts, but am really choosy in general about followers. For my own posts, I try to picture someone looking down my timeline and trying to decide whether I'm worth their time to follow. If I put a bunch of cr*p up, I figure they'd move on. Twitter is also the predominant source of my online persona, and I'm really careful about maintaining this.
Right now I follow 239 accounts and not all are terribly active. That keeps the stream manageable. I actually get a popup on the laptop for every thing that posts to my timeline. Because I use my laptop for all hospital charting, this means I see A LOT of tweets. That setup is clearly not for everyone, but I've gotten good at just glancing up to see who is posting before I commit to reading. The tweets fill the dead and mindless spaces we get during EHR data entry (which are a lot). At any given time I'll also have 5 or 6 searches running that also generate popups. Right now these include meaningfuluse, St Jude Riata, Barry Meier, EHR, @burbdoc, #HRS2013 among others. All of these also generate popups.
If you want to filter down you list to highlight your most important accounts, you can set up a list in Tweetdeck (and I'm sure in the other clients, as well). That will become a column, and you could turn on alerts for just this stuff if you're not at ADD as me. I have a friends/family list that shows up on my front page so I can quickly see if I missed anything good without having to obsessively scroll back through everything.
On the laptop, I use Tweetdeck. The old version before Twitter bought it is the best, but will stop working in a few days. I've put up the new version, but don't like it as much. The biggest drawback is not having the profile photo on the popups. With the old Tweetdeck, it was easier to see who was posting with just peripheral vision.
On the iPhone and iPad I use Tweetbot. It's really good and worth the few bucks it costs.
I'd tell any cardiologist starting on twitter to follow a bunch of health care journalists, along with you guys. The interactions you get with the journalists are really rewarding, and truly are a two way street.
I really don't see much professional purpose for Facebook for an EP doc. If you were a plastic surgeon or ortho, maybe there would be a role. I'm actually trying not to market directly to patients, given the nature of my practice. Maybe you could pick up some AF that way, but I suspect a lot of nervous people with sinus tach or PACs would clog up your office if you did that.
VDMD: Hi John and colleagues,
Here are my answers:
re: "Do you guys keep a list of favorites on Twitter?" -- yes, I have 2 lists - 1. list of favorite tweets that I use as bookmark, 2. list of "allergists on Twitter".
re: "Mandrola-twenty--of folks I did not want to miss" - yes, KevinMD has that - top 20 Twitters he doesn't want to miss. I follow few people - less than 100, I think, and only 50 of them tweet regularly.
re: "What Twitter app do you all use on Computer? On smartphone?" - I use TweetDeck on my home PC, HootSuite at work (TweetDeck is blocked), and mobile Twitter on my Android phone. I "favorite"/bookmark the links I want to check later.
re: "Do you have thoughts on Facebook?" - Facebook (FB) is here to stay - until a new network replaces it. You have to use it to stay relevant if you have a blog. In addition, people look at the number of your likes to see how large a following you have as a blogger. FB has limitations and can be annoying but Google Plus is not a replacement yet. FB will evolve for sure, they are a young, aggressive company, and will keep searching for ways to combat "user fatigue".
These are some quick thoughts. Please let me know if you would like me to expand on any of these.
WGF: "Twitter is for the person with ADHD while blogs are for the obessive compulsive.
Twitter, by its very nature, has a low barrier for entry and can serve as an information "gatherer" initially. I'd encourage people to LURK first. It's easy to use and feeds lots of information of interest quickly to docs. As a "MUST HAVE" for doctors, they should follow the journals they subscribe to: Heart Rhythm, NEJM, Circulation, JACC, etc, as well as major news orgs: WSJ, CNN breaking news, local newsorgs or radios, etc. I also follow Steve Colbert for a laugh once in a while.
Twitter is also VERY useful for collaboration (as we have seen) and for "hunters" of information by using your network. I especially encourage follows of docs of the same subspeciality.
Facebook is for family/personal friends for me. No patients there. I find it's the best way to stay connected with my kids after they're out of the house.
