What do US cardiologists and electrophysiologists REALLY think about the American College of Cardiology's (ACC) heavily-promoted collaboration with the American Board of Internal Medicine (ABIM) to create their "Continuous Maintenance Pathway" (CMP) for continually maintaining their ABIM board certification?
That's a question I wanted to know, so I helped create a quick 5-minute survey on the matter open to US cardiac electrophysiologists, cardiologists, and heart failure specialists.
I hope to have the results compiled by the Heart Rhythm Society in May, 2019.
I look forward to your responses and thoughts. Additional comments regarding the CMP program not covered in the survey can be left in the comments on this blog post.
Thanks-
-Wes
Showing posts with label American College of Cardiology. Show all posts
Showing posts with label American College of Cardiology. Show all posts
Tuesday, April 02, 2019
Sunday, July 26, 2015
American College of Cardiology and the MOC Crisis
This week's issue of the Journal of the American College of Cardiology (JACC) contains an editorial from Robert Shor, MD, Chair of the American College of Cardiology (ACC) Board of Governors entitled "Addressing the Maintenance of Certification Crisis Calls for Working Together." The editorial touches on the relationship of the American Board of Medical Specialties (ABMS) and the American Board of Internal Medicine (ABIM) and that "ACC-sponsored polls have shown that the vast majority of cardiologists have concerns about the validity, relevance, utility and associated financial and opportunity costs of meeting these revised (MOC) requirements."
Importantly, the editorial also mentioned several other well-known facts: that new 2014 MOC rules established by the ABIM that "required newly graduated fellows who have successfully completed their initial certifying examination to also sign up for ABIM MOC or be listed as "not certified."
Fortunately for our most vulnerable new cardiologists, the ACC is pressuring the ABIM to revise this policy that financially benefits the ABIM exclusively. It seems the ABIM will stop at nothing to monopolize the recertification market for themselves.
While the ACC Leadership under Dr. Shor 's direction seems sincere, his letter ignores the financial cover-up at the ABIM, specifically the fees that were funneled from the ABIM to the ABIM Foundation from 1989 to 1999, the lavish salaries of the officers and staff there, and the fact the ABIM remains has a balance sheet that is over $47 million in the red. Instead, the chooses to "be cautious because we realize the complexity of the situation." Dr. Shor continues with a half-truth, saying: "In the interim, all of us have alternatives. These include joining a new board, waiting to see the final ABIM proposal, and waiting to see if an alternative ACC board is feasible and/or needed."
Because of the regulatory capture created by the ABMS and their demand for "recertification," contrary to Dr. Shor's statement practicing physicians do NOT have a choice avoid ABIM recertification. Practicing physicians cannot "wait." Practicing physicians MUST continue on their ABIM recertification pathway lest they lose their hospital privileges or aren't allowed to participate on insurance panels to receive payment for services.
We should note that after revealing ABIM lobbying efforts that were not disclosed the ABIM's tax forms on 31 May 2015, the ABIM terminated their relationship with their lobbying firm on 30 June 2015.
It is increasingly clear that the ABIM and the ABMS have constructed a lucrative money stream for themselves thanks to "recertification" at the expense of practicing physicians. Recertification after initial certification still has no Level A evidence that it improves patient outcome or care. Instead, as clearly documented on this blog and elsewhere, recertification has been proven to be a corrupt and potentially illegal process that demands thorough investigation by the IRS, Iowa and/or Pennsylvania Attorney Generals, and the US Attorney General or the Inspector General of the Department of Health and Human Services.
This is where the ACC should insist on action. It is simply not in keeping with the highest standards of medical ethics and integrity to collude with organizations that have shown themselves to be working in their own interests over those of practicing physicians and their patients everywhere.
-Wes
Importantly, the editorial also mentioned several other well-known facts: that new 2014 MOC rules established by the ABIM that "required newly graduated fellows who have successfully completed their initial certifying examination to also sign up for ABIM MOC or be listed as "not certified."
Fortunately for our most vulnerable new cardiologists, the ACC is pressuring the ABIM to revise this policy that financially benefits the ABIM exclusively. It seems the ABIM will stop at nothing to monopolize the recertification market for themselves.
While the ACC Leadership under Dr. Shor 's direction seems sincere, his letter ignores the financial cover-up at the ABIM, specifically the fees that were funneled from the ABIM to the ABIM Foundation from 1989 to 1999, the lavish salaries of the officers and staff there, and the fact the ABIM remains has a balance sheet that is over $47 million in the red. Instead, the chooses to "be cautious because we realize the complexity of the situation." Dr. Shor continues with a half-truth, saying: "In the interim, all of us have alternatives. These include joining a new board, waiting to see the final ABIM proposal, and waiting to see if an alternative ACC board is feasible and/or needed."
Because of the regulatory capture created by the ABMS and their demand for "recertification," contrary to Dr. Shor's statement practicing physicians do NOT have a choice avoid ABIM recertification. Practicing physicians cannot "wait." Practicing physicians MUST continue on their ABIM recertification pathway lest they lose their hospital privileges or aren't allowed to participate on insurance panels to receive payment for services.
We should note that after revealing ABIM lobbying efforts that were not disclosed the ABIM's tax forms on 31 May 2015, the ABIM terminated their relationship with their lobbying firm on 30 June 2015.
It is increasingly clear that the ABIM and the ABMS have constructed a lucrative money stream for themselves thanks to "recertification" at the expense of practicing physicians. Recertification after initial certification still has no Level A evidence that it improves patient outcome or care. Instead, as clearly documented on this blog and elsewhere, recertification has been proven to be a corrupt and potentially illegal process that demands thorough investigation by the IRS, Iowa and/or Pennsylvania Attorney Generals, and the US Attorney General or the Inspector General of the Department of Health and Human Services.
This is where the ACC should insist on action. It is simply not in keeping with the highest standards of medical ethics and integrity to collude with organizations that have shown themselves to be working in their own interests over those of practicing physicians and their patients everywhere.
-Wes
Friday, March 13, 2015
Scientific Meetings Are Becoming MOC Training Sessions
Tomorrow marks the beginning of the 2015 American College of Cardiology (ACC) Scientific Sessions in San Diego, CA. This morning I was struck by the "Schedule At-a-Glance" sent to registrants participating in these sessions:
Using Photoshop, I decided to rearrange the schedule in a linear graph format day-by-day instead:
As we can clearly see, the time devoted to Maintenance of Certification Study Sessions exceeds that of other collegial scientific and learning opportunities.
Does the American College of Cardiology really value the development of physician test-taking skills for the American Board of Medical Specialties Maintenance of Certification® program over the sharing of innovative ideas and scientific content at our largest world-wide cardiology meeting?
It would appear the largest purpose of our national meetings has changed to quelling the fear and implications of failing the ABMS MOC secure examination. I wonder what cardiovascular physicians and patients are losing as a result of this coercive and corrupt program being foisted upon us.
-Wes
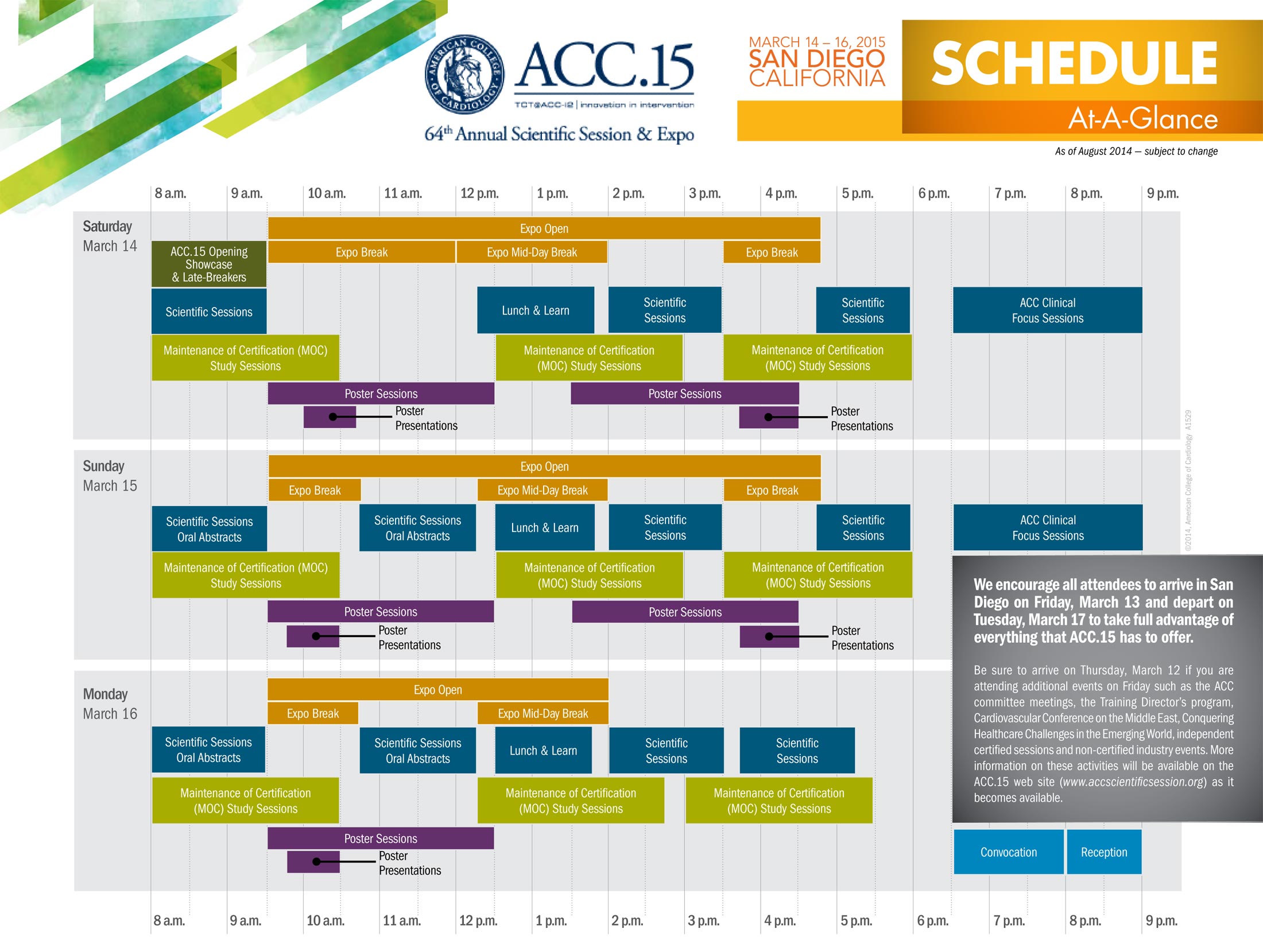 |
| ACC.15 Schedule at a Glance - Click to enlarge |
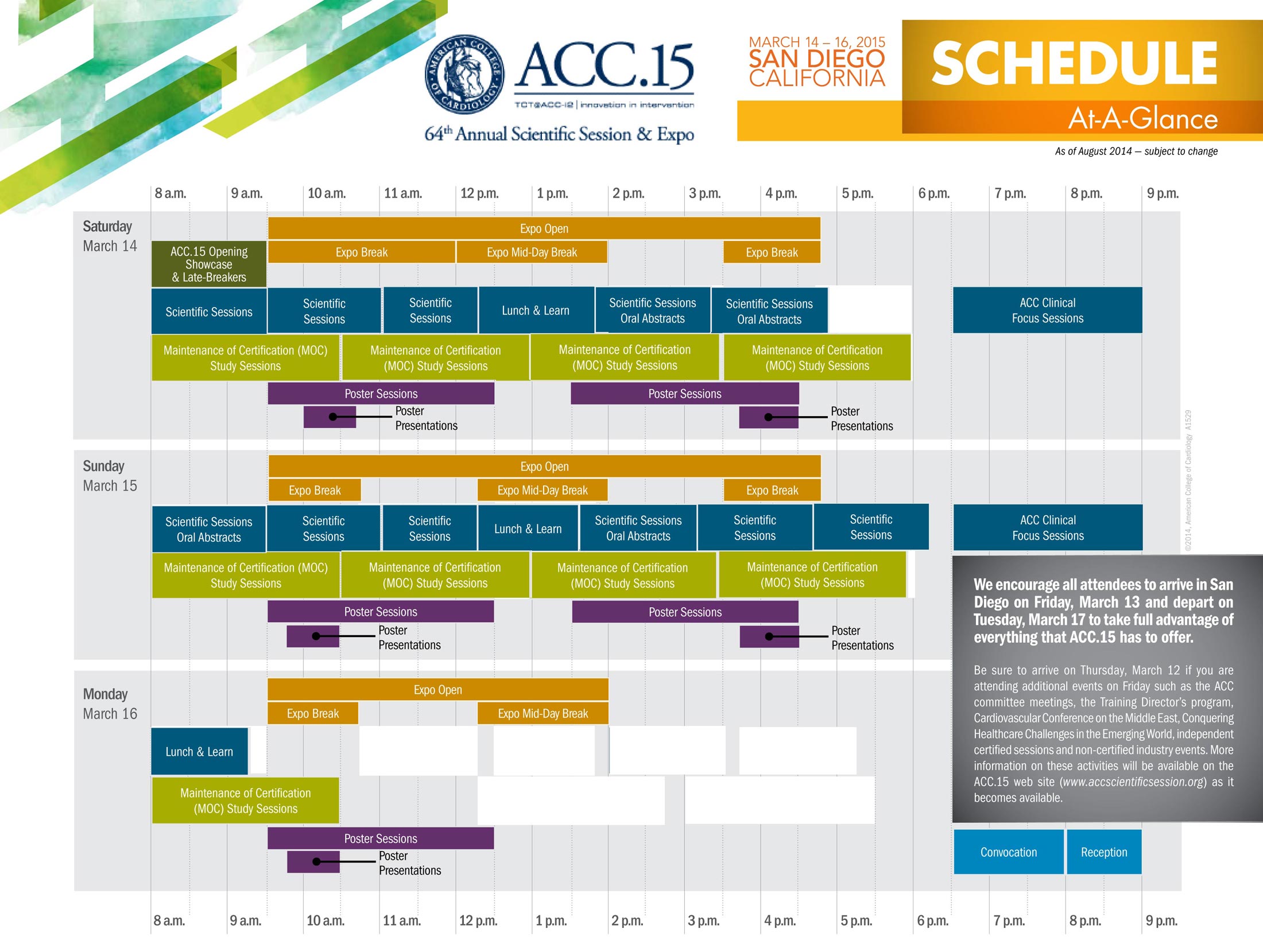 |
| ACC.15 Schedule Rearranged in Graphical Format - Click to enlarge |
As we can clearly see, the time devoted to Maintenance of Certification Study Sessions exceeds that of other collegial scientific and learning opportunities.
Does the American College of Cardiology really value the development of physician test-taking skills for the American Board of Medical Specialties Maintenance of Certification® program over the sharing of innovative ideas and scientific content at our largest world-wide cardiology meeting?
It would appear the largest purpose of our national meetings has changed to quelling the fear and implications of failing the ABMS MOC secure examination. I wonder what cardiovascular physicians and patients are losing as a result of this coercive and corrupt program being foisted upon us.
-Wes
Tuesday, March 10, 2015
Where Will Social Media Be in Five Years?
Where will social media be in five years? Will it be dead? Will it be thriving? What will it look like?
This was just one question posed to me as a speaker in this topic for the 2015 American College of Cardiology Scientific Sessions in San Diego this upcoming weekend. Here are some of my thoughts and I'd love to hear what others think (I need CONTENT people!) since I'm really not an expert:
Your thoughts?
-Wes
This was just one question posed to me as a speaker in this topic for the 2015 American College of Cardiology Scientific Sessions in San Diego this upcoming weekend. Here are some of my thoughts and I'd love to hear what others think (I need CONTENT people!) since I'm really not an expert:
- The word "social" in "social media" will disappear.
- The term "rectangle deficiency" (aka, misplaced cellphone) will achieve DSM-V status.
- True privacy will be the "new black" for medicine (as will actually looking at the patient).
- Text messaging will overwhelmingly replace paging for day-to-day patient care.
- Research will increasingly recruit patients via this channel.
- Credible content on social media will be recognized and even encouraged by academic institutions.
- US physician attendance at Scientific sessions will further dwindle due to costs while subsidized overseas physician attendance will grow.
- The Apple iWatch will be so, well, yesterday...
Your thoughts?
-Wes
Tuesday, January 13, 2015
Some Thoughts on the National Board of Physicians and Surgeons
I admire Paul Tierstein, MD's honest attempt to create a greatly simplified alternative to the ABMS's Maintenance of Certification® (MOC) program called the National Board of Physicians and Surgeons (NBPAS). I hope he's successful, but I sense there will be large headwinds for the effort ahead.
Here's why.
The Affordable Care Act (ACA) modified Sections 1848(k) and 1848(m) of the Social Security Act which defines how CMS pays physicians for their services. Section (k) is the section that defines how a "Quality Reporting System" is to be set up (with subsection (4) requiring the "Use of Registry-based Reporting") and Section (m) defining physician incentive payments physicians might receive if quality reporting occurs properly. (Sadly, those CMS incentive payments do not cover the cost of participating in MOC for most of us.)*
Section (k) was modified by the ACA to include the ABMS MOC program as a "physician registry." The registry was "defined" as requiring all four parts of the MOC program created by the ABMS, including the much-maligned "practice improvement modules" that have been described by the physician community as overly time-consuming, irrelevant and may even violate federal research statutes regarding the study of physicians, their practices, and patients.
Unfortunately the new NBPAS does not address these requirements of the our new health care law, leaving the creation of the NBPAS to look like a Rand Paul moment all over again with physicians signing up for something that, legislatively, means nothing.
Welcome to the concept of "regulatory capture."
Physicians should realize that special interests and their lobbyists (including the US hospital, pharmaceutical, survey companies, and insurance lobbying groups) were highly influential in the creation of our new health care law. They are also very good at politics. It is unlikely that these entities want to see MOC go away, irrespective of how corrupt the system has become. There's just too much money involved. Even our own specialty societies use the MOC program's educational requirements to coerce physicians to take their educational courses to "earn MOC points" to help pad their bottom lines as physician attendance (and corporate sponsorship) at scientific sessions has dwindled over the past years.
But what's more important to our patients in the long run? Time for their needs or time for test-taking and survey collection? Is it more important to satisfy government requirements or address the real needs of our patients? Certainly continuing education of physicians is needed, but irrelevant work for an unaccountable third-party organization so they can measure us rather than help us is not.
Physicians need to take the stick, but we can't do this alone since we care for patients. So we need to ask this question: will our specialty societies commit to supporting practicing physicians or the new bureaucratic divide? (They can't do both.) Will they truly step up to the plate and commit their considerable staff, dollars, pager-less hours, lobbying and legislative efforts to help remove the corrupt MOC program from the Affordable Care Act or allow practicing physicians - their members - to wallow in the corrupt status quo as they are coerced to participate in MOC?
I remain pessimistic that creating another "board" will fix the current deep-seated problems with the ABMS MOC construct with ABMS as the mothership directing a flotilla of 24 member boards. In my view the only way to truly "change" MOC is to have a coordinated effort from all specialty societies to insist our legislators remove the portion of our new health care law that requires we participate in a "physician registry" that robs not only practicing physicians, but patient care itself.
HRS and ACC, are you on board?
-Wes
*Addendum 2/12/2015:
It should be noted that the payment incentives offered 2012-2104 from CMS for participation in MOC ended January 1, 2015, but that MOC participation will still be used as a physician quality reporting metric.
Here's why.
The Affordable Care Act (ACA) modified Sections 1848(k) and 1848(m) of the Social Security Act which defines how CMS pays physicians for their services. Section (k) is the section that defines how a "Quality Reporting System" is to be set up (with subsection (4) requiring the "Use of Registry-based Reporting") and Section (m) defining physician incentive payments physicians might receive if quality reporting occurs properly. (Sadly, those CMS incentive payments do not cover the cost of participating in MOC for most of us.)*
Section (k) was modified by the ACA to include the ABMS MOC program as a "physician registry." The registry was "defined" as requiring all four parts of the MOC program created by the ABMS, including the much-maligned "practice improvement modules" that have been described by the physician community as overly time-consuming, irrelevant and may even violate federal research statutes regarding the study of physicians, their practices, and patients.
Unfortunately the new NBPAS does not address these requirements of the our new health care law, leaving the creation of the NBPAS to look like a Rand Paul moment all over again with physicians signing up for something that, legislatively, means nothing.
Welcome to the concept of "regulatory capture."
 |
| Screenshot of Heart Rhythm Society webpage |
But what's more important to our patients in the long run? Time for their needs or time for test-taking and survey collection? Is it more important to satisfy government requirements or address the real needs of our patients? Certainly continuing education of physicians is needed, but irrelevant work for an unaccountable third-party organization so they can measure us rather than help us is not.
 |
| A second Heart Rhythm Society webpage devoted to MOC |
I remain pessimistic that creating another "board" will fix the current deep-seated problems with the ABMS MOC construct with ABMS as the mothership directing a flotilla of 24 member boards. In my view the only way to truly "change" MOC is to have a coordinated effort from all specialty societies to insist our legislators remove the portion of our new health care law that requires we participate in a "physician registry" that robs not only practicing physicians, but patient care itself.
HRS and ACC, are you on board?
-Wes
*Addendum 2/12/2015:
It should be noted that the payment incentives offered 2012-2104 from CMS for participation in MOC ended January 1, 2015, but that MOC participation will still be used as a physician quality reporting metric.
Monday, July 28, 2014
Should Cardiologists Boycott the 2014 TCT/ACC Conference?

In reality, most cardiologists couldn't care less about Ms. Clinton. They'll oversleep or consider her address as nothing more than marketing theater. But to dismiss Ms. Clinton's presence at this event misses some important considerations.
Is the purpose of the TCT conference to hobnob and aggrandize politicians, especially one who could become President, or is to educate and inform physicians? Is the purpose of paying Ms. Clinton's hefty speaking fee about gaining her ear, or to make a political contribution from Big Business and the crony capitalism that pervades health care now? Is the real purpose to of her presence as keynote speaker to address cardiologists real concerns or so that ACC leadership can position their proprietary NCDR databases and "Appropriateness Criteria" as quality metrics to permanently pad their bottom line? Suddenly, Ms. Clinton's appearance takes on more cardiovascular gravitas.
Every cardiologist sitting in that hall will have just come through a year experiencing less time with their patients, less clinical autonomy, intrusions on their practice, while increasingly being coerced to perform bureaucratic tasks that mean little to patients yet everything to corporate interests. What do we imagine will, in fact, be addressed by Ms. Clinton as we buy our plane tickets and carefully pack our suitcases? Do we think for one moment that Ms. Clinton or the ACC will have the slightest compunction to address the serious concerns of the cardiology community? What do we imagine the ACC will address about these concerns in the rest of the meeting?
ACC should wake up to a new reality. Recall that it was a small group of cardiologists who started the anti-Maintenance of Certification (MOC) petition against the new, more onerous MOC program devised by the privately held American Board of Medical Specialties and the American Board of Internal Medicine. Over 18,000 doctors of all types have signed that petition now. In response to that petition, the ACC performed a survey of their member chapters nationwide. The anti-MOC sentiment from this survey was overwhelming. Many senior doctors even mentioned it might make them consider early retirement. In turn, the ACC's response was lukewarm at best. This was likely because the ACC's history has been to support the lucrative review courses this program requires. These courses are so important to the ACC's bottom line that they even devoted an entire "MOC Complex" hall at their last scientific session to promote the MOC program and still aggressively market the program on their website. This is hardly a show of solidarity with their member cardiologists'.
{kind=link}
It is time front line cardiologists put action behind their anger over the MOC process and the ACC's indifference. It is time to consider a boycott of the ACC/TCT meeting in Washington.
To that end, the ACC leadership needs to stop pandering to politicians and corporations eager to profit on doctors and instead start advocating for their own members. The preeminent assumption in program planning at events such as these appears to be that physicians are passive, apolitical, and unaware. Why would the ACC or any other physician membership organization feel the need to change? For this reason, the time to boycott is now. If the boycott is successful, perhaps the ACC leadership will take the concerns of the member cardiologists' more seriously than the politics of creating public-private partnerships that threaten to compromise, rather than promote, the care of our patients. Does the ACC really believe they can remain relevant without physician participation? We should note that alternative professional organizations are beginning to evolve.
Whether the ACC has realized this or not, they are coming to a juncture where they will have to decide whether they represent physicians and their patients or the Iron Triangle. Physicians are not lawyers, they are uncomfortable acting collectively or politically, much to their detriment in this era of rapidly morphing health care regulation and intrusion. I can still hope that the ACC and other organizations such as state medical societies will have the capacity to represent the real interests of their physician members. But increasingly I am concerned they won't.
But we should be clear: physicians' actions mean something. So this doctor will not be attending this year's meeting because it's one of the only ways I have left to send a message.
I hope others will consider the same.
-Wes
Tuesday, June 03, 2014
On the ACC's Response to ABIM’s MOC Requirements
The American College of Cardiology (ACC) recently issued a response to the American Board of Medical Specialties (ABMS) and American Board of Internal Medicine's (ABIM) recent change to their Maintenance of Certification (MOC) requirements. The ACC's response was based in part on the results of a completed member survey that was distributed through their state chapters in the spring of 2014. The survey was completed within four weeks by over 4,400 members (12 percent of the total solicited). Nearly 90 percent of respondents opposed the changes to the American Board of Medical Specialty (ABMS)/American Board of Internal Medicine (ABIM)'s new Maintenance of Certification (MOC) requirements, citing, among multiple concerns, higher than expected costs. Nearly a third of respondents indicated that the changes will affect their future career plans and will likely accelerate career decisions such as early retirement, part-time work, or transition to non-clinical work. Approximately one-quarter of physicians in practice for 15 years or more specified that early retirement was a probable outcome.
If true, the implication of this change to MOC has significant implications for patients everywhere.
This must have prompted the leadership of the ACC to throw their considerable weight into the discussion with the ABIM. In their statement, the ACC promised to:
The good news (if there is any with the ACC's announcement), is that front-line doctors are starting to be heard. While the ACC's actions might be a step in the right direction (one can hope), it is disappointing that their statement still sides with the ABIM's requirements for the unproven MOC process in the first place, the busy-work requirement for "Practice Improvement Modules" (especially when quality measures are already required by hospitals), and for permitting a private organization to monopolize the ability of physicians to practice their trade. Furthermore, the ACC's statement does nothing to insist upon changes to the ABIM's non-transparent and self-serving Conflict of Interest policies that keeps conflicts confidential except to certain chosen individuals within the ABIM.
Unless the ACC can convince the ABMS and ABIM to come clean on these important issues, significant physician resistance to this process will remain. Furthermore, the lack of involvement by other subspecialty boards in resisting the ABMS/ABIM's MOC process is concerning. Hopefully, other subspecialty boards will be encouraged by the ACC's example.
After all, cardiologists aren't the only ones frustrated by this change in MOC policy.
-Wes
If true, the implication of this change to MOC has significant implications for patients everywhere.
This must have prompted the leadership of the ACC to throw their considerable weight into the discussion with the ABIM. In their statement, the ACC promised to:
- Have "ongoing discussions" with ABIM leadership, in partnership with other cardiovascular professional organizations whose members are similarly affected, to review these issues and to explore changes in MOC requirements that will result in more meaningful outcomes and less onerous burdens for ACC members (Editor's note: To date, MOC has never been shown to alter outcomes, so we are left to wonder what this statement really means.)
- Request for ACC representation at ABIM to participate in discussions involving MOC, including its educational and financial aspects (Editor's note: What financial aspects might they mean? Does the ACC want in on this cash cow, too? Or might they want to strike a deal offset some of the fees since they want to keep their educational MOC-preparation income stream coming?
- Review of the evidence base underlying current recommendations (Editor's note: Let me help: there are none. Any positive articles are likely authored by those standing to profit from the endeavor or research paid for by the ABMS. Negative articles are also suppressed from publications sympathetic to the regulatory world. And we should recognize that we have never developed a definition of the "quality" physician. Quality to whom? Is "quality" following rubrics and care pathways? Or might "quality" be something very different, like empathy, listening skills, interpretative skills, or surgical skill? The reality is, if you can't agree on what defines quality, you can't define how to measure it.)
- Investigation of impact of MOC changes on non-ABIM certified members (Editor's note: I strongly agree with this - it is unethical to impose MOC mandates of any kind without first understanding how they negatively affect doctors, especially if a doctor should not pass and is unable to practice their vocation on the basis of a 180-question timed test)
- In the interim, ACC will support its membership by:
- Free provision of web-based MOC modules and navigation tools to ACC members
- Expansion of Part IV MOC modules through ACC programs such as the NCDR’s inpatient registries and the PINNACLE Registry
- Creation of mechanisms for ACC members by which patient safety and patient survey requirements can be efficiently fulfilled
- Bidirectional communication with and engagement of membership through Chapters, Sections and Councils.
The good news (if there is any with the ACC's announcement), is that front-line doctors are starting to be heard. While the ACC's actions might be a step in the right direction (one can hope), it is disappointing that their statement still sides with the ABIM's requirements for the unproven MOC process in the first place, the busy-work requirement for "Practice Improvement Modules" (especially when quality measures are already required by hospitals), and for permitting a private organization to monopolize the ability of physicians to practice their trade. Furthermore, the ACC's statement does nothing to insist upon changes to the ABIM's non-transparent and self-serving Conflict of Interest policies that keeps conflicts confidential except to certain chosen individuals within the ABIM.
Unless the ACC can convince the ABMS and ABIM to come clean on these important issues, significant physician resistance to this process will remain. Furthermore, the lack of involvement by other subspecialty boards in resisting the ABMS/ABIM's MOC process is concerning. Hopefully, other subspecialty boards will be encouraged by the ACC's example.
After all, cardiologists aren't the only ones frustrated by this change in MOC policy.
-Wes
Friday, March 28, 2014
Why Do Most Medical Professional Societies Call Chicago Home?
Why is this?
First, there is the grand-daddy of all physician professional societies: the American Medial Association based at AMA Plaza, 330 N Wacker Drive, Chicago.
Next, there's the American Board of Medial Specialties (ABMS) (who boasts its supervisory role over 24 subsidiary specialty medical societies across the nation, including the American Board of Internal Medicine and the American College of Cardiology among others) that has it's home at 222 North LaSalle Street in Chicago, just blocks away from the AMA building.
Next, there's the little-known Council on Medical Specialty Societies, who also seemed to be concerned with physician "quality" located just across the Chicago river at 35 E. Wacker Drive.
And let's not forget the Acceditation Council on Graduate Medical Education who oversees all graduate medical education in the United States located at 515 North State Street in Chicago.
Makes you wonder why all of these societies are within blocks of each another in Chicago.
Maybe it's so they can have lunch together. Maybe it's because of all of the academic medical centers located here in Chicago who have retiring professors that need a place to land. Maybe it's because of the state's political leanings. Or perhaps it's just because of Chicago's fairly central US geographic location?
One thing's for sure, it certainly isn't because of low real estate prices or low taxes.
-Wes
Saturday, December 07, 2013
When Scientists Accept "Flawed" as "Reassuring"
A recent essay entitled "Understanding the Customer and the New MOC Changes" by David May, MD, PhD, chair of the Board of Governors and secretary of the Board of Trustees for the American Board of Cardiology, was published online and tugs at our heartstrings by describing the Maintenance of Certification (MOC) secure examination in Cardiovascular Diseases as "flawed but reassuring measure of our competence for the real customer here … our patients and their families who trust us with their very lives."
I read this piece after recently completing the MOC process in both cardiology and cardiac electrophysiology for the third time. After devoting hundreds of hours preparing for an impersonal timed computer test yet again, I couldn't help but wonder if physician scientists should ever accept a "flawed" process as acceptable for our ourselves or our patients. Imagine the implications to scientific inquiry and the process of challenging (and thereby improving) the educational process if we did: we might have to accept media reports to justify the process so we can make it even bigger.
Patients deserve transparent quality metrics of care provided by their doctors and the American College of Cardiology (ACC) has been a unique leader in bringing measurable care metrics to the public with the development of their NCDR databases. Yet instead of turning to these real life metrics of care delivery, it seems the leadership of the ACC also feels compelled to sell a "flawed" educational testing construct to its members too. Is this decision based on a self-imposed imperative to dispense social justice at the bedside or more for the direct financial renumeration received by the officers of the College or it's parent, the American Board of Medical Specialities?
I believe there is merit to becoming Board Certified in a subspecialty once. A baseline of knowledge is assessed by this process. But the move to the current model of "maintaining" certification through complicated, costly, and unproven methods of survey completion, administrative and academic busy-work, followed by a timed multiple-choice computerized test overreaches into unproven areas of quality assurance.
To me, a better measure of physician competence and quality would be this: Board Certification once followed by disclosure of the total number of patients treated or the total number of procedures performed pulled from databases akin to the NCDR databases in development. Such a method would align with current documentation requirements for assuring quality patient care and would avoid alienating busy physicians already faced with unprecedented regulatory scrutiny, steep pay cuts and loss of autonomy.
Pretending that the MOC process is a better method to assess competence rather than one's clinical experience in delivering real, live, clinical care feeds unrealistic expectations and may even promote a false sense of security to our patients.
What patients and their doctors deserve (and need) is verifiable data, not propaganda.
What patients and their doctors deserve (and need) is verifiable data, not propaganda.
-Wes
Tuesday, April 23, 2013
The American College of Cardiology Gets a New CEO
Since when does a pharmaceutical executive become CEO of the American College of Cardiology (ACC)?
Since now.
Call me crazy, but does this strike anyone else as strange? Are physicians now officially incapable of leading the ACC or any other major professional doctor organization? Have we not learned anything about the appearance of co-mingling pharmaceutical or medical device company executives with doctors?
Oh, wait...
Maybe this is happening thanks to our grand health care reform efforts underway. Maybe cardiology future battles will not be fought at the bedside, but rather in the boardroom or the halls of Congress. When government calls the shots, lobbying is king, not 60-minute door-to-balloon times.
Need more Regulations? Check. Need some Appropriateness Criteria? Check. Guidelines? Check. Steering committees? Check. Ways to keep industry at scientific sessions? Check. Need an industry thoughtleader to write white papers on physician payment reform? Check.
What was I thinking? After all, pharmaceutical executives have "unique skills" and are accustomed to back-room deal-making, facing regulatory hurdles, basking in paperwork, and getting great benefits for themselves! They know how to schmooze and mollycoddle the political class much better than doctors do, so why not turn to them for advise? I get the plan - it's brilliant! Who needs clinical cardiologists for leadership positions in their professional societies?
Seriously, what could possibly go wrong?
-Wes
Since now.
Call me crazy, but does this strike anyone else as strange? Are physicians now officially incapable of leading the ACC or any other major professional doctor organization? Have we not learned anything about the appearance of co-mingling pharmaceutical or medical device company executives with doctors?
Oh, wait...
Maybe this is happening thanks to our grand health care reform efforts underway. Maybe cardiology future battles will not be fought at the bedside, but rather in the boardroom or the halls of Congress. When government calls the shots, lobbying is king, not 60-minute door-to-balloon times.
Need more Regulations? Check. Need some Appropriateness Criteria? Check. Guidelines? Check. Steering committees? Check. Ways to keep industry at scientific sessions? Check. Need an industry thoughtleader to write white papers on physician payment reform? Check.
What was I thinking? After all, pharmaceutical executives have "unique skills" and are accustomed to back-room deal-making, facing regulatory hurdles, basking in paperwork, and getting great benefits for themselves! They know how to schmooze and mollycoddle the political class much better than doctors do, so why not turn to them for advise? I get the plan - it's brilliant! Who needs clinical cardiologists for leadership positions in their professional societies?
Seriously, what could possibly go wrong?
-Wes
Friday, November 11, 2011
Miss Manners Goes to the ACCF
Dear Ms. Manners:
I am a fellow of the American College of Cardiology and I just learned that the American College of Cardiology Foundation (ACCF), the same foundation that publishes most of our patient care and treatment guidelines, is providing training to medical device and pharmaceutical personnel so our interactions with them become “effective and efficient.”
How nice.
Is this how Multaq (er, dronedarone) got such an early mention in our latest atrial fibrillation treatment guidelines? I've always wondered, especially after we later learned that there might be a few unsavory issues with this drug.
Still, I have no doubt the need is there. Glad to see that my annual membership fees are being put to such good use. After all, up until now, it really HAS been hard interacting with industry reps when they brought lunch. Don’t get me wrong, it wasn’t their professional demeanor or their knowledge of their device or drug. No, that wasn’t it. It was just so hard to explain to them why I had to dine and dash.
Now, thanks to you, I won't have to. I'll just spend more of my limited time getting down with industry personnel so we can share. Imagine: having smart people we can talk to about our latest, coolest case so they can record how much money they spend on our get-togethers. That's efficiency exemplified.
I'm especially impressed that the ACCF training of industry personnel will occur every two years. I was worried about quality of our industry reps' knowledge base, so I'm glad you've made this effort a full-time job. (By the way, I had NO IDEA the ACCF now has a vivarium for all this training - when did you guys spring for that?) Impressive. Rest assured that I'll be SURE to check for your ACCF Training Logo on their business cards before I help myself to a gyro.
But do me a favor, will you? Would you mind passing on some of those fees you receive for that industry training to those of us helping ourselves to lunch? After all, those membership fees we're paying to the ACC are getting a bit stiff. (*wink wink*)
Just kidding.
I'm sure you're really collecting those fees to help lower the cost of my patients' medical devices and drugs in an effort to support their "positive health outcomes." After all, it's this cost thing that's reaking havoc on our health care system, right? (I wish I had thought of such a clever way to address this problem).
Ms. Manners?
Ms. Manners?
Right?
-Wes
h/t: Larry Husten over at Cardiobrief.
I am a fellow of the American College of Cardiology and I just learned that the American College of Cardiology Foundation (ACCF), the same foundation that publishes most of our patient care and treatment guidelines, is providing training to medical device and pharmaceutical personnel so our interactions with them become “effective and efficient.”
How nice.
Is this how Multaq (er, dronedarone) got such an early mention in our latest atrial fibrillation treatment guidelines? I've always wondered, especially after we later learned that there might be a few unsavory issues with this drug.
Still, I have no doubt the need is there. Glad to see that my annual membership fees are being put to such good use. After all, up until now, it really HAS been hard interacting with industry reps when they brought lunch. Don’t get me wrong, it wasn’t their professional demeanor or their knowledge of their device or drug. No, that wasn’t it. It was just so hard to explain to them why I had to dine and dash.
Now, thanks to you, I won't have to. I'll just spend more of my limited time getting down with industry personnel so we can share. Imagine: having smart people we can talk to about our latest, coolest case so they can record how much money they spend on our get-togethers. That's efficiency exemplified.
I'm especially impressed that the ACCF training of industry personnel will occur every two years. I was worried about quality of our industry reps' knowledge base, so I'm glad you've made this effort a full-time job. (By the way, I had NO IDEA the ACCF now has a vivarium for all this training - when did you guys spring for that?) Impressive. Rest assured that I'll be SURE to check for your ACCF Training Logo on their business cards before I help myself to a gyro.
But do me a favor, will you? Would you mind passing on some of those fees you receive for that industry training to those of us helping ourselves to lunch? After all, those membership fees we're paying to the ACC are getting a bit stiff. (*wink wink*)
Just kidding.
I'm sure you're really collecting those fees to help lower the cost of my patients' medical devices and drugs in an effort to support their "positive health outcomes." After all, it's this cost thing that's reaking havoc on our health care system, right? (I wish I had thought of such a clever way to address this problem).
Ms. Manners?
Ms. Manners?
Right?
-Wes
h/t: Larry Husten over at Cardiobrief.
Friday, April 29, 2011
ACC Responds (Again) to Why They Track Their Membership
I appreciate the American College of Cardiology responding to my concerns regarding the finding of RFID tags in our name badges at the recent ACC.11 & i2 Summit Scientific Conferences and expanding upon their earlier explanation. I encourage all readers of this blog to read it.
Now for a bit of a respectful rebuttal.
I admit: I missed the need to "opt-out" of this tracking when I registered for their meeting. But I really didn't realize that registering for a scientific meeting also required signing (checking?) a contract to not permit tracking when I registered at the time. Who knew?
Now more than ever, I believe the use of our personal data should be on the basis of an “opt-in” policy rather than an “opt-out” policy. Requiring someone the check a box to NOT have something is a pernicious way to illicit approval for an activity. I get that we could “opt-out,” but why should I HAVE to? My privacy (and that of all of the ACC’s membership) should be kept confidential first and foremost, marketing efforts should come second.
The ACC states that they use the RFID data for “two main functions,” (1) meeting planning and (2) to collect “rent” for the use of RFID data by exhibitors:
This is not to say the ACC does not need the revenue. Putting on these meetings is expensive. But we must not lose sight of the real purpose of these meetings, education. Many doctors I know shook their head when the opening plenary session started with a light show and red carpet walk. Is funding of these “shows” why they need to see our personal data? Like it or not, we have to wonder.
Also, RFID data are easily hacked. One only needs to watch the short video of Adam Savage from the popular TV show Mythbusters at the 2010 Hackers Conference to see why the Discovery Channel opted not to air their show on RFID technology to understand how important this data is to businesses.
No doubt the ACC need to find ways to raise funds as pressure mounts on all of us to cut costs in health care. These scientific meetings are a major source of revenue for their organization and they do perform an important advocacy role for cardiologists in Washington. But there is a need to remember why they exist in the first place: to advocate for their physician members while respecting their practice of medicine, not sell us (and our personal data) short to other industry interests.
-Wes
Now for a bit of a respectful rebuttal.
I admit: I missed the need to "opt-out" of this tracking when I registered for their meeting. But I really didn't realize that registering for a scientific meeting also required signing (checking?) a contract to not permit tracking when I registered at the time. Who knew?
Now more than ever, I believe the use of our personal data should be on the basis of an “opt-in” policy rather than an “opt-out” policy. Requiring someone the check a box to NOT have something is a pernicious way to illicit approval for an activity. I get that we could “opt-out,” but why should I HAVE to? My privacy (and that of all of the ACC’s membership) should be kept confidential first and foremost, marketing efforts should come second.
The ACC states that they use the RFID data for “two main functions,” (1) meeting planning and (2) to collect “rent” for the use of RFID data by exhibitors:
Exhibitors were able to rent RFID readers from the vendor. They are able to use the data in much the same way as the ACC – to evaluate how effectively their work stations are structured and to improve their offerings to attendees….ACC’s intention was not to create a revenue source by offering attendee data to exhibitors (in fact, only five out of more than 300 exhibiting companies decided to invest in RFID in their booths), but rather to provide exhibitors another resource by which to understand the traffic flow in their booths and to better align their displays with attendees’ needs.They suggest that the ACC’s “intent” was not to create a revenue source by offering attendee data to exhibitors because only 5 vendors opted to pay for the rental. If so, why not offer the data for free? While the data given was reportedly “the same information that was available on meeting attendees badges in print (name/city/state/institution). No contact information is provided” we really see that other data were also derived from this meeting, and hence distributable:
The attendee then goes to a session on appropriate use of PCI, followed by a session on imaging because he or she is interested in new advances in the intersection of imaging and intervention. Let’s also say that several other people in these sessions followed a similar track. In this scenario, the ACC would receive a report of aggregated data, showing a significant level of physician interest in both imaging and interventional sessions.If the ACC collected and controlled the data themselves, then the ACC could assure the data’s privacy, but they did not. The ACC contracted with an outside vendor, Alliance Tech, to collect the tracking data and, as such, they have the ultimate control over it. By supplying our demographic information to Alliance Tech, the ACC makes the tracking data useful to vendors and others. What assurance do members have that Alliance Tech has the same good intentions with the data as the ACC? Realize that this same tactic was used by the American Medical Association to provide our prescribing information to Heath Information Organizations with the same "opt-out" requirement.
This is not to say the ACC does not need the revenue. Putting on these meetings is expensive. But we must not lose sight of the real purpose of these meetings, education. Many doctors I know shook their head when the opening plenary session started with a light show and red carpet walk. Is funding of these “shows” why they need to see our personal data? Like it or not, we have to wonder.
Also, RFID data are easily hacked. One only needs to watch the short video of Adam Savage from the popular TV show Mythbusters at the 2010 Hackers Conference to see why the Discovery Channel opted not to air their show on RFID technology to understand how important this data is to businesses.
No doubt the ACC need to find ways to raise funds as pressure mounts on all of us to cut costs in health care. These scientific meetings are a major source of revenue for their organization and they do perform an important advocacy role for cardiologists in Washington. But there is a need to remember why they exist in the first place: to advocate for their physician members while respecting their practice of medicine, not sell us (and our personal data) short to other industry interests.
-Wes
Sunday, April 24, 2011
The Implications of Physician Tag and Release
Recently, a disturbing trend of monitoring physician quality and accountability has taken another ominous turn: tracking physician's movements at scientific conferences (so called "tag and release") using RFID tags imbedded in attendees name badges at national scientific sessions. Having had personal experience with the recent American College of Cardiology meeting, this technology will also be imbedded in the name badges for attendees at the upcoming Heart Rhythm Society meeting to be held in San Francisco in May.Not everything that counts can be measured.
Not everything that can be measured counts.
-Albert Einstein
On first blush, it shouldn't be such a big deal, right? It was all just a great way for companies to obtain, for a fee, the names and institutions of people who visited their display booths and for the conference organizers to track the movements of attendees. (Heck, maybe they can partner with an industry sponsor to pick up our traffic tolls on the way to the conference hall or arrange other exciting activities for us! [Said tongue-in-cheek, of course])
Instead of "opting in" for tracking at scientific meetings, doctors must "opt out" from the use of tracking technology when registering for scientific meetings. At the upcoming Heart Rhythm Society meeting for instance, doctors had to "opt out" from the use of RFID technology tracking by checking a box that says:
Badge scanning technology will be utilized at this event in order to better understand attendee/delegate interests and preferences. The information collected will be used to improve future events to better address your preferences. No personal information is stored in the RFID badge, only an ID number. We encourage all participants to take part in this process to ensure the most accurate data is obtained. You may check this box to opt-out of the RFID data collection.There's full disclosure, doctor.
But to me, the default tracking of doctors is disturbing on several levels.
First, tracking was approved by our professional society organizers upon their own members. It is no secret that these societies make a significant portion of their operating revenues from industry sponsors at these meetings. By instituting tracking, the value of their membership's privacy has taken a back seat to the income generated from tracking revenues. By NOT checking a box, we have implicitly "agreed" to this tracking. (Realize we MUST wear our badge to attend these conferences where we gain our REQUIRED continuing education credits.) Because we have "agreed" in this manner, the tracking data are now legally "discoverable." At the risk of sounding like a conspiracy theorist, it is not too hard to imagine one's credentials being called into question in court because a doctor did not demonstrate enough time in CME activities at the scientific sessions to quality for credit or because these data implicate a doctor in a purchasing agreement between a vendor and hospital system simply because a doctor visited a display booth.
Doctors have seen this sort of activity before when "only" our license and demographic information was sold by the American Medical Association (AMA). The AMA currently "licenses" physician state medical license numbers and demographic information to health care information organizations (HIOs), HIOs then collect and compile this information with prescribing data that contains the doctors' license numbers (no names, mind you) and then sell the lists to pharmaceutical companies. The AMA tells its members it does "not collect, license, sell or have access to physician prescribing data" and this is true. But the AMA facilitates an intermediary's ability to pair doctors' license information to a their prescribing habits via a third party. One can only speculate how out prescribing and practice profiles are being developed by other similar health information companies with the use of our RFID tracking data.
Behind all of this is a bigger issue: doctors are frustrated by the increasing intrusion into our day-to-day practice of medicine to measure things. Take, as one example, our "quality performance measures" that have done little to facilitate patients office visits, but rather add burdonsome documentation requirements in the interest of government payments. A number of hospital administrators have confided in me that it costs more to collect this data than they make in government payments. In fact, whether these programs are ultimately are found to be cost-effective or improve the quality of care has been brought into question in our literature. Yet we continue to collect these measures and expand them. We are now dispatching legions of people to collect and compile data to "prove" that Electronic Medical Records are used in a "meaningful" way. But an honest appraisal of this policy discloses the reality: these measures permit health care systems to collect another $40,000 per doctor from the government because they are using computers, not because it improves patients' care in any "meaningful" way. As proof of the overburdensome nature of all this data collection for the physician, doctors (or their health care systems) are increasingly employing "scribes" to relieve them of the data-entry burdens in the name of "efficiency." How much, exactly, do these scribes cost our health care system? Few dare to ask the question since no one wants to deny themselves of that juicy $40,000 pot of gold being paid per doctor.
Adding insult to injury, all doctors will soon be required to disclose if we receive anything over $100 from industry representatives. Like the public, most of us recognize the pernicious nature of industry influence upon our profession. Yet we now find we are being used. Should our professional organizations be any less forthright with their industry dealings and the use of our demographic data at national scientific sessions? How much is at stake?
Finally, we see more and more onerous licensure requirements and fees paid to the same tag-and-release operatives at considerable cost to ourselves. We now spend thousands of dollars to remain "credentialed." We wonder how much the RFID "return on investment" to industry sponsors adds to our annual membership fees. Could it reduces them? Who knows? Maybe, like other IT models, we should insist our membership fees be waived if we agree to being RFID tagged and released because most of us realize someone's making money on this deal.
In summary, doctors increasingly find the imperative to guard the privacy of our patients without regard to our own personal and professional privacy with the very same patients disturbing. Everything about doctors is being measured these days and it's taking its toll on patient care. We are frustrated with the governmental bureaucratic standards that threaten our time with patients. But time with patients does not pay bills. Meeting data-collection milestones do. Our government and employers have lost sight of the main issue here: improving and expanding our contact with (and the ability to do good for) our patients.
But as long as there is money to be made with our personal information, it is clear that there will be those that will try to capitalize upon it, whether we realize it or not. Only by demanding constant accountability and transparency from the collectors of this information be they government bureaucrats or our professional society appointees, can we hope to maintain any modicum of professionalism in our tenuous doctor-patient relationships of the future.
-Wes
Wednesday, April 20, 2011
ACC Explains the Use of RFID Tags on Attendee's Name Badges
In response to my earlier post on the use of RFID tags at the ACC's Scientific Sessions, I left a message on the ACC's blog to inquire about this practice. My comment was not initially published, but today I noticed that traffic came from their blog and that my comment and a response to my inquiry was published on the 12th of April. Here's what they said:
My bet: there will be one heck on an "opt in" clause for this technology going forward for future meetings.
At least I hope so.
-Wes
Hi Dr. Fisher,First, this was very nice of them to respond. I am concerned, however, that this company that tracks these RFID tags can identify the individual and their associated institution in real-time at these meetings (see their promotional video). As Calvin Powers from IBM notes on his blog:
Thanks for your question and your feedback on the meeting. RFID is used by many large meetings -- the technology allows us to track which sessions an attendee attends, and also to track flow -- this will help us a lot to plan the education program next year, as we will be able to use data to determine co-location of pathways etc. to make for an ever better attendee experience on show site. Info that the ACC collected at ACC.11/i2 will help us better plan meeting rooms and expo entrances, adjust our conference programming & expo hall floor plan, and quantify to exhibitor prospects the value of investing in our event, among other things. We are not using the RFID to award CME.
Thank you again for your feedback. Please know we will certainly take your concerns into consideration as we plan for 2012.
All the best,
Sue Sears Hamilton
Associate Vice President, Annual Scientific Session
American College of Cardiology
Is it OK for the ACC to give the names, demographic information, contact info, etc of every individual that visited the booth?We do not know if this practice occurred, but we do know that the capability was there.
At this point in the continuum we have moved into the realm of identified tracking and I suspect most people would feel like their privacy had been invaded if their individual movements were tracked and this level of detail was sold to the exhibitors. When the tracking becomes identifiable down to the individual, privacy practices regarding transparency, opt in/out policies, etf become very important.
My bet: there will be one heck on an "opt in" clause for this technology going forward for future meetings.
At least I hope so.
-Wes
Wednesday, April 06, 2011
What They Know
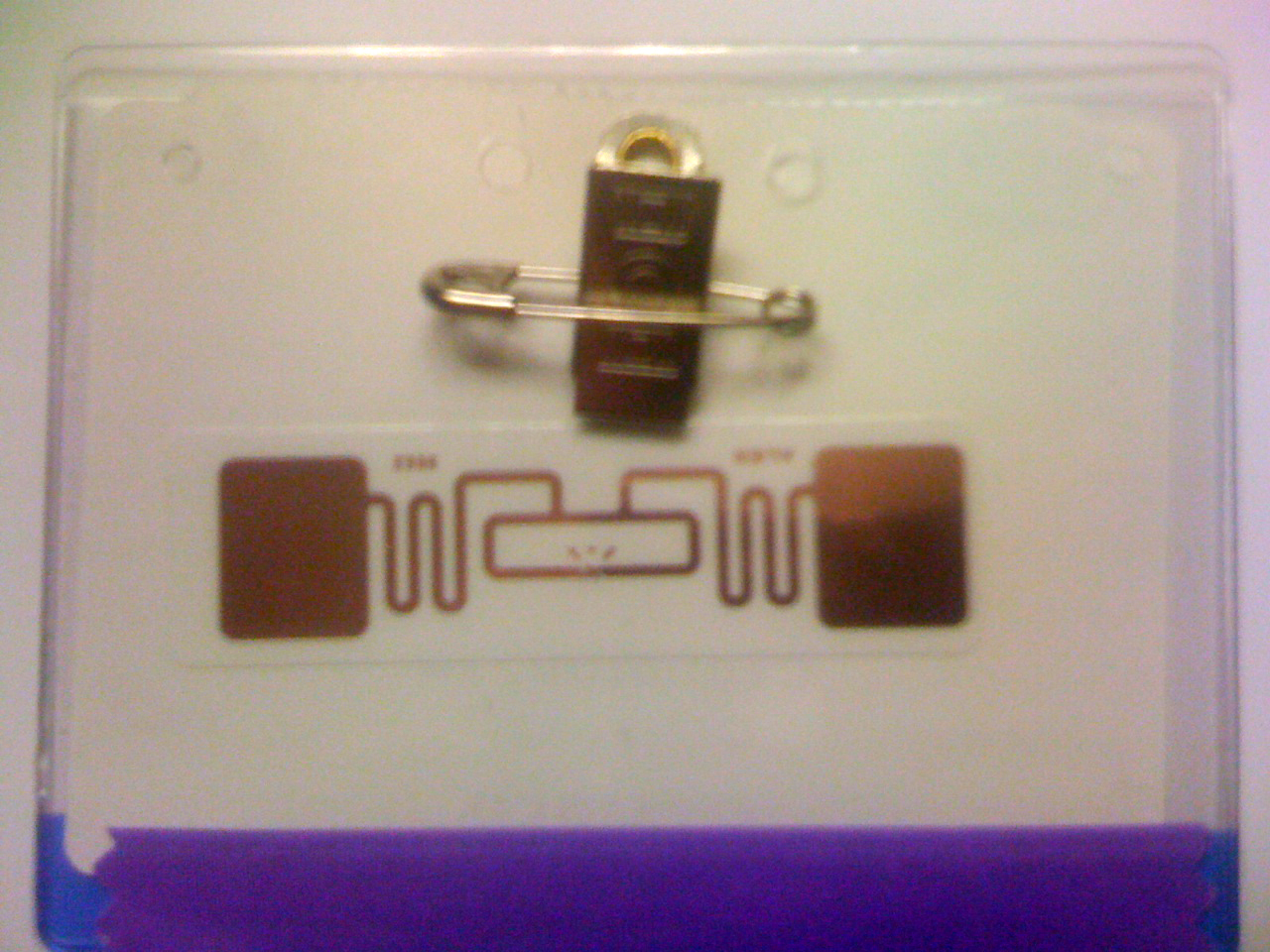
Here's a picture of the back of my badge at the recent American College of Cardiology Conference held 2-5 April 2011 in New Orleans, LA:
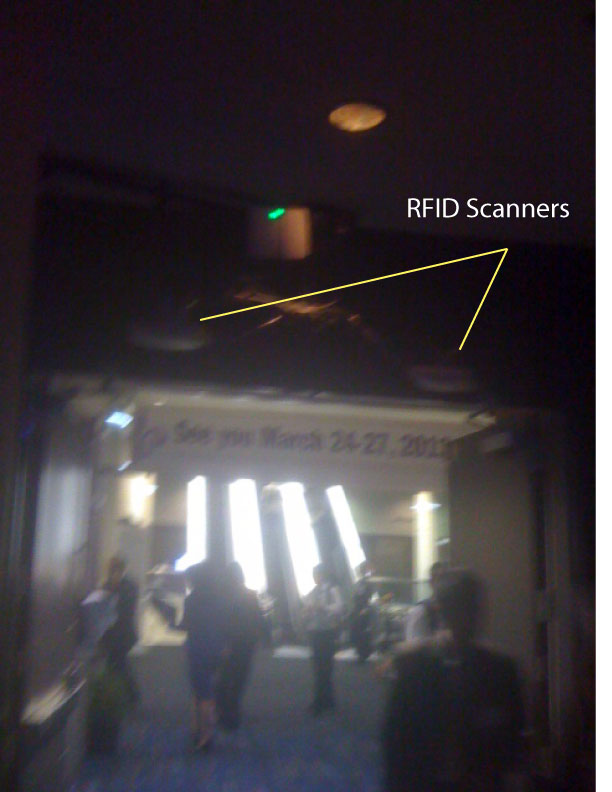
 And here's the scanners used to track those RFID tags above one of the conference rooms:
And here's the scanners used to track those RFID tags above one of the conference rooms:

I wonder what they know about me and if I'll still get credit for the sessions that I walked out early on?
-Wes
Addendum 8 Apr 2011: here's an excellent take on these issues from Calvin Powers from IBM's blog.
I wonder what they know about me and if I'll still get credit for the sessions that I walked out early on?
-Wes
Addendum 8 Apr 2011: here's an excellent take on these issues from Calvin Powers from IBM's blog.
Saturday, April 02, 2011
Off to the Land of Make Believe
Tomorrow I head off to Land of Make-Believe: The 2011 American College of Cardiology Scientific Sessions in New Orleans, Louisiana.
I say this not out of spite for the organizers who have toiled to streamline the registration process and prepare the display hall, nor because I have anything against the presenters who have spent hours perfecting their talks and preparing their slides, nor because I won't learn anything there, nor because I don't have faith in the incredible will and wonder of the people of New Orleans. Seriously, it's a huge, fun, informative conference in a warm, welcoming, and conference-friendly city.
Rather, I say this because I fear these meetings will have less and less influence on how health care delivery will occur going forward as limits to how and how much care is delivered - at least as far as technology and innovation are to be used in the years ahead.
The sands are shifting beneath our feet. Every doctor I speak to knows it - some with more foreboding an outlook than others - but no one dares to show it lest they not appear to be a "team player." Instead, most of us act on the outside as though we are stalwart stewards of the status quo marching ahead to our future Land of Make Believe.
As such, we’re elated at the prospect that percutaneous aortic valve replacement will be available to all of our patients over eighty years of age with multiple severe co-morbidities soon (at least those are the only patients studied so far) and that all us who are fantastic interventionalists will soon be able to perform the procedure for all of our patients to meet the overwhelming demand. After all, the data at this meeting will show how safe the procedure is for them, right? Surely CMS would never drag it's feet toward approval of this expensive technology, would they?
Make Believe.
We watch the Stent Wars between companies and clinical investigators like a good Ultimate Fighter match: each company sparing for the right to claim a hair-thin victory over their competitor. And those bio-absorbing stents? Rock on! Surely the winner hear will take the sales prize, right? Especially since doctors have such influence over purchase orders these days. Everyone will be watching when a p value gets low enough and the legions of Press Corps spring to action as willing sycophants to the marketing hype so critical to promotion and adoption by the cardiovascular community at these meetings. As if it will soon really matter.
Make Believe.
We urge our medical students, residents, and fellows to attend these meetings and offer cash rewards to our best and brightest Young Investigators as if to suggest that most of them can still become entrepreneurs in the medical device arena in the years ahead. After all, regulatory approval hurdles for new technology aren't prohibitive, right? And those fees to the FDA, they're not too high, are they? Profits surely will be showered upon our young employee-inventors, too, right?
Make Believe.
And then there will be the transparency about how much all this stuff displayed costs, like the hybrid cath-lab/operating rooms (being developed now to install all those percutaneous valves in our elderly patients). Better to ignore this in favor of the bright, the shiny, and the new. Never mind that doctors and hospitals will soon be paid in lump sum payments from Medicare. Never mind that those payment amounts will be about 20% of where they are now. The sky's the limit for these purchase orders, right? Hospitals will get their return on investment quickly and doctors will still get their fare share of those bundled payments. Finally, look for these issues to be discussed front and center every single day at these Scientific Sessions.
Make Believe.
But I still can’t stay away. It will be a welcome respite from the cold to enjoy some nice warm weather. There’ll be nice people from all over the country and all over the world there. I enjoy speaking at these events, too: you realize the depth and breadth of commitment of today's doctors despite the forces that are changing. There’s a unique camaraderie that's developing, I feel, despite all of these changes. No matter what happens ahead, so far we are still afforded the luxury of meeting face-to-face to share our stories of patient care – both good and bad. And once in a while those stories can sometimes be shared nice glass of self-bought wine.
Better yet: it’ll be my excuse to leave those insidious Electronic Medical Record communications, office and patient e-mails, and results-reviewing behind for a few days.
Oops, I forgot.
Make Believe.
-Wes
P.S.: Anyone who wants to share some stories and a good glass of wine between e-mails at the ACC 2011 Meeting can reach me via Twitter at @doctorwes. If you're still not on Twitter, here's how and why you should consider signing up.
I say this not out of spite for the organizers who have toiled to streamline the registration process and prepare the display hall, nor because I have anything against the presenters who have spent hours perfecting their talks and preparing their slides, nor because I won't learn anything there, nor because I don't have faith in the incredible will and wonder of the people of New Orleans. Seriously, it's a huge, fun, informative conference in a warm, welcoming, and conference-friendly city.
Rather, I say this because I fear these meetings will have less and less influence on how health care delivery will occur going forward as limits to how and how much care is delivered - at least as far as technology and innovation are to be used in the years ahead.
The sands are shifting beneath our feet. Every doctor I speak to knows it - some with more foreboding an outlook than others - but no one dares to show it lest they not appear to be a "team player." Instead, most of us act on the outside as though we are stalwart stewards of the status quo marching ahead to our future Land of Make Believe.
As such, we’re elated at the prospect that percutaneous aortic valve replacement will be available to all of our patients over eighty years of age with multiple severe co-morbidities soon (at least those are the only patients studied so far) and that all us who are fantastic interventionalists will soon be able to perform the procedure for all of our patients to meet the overwhelming demand. After all, the data at this meeting will show how safe the procedure is for them, right? Surely CMS would never drag it's feet toward approval of this expensive technology, would they?
Make Believe.
We watch the Stent Wars between companies and clinical investigators like a good Ultimate Fighter match: each company sparing for the right to claim a hair-thin victory over their competitor. And those bio-absorbing stents? Rock on! Surely the winner hear will take the sales prize, right? Especially since doctors have such influence over purchase orders these days. Everyone will be watching when a p value gets low enough and the legions of Press Corps spring to action as willing sycophants to the marketing hype so critical to promotion and adoption by the cardiovascular community at these meetings. As if it will soon really matter.
Make Believe.
We urge our medical students, residents, and fellows to attend these meetings and offer cash rewards to our best and brightest Young Investigators as if to suggest that most of them can still become entrepreneurs in the medical device arena in the years ahead. After all, regulatory approval hurdles for new technology aren't prohibitive, right? And those fees to the FDA, they're not too high, are they? Profits surely will be showered upon our young employee-inventors, too, right?
Make Believe.
And then there will be the transparency about how much all this stuff displayed costs, like the hybrid cath-lab/operating rooms (being developed now to install all those percutaneous valves in our elderly patients). Better to ignore this in favor of the bright, the shiny, and the new. Never mind that doctors and hospitals will soon be paid in lump sum payments from Medicare. Never mind that those payment amounts will be about 20% of where they are now. The sky's the limit for these purchase orders, right? Hospitals will get their return on investment quickly and doctors will still get their fare share of those bundled payments. Finally, look for these issues to be discussed front and center every single day at these Scientific Sessions.
Make Believe.
But I still can’t stay away. It will be a welcome respite from the cold to enjoy some nice warm weather. There’ll be nice people from all over the country and all over the world there. I enjoy speaking at these events, too: you realize the depth and breadth of commitment of today's doctors despite the forces that are changing. There’s a unique camaraderie that's developing, I feel, despite all of these changes. No matter what happens ahead, so far we are still afforded the luxury of meeting face-to-face to share our stories of patient care – both good and bad. And once in a while those stories can sometimes be shared nice glass of self-bought wine.
Better yet: it’ll be my excuse to leave those insidious Electronic Medical Record communications, office and patient e-mails, and results-reviewing behind for a few days.
Oops, I forgot.
Make Believe.
-Wes
P.S.: Anyone who wants to share some stories and a good glass of wine between e-mails at the ACC 2011 Meeting can reach me via Twitter at @doctorwes. If you're still not on Twitter, here's how and why you should consider signing up.
Monday, August 16, 2010
On the ACC's Growing Pains With Social Media
As discussed by Emily Zeigenfuse of the American College of Cardiology (ACC):
Of course, the greatest challenge will be getting doctors to realize the benefits of social media compared to the liabilities when interacting with patients this way. Still, the value of providing rapid, reputable content to patients while improving their understanding of complicated treatments should serve to improve the caliber of health information available to our patients and might just improve outcomes.
-Wes
We went live on June 14, 2010, and we’ve had a few challenges. The website wasn’t 100% perfect, and our readers let us know immediately. The comments box, where we expected readers to discuss medical content, was used instead for help-desk issues, which inhibited the discussion of cardiology topics.Kudos for the ACC for getting involved with social media. Their efforts will help pave way for others interested in using the medium creatively to address issues important to doctors and their patients.
Since then, we’ve added a separate button to report tech problems, collaborated directly with members who left complaints, and took a second look at usability. It’s been a sleepless summer, but we’ve solved a lot of problems quickly by honestly listening to and engaging our readership.
Lastly, what other trends do you see in health care social media? What’s next?
I’m very curious about how mobile devices will fit into a doctor’s daily workflow. We know our members, by virtue of being on their feet all day, spend less time in front of a computer than those of us with desk jobs. We’re also watching how patients with chronic diseases like heart disease use social media to talk about their condition so that we can reach them in those spaces.
Of course, the greatest challenge will be getting doctors to realize the benefits of social media compared to the liabilities when interacting with patients this way. Still, the value of providing rapid, reputable content to patients while improving their understanding of complicated treatments should serve to improve the caliber of health information available to our patients and might just improve outcomes.
-Wes
Tuesday, July 06, 2010
How Do Cardiologists Want to Get Paid?
According to the American College of Cardiology, here's what you get when you ask nearly 400 of 'em:
Of course the whole damn physician payment mess is complicated by a billing coding scheme that is so ridiculous, arbitrary, and insane that no matter which method you pick, it can be gamed to everyone's benefit except the patient. Get rid of THAT system and we might be able to talk about REAL physician payment reform.
How?
Pay ALL doctors, be they specialists or not, a fair, market-based hourly wage for work performed. That's ALL work: from the most mundane e-mail response or medication refill to the most time-consuming history-taking or complex neurosurgical procedure. Pay them time-and-a-quarter or time-and-a-half for after hours duty.
Since most of our legislature are lawyers, even they should understand this concept, right?
Imagine: no diagnosis codes, no procedure codes, no coding specialists, no 500,000 permutations and combinations of procedure codes that must match pre-determined and frequently varying diagnosis codes. If hospitals and government want to screw with that system - go for it - but keep the physician workforce separate from these coding shenanigans. Pay us what our time and intellectual capabilities are worth. Period.
And what might these hourly wages be?
That would have to be worked out based on training, years of practice, malpractice risk, board-certification, etc. But compared to the mess we have now, I'm betting this system would be a whole hell-of-a-lot more understandable and transparent than the monkey business we're doing now.
-Wes
Nearly two-thirds (63%) of cardiologists in private practices are currently compensated on a fee-for-service basis (FFS) exclusively; and, similarly, nearly two-thirds (65%) of these private practice cardiologists indicate that their ideal compensation is fee-for-service. Some of this response seems to be related to fear that doctors are due to be shafted regardless of what form of reimbursement is used. Therefore stick with the devil you know -- even if it is constantly declining.In my view, fee-for-service is effectively (and appropriately) on life-support and fading fast. Oh sure, "concierge" fees can make up a difference between medicare payments and drops in fees for a while in affluent areas, but these fees do nothing to address the very real needs for doctors in less affluent or rural health care delivery areas. On first blush, the market is moving to a health care system salary-based structure, but straight salaries do little to promote team collaboration nor reward exceptional personal effort. If productivity incentives are added to straight salary structures, there is a risk of promoting of even more testing to benefit the hospital (and hence employee-doctor's) bottom line at the expense of the patient or their insurer.
Conversely, more than three-fourths (78%) of the cardiologists who are not in private practice currently receive a salary as their primary source of income. However, interesting to note is that only 57% of these cardiologists state that a salary is their ideal form of compensation. Fee-for-service (19%) and a mixed compensation system (22%) actually gain strength among them for ideal compensation. This makes sense. Salaried cardiologists deserve incentives for productivity (everybody doesn’t work as hard) and quality (everybody doesn’t strive as effectively for better outcomes). Incentives have to be based on relevant data comparisons—not conjecture.
Of course the whole damn physician payment mess is complicated by a billing coding scheme that is so ridiculous, arbitrary, and insane that no matter which method you pick, it can be gamed to everyone's benefit except the patient. Get rid of THAT system and we might be able to talk about REAL physician payment reform.
How?
Pay ALL doctors, be they specialists or not, a fair, market-based hourly wage for work performed. That's ALL work: from the most mundane e-mail response or medication refill to the most time-consuming history-taking or complex neurosurgical procedure. Pay them time-and-a-quarter or time-and-a-half for after hours duty.
Since most of our legislature are lawyers, even they should understand this concept, right?
Imagine: no diagnosis codes, no procedure codes, no coding specialists, no 500,000 permutations and combinations of procedure codes that must match pre-determined and frequently varying diagnosis codes. If hospitals and government want to screw with that system - go for it - but keep the physician workforce separate from these coding shenanigans. Pay us what our time and intellectual capabilities are worth. Period.
And what might these hourly wages be?
That would have to be worked out based on training, years of practice, malpractice risk, board-certification, etc. But compared to the mess we have now, I'm betting this system would be a whole hell-of-a-lot more understandable and transparent than the monkey business we're doing now.
-Wes
Wednesday, March 17, 2010
Could This Be the ACC Meeting of the Future?

Click image to enlarge
I couldn't help but notice the "Heart Hub" at the American College of Cardiology Meeting this year, pictured above. There were doctors nicely nuzzled up to a bar in a relaxed atmosphere where a bartender served cranberry juice, soft drinks and perhaps a small snack, as doctors watched and interacted with any of four talks occurring simultaneously at the meeting. Some were interesting case discussions with a question and answer format where you could text message your answer to a multiple-choice question on your cell phone and, like American Idol, the results would be instantly displayed on the screen for the audience to view before the correct answer was given.
Which made one wonder, with all the concern about industry influence that was aired publicly at the meeting with gargantuan corporate displays that stretched 25-30 feet in the air for over a quarter of a mile in the display hall as a backdrop, might his be a better way to provide education for tomorrow's doctors?
But there was only one problem:
This is very expensive to produce. Who the heck would pay for it?
-Wes
Monday, March 15, 2010
Back By Popular Demand: Sex, the Heart, and ED
Today, I proved what I suspected: if you want readership, write or Tweet about sex and the heart.
Needless to say, in a little over 30 minutes, I garnered 30 new Twitter followers by live-tweeting what I learned in the "Sex, the Heart, and Erectile Dysfunction (ED)" session at the American College of Cardiology meeting in Atlanta. For those who might have missed it, I have organized the tweets in chronicalogical order for yourenjoyment benefit:
I must admit, that was, by far, the most fun I've ever had attending a scientific session.
-Wes
Needless to say, in a little over 30 minutes, I garnered 30 new Twitter followers by live-tweeting what I learned in the "Sex, the Heart, and Erectile Dysfunction (ED)" session at the American College of Cardiology meeting in Atlanta. For those who might have missed it, I have organized the tweets in chronicalogical order for your
Okay, at Sex/Heart session: Standing room only. Docs, pharma here. Um, will doctors attending please stand up?So there you have it.#acc10
NEWS! Most people with CAD have ED! Up next: Cardiac response to sexual activity... #acc10
10 healthy married couples studied: all kinds of positions and O2 consumption measured. #acc10 orgasm rocks the heart rate up 72%!
Guys on top: MUCH more exertion for men. Who knew? #acc10 Large variability of HR & VO2 - younger men a bit more, um, vigorous.
Man on top: 3.3 Mets, partner on top 2.5 Mets. Uh oh: Topic now not PG-13 rated... #acc10
Extramarital sex: HR 96->150; later same day w/wife: HR 62->92. REAL data. Conclsn: extramarital sex more risky #acc10< In more ways than 1
2 flights of stairs w/o stopping equals one romp in the hay in terms of workout #acc10
Oops, seems 6 Mets of exertion on treadmill tolerated means sex is safe. #acc10 Rock on, folks!
RT @gruntdoc: twitter rank skyrocketing. NEWS! Most people with CAD have ED! Up next: Cardiac response to sexual activity...< heh #acc10
OMG! Lots of therapeutic options if meds don't work: topical, intrcavernosal or intrarethral options; implants too. #acc10 Can I go now?
Remember nitrate warning...wait 48 hrs after stopping nitrate b4 using Viagra or Cialis or Levitra. #acc10 Now if u have CP, don't call me.
RELAX trial: randomized trial (evaluating use of ED drugs) looking at "stiff hearts" (diastolic dysfn) underway. #acc10 Wait, I thought stiff was good.... [kidding]
Revatio 20tid & Adcirca 20 qd used for pulmonary HTN to decrease pulmonary pressures. #acc10 Looks like juicy sex stuff has to wait.
Email inbox full after twittering sex/heart info. #acc10 (well, not quite, but 13 new followers in under 30 min) < Proof that sex sells!
Zzzz. Discussing sildanefil (Viagra) in mice. #acc10 Mice have enough sex, can we move on?
Great! A woman is about to speak! #acc10 Endocrine aspects of sex - awww, talking about male hypogonadism. Sorry ladies...
Yikes! 2000 men with low testosterone had higher mortality in Europe. #acc10 Arnold (Swartzenegger) is safe.
Peak testosterone level in men is age 28! #acc10 I'm dyin'.... [scratch that] I'm dead.
Can we use ED to prevent heart disease? #acc10 ED is assoc w/ incr CV death. ID of pts offers opportunity to steal cases from urologists!
ED is, after all, a VASCULAR disease. #acc10 I've heart of a throbbing heart but... er, never mind. (Urologists beware).
Asking about ED is as good as drawing CRP level in men! #acc10 hey, great way to save $$$$!
We were introduced to a new concept: A cardiac sexologist! #acc10 I'm in!
Q: what about women? A: Women getting Viagra. Women w/pulmonary HTN report greater sexual activity #acc10 honey, you're script's waiting 4u!
I must admit, that was, by far, the most fun I've ever had attending a scientific session.
-Wes
Subscribe to:
Comments (Atom)