Oh, the wonders of Apple's iOS8! Now there's no excuse for slow room turnovers:
Yeah, I can see all kinds of applications for time lapse photography, especially when it comes to improving my productivity...
-Wes
Tuesday, September 23, 2014
Friday, September 19, 2014
Case Study: What They Don't Teach You in EP Fellowship
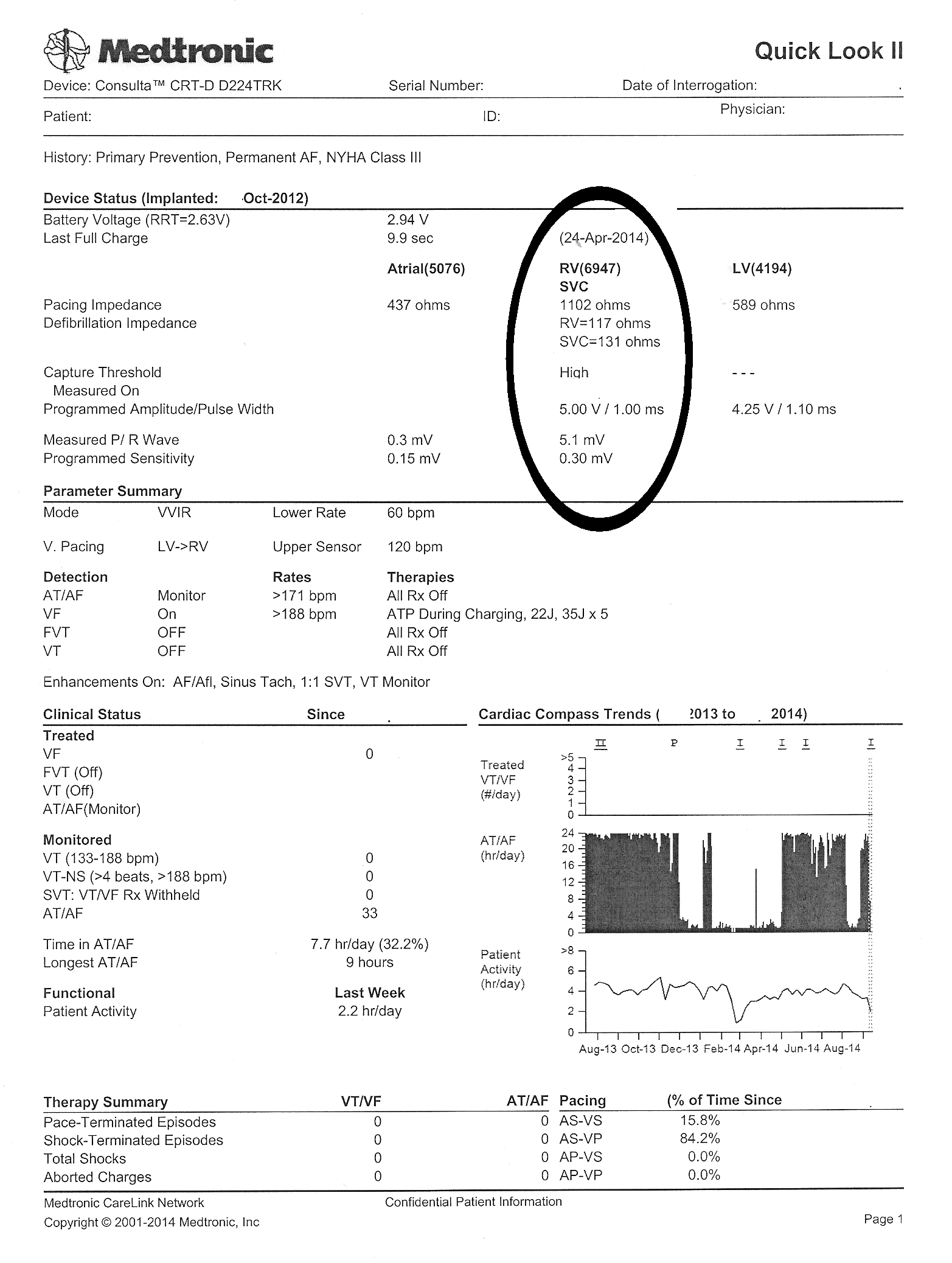
These days, pacemakers and defibrillators are often interrogated via a home-monitoring system that uploads information contained in the implanted cardiac devices automatically to a central server so it can be accessed by physicians remotely. This feature was added to most defibrillators after the rash of recalls struck the industry in 2005-6. Not only can the information be uploaded electively by the patient, it can also be automatically uploaded if a nightly self-check detects a parameter out of range. In this case, the patient was being monitored by Medtronic's Carelink remote monitoring system.
"Dr. Fisher, I think we have a problem with Mr. Smith's RV lead (not his real name)," my device nurse said as she handed me the Carelink transmission that triggered an superior vena cava (SVC) high voltage coil impedance warning:
 |
| Click to enlarge |
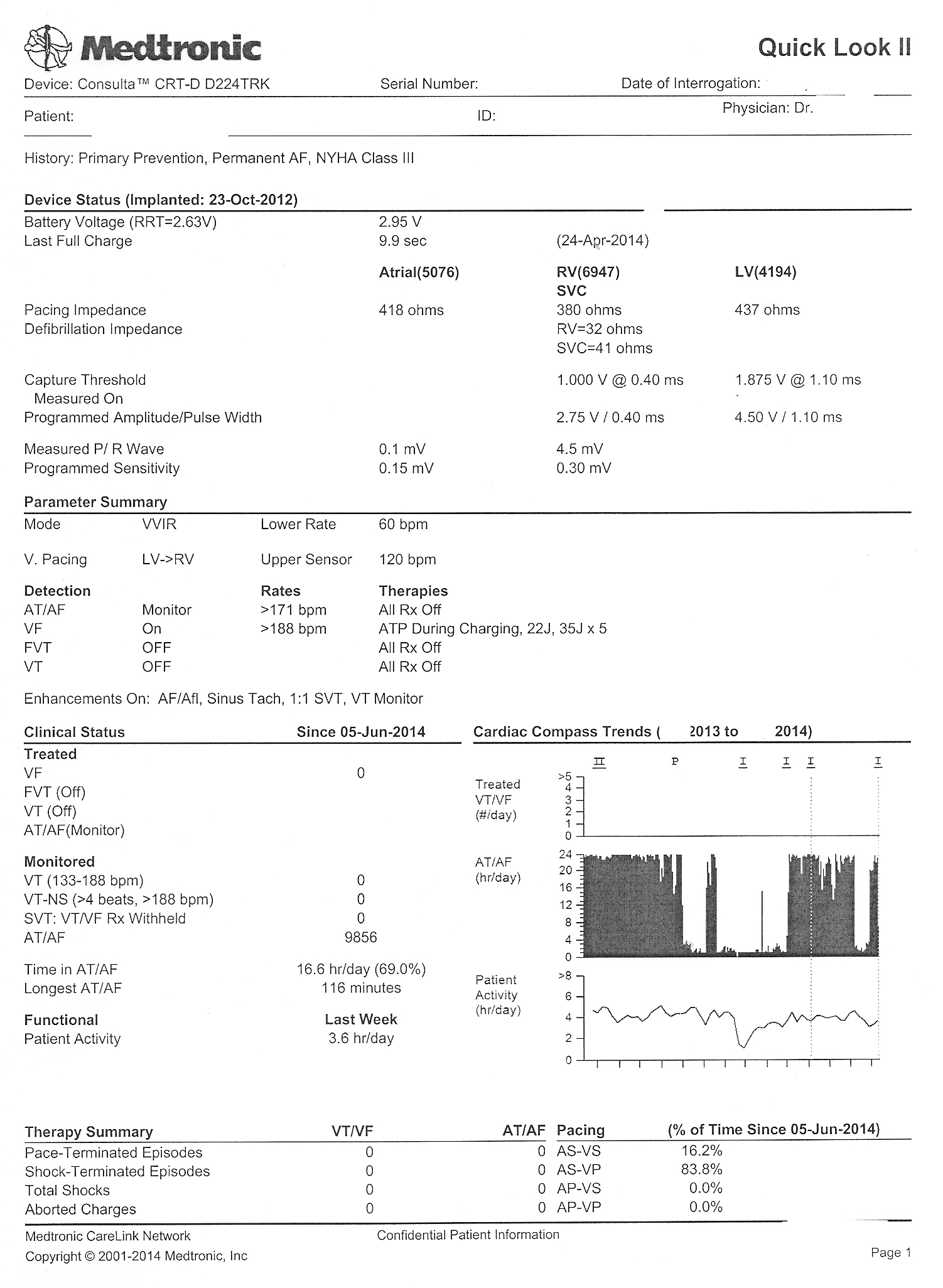
"What did the last interrogation look like?" I asked.
"Here's the old one was sent just three days before and looked fine," she said. "It's so weird. We've not had a problem with this patient's device since it was implanted in 2012."
 |
| Click to enlarge |
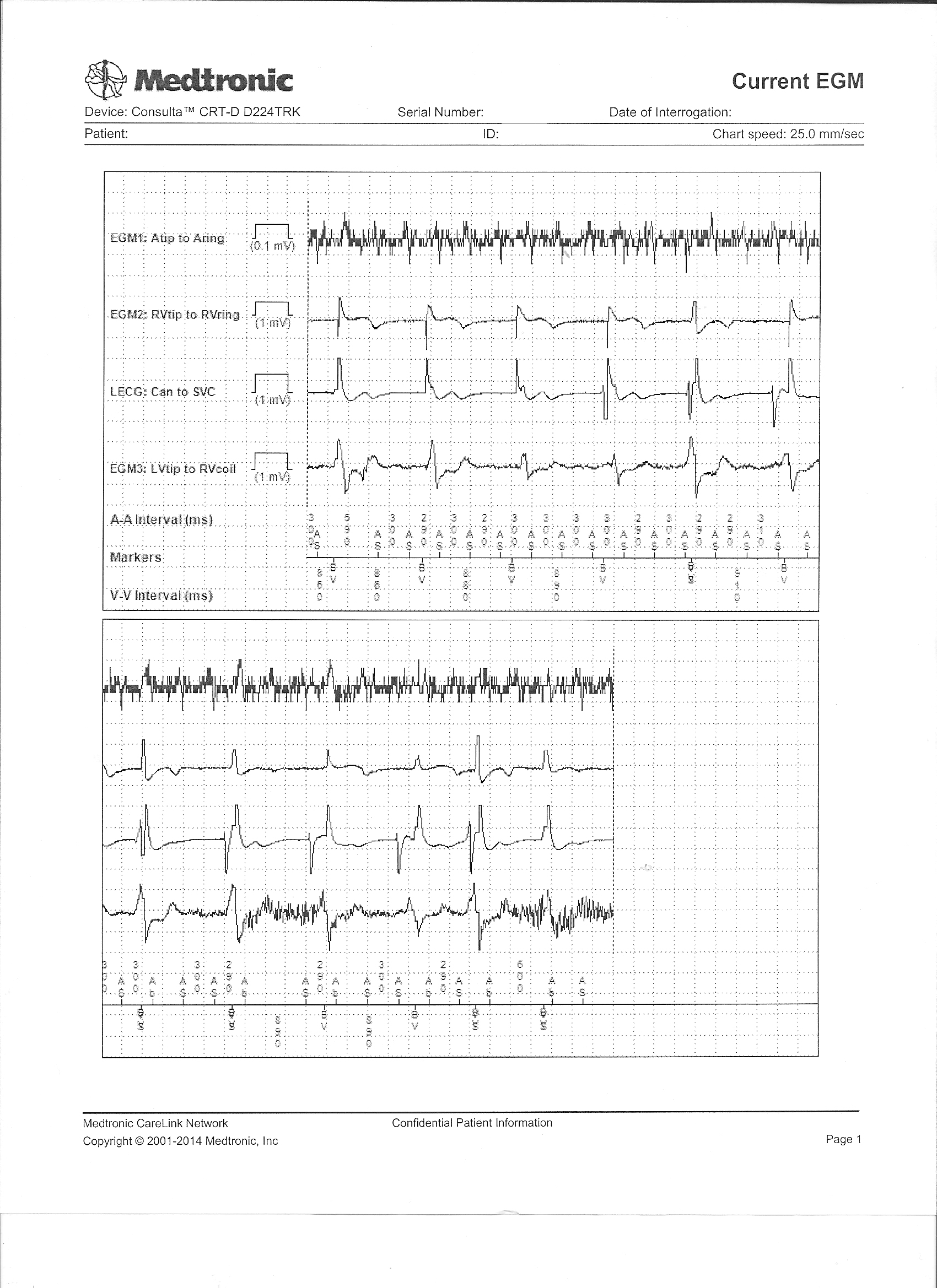 |
| Real-time intracardiac electrograms seen on the earlier transmission - Click to enlarge |
"Strange. I'm not sure what to make of this. Give him a call - we might have to change that RV lead," I said.
"Okay," she said, then returned to the device clinic and I went back to seeing patients.
Some time later, my nurse returned.
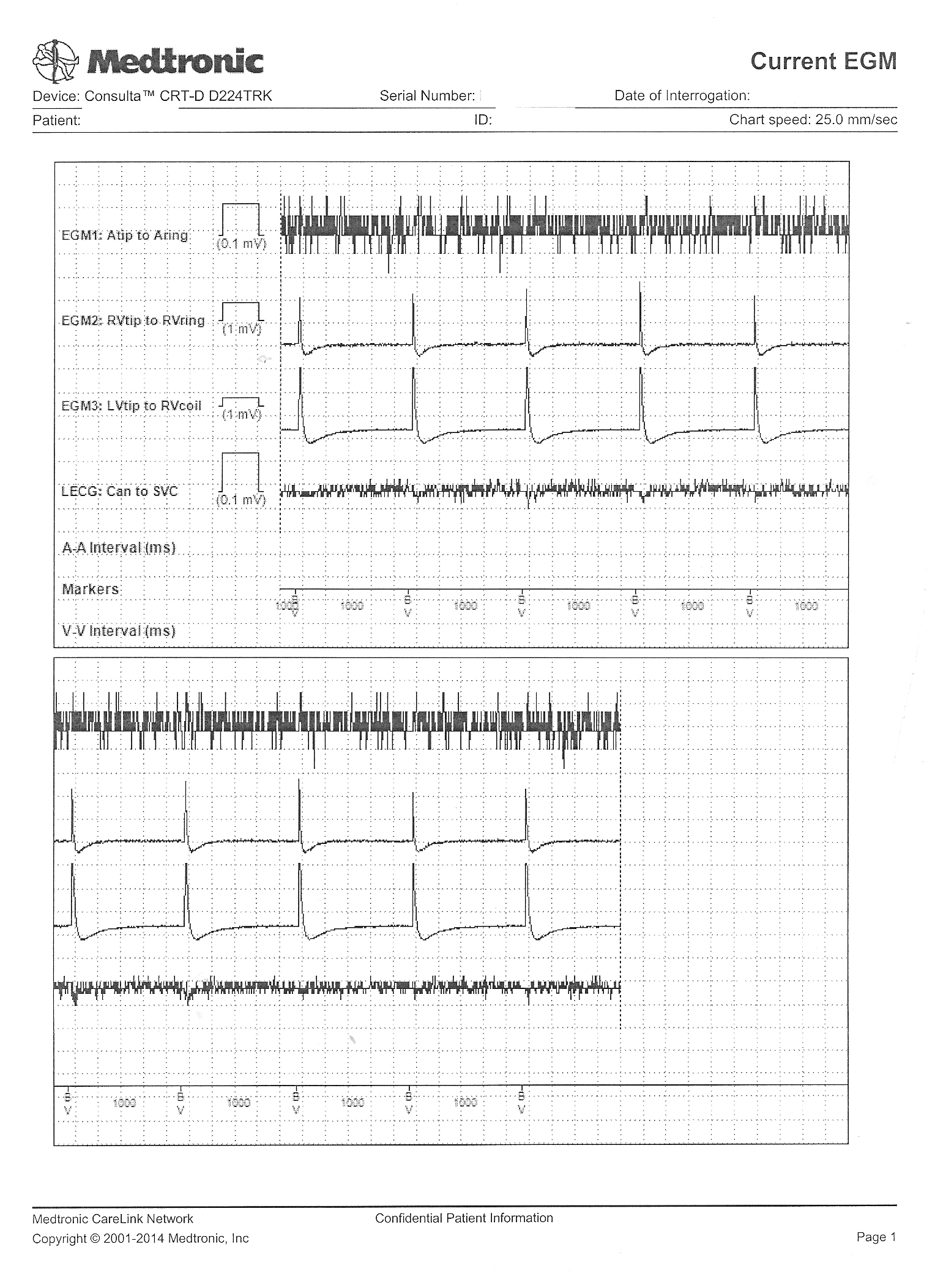
"Um, Dr. Fisher, could I speak with you a moment?" she asked. "I got some more information. I think you better look at this" and she handed me his most recently transmitted real-time intracardiac electrogram recording that was sent with the latest transmission.
{kind=link}
What did it show and why were the RV lead parameters abnormal?
-Wes
Wednesday, September 17, 2014
Rebuttal: A Bit More on MOC Failure Rates
Recently, David H. Johnson, MD, Chair of the American Board of Internal Medicine (ABIM) Board of Directors and Internal Medicine Chairman at UT Southwestern Medical Center in Dallas, and Rebecca Lipner, PhD, Senior Vice President of Evaluation, Research, and Development at the ABIM published a "guest blog post" over at MedPageToday regarding Maintenance of Certification (MOC) pass rates, entitled "Debunking the MOC Pass Rate Myths." I do not know if they were directing their comments directly to me, but since I was the one who brought the issue of rising MOC failure rates to the public's attention some time ago using the ABIM's own published data of first-time MOC takers, I thought I should respond.
I appreciate Drs. Johnson and Lipner providing more insight into how the MOC examinations are constructed and scored. The ABIM's arbitrarily-defined "65%" marker based on "expert consensus" and undisclosed "psychometrics" is an interesting one, and at least now we understand how this benchmark was arbitrarily created. They also acknowledge that "significant changes in the practice of the discipline may require that the passing standard be reset." Unfortunately, they do not disclose what those changes might be, which way their 'standard' might be adjusted, or what internal or external force might mandate such an "reset."
Drs. Johnson and Lipner also confirmed the rising failure rates of board examinations over the past five years. Oddly, they then seem to imply that this "decline in pass rates" is due to a misunderstanding by "some social media observers" of their testing and scoring process:
Drs. Johnson and Lipner also remind us that "pass rates are higher among first-time test takers." While there are likely many reasons for this, we must conclude that significant AGE BIAS against older, more experienced physicians exists. Since this proprietary MOC process was cleverly made a "quality measure" imbedded in our new health care law, the logic of this biased process contradicts common sense. Are patients not our best teachers? Are we to assume that physician experience after years of direct patient care is of less value than ABIM-selected facts and principles culled from an exponentially-growing body of medical literature regurgitated on a computer screen in an expensive testing center? Furthermore, how the test is constructed or scored is of little relevance to more procedural based specialties of internal medicine like mine because these skills are never assessed.
Drs. Johnson and Lipner also mention (without supporting data) that physicians who take their examination three times (at their expense) ultimately achieve a 95% pass rate. As if this is the point. Instead, we should ask what patients and physicians lose each time they must repeat this onerous, time-consuming and unproven process. Can the personal, financial and professional losses of repeated testing ever be regained? How, exactly, does repeated testing of a flawed process help our patients? What marginal utility to our health care system does this whole test-taking exercise really provide? Does this MOC process actually separate the good physician from the bad physician or the good test-taker from the bad one? Since ABIM never knows a doctor's scope of practice before their assessment, they make some heady assumptions about what they should test. In reality, the ABIM only tests what THEY think should be tested, rather than what matters to the particular physician's patient population. Worse still, since the ABIM remains completely unaccountable to doctors or patients in regard to their MOC process, their assessment may have absolutely no relevance to a particular physician's practice. Shouldn't we be discussing these issues before arguing how the test is constructed and scored?
No physician I know argues with the need for continuing, life-long education in medicine, especially when its performed in a relevant, transparent, informative, collegial and feedback-oriented process without a ulterior financial motive. If fact, most of us do this every week as part of our state licensure requirements and have plenty of continuing medical education credits to prove it. Allowing the ABIM to monopolize this process as we have through artificial MOC point acquisition exercises that are often irrelevant to a physician's scope of practice not only circumvents more healthy and sustainable learning environment, but also might cause more harm than good if that physician loses their practice privileges as a result.
In summary, I believe the ABIM's lucrative MOC process is no more valid than what doctors have already been doing for years before the American Board of Medical Specialties decided to make their MOC program an annual exercise. The MOC process remains unproven in its ability to improve patient care and (as we've now confirmed) discriminates against more senior physicians. Those of us who have endured this process multiple times have witnessed the growth of "board certification" from a self-imposed professional milestone to a money-making scheme filled with clinically-irrelevant busywork that often detracts, rather than augments, patient care (especially those non-validated "practice improvement modules").
It is time that doctors of all ages insist that these self-appointed non-profits organizations cease their attempt to become expensive continuing education providers and stick to what they do best: assessing a doctor's ability to reach a level of exceptionalism of their practice during their career, rather than pretending that they can assure some arbitrary level of ongoing practice adequacy for the business community. Until the ABIM comes to grips with their increasingly bipolar agenda, their ability to remain credible and relevant to practicing physicians, the public, and the mysterious "stake holders" they claim to serve will continue to be challenged, both on social media and in the court of law, as "significant consequences from losing certification" occur with increasing frequency to experienced and fully-capable physicians.
-Wes
I appreciate Drs. Johnson and Lipner providing more insight into how the MOC examinations are constructed and scored. The ABIM's arbitrarily-defined "65%" marker based on "expert consensus" and undisclosed "psychometrics" is an interesting one, and at least now we understand how this benchmark was arbitrarily created. They also acknowledge that "significant changes in the practice of the discipline may require that the passing standard be reset." Unfortunately, they do not disclose what those changes might be, which way their 'standard' might be adjusted, or what internal or external force might mandate such an "reset."
Drs. Johnson and Lipner also confirmed the rising failure rates of board examinations over the past five years. Oddly, they then seem to imply that this "decline in pass rates" is due to a misunderstanding by "some social media observers" of their testing and scoring process:
"Recently, based on a slow decline in pass rates over the past 5 years for the American Board of Internal Medicine Maintenance of Certification exam, some social media observers have made erroneous assertions about how the exams are constructed and scored.Rather than attack what was said or what wasn't by those unruly social media types, I will merely say this: my assessment of the rising failure just focused on simple math. Because there are higher numbers of doctors taking this examination year after year due to the American Board of Medical Specialties' recently-imposed MOC requirement, the stable "65%" pass rate means there is necessarily an INCREASE in the number of total physicians who are FAILING the examination. It goes without saying that a requirement for repeated testing or adding more people to the testing pool handsomely profits the ABIM and similar subspecialty organizations that provide proprietary subspecialty MOC-preparation courses taught by ABIM test question contributors (this relationship is also conflicted, by the way). But the downside of more testing is multi-pronged: it also redirects physicians away from direct patient care to formal classrooms, expensive hotel meeting rooms in cities often outside the physician's hometown, and ultimately to expensive corporate test taking centers. The ABIM never considers these high costs nor the negative effects absence from one's practice has on patients or a physician's limited family time.
Without a full understanding of the exam process, they have nevertheless claimed that the exam is being made more difficult, that the standard for passing the exam changes every time an exam is given, or that the exam is 'graded on a curve.' These assertions are all incorrect."
Drs. Johnson and Lipner also remind us that "pass rates are higher among first-time test takers." While there are likely many reasons for this, we must conclude that significant AGE BIAS against older, more experienced physicians exists. Since this proprietary MOC process was cleverly made a "quality measure" imbedded in our new health care law, the logic of this biased process contradicts common sense. Are patients not our best teachers? Are we to assume that physician experience after years of direct patient care is of less value than ABIM-selected facts and principles culled from an exponentially-growing body of medical literature regurgitated on a computer screen in an expensive testing center? Furthermore, how the test is constructed or scored is of little relevance to more procedural based specialties of internal medicine like mine because these skills are never assessed.
Drs. Johnson and Lipner also mention (without supporting data) that physicians who take their examination three times (at their expense) ultimately achieve a 95% pass rate. As if this is the point. Instead, we should ask what patients and physicians lose each time they must repeat this onerous, time-consuming and unproven process. Can the personal, financial and professional losses of repeated testing ever be regained? How, exactly, does repeated testing of a flawed process help our patients? What marginal utility to our health care system does this whole test-taking exercise really provide? Does this MOC process actually separate the good physician from the bad physician or the good test-taker from the bad one? Since ABIM never knows a doctor's scope of practice before their assessment, they make some heady assumptions about what they should test. In reality, the ABIM only tests what THEY think should be tested, rather than what matters to the particular physician's patient population. Worse still, since the ABIM remains completely unaccountable to doctors or patients in regard to their MOC process, their assessment may have absolutely no relevance to a particular physician's practice. Shouldn't we be discussing these issues before arguing how the test is constructed and scored?
No physician I know argues with the need for continuing, life-long education in medicine, especially when its performed in a relevant, transparent, informative, collegial and feedback-oriented process without a ulterior financial motive. If fact, most of us do this every week as part of our state licensure requirements and have plenty of continuing medical education credits to prove it. Allowing the ABIM to monopolize this process as we have through artificial MOC point acquisition exercises that are often irrelevant to a physician's scope of practice not only circumvents more healthy and sustainable learning environment, but also might cause more harm than good if that physician loses their practice privileges as a result.
In summary, I believe the ABIM's lucrative MOC process is no more valid than what doctors have already been doing for years before the American Board of Medical Specialties decided to make their MOC program an annual exercise. The MOC process remains unproven in its ability to improve patient care and (as we've now confirmed) discriminates against more senior physicians. Those of us who have endured this process multiple times have witnessed the growth of "board certification" from a self-imposed professional milestone to a money-making scheme filled with clinically-irrelevant busywork that often detracts, rather than augments, patient care (especially those non-validated "practice improvement modules").
It is time that doctors of all ages insist that these self-appointed non-profits organizations cease their attempt to become expensive continuing education providers and stick to what they do best: assessing a doctor's ability to reach a level of exceptionalism of their practice during their career, rather than pretending that they can assure some arbitrary level of ongoing practice adequacy for the business community. Until the ABIM comes to grips with their increasingly bipolar agenda, their ability to remain credible and relevant to practicing physicians, the public, and the mysterious "stake holders" they claim to serve will continue to be challenged, both on social media and in the court of law, as "significant consequences from losing certification" occur with increasing frequency to experienced and fully-capable physicians.
-Wes
Thursday, September 11, 2014
The Big Flail
After you've written on a blog for a long time, you begin to ask yourself why. Oh sure, there are the great opportunities for a single person to make a point, to act as a tiny tugboat trying to push a corporate mothership in a slightly different direction, but you begin to realize that there are very few times that actually happens. You try to provide a voice to issues that are often unheard, then realize that voice is only occasionally appreciated but more often duly noted, then ignored. This is the nature of internet and quite frankly, medicine now - it is a world of competing interests. On one side you have the patients, doing a messy job of getting sick, and corporate health care systems - either government, private, for-profit or non-profit - doing their very best to make sure their illness is neat and tidy, easy to control, perfectly understood, and quantifiable. To this end, each has their own agendas that must be served, be it another regulation, value-added improvement, or a profit motive to secure the bottom line.
This idea came to me yesterday in clinic. Increasingly, every microsecond of my day, my week, my weekend has now been efficiently parsed into tiny computerized scheduling chunks. It doesn't matter where I work, because like The Cloud, location doesn't matter - schedulers and administrative handlers can reach me, be it by beeper, computer, Outlook email, EPIC email, desk phone or my personal iPhone. There are so many places to check for messages that when I don't respond, the person trying to reach me just moves up the chain of communication options. Eventually there's no down time, no time to think, there are few places to go where there is quiet any longer. It's become life by a thousand interruptions - a Big Flail.
Increasingly, there's a push to do away with beepers and move telecommunications in medicine to my personal iPhone. But I an resisting this because I need to set a boundary between work and my personal life - if for nothing else but self preservation. We are told this is being done in the name of "security" and "non-secure beeper messages" but I think it's because people don't want to wait. They need their answer now. I really wonder what the evidenced based data on beeper message hacking is in health care and if more patients were helped or hurt by beeper data breeches. There's a better idea, they say: consolidate. It's more "efficient." I know, I'm such a Luddite. But to whom do I respond when that head administrator calls on my iPhone as I'm examining a patient? How to I separate a Twitter message from an ER message? Does the act of looking at my phone when I'm with a patient engender trust or an appearance of distraction?
It's hard to argue with "security" when someone creates a new medical policy. We all want to be secure. We all want to know that our most private and personal medical information is protected from prying eyes. But quite frankly (and this is very politically incorrect to say) real information security in medicine is a joke. After all, people's lives are perfectly encoded on a computer now and eight different billers, coders, insurance company trolls or hospital marketers can delve into that database of information and find specifics about a patient or group of patients with simply the click of a button. Phishing schemes make a mockery of our passwords. Seriously, who are we fooling? Let's be honest: paper charts housed in a known location behind a locked door were MUCH more secure.
Hurry up. Click here, click there, "Excuse me," "Can I have a moment of your time?", "There's a the 7 am meeting tomorrow," "What was that Ms. Jones?", "Yes, I'll try to make it," "Did you try it unipolar?", "Yes, I'll check my inbasket,""You left your addendum open,""They're calling for the cardioversion,""Should we add him in?", "I have to take my board review course, can you take call?,"The ER's calling,""Can you check her pacer, too, when you see her?", "Did you sign the EKG?"
Doctors need some quiet, down time, some time to think, to pay attention. We need to create our own boundaries between our personal and professional lives that are respected. We need to think we can get away, to regroup, have some quiet time for ourselves or with a patient, even for a moment. And if that means that some of us want to separate work from home by the use of a beeper instead of an iPhone, so be it.
Otherwise, our personal lives will become a Big Flail, too.
-Wes
This idea came to me yesterday in clinic. Increasingly, every microsecond of my day, my week, my weekend has now been efficiently parsed into tiny computerized scheduling chunks. It doesn't matter where I work, because like The Cloud, location doesn't matter - schedulers and administrative handlers can reach me, be it by beeper, computer, Outlook email, EPIC email, desk phone or my personal iPhone. There are so many places to check for messages that when I don't respond, the person trying to reach me just moves up the chain of communication options. Eventually there's no down time, no time to think, there are few places to go where there is quiet any longer. It's become life by a thousand interruptions - a Big Flail.
Increasingly, there's a push to do away with beepers and move telecommunications in medicine to my personal iPhone. But I an resisting this because I need to set a boundary between work and my personal life - if for nothing else but self preservation. We are told this is being done in the name of "security" and "non-secure beeper messages" but I think it's because people don't want to wait. They need their answer now. I really wonder what the evidenced based data on beeper message hacking is in health care and if more patients were helped or hurt by beeper data breeches. There's a better idea, they say: consolidate. It's more "efficient." I know, I'm such a Luddite. But to whom do I respond when that head administrator calls on my iPhone as I'm examining a patient? How to I separate a Twitter message from an ER message? Does the act of looking at my phone when I'm with a patient engender trust or an appearance of distraction?
It's hard to argue with "security" when someone creates a new medical policy. We all want to be secure. We all want to know that our most private and personal medical information is protected from prying eyes. But quite frankly (and this is very politically incorrect to say) real information security in medicine is a joke. After all, people's lives are perfectly encoded on a computer now and eight different billers, coders, insurance company trolls or hospital marketers can delve into that database of information and find specifics about a patient or group of patients with simply the click of a button. Phishing schemes make a mockery of our passwords. Seriously, who are we fooling? Let's be honest: paper charts housed in a known location behind a locked door were MUCH more secure.
Hurry up. Click here, click there, "Excuse me," "Can I have a moment of your time?", "There's a the 7 am meeting tomorrow," "What was that Ms. Jones?", "Yes, I'll try to make it," "Did you try it unipolar?", "Yes, I'll check my inbasket,""You left your addendum open,""They're calling for the cardioversion,""Should we add him in?", "I have to take my board review course, can you take call?,"The ER's calling,""Can you check her pacer, too, when you see her?", "Did you sign the EKG?"
Doctors need some quiet, down time, some time to think, to pay attention. We need to create our own boundaries between our personal and professional lives that are respected. We need to think we can get away, to regroup, have some quiet time for ourselves or with a patient, even for a moment. And if that means that some of us want to separate work from home by the use of a beeper instead of an iPhone, so be it.
Otherwise, our personal lives will become a Big Flail, too.
-Wes
Monday, September 08, 2014
Another MacGyver Moment in Pacemaker Implantation
Installing a permanent pacemaker or defibrillator has become commonplace event in cardiology these days. These devices implanted in a patient are comprised of two main parts: the lead(s) and the pulse generator. After installing the leads in the heart and connecting them to the pulse generator, the lead and pulse generator assembly are then placed beneath the skin in a small subcutaneous (or in rarer cases, submuscular) "pocket" that is created surgically. Considerable care is taken to cauterize bleeding vessels when the pocket is created. To facilitate visualization of these occasional bleeding vessels deep within the created pocket, I prefer to use a surgical headlamp to direct the light deep within the pocket cavity rather than relying on a conventional overhead surgical light. I have found that headlamps have helped me limit my incidence of post-operative pocket hematoma development.
So as things have had it, I seem to have a knack for attracting every eighty- or ninety-plus year old who needs an emergency pacemaker on the weekend when I'm on call, and this past weekend was no exception.
So the team was assembled and the pacemaker implantation equipment readied. They knew I liked a headlamp, so they dug deep into the recesses of their inventory to pull out their only headlamp that appeared to be from a bygone surgical era. Being pressed for time, I couldn't argue and had to make due, but knew that this headlamp might not be very reliable, especially as I saw how the headlamp's fiberoptic cord was secured to the light source that generated about as much light as a few well-lit candles by a cumbersome spring-loaded Rube Goldberg contraption. As I placed the headlamp on my head, and tightened the plastic strap that housed the headlamp to my head, I needed a backup plan in case the light failed.
Would I have to use the overhead light and make do, or might there be another way?
I needed another MacGyver Moment.
That's when my on-call staff team came up with a brilliant, simplified idea:
-Wes
(PS: This device is experimental and has not been approved by the FDA. Use this device at your own risk. If you experience headaches, nausea, difficulty with concentration, or an erection lasting for longer than four hours, discontinue use of this device and contact your doctor immediately. I have no commercial interest in this device. Also, since the headlamp still worked this weekend, no workaround was needed for the patient, but something tells me we might be getting a new headlamp soon.)
So as things have had it, I seem to have a knack for attracting every eighty- or ninety-plus year old who needs an emergency pacemaker on the weekend when I'm on call, and this past weekend was no exception.
So the team was assembled and the pacemaker implantation equipment readied. They knew I liked a headlamp, so they dug deep into the recesses of their inventory to pull out their only headlamp that appeared to be from a bygone surgical era. Being pressed for time, I couldn't argue and had to make due, but knew that this headlamp might not be very reliable, especially as I saw how the headlamp's fiberoptic cord was secured to the light source that generated about as much light as a few well-lit candles by a cumbersome spring-loaded Rube Goldberg contraption. As I placed the headlamp on my head, and tightened the plastic strap that housed the headlamp to my head, I needed a backup plan in case the light failed.
Would I have to use the overhead light and make do, or might there be another way?
I needed another MacGyver Moment.
That's when my on-call staff team came up with a brilliant, simplified idea:
 |
| iPhone to the rescue! |
-Wes
(PS: This device is experimental and has not been approved by the FDA. Use this device at your own risk. If you experience headaches, nausea, difficulty with concentration, or an erection lasting for longer than four hours, discontinue use of this device and contact your doctor immediately. I have no commercial interest in this device. Also, since the headlamp still worked this weekend, no workaround was needed for the patient, but something tells me we might be getting a new headlamp soon.)
Friday, September 05, 2014
Cybernetic Medicine

Every day, the exponential explosion of data entry and regulatory requirements doctors endure boggles the mind, all in the name of "health care."
Feedback is critical to field of cybernetics. And when Medicare's straps have you by the balls, you comply.
No longer is it good enough to learn a diagnosis or procedure code, doctors must attend online courses to learn how to use a new "calculator" to determine a more proper code. After all, there will soon be over 70,000 of them. Each more specific than the other, each more ridiculous. There are five data-entry fields to click on that calculator, each another tiny, yet time-consuming decision to be made, just to determine a code. No doubt teams of clever twenty-something computer programmers are overjoyed with their coding calculator and the way it pops up automatically on our screen when needed, then disappears. So pretty. So cool. See how easy they've made it to complete that regulatory requirement?
And this does not begin to address the increasingly algorithmically-driven electronic medical record and procedures envisioned in the years ahead. As if all things can and must be perfectly defined and quantified in medicine. No mistakes. No judgment needed. No need to type. Just close your eyes, click a few buttons, and follow the pathway. Stop thinking. Just do it. Enter the data. Resistance is futile.
After all, it's about the money...
... and perfect physician cyborgs.
Feel that strap tightening?
-Wes
Friday, August 22, 2014
Where To Teach?
As I begin another year teaching EKG's to our new residents, I find I am increasingly asking myself "Where to teach?"
I do not mean to imply a geographic sense to the word "where" (although this is difficult, too, as residents move from hospital to hospital in large health care systems like ours as they change rotations), but rather as more of a "level." What level do I teach our residents the art of EKG reading? Do I keep it rudimentary or do I teach it at the level of a good cardiology fellow? Are we striving for excellence or striving for adequacy in EKG interpretation? Said another way: do I teach at a Dubin's level of EKG interpretation or a Marriott's?
This is not an easy decision for those engaged in teaching medical students and residents.
Every year I am evaluated by the residents for my instruction, and every year I get good marks. But an e-mail received from our program director made me concerned, because a criticism they had heard from the residents was that my instruction was too advanced. (This was a first for me despite using similar core lecture materials year to year).
Which led me to wonder, is my curriculum too advanced for our newer residents or are medical students not receiving instruction on EKGs in medical schools before residency? Or has is the art of EKG interpretation evolving to simply reading the computer-generated interpretation at the top of the tracing? Should residents just be taught basic ACLS-level tracings or the more subtle findings of hypothermia and hypercalcemia?
I wonder why there's such a difference now, why there is a draw to spoon-feed our residents rather than to teach them basic principles upon which to grow their understanding. Perhaps residents are flooded. Perhaps they are scared. Or (more likely) perhaps we need to do a better job leading by example. Perhaps, as one fellow of mine said, our attendings in medical schools are so hurried to get back to clinic that they never do chalk-talks or EKG reading with residents any more. Maybe the pressures to make medicine more efficient is robbing from education.
Whatever it is, there is a change.
I'm sure I'm not the only teacher who's encountered the same difficulty knowing where to teach now. But I continue to believe that our youngest doctors can rise to any challenge they are given as long as they have enough time, so don't expect it to be any easier from now on, but maybe just a bit slower.
My time, after all, is unlimited. (* cough *)
-Wes
I do not mean to imply a geographic sense to the word "where" (although this is difficult, too, as residents move from hospital to hospital in large health care systems like ours as they change rotations), but rather as more of a "level." What level do I teach our residents the art of EKG reading? Do I keep it rudimentary or do I teach it at the level of a good cardiology fellow? Are we striving for excellence or striving for adequacy in EKG interpretation? Said another way: do I teach at a Dubin's level of EKG interpretation or a Marriott's?
This is not an easy decision for those engaged in teaching medical students and residents.
Every year I am evaluated by the residents for my instruction, and every year I get good marks. But an e-mail received from our program director made me concerned, because a criticism they had heard from the residents was that my instruction was too advanced. (This was a first for me despite using similar core lecture materials year to year).
Which led me to wonder, is my curriculum too advanced for our newer residents or are medical students not receiving instruction on EKGs in medical schools before residency? Or has is the art of EKG interpretation evolving to simply reading the computer-generated interpretation at the top of the tracing? Should residents just be taught basic ACLS-level tracings or the more subtle findings of hypothermia and hypercalcemia?
I wonder why there's such a difference now, why there is a draw to spoon-feed our residents rather than to teach them basic principles upon which to grow their understanding. Perhaps residents are flooded. Perhaps they are scared. Or (more likely) perhaps we need to do a better job leading by example. Perhaps, as one fellow of mine said, our attendings in medical schools are so hurried to get back to clinic that they never do chalk-talks or EKG reading with residents any more. Maybe the pressures to make medicine more efficient is robbing from education.
Whatever it is, there is a change.
I'm sure I'm not the only teacher who's encountered the same difficulty knowing where to teach now. But I continue to believe that our youngest doctors can rise to any challenge they are given as long as they have enough time, so don't expect it to be any easier from now on, but maybe just a bit slower.
My time, after all, is unlimited. (* cough *)
-Wes
Friday, August 15, 2014
To the ABIM: What Real Life-long Learning Should Look Like
He left a little early to stop by the cath lab to see his patient before her procedure. Cordial "Hello's" and "Good mornings" and "Any last questions?" were mentioned before she signed her consent. The team was working feverishly to prepare her for her procedure. "Have you met the anesthesiologist yet?" was next, and almost on cue, the anesthesiologist arrived and took over for a bit.
He hurried upstairs to the conference room. There, was an all-too-fattening array of welcoming donuts and bagels, a coffee and hot water dispenser, and a few remaining empty cups. This was the stuff of breakfast on more hurried days. Still, a small cup of coffee was welcomed and poured quickly. Another nurse had arrived with him and he asked, "Can I pour you one?" She accepted and they quickly made their way into the conference room after signing the attendance sheet. They didn't want to miss the start of the conference for that was sometimes the best part of the conference.
In a stroke of genius, the organizers of the Cath Conference quickly review the news of the week, both locally, nationally, and medical. They even show wild things colleagues did the week before outside of conference, like flyboarding or a shot of a colleague holding a huge striped bass they caught the weekend before with their 8 year-old daughter. Complaints about the design of the restrospective trial reviewing digoxin's use for atrial fibrillation, sodium's uncertain consumption recommendations this week were met with rolled eyes, and the possibility of transcaval retrograde transaortic valve replacement in patients with no other access was discussed, with a quick aside of direct translumbar aortic punctures and even direct left atrial punctures being performed by surgeons in earlier times. In short, they shared the other side of themselves together, the reality of science, their humanness.
Then they shared cases.
The cases are not always pretty. Some were tough cases, wonderful cases, cases no one had seen before. They discuss the complicated social situations that bring even more complicated dynamics to the case. They discuss the errors and the complications. Importantly, they all understand this is a legally protected conference - a morbidity and mortality conference, if you will - a place where there are frank discussions about the right way to treat things and the wrong way, but a place that is supportive to those who have struggled, and incredibly helpful to those who still struggle with many challenges. Administration hears about the problems doctors had with the lab equipment or staff or whatever - professionally.
And it's the most popular conference in our hospital. People of all ages and technical backgrounds are welcomed. Old and young, cath lab staff, nurses, quality personnel, research staff, administrators, guest speakers, cardiologists and surgeons. Everyone, that is, except industry or pharmaceutical folks. This is, after all, the work of health care, not marketing.
At the end, they greeted, however briefly. A quick question is asked. A consult requested. A research form signed. Then off they went on their ways for another week to do their jobs.
This is lifelong learning as it should be: cordial, professional, collaborative, fulfilling, timely, up to date, and self-generated. And it happens because it has to, not because it's directed by a centralized bureaucratic money-making organization who claims they know what's best for doctors and what's best for society.
When doctors, nurses, technologists and health care teams learn this way it's sustainable for a lifetime for one simple reason:
... because it's enjoyed.
-Wes
He hurried upstairs to the conference room. There, was an all-too-fattening array of welcoming donuts and bagels, a coffee and hot water dispenser, and a few remaining empty cups. This was the stuff of breakfast on more hurried days. Still, a small cup of coffee was welcomed and poured quickly. Another nurse had arrived with him and he asked, "Can I pour you one?" She accepted and they quickly made their way into the conference room after signing the attendance sheet. They didn't want to miss the start of the conference for that was sometimes the best part of the conference.
In a stroke of genius, the organizers of the Cath Conference quickly review the news of the week, both locally, nationally, and medical. They even show wild things colleagues did the week before outside of conference, like flyboarding or a shot of a colleague holding a huge striped bass they caught the weekend before with their 8 year-old daughter. Complaints about the design of the restrospective trial reviewing digoxin's use for atrial fibrillation, sodium's uncertain consumption recommendations this week were met with rolled eyes, and the possibility of transcaval retrograde transaortic valve replacement in patients with no other access was discussed, with a quick aside of direct translumbar aortic punctures and even direct left atrial punctures being performed by surgeons in earlier times. In short, they shared the other side of themselves together, the reality of science, their humanness.
Then they shared cases.
The cases are not always pretty. Some were tough cases, wonderful cases, cases no one had seen before. They discuss the complicated social situations that bring even more complicated dynamics to the case. They discuss the errors and the complications. Importantly, they all understand this is a legally protected conference - a morbidity and mortality conference, if you will - a place where there are frank discussions about the right way to treat things and the wrong way, but a place that is supportive to those who have struggled, and incredibly helpful to those who still struggle with many challenges. Administration hears about the problems doctors had with the lab equipment or staff or whatever - professionally.
And it's the most popular conference in our hospital. People of all ages and technical backgrounds are welcomed. Old and young, cath lab staff, nurses, quality personnel, research staff, administrators, guest speakers, cardiologists and surgeons. Everyone, that is, except industry or pharmaceutical folks. This is, after all, the work of health care, not marketing.
At the end, they greeted, however briefly. A quick question is asked. A consult requested. A research form signed. Then off they went on their ways for another week to do their jobs.
This is lifelong learning as it should be: cordial, professional, collaborative, fulfilling, timely, up to date, and self-generated. And it happens because it has to, not because it's directed by a centralized bureaucratic money-making organization who claims they know what's best for doctors and what's best for society.
When doctors, nurses, technologists and health care teams learn this way it's sustainable for a lifetime for one simple reason:
... because it's enjoyed.
-Wes
Tuesday, August 12, 2014
Data Plan Health Care Shows Promise
CHICAGO - Citing mounting health care costs, electronic note bloat, and concerns with the quality and quality of Big Data, IBM, Apple, and EPIC Systems recently announced a new initiative to totally revamp US health care by offering health care services by data plan. The health care initiative was recently discovered in a little known section of the Patient Protection and Affordable Care Act (ACA) that changed portions of the U.S. Tax Code.
Under the new system, the brainchild of prominent Chicago physician-turned-health care entrepreneur Henry Throckmorton, MD, patients will purchase an initial 250 megabytes of data space on the EMR for all their health needs for $250 per month. “It’s cheaper than most current cell phone service," Throckmorton explained. "When patients exceed their data allotment, health care ceases until patients purchase an additional data storage plan." Expansion data plans come in Bronze (250 M Bytes), Silver (500 Mbytes), Gold (5 G Byte), and Platinum (10 GB) storage increments.
Rollover plans for family members are also offered for those nearing the end of life.
“Health care systems that promise to limit the use of macros, dot phrases and cut-and-paste tactices have a real competetive advantage over competitors insensitive to the patient's data needs!” Throckmorton explained. "This system finally puts health care incentives in the right place.”
But Roger Wilco, spokesperson for America’s Health Insurance Plans (AHIP), the national trade association representing the health insurance industry, seemed less enthusiastic. "This is preposterous! Who do these flowery internet types think they are? Don't they realize there are advantages to more middle men in health care? How are we supposed to get our cut of the money?"
Dr. I.P. Knightly of Urocare Health System in Beaverton, New York, seemed less concerned about the middlemen and appreciated the improvements he's seen in patient care: “Because I document everything on the EMR, including phone calls, results and work schedules, patient are less likely to call so I get a good night’s sleep!”
Nursing and medical students seem torn, however. While some see benefits to shorter notes, some like Tim Allen, MD, a hard-working fourth-year medical student from Roanoke, VA, sees other challenges “I’m still trying to understand ortho notes that no longer contain the critical information fields like the patient’s full name, VIP status, research status, and a complete review of systems. How's a guy supposed to understand what ‘Silt @ t/s/s/sp/dp’ means?”
Market analyst Rebecca Solomon of Lock, Stock and Barrel Equity Partners noted "Apple, IBM and EPIC are quickly gaining market share from more conventional insurance policies. The concept has also resonated with the Department of Health and Human Services because of the cost savings seen from fewer data-hungry imaging studies being ordered."
Mobile partnerships with AT&T, Verizon, and T-mobile are planned in the next fiscal year.
* * *
-Wes
P.S.: If you thought this press release might be real, even for a second, consider why.
Maintenance of Certification: Beauty Is in the Eyes of the Beholder
This must-read paper from Drs Centor, Fleming and Moyer was recently published in the Annals of Internal Medicine. While it does not pertain to specialists, it serves as a level-headed rebuttal to the positive perspective of the Maintenance of Certification program (MOC) developed and marketed by the American Board of Internal Medicine and the American Board of Medical Specialties:
-Wes
Reference: Centor RM, Fleming DA,and Moyer, DV. "Maintenance of Certification: Beauty Is in the Eyes of the Beholder" from Ann Intern Med. 2014;161(3):226-227. doi:10.7326/M14-1014
While these authors' polite critique of the ABIM's method of assessing fellow physicians makes excellent points, we should still question the relevance of such a system for specialitist, especially for those who gain clinical and surgical experience over time. Furthermore, the MOC requirement that requires the performance of research on physicians using unscientifically validated patient surveys fails to afford doctors the most basic research protections created after the unintended consequences of similar well-meaning government research programs came to light. To ignore these additional shortcomings of the ABIM's MOC process should not be tolerated by any practicing member of our profession."There are no facts, only interpretations."
—Friedrich Nietzsche
In this issue, Baron and Johnson (1) describe the history of and rationale for the creation of the American Board of Internal Medicine (ABIM) and recent changes in maintenance of certification (MOC). They focus on setting standards and identifying “good doctors” who meet those standards. By implication, those who do not participate or are unsuccessful in achieving recertification are substandard. Although the ABIM is clearly proud of the MOC process that it has developed, many internists find it a source of great distress.
We suggest considering a basic observation in cognitive psychology, the affect heuristic, as a construct to help understand the disconnect between the ABIM's and internists' views of MOC (2–3). According to this heuristic, when we like a thing or an idea, we overestimate the benefits and underestimate the risks or unintended consequences. If we dislike something, we underestimate the benefits and overestimate the risks.
Those invested in developing the MOC process seem to highlight potential benefits and minimize possible unintended consequences. We have deep concerns that this well-intended policy will, indeed, cause negative consequences for physicians and society.
Over the past several months, we have heard from many internists about the MOC process. These physicians have a wide variety of training and experience and include well-trained, insightful, and skilled internists who share a commitment to maintaining high standards of professional performance. Yet, their concerns over the new demands that the MOC process entails are palpable. Their focus is on the potential unintended consequences, and they are struggling to acknowledge the potential benefits. When these physicians talk with us about MOC, frustration and dismay about the process dominate the conversations.
Internists feel increasing pressure from many directions. Time is an entity that none of us can recoup, and internists appropriately raise concerns about growing time pressures on all fronts (4). They are experiencing increasing administrative burdens that limit their ability to provide the type of patient care that they want to deliver.
These burdens include issues related to usability and interoperability of electronic health records, complex documentation requirements, growing requirements for prior authorization of the tests and treatments that they prescribe, and a payment system that does not recognize the time and effort that they spend on telephone or e-mail communication. The new MOC requirements add to this burden by being time-consuming and costly and having unclear benefits on patient care. Added to these concerns is a high-stakes, secure recertification examination whose first-time failure rate has increased from 10% to 22% over the past 5 years.
Although most first-time recertifying examinees who fail eventually pass the examination, they suffer distress and additional cost to retake it. Internists, like all physicians, want to bring their best, evidence-based practice to every patient every day. They want to test their knowledge and better their practices in a formative way to improve patient care and outcomes.
We worry that the ABIM may focus too much on metrics, administrative processes, and finding the “substandard doctors” who theoretically place the public at risk and too little on the design and implementation of a process that encourages ongoing education and professional development. The implication is that MOC will allow for better policing of “bad” internists rather than helping us all be “better” internists. We believe that the ABIM's stated accountability to the profession, which accompanies its accountability to the public, should lead to better recognition of dissatisfaction among its diplomates and a more collaborative approach with internal medicine specialty and subspecialty societies to address this dissatisfaction.
Unfortunately, the new MOC process has become the straw that broke the camel's back in many internists' minds. They dislike each part of the process but seem most angry about the practice improvement modules and secure examination. They see the first as “busy work” and the second as lacking relevance to their personal practice and to how medicine is currently practiced. The present structure of the summative secure examination of the ABIM does not provide specific feedback to facilitate this process let alone reflect the current state of practice, namely, collaboration in patient care and real-time engagement of evidence-based resources.
Any physician evaluation process should consider the practical wisdom, knowledge, and skill necessary to be a good practicing physician and test how those attributes are actually used in patient care. Fostering the development of phronesis (practical wisdom) in physicians through the effective and safe use of knowledge and skill in the clinical moment allows us to fulfill the covenant we have with patients and the contract we have with society.
Our internist colleagues tell us that they embrace the importance of remaining current, but they do not believe that the current MOC process helps them achieve that goal. As currently implemented, MOC involves substantial time, and internists believe that time supersedes more educationally sound activities. Current learning theory supports the use of testing to guide further learning and the provision of educational tools to address knowledge weaknesses.
Testing for knowledge alone does not determine how skilled and effective an internist is at the bedside, in history-taking, and in performing a targeted physical examination. Would it not be better and more practical to have a testing process that assesses the ability to gather and interpret information and that encompasses the entire clinical encounter? Can the MOC process as it stands truly evaluate our ability to deliver patient-centered care?
Too many internists view “professional self-regulation” as currently conceived by the ABIM to be a nonproductive and often punitive experience. All too often, they see regulatory bodies as depleting money, time, and joy from their professional lives. Further, many do not believe that burdensome processes being forced on them will benefit their patients or their professional lives. Thus, it should be no surprise that internists focus on the direct and indirect costs of MOC rather than on the potential benefits that are the focus of the current commentary of the ABIM leaders.
We recognize the ABIM's good intent and the substantive challenges of developing an effective assessment process that ensures a corps of good internists. Unfortunately, too many internists find some aspects of the current process lacking at a time when concerns about the ramifications of this high-stakes professional endeavor are increasing.
-Wes
Reference: Centor RM, Fleming DA,and Moyer, DV. "Maintenance of Certification: Beauty Is in the Eyes of the Beholder" from Ann Intern Med. 2014;161(3):226-227. doi:10.7326/M14-1014
The Tradeoffs of Obamacare
A few from above, from Saurabh Jha, MD (Twitter: @roguerad):
-Wes
The biggest trade-off is between a constitutional republic, with all its checks and balances, and a centrally-planned healthcare. The two are fundamentally incompatible. The future will yield many more convulsions. Many more Halbigs.Read the whole thing.
The optimism surrounding the ACA, summed up by President Obama's promise "if you like your doctor, you can keep your doctor," gave many the impression, myself included, that healthcare reform can be Pareto optimal; a win-win for all.
Regrettably, trade-offs are a fact of life. Which means there are winners and there are losers. This is not unusual. But by not acknowledging the trade-offs we have created resentment in the losers, and widened the partisan chasm.
-Wes
Sunday, August 10, 2014
From the Mouths of Babes
"Dad, you have the nicest patients!"
She was right, of course. Daughters that you bring to work with you to shadow for a day can bring you back to what's important in medicine. In fact, seeing medicine through fresh eyes is helpful, especially when we forget to look up from our work-a-day lives.
 It had been over ten years since I had my first "Bring Your Daugher to Work" experience. Her first time she wore scrubs they were bigger than she was. She always remembered that day.
It had been over ten years since I had my first "Bring Your Daugher to Work" experience. Her first time she wore scrubs they were bigger than she was. She always remembered that day.
There probably won't be too many more times we'll share such an experience together. Like most young college kids she's growing her own life now, trying to decide what to do.
"Why not shadow me and my nurse practitioner for a day to see what think? I have a light day, you could really see what we do first-hand!"
Much to my surprise, she agreed. And so we spent the entire day together once more.
She saw everything I did but this time with a more critical eye. She saw everything my nurse practitioner did, too. Just in case. She witnessed the miracle of anesthesia, a strangeness of the "time-out," then the jolt of a cardioversion. She saw the smile of the patient after it was all over. She saw the real discourse that occurs between colleagues that are used to working with each other. She saw the computer. She saw the EKG. She saw the family discussion afterward. Everything.
Perhaps most touching was the moment we walked into a long-time patient's room - a fellow doctor - and there he was, lying in bed with his ankles too swollen with his wife, daughter, and granddaughters by his side. His eyes, while a bit sunken, were beaming when he saw me.
"I'd like to introduce you you my family!" he exclaimed. And one by one he introduced me to his lovely wife, daughter, and granddaughters who had all come to spend some time with him. Of course, I couldn't resist, and similarly gushed, "I'd like to introduce you to a member of my family, too!" I proudly introducing my daughter to him and the rest of his extended family. His grandaughters were slightly younger than my daughter - just starting to think about college. My daughter, now a veteran of the college experience, offered some words of encouragement to them. They graciously nodded. I couldn't help but marvel how therapeutic that interaction was for both of us - doctor and patient - a way to bring our lives a bit closer, our understanding, more meaningful. Medicine is like that sometimes: one minute you're there to help the patient then you realize how much, in their grace, they help you.
I pretended not to think about this as I checked his defibrillator. "Working fine," I told him. He glanced at me and said "thank you" in a way I'll never forget: non-verbally with his eyes, as if to say, "I know how you're feeling."
We left the room and returned to the nurse's station - or maybe it should be called the "Computer Terminal Station," since doctors, pharmacists, physical therapists were all playing a game of musical chairs waiting for a terminal to open. More typing and staring at screens, more phone messages, documentation, lab checks, more typing, all clicked as fast as possible. Finally, after seeing more patients and typing more notes, we had a debriefing. Relaxed and looking forward to heading home, I asked her: "So what did you think?"
"You know, Dad, it was wonderful. Your patients are all so nice. But..."
There was a moment of hesitation in her voice, a concern, as she wrestled with how to break the news to me slowly; I could tell she didn't want to disappoint me.
"What is it?" I asked.
"... there's just so much typing!"
-Wes
She was right, of course. Daughters that you bring to work with you to shadow for a day can bring you back to what's important in medicine. In fact, seeing medicine through fresh eyes is helpful, especially when we forget to look up from our work-a-day lives.
It had been over ten years since I had my first "Bring Your Daugher to Work" experience. Her first time she wore scrubs they were bigger than she was. She always remembered that day.There probably won't be too many more times we'll share such an experience together. Like most young college kids she's growing her own life now, trying to decide what to do.
"Why not shadow me and my nurse practitioner for a day to see what think? I have a light day, you could really see what we do first-hand!"
Much to my surprise, she agreed. And so we spent the entire day together once more.
She saw everything I did but this time with a more critical eye. She saw everything my nurse practitioner did, too. Just in case. She witnessed the miracle of anesthesia, a strangeness of the "time-out," then the jolt of a cardioversion. She saw the smile of the patient after it was all over. She saw the real discourse that occurs between colleagues that are used to working with each other. She saw the computer. She saw the EKG. She saw the family discussion afterward. Everything.
Perhaps most touching was the moment we walked into a long-time patient's room - a fellow doctor - and there he was, lying in bed with his ankles too swollen with his wife, daughter, and granddaughters by his side. His eyes, while a bit sunken, were beaming when he saw me.
"I'd like to introduce you you my family!" he exclaimed. And one by one he introduced me to his lovely wife, daughter, and granddaughters who had all come to spend some time with him. Of course, I couldn't resist, and similarly gushed, "I'd like to introduce you to a member of my family, too!" I proudly introducing my daughter to him and the rest of his extended family. His grandaughters were slightly younger than my daughter - just starting to think about college. My daughter, now a veteran of the college experience, offered some words of encouragement to them. They graciously nodded. I couldn't help but marvel how therapeutic that interaction was for both of us - doctor and patient - a way to bring our lives a bit closer, our understanding, more meaningful. Medicine is like that sometimes: one minute you're there to help the patient then you realize how much, in their grace, they help you.
I pretended not to think about this as I checked his defibrillator. "Working fine," I told him. He glanced at me and said "thank you" in a way I'll never forget: non-verbally with his eyes, as if to say, "I know how you're feeling."
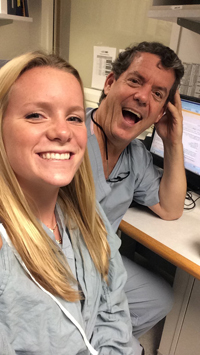 |
| Our "selfie" that day |
We left the room and returned to the nurse's station - or maybe it should be called the "Computer Terminal Station," since doctors, pharmacists, physical therapists were all playing a game of musical chairs waiting for a terminal to open. More typing and staring at screens, more phone messages, documentation, lab checks, more typing, all clicked as fast as possible. Finally, after seeing more patients and typing more notes, we had a debriefing. Relaxed and looking forward to heading home, I asked her: "So what did you think?"
"You know, Dad, it was wonderful. Your patients are all so nice. But..."
There was a moment of hesitation in her voice, a concern, as she wrestled with how to break the news to me slowly; I could tell she didn't want to disappoint me.
"What is it?" I asked.
"... there's just so much typing!"
-Wes
Wednesday, August 06, 2014
Medscape: 36% of Residents Have Over $200,000 Debt
From Medscape:
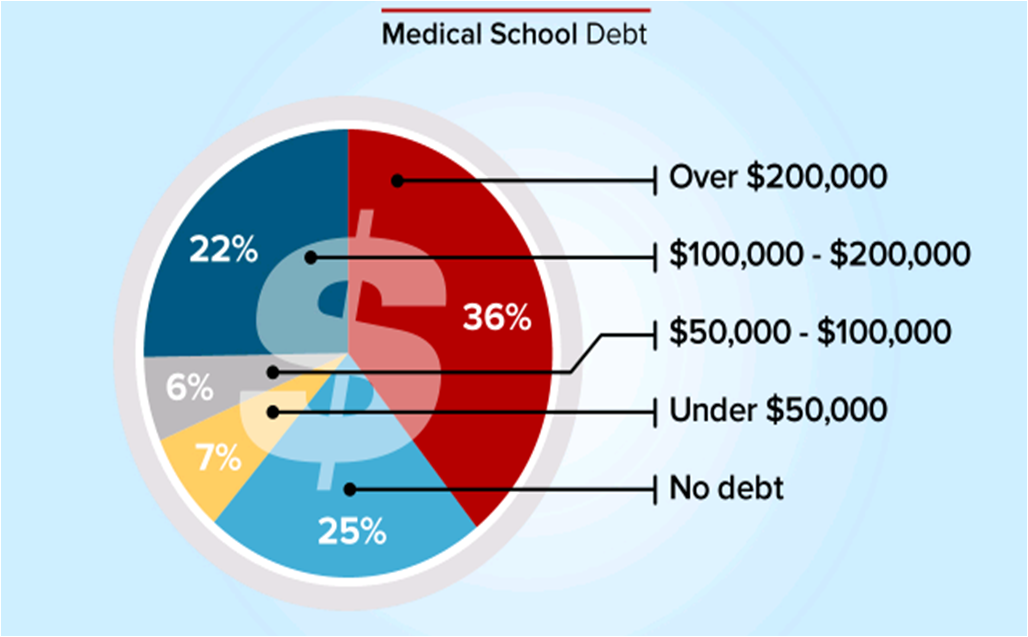
The same article quotes the average resident salary as $55,300. The actual "take-home"pay for residents is actually much lower and must be calculated for the state in which the doctor practices. For this, I turned to PayCheckCity.com's salary calculator.
Taking the $55,300 salary for a single doctor in Illinois, the weekly pay is $1063.46. From this comes the Federal withholding ($175.36), Social Security withholding ($65.93), Medicare withholding ($15.42), and Illinois witholding ($53.17), leaving $753.58 per week in income ($18.84 / hour for a 40-hour work week).
Now, if we just look at a monthly payment at 4.5% interest on a (conservative) $200,000 thirty-year loan, the monthy payment comes to $836.03. It becomes apparent that medical residents will have to work more than 8 days a month to just paying off their medical school loans.
More cheap money offered to residents in the form of new loans won't help this problem, it will only make things worse.
With the average public medical school tuition exceeding $207,000 and the average private medical school tuition exceeding $270,000, the joy of doctoring will quickly lose its luster for tomorrow's doctors-in-training.
And this crisis promises to only get larger for tomorrow's physicians.
For those planning on medical school, you might want to consider other sources of funding for your education. While the Navy had its drawbacks, at least I left medical school with $0 debt.
-Wes
The same article quotes the average resident salary as $55,300. The actual "take-home"pay for residents is actually much lower and must be calculated for the state in which the doctor practices. For this, I turned to PayCheckCity.com's salary calculator.
Taking the $55,300 salary for a single doctor in Illinois, the weekly pay is $1063.46. From this comes the Federal withholding ($175.36), Social Security withholding ($65.93), Medicare withholding ($15.42), and Illinois witholding ($53.17), leaving $753.58 per week in income ($18.84 / hour for a 40-hour work week).
Now, if we just look at a monthly payment at 4.5% interest on a (conservative) $200,000 thirty-year loan, the monthy payment comes to $836.03. It becomes apparent that medical residents will have to work more than 8 days a month to just paying off their medical school loans.
More cheap money offered to residents in the form of new loans won't help this problem, it will only make things worse.
With the average public medical school tuition exceeding $207,000 and the average private medical school tuition exceeding $270,000, the joy of doctoring will quickly lose its luster for tomorrow's doctors-in-training.
And this crisis promises to only get larger for tomorrow's physicians.
For those planning on medical school, you might want to consider other sources of funding for your education. While the Navy had its drawbacks, at least I left medical school with $0 debt.
-Wes
ABIM Placates Physician Anti-MOC Sentiment with "Commitments"
From the 5 Aug 2014 issue of the Journal of the American College of Cardiology (JACC):
Provide a 1-year grace period for those who have attempted but failed to pass the secure examination.
We can only imagine what this means. Does it mean your name won't be posted on the ABMS's Wall of Shame for a year so you can attempt to take the test twice more? Nowhere is there a concern for the lost revenue, additional hours of study, psychological stress, and damage to a physician's professional reputation created by this unproven process. While the ABIM acknowledges the increasing failure rate of their examinations in their "letter" to the Internal Medicine community, they provide no evidence of critical self-apprraisal nor a viable rationale for this. Instead, the spin is that doctors should feel grateful they were granted a 1-year grace period to complete the MOC testing.
Update its governance and financial information on its website.
Updating a website does not mean change in governance will occur at the ABIM. All ABIM members should be elected by physician peers, not selected by ABIM members themselves. Is this what they mean? Of course not. Do we really think these back-slapping chums will change their self-serving ways? The fact that ABIM members "exercise ultimate fiduciary responsibility and authority" is not acceptable to professionals whose livelihoods are placed at risk by ABIM members who remain unaccountable to those they regulate. Until physicians have an active voice in the ABIM's "governance," this organization's professional credibility will remain suspect.
Regarding the financial information they will disclose: How will they justify the high salaries of the executives of the member boards that exceed the salaries of the doctors they pretend to represent by many times? Will they insist on the disclosure of all conflicts of interest and income gained as consultants? So far, the ABIM has failed to list the transfers of funds between organizations like the ABIM and it's separate "ABIM Foundation" publicly. Shouldn't all financial and societal relationships with the ABMS, AMA, ACP, CMS, National Quality Forum, AMA's legal team, academic centers, the American Hospital Association, insurers and other "stakeholders" eager to use the ABIM's data trove be disclosed as well? Will the ABIM disclose how the survey and test data collected on their server is protected, sold and/or shared? Why is this unproven MOC process being promoted as a measure of physician "quality?" Why has it been allowed to continue as a Medicare physician payment incentive? Given these problems with fiscal transparency, why does our government collude with this private entity? If the ABIM's "governance and financial information" fails to change sufficiently or mention these specifics, physicians and the public have gained very little from any "commitments" promised by the ABIM.
Ensure a broader range of CME options for medical knowledge and skills self-assessment (Part II).
This is really not a concern, so why it was included as an "action item" for the ABIM is uncertain. Physicians have always had many ways to earn continuing medical education (CME) credits that do NOT involve the ABIM's MOC process and these MUST be preserved. Physicians to not want the ABIM to monopolize their ability to gain CME from other sources or methods, especially when the ABIM commands repeated high payments from physicians for their products.
Provide more feedback regarding test scores.
"Feedback" can come in many ways: statistics, providing answers, or maybe even disclosing a passing level. But let's be honest. Why do we care? Especially when failing still has significant employment, credentialing and social ramifications. Isn't the point to of life-long-learning to educate? Isn't the point to learn? Is forcing doctors to take a computerized test in a secure prison-like environment really beneficial to patients, or just a means of making subordinates of clinical professionals? Why do we physicians continue to allow such a punitive means for assessment to take hold when there is no independently validated evidence that MOC does anything to improve patient care?
Evolve the “patient survey” requirement to a “patient voice” requirement and increase the number of ways this requirement can be met.
Oh my goodness. Really? A "patient voice" requirement rather than a "patient survey?" The ABIM really has no idea whom they are serving. They have a Utopian vision for themselves: as one Great Overseer of All Things Perfect and to define for both doctors and "the Public" (whoever they feel that comprises) what "voice" we should all hear. I can see it now: patient's flying in a horrible thunderstorm with their doctor piloting the plane and the ABIM's answer to improving the safety of the flight? Make sure the patient's have a "voice" or let's pass out a "survey!" The reality today is that patients have a voice in their health care: they can go elsewhere, they can sue, they can critique their doctors publicly. To suggest that patients need a "voice" in assuring physician competency, courtesy of the ABIM's expensive MOC requirement, is not only patronizing, but insulting to both patients and doctors.
Reduce the data collection requirement for the practice assessment requirement; utilizing performance improvement activities already in place and minimizing the time and complexity of data input.
This is nothing new. It already existed and is exactly what I did recently in my recent recertification process in 2013.
Investigate changes in the secure examination to increase relevance with specific attention to exploring applications for practice focus areas (“modular examinations”) and open-book examinations.
This sounds like a Carte Blanche idea to expand the ABIM's reach and costs without oversight. Who will fund such an initiative? Who will regulate the spending of these self-imposed regulators? How can we control costs of this whole process when the process is continually expanded with such unrealistic and grandiose ideas? Isn't medicine and real life already an "open book test" for today's physicians? Why do we need the pleasure of paying $750 or even more for a another secure exam in a videotaped office building that prides itself on cavity searches? This whole process is already out of hand. Cut it back and make it manageable, don't expand it.
Why should anyone care about all of this? Yesterday morning, my good friend John Mandrola, MD sent a prescient tweet my way:
After all, actions speak louder than words.
-Wes
Addendum: If you've failed a recent Maintenance of Certification examination, I am still confidentially collecting stories from affected physicians. Please consider contributing yours.
"Note: There is evidence that the ABIM has heard the concerns of its diplomats and is acting responsively. In a July 10, 2014 letter to the internal medicine community, and in a face-to-face meeting in Philadelphia on July 15, 2014, which was attended by 26 internal medicine subspecialty societies including the ACC, the ABIM committed to:
- •Provide a 1-year grace period for those who have attempted but failed to pass the secure examination.
- •Update its governance and financial information on its website.
- •Ensure a broader range of CME options for medical knowledge and skills self-assessment (Part II).
- •Provide more feedback regarding test scores.
- •Evolve the “patient survey” requirement to a “patient voice” requirement and increase the number of ways this requirement can be met.
- •Reduce the data collection requirement for the practice assessment requirement; utilizing performance improvement activities already in place and minimizing the time and complexity of data input.
- •Investigate changes in the secure examination to increase relevance with specific attention to exploring applications for practice focus areas (“modular examinations”) and open-book examinations.
It is concerning that the ACC leadership feels the ABIM is "acting responsively" and continues to market the MOC proess so aggressively. Let's critically review the list of proposed ABIM "commitments" outlined above:For its part, the ACC has recently:
- •Released a special video that catalogs the suite of ACC resources available to help members meet the MOC Part IV requirements.
- •Determined that free-standing MOC modules will be offered to ACC members at no charge.
- •Posted online (CardioSource.org/MOC) a comprehensive list of ACC MOC Part II offerings. New modules will be added as they become available."
Provide a 1-year grace period for those who have attempted but failed to pass the secure examination.
We can only imagine what this means. Does it mean your name won't be posted on the ABMS's Wall of Shame for a year so you can attempt to take the test twice more? Nowhere is there a concern for the lost revenue, additional hours of study, psychological stress, and damage to a physician's professional reputation created by this unproven process. While the ABIM acknowledges the increasing failure rate of their examinations in their "letter" to the Internal Medicine community, they provide no evidence of critical self-apprraisal nor a viable rationale for this. Instead, the spin is that doctors should feel grateful they were granted a 1-year grace period to complete the MOC testing.
Update its governance and financial information on its website.
Updating a website does not mean change in governance will occur at the ABIM. All ABIM members should be elected by physician peers, not selected by ABIM members themselves. Is this what they mean? Of course not. Do we really think these back-slapping chums will change their self-serving ways? The fact that ABIM members "exercise ultimate fiduciary responsibility and authority" is not acceptable to professionals whose livelihoods are placed at risk by ABIM members who remain unaccountable to those they regulate. Until physicians have an active voice in the ABIM's "governance," this organization's professional credibility will remain suspect.
Regarding the financial information they will disclose: How will they justify the high salaries of the executives of the member boards that exceed the salaries of the doctors they pretend to represent by many times? Will they insist on the disclosure of all conflicts of interest and income gained as consultants? So far, the ABIM has failed to list the transfers of funds between organizations like the ABIM and it's separate "ABIM Foundation" publicly. Shouldn't all financial and societal relationships with the ABMS, AMA, ACP, CMS, National Quality Forum, AMA's legal team, academic centers, the American Hospital Association, insurers and other "stakeholders" eager to use the ABIM's data trove be disclosed as well? Will the ABIM disclose how the survey and test data collected on their server is protected, sold and/or shared? Why is this unproven MOC process being promoted as a measure of physician "quality?" Why has it been allowed to continue as a Medicare physician payment incentive? Given these problems with fiscal transparency, why does our government collude with this private entity? If the ABIM's "governance and financial information" fails to change sufficiently or mention these specifics, physicians and the public have gained very little from any "commitments" promised by the ABIM.
Ensure a broader range of CME options for medical knowledge and skills self-assessment (Part II).
This is really not a concern, so why it was included as an "action item" for the ABIM is uncertain. Physicians have always had many ways to earn continuing medical education (CME) credits that do NOT involve the ABIM's MOC process and these MUST be preserved. Physicians to not want the ABIM to monopolize their ability to gain CME from other sources or methods, especially when the ABIM commands repeated high payments from physicians for their products.
Provide more feedback regarding test scores.
"Feedback" can come in many ways: statistics, providing answers, or maybe even disclosing a passing level. But let's be honest. Why do we care? Especially when failing still has significant employment, credentialing and social ramifications. Isn't the point to of life-long-learning to educate? Isn't the point to learn? Is forcing doctors to take a computerized test in a secure prison-like environment really beneficial to patients, or just a means of making subordinates of clinical professionals? Why do we physicians continue to allow such a punitive means for assessment to take hold when there is no independently validated evidence that MOC does anything to improve patient care?
Evolve the “patient survey” requirement to a “patient voice” requirement and increase the number of ways this requirement can be met.
Oh my goodness. Really? A "patient voice" requirement rather than a "patient survey?" The ABIM really has no idea whom they are serving. They have a Utopian vision for themselves: as one Great Overseer of All Things Perfect and to define for both doctors and "the Public" (whoever they feel that comprises) what "voice" we should all hear. I can see it now: patient's flying in a horrible thunderstorm with their doctor piloting the plane and the ABIM's answer to improving the safety of the flight? Make sure the patient's have a "voice" or let's pass out a "survey!" The reality today is that patients have a voice in their health care: they can go elsewhere, they can sue, they can critique their doctors publicly. To suggest that patients need a "voice" in assuring physician competency, courtesy of the ABIM's expensive MOC requirement, is not only patronizing, but insulting to both patients and doctors.
Reduce the data collection requirement for the practice assessment requirement; utilizing performance improvement activities already in place and minimizing the time and complexity of data input.
This is nothing new. It already existed and is exactly what I did recently in my recent recertification process in 2013.
Investigate changes in the secure examination to increase relevance with specific attention to exploring applications for practice focus areas (“modular examinations”) and open-book examinations.
This sounds like a Carte Blanche idea to expand the ABIM's reach and costs without oversight. Who will fund such an initiative? Who will regulate the spending of these self-imposed regulators? How can we control costs of this whole process