As far as lists are concerned: I think they're a waste of time. I tried it, but since you cant send a targeted message or "tweet" to a list, it's only a way to group accounts.
I use Echofon on my iPhone (like it better than Hootsuite) - easy user interface and free. I use Tweetdeck on my PC and MAC.
I follow 446 people - probably too many - but it's a broad group that includes right and left-wing health care thinkers, IT nerds, politicians, bloggers, and you guys, and Steve Colbert. :)
Perhaps the most amazing use for Twitter (recently) was the immediacy of info provided there during the Boston bombings. It was unbelieveable how quickly updates happened and totally smoked the main news organizations. Imagine if doctors had a similar network at times of crisis! That's why I think it would be VERY cool to push that concept with our audience. Consider, for example, the need to get an EKG interpretation immediately (check my recent Twitter stream to see an example of just that) - lots of folks weighed in with ideas - some good - some bad - but in the end it was vetted pretty well.
Looking forward to this..."
VDMD: re: Journals on Twitter - I'm not a big fan of these. It's mostly the administrative staff pushing some articles they have picked. RSS feeds for the journals are much better, in my opinion. They save time and include most (all) articles of each issue.So there you have it. A sneek peak behiund the social media physician curtain on their take of current software, apps, and uses they find for social media in health care today.
For those attending the 2013 Heart Rhythm Society Scientific Sessions in Denver, CO next week, Drs. Schloss, Mandrola and myself (as well as Robert Coffield, Esq. of the Health Care Law Blog fame) will be speaking at the Rhythm Theatre at 3:15pm on 10 May 2013 on Physicians in Social Media.
Hope to see you there!
-Wes
PS: For doctors considering the leap to social media, here's a basic Twitter Primer.
Thursday, May 26, 2011
A Variant of "Where's Waldo?"
For doctors, there's a new game they can play at their next professional society's scientific meeting: "Where's the RFID Scanner?"
See if you can find them in this picture from this year's earlier Heart Rhythm Society Scientific session:

-Wes
See if you can find them in this picture from this year's earlier Heart Rhythm Society Scientific session:

Click to enlarge
-Wes
Thursday, May 05, 2011
Heart Rhythm Society Responds to Scrutiny Over Industry Ties
Tomorrow professional medical societies will be looking long and hard at how they disclose industry ties in response to an article published this evening by ProPublica (and co-published in USA Today) entitled: "Financial Ties Bind Medical Societies To Drug and Device Makers." The investigative reporting by Charles Ornstein and Tracy Weber examines the medical conference trade and the associated funding sources, focusing on the Heart Rhythm Society 2011 meeting underway in San Francisco. The report includes an interactive graphic, and slideshow of "promotional opportunities" available for purchase from the Heart Rhythm Society. The authors also organized the responses of 33 other prominent medical societies to an inquiry of Senator Charles Grassley's regarding funds they receive from the pharmaceutical and medical device industries. There is much for the public to learn here.
But what should not go un-noticed, however, is the Heart Rhythm Society's willingness to "bear all" about their practices. In fact, they answered, head-on, questions posed to them by the ProPublica reporters. In this respect, they should be commended for pulling back the curtain on the sources of funding for these scientific sessions and their operations.
It will be interesting to see if other medical societies are as forthcoming as the Heart Rhythm Society has been. What is clear is that as dollars get tighter and tighter for health care, the scrutiny of these practices and their potential to influence doctors will only continue to intensify.
-Wes
But what should not go un-noticed, however, is the Heart Rhythm Society's willingness to "bear all" about their practices. In fact, they answered, head-on, questions posed to them by the ProPublica reporters. In this respect, they should be commended for pulling back the curtain on the sources of funding for these scientific sessions and their operations.
It will be interesting to see if other medical societies are as forthcoming as the Heart Rhythm Society has been. What is clear is that as dollars get tighter and tighter for health care, the scrutiny of these practices and their potential to influence doctors will only continue to intensify.
-Wes
Sunday, April 24, 2011
The Implications of Physician Tag and Release
Recently, a disturbing trend of monitoring physician quality and accountability has taken another ominous turn: tracking physician's movements at scientific conferences (so called "tag and release") using RFID tags imbedded in attendees name badges at national scientific sessions. Having had personal experience with the recent American College of Cardiology meeting, this technology will also be imbedded in the name badges for attendees at the upcoming Heart Rhythm Society meeting to be held in San Francisco in May.Not everything that counts can be measured.
Not everything that can be measured counts.
-Albert Einstein
On first blush, it shouldn't be such a big deal, right? It was all just a great way for companies to obtain, for a fee, the names and institutions of people who visited their display booths and for the conference organizers to track the movements of attendees. (Heck, maybe they can partner with an industry sponsor to pick up our traffic tolls on the way to the conference hall or arrange other exciting activities for us! [Said tongue-in-cheek, of course])
Instead of "opting in" for tracking at scientific meetings, doctors must "opt out" from the use of tracking technology when registering for scientific meetings. At the upcoming Heart Rhythm Society meeting for instance, doctors had to "opt out" from the use of RFID technology tracking by checking a box that says:
Badge scanning technology will be utilized at this event in order to better understand attendee/delegate interests and preferences. The information collected will be used to improve future events to better address your preferences. No personal information is stored in the RFID badge, only an ID number. We encourage all participants to take part in this process to ensure the most accurate data is obtained. You may check this box to opt-out of the RFID data collection.There's full disclosure, doctor.
But to me, the default tracking of doctors is disturbing on several levels.
First, tracking was approved by our professional society organizers upon their own members. It is no secret that these societies make a significant portion of their operating revenues from industry sponsors at these meetings. By instituting tracking, the value of their membership's privacy has taken a back seat to the income generated from tracking revenues. By NOT checking a box, we have implicitly "agreed" to this tracking. (Realize we MUST wear our badge to attend these conferences where we gain our REQUIRED continuing education credits.) Because we have "agreed" in this manner, the tracking data are now legally "discoverable." At the risk of sounding like a conspiracy theorist, it is not too hard to imagine one's credentials being called into question in court because a doctor did not demonstrate enough time in CME activities at the scientific sessions to quality for credit or because these data implicate a doctor in a purchasing agreement between a vendor and hospital system simply because a doctor visited a display booth.
Doctors have seen this sort of activity before when "only" our license and demographic information was sold by the American Medical Association (AMA). The AMA currently "licenses" physician state medical license numbers and demographic information to health care information organizations (HIOs), HIOs then collect and compile this information with prescribing data that contains the doctors' license numbers (no names, mind you) and then sell the lists to pharmaceutical companies. The AMA tells its members it does "not collect, license, sell or have access to physician prescribing data" and this is true. But the AMA facilitates an intermediary's ability to pair doctors' license information to a their prescribing habits via a third party. One can only speculate how out prescribing and practice profiles are being developed by other similar health information companies with the use of our RFID tracking data.
Behind all of this is a bigger issue: doctors are frustrated by the increasing intrusion into our day-to-day practice of medicine to measure things. Take, as one example, our "quality performance measures" that have done little to facilitate patients office visits, but rather add burdonsome documentation requirements in the interest of government payments. A number of hospital administrators have confided in me that it costs more to collect this data than they make in government payments. In fact, whether these programs are ultimately are found to be cost-effective or improve the quality of care has been brought into question in our literature. Yet we continue to collect these measures and expand them. We are now dispatching legions of people to collect and compile data to "prove" that Electronic Medical Records are used in a "meaningful" way. But an honest appraisal of this policy discloses the reality: these measures permit health care systems to collect another $40,000 per doctor from the government because they are using computers, not because it improves patients' care in any "meaningful" way. As proof of the overburdensome nature of all this data collection for the physician, doctors (or their health care systems) are increasingly employing "scribes" to relieve them of the data-entry burdens in the name of "efficiency." How much, exactly, do these scribes cost our health care system? Few dare to ask the question since no one wants to deny themselves of that juicy $40,000 pot of gold being paid per doctor.
Adding insult to injury, all doctors will soon be required to disclose if we receive anything over $100 from industry representatives. Like the public, most of us recognize the pernicious nature of industry influence upon our profession. Yet we now find we are being used. Should our professional organizations be any less forthright with their industry dealings and the use of our demographic data at national scientific sessions? How much is at stake?
Finally, we see more and more onerous licensure requirements and fees paid to the same tag-and-release operatives at considerable cost to ourselves. We now spend thousands of dollars to remain "credentialed." We wonder how much the RFID "return on investment" to industry sponsors adds to our annual membership fees. Could it reduces them? Who knows? Maybe, like other IT models, we should insist our membership fees be waived if we agree to being RFID tagged and released because most of us realize someone's making money on this deal.
In summary, doctors increasingly find the imperative to guard the privacy of our patients without regard to our own personal and professional privacy with the very same patients disturbing. Everything about doctors is being measured these days and it's taking its toll on patient care. We are frustrated with the governmental bureaucratic standards that threaten our time with patients. But time with patients does not pay bills. Meeting data-collection milestones do. Our government and employers have lost sight of the main issue here: improving and expanding our contact with (and the ability to do good for) our patients.
But as long as there is money to be made with our personal information, it is clear that there will be those that will try to capitalize upon it, whether we realize it or not. Only by demanding constant accountability and transparency from the collectors of this information be they government bureaucrats or our professional society appointees, can we hope to maintain any modicum of professionalism in our tenuous doctor-patient relationships of the future.
-Wes
Thursday, January 20, 2011
DOJ Investigating Defibrillator Implanters
From the Heart Rhythm Society member's website today:
Now all of us know people make money implanting ICD's, including me. Given the time, the expertise, and the management issues involved with the 24/7 care of the patients with these devices, they should.
But no one wants to waste money to our health care system, either, and we must acknowledge there's been a heck of a marketing push to get more devices implanted. This has occurred because many patients who might benefit (legitimately) from these devices remain untreated and, yes, hospitals and medical device companies benefit handsomely from these procedures.
But before witch hunts ensue, we should take a moment and consider the implications of the DOJ's current actions.
First of all, I think most of us would acknowledge that every set of clinical guidelines published has holes. (One only has to look at the latest published atrial fibrillation management guidelines to note that the use of the newly-released anticoagulant dabigatran (Pradaxa) is not mentioned in those guidelines, rendering them already obsolete). Further, the studies upon which recommendations are made in published guidelines are often made on relatively weak data or by people with substantial industry ties. Further, prospective randomized trials are rarely used to make those recommendations.
Simply put, there is no way a published document can cover every clinical circumstance a doctor might encounter when he or she is in the trenches with an individual patient.
So this begs a simple question: If guidelines are not perfect and we must accept that doctors must deviate from them from time to time to work toward the best interest of their patient, what IS the percentage of care (in this case, ICDs) that SHOULD fall outside of guidelines?
Is 0% the correct number?
Clearly, no.
Is 5%, 10%, 15%, 20%, 22%?
The reality of this situation is that no one knows.
But that does not seem to be stopping the DOJ from investigating doctors for their criminal intent...
... based on the guidelines, of course.
-Wes
References:
Al-Khatib SM, Hellkamp A, Curtis J, et al. Non-evidence-based ICD implantations in the United States. JAMA 2011; 305:43-49.
Dr. Rich over at the Covert Rationing blog appropriately rips the abuse of the ICD guidelines in his must-read essay.
John Mandrola, MD, another EP, gives his take.
Larry Husten, at Cardiobrief, summarizes.
21 Jan 2011: An now, thanks to new SCD-HeFT data, maybe the 40-day wait period post-MI for ICD's is not such a good idea. Oh wait, that's not in the guidelines.
"The Heart Rhythm Society (HRS) is aware of an ongoing U.S. Department of Justice (DOJ) civil investigation of Implantable Cardioverter Defibrillator (ICD) implants and has agreed to assist in an advisory role to lend expertise concerning proper guidelines for clinical decision making. As an advisor to this investigation, HRS is reviewing information that does not include either identifiable patient or facility level data. Rather, we are providing insight on the field of electrophysiology to the DOJ. Because this is an ongoing investigation, HRS Staff or Leadership is not available for further comment. HRS will communicate additional information to its membership when permitted to do so by the DOJ."This action comes, no doubt, on the heels of the recent publication in JAMA which reviewed an ICD registry of implantation practices in America from 2006 to 2009 and found 22% of ICD implants were implanted outside published guidelines.
Now all of us know people make money implanting ICD's, including me. Given the time, the expertise, and the management issues involved with the 24/7 care of the patients with these devices, they should.
But no one wants to waste money to our health care system, either, and we must acknowledge there's been a heck of a marketing push to get more devices implanted. This has occurred because many patients who might benefit (legitimately) from these devices remain untreated and, yes, hospitals and medical device companies benefit handsomely from these procedures.
But before witch hunts ensue, we should take a moment and consider the implications of the DOJ's current actions.
First of all, I think most of us would acknowledge that every set of clinical guidelines published has holes. (One only has to look at the latest published atrial fibrillation management guidelines to note that the use of the newly-released anticoagulant dabigatran (Pradaxa) is not mentioned in those guidelines, rendering them already obsolete). Further, the studies upon which recommendations are made in published guidelines are often made on relatively weak data or by people with substantial industry ties. Further, prospective randomized trials are rarely used to make those recommendations.
Simply put, there is no way a published document can cover every clinical circumstance a doctor might encounter when he or she is in the trenches with an individual patient.
So this begs a simple question: If guidelines are not perfect and we must accept that doctors must deviate from them from time to time to work toward the best interest of their patient, what IS the percentage of care (in this case, ICDs) that SHOULD fall outside of guidelines?
Is 0% the correct number?
Clearly, no.
Is 5%, 10%, 15%, 20%, 22%?
The reality of this situation is that no one knows.
But that does not seem to be stopping the DOJ from investigating doctors for their criminal intent...
... based on the guidelines, of course.
-Wes
References:
Al-Khatib SM, Hellkamp A, Curtis J, et al. Non-evidence-based ICD implantations in the United States. JAMA 2011; 305:43-49.
Dr. Rich over at the Covert Rationing blog appropriately rips the abuse of the ICD guidelines in his must-read essay.
John Mandrola, MD, another EP, gives his take.
Larry Husten, at Cardiobrief, summarizes.
21 Jan 2011: An now, thanks to new SCD-HeFT data, maybe the 40-day wait period post-MI for ICD's is not such a good idea. Oh wait, that's not in the guidelines.
Thursday, May 14, 2009
Heart Rhythm Society Scientific Meeting Quiet

Boston Convention Center May, 2009
Well, maybe the Heart Rhythm Society Meeting wasn't quite as bad as depicted in the above photoshopped image, but there's no question that attendance was lighter than I have remembered it in some time this year.
There were a number of factors for this: I am told a whole contingent of doctors from Japan were held back because of the lingering concerns of Swine flu. Then there's the fact that the Boston Atrial Fibrillation Summit was here earlier this past winter (who wants to travel to the same city twice?), and finally and perhaps most importantly, the recession. I met one nurse from Vanderbilt (Nashville, TN) who noted that all elective travel was suspended as a cost-saving measures in place. She only attended because she was paid to come and speak to a session for Allied Health professionals, effectively making her attendance at the meeting cost-neutral for her.
Now while this might not seem like a big deal, the implications to limiting continuing medical education to our health care team is concerning. But it's an easy thing to cut, right? After all, a penny saved is a penny earned. But what are the long-term implications for patient care if funds for continuing education are sacrificed? Certainly, if the downturn is brief, missing a meeting or two probably won't have much effect... or will it? Do we know?
And yet, despite this, the usual regiment of sales representatives for companies eager to get their face in front of doctors were ever-present. But the mood seemed muted, uncertain, as device companies were doing their best to stay upbeat despite the economic uncertainty. All were aware that Massachusetts, the home of the original North American Society of Pacing and Electrophysiology (from which the Heart Rhythm Society morphed) and home of the current organization's president, will implement a law 1 July 2009 prohibiting medical device companies and pharmaceutical companies from courting their physician customers at these meetings. (No wonder the Heart Rhythm Society moved from Massachusetts to Washington, DC, eh?) While I understand the implications of the law, will this trend continue nationwide? Are medical conventions and doctor meetings as we've known them a thing of the past? Will we just meet online instead as the ultimate cost-saving trend?
Hopefully not. But it was not easy to see a definite change is occurring, and it's coming faster than we think.
Well, got to board the plane back to Chicago. See you back home soon.
-Wes
Tuesday, May 12, 2009
Heart Rhythm Society Meeting 2009
The Heart Rhythm Society's Scientific Sessions will kick off tomorrow in Boston, MA. This is where the latest and greatest ideas in heart rhythm management and research are shared. It offers valuable educational content, but also serves as a wonderful social backdrop to meet old friends and colleagues from around the world. It is here we reconnect, if ever so briefly. I'm not sure about the blog, the twittering, or whatever over the next few days since my stay will actually be very short this year - clinical coverage back home require it to be so.
But one thing I would like to see is a session entitled "Tales from the Unknown EPs" delivered by EP's who have never spoken at this conference around the country discussing their issues. It seems every year I go to this meeting, I always here from the same folks n similar topics. Not that they don't do a fine job, but it would nice to hear how common EP folks around the country are dealing with atrial fibrillation ablation at smaller institutions, or with their local cardiologists implanting defibrillators instead of them. Sessions like that can get pretty interesting! (heh, heh)
But we'll see what I can learn in the short two days I'll be there. I can never cover all the topics at a meeting this large, but if I find some new stuff, I'll be sure to share.
Cheers-
-Wes
But one thing I would like to see is a session entitled "Tales from the Unknown EPs" delivered by EP's who have never spoken at this conference around the country discussing their issues. It seems every year I go to this meeting, I always here from the same folks n similar topics. Not that they don't do a fine job, but it would nice to hear how common EP folks around the country are dealing with atrial fibrillation ablation at smaller institutions, or with their local cardiologists implanting defibrillators instead of them. Sessions like that can get pretty interesting! (heh, heh)
But we'll see what I can learn in the short two days I'll be there. I can never cover all the topics at a meeting this large, but if I find some new stuff, I'll be sure to share.
Cheers-
-Wes
Friday, May 16, 2008
Heart Rhythm Society Meeting 2008: A Conversation Overheard

“I always enjoy meeting old friends at this meeting.”
“Me, too.”
“Learned anything?”
“A few things, but there doesn’t seem to be much new.”
“I know what you mean.”
“It just seems to be the same old researchers and companies. But there's just so much more over-the-top marketing going on. God, if I see one more 256-color mapping system with little dots all over the left atrium, all claiming to be better than the next system, I'm gonna puke! There must be huge budgets to promote this stuff – most of which does help a rat’s ass at fixin’ the frickin’ afib – it looks more like a radiology meeting than an EP meeting. And did you see? Boston Scientific miraculously got their new devices approved by the FDA three to four months earlier than expected they said and yet, boy, somehow they had all the displays up already – like they “knew” all along! What a crock...."
* * * Laughing * * *
“Hey, do you know what that (Medtronic) ‘Vision 3D’ on that go-cart over there means?”
“No. Do you?”
“No clue. But man, did you see it’s plastered on the sides of the buildings and the stairs and frickin’ everywhere?. I heard someone say they got pissed that they were out-marketed by the other guys at last year’s conference, so they decided to go all out this year. I do kind of like those little go-cart thingies... maybe they should use those as shuttles to the hotels..."
“The commercialism just seems over-the-top. The *&#$*# poster sessions were like an afterthought – HRS gave more convention floor space to the companies than the poster display areas. There were so many people, I couldn’t even walk between the rows of posters! All that work – overshadowed by corporate displays.”
“Yeah, I know what you mean. The abstract sessions today – you know, the good, stuff – I heard there were 23 different sessions running concurrently. How could we even see a small portion of that?”
“You know what I think?”
“What?”
“I think that if they keep this up, that lots of folks will stop coming and just wait to see the presentations online.”
-Wes
Subscribe to:
Comments (Atom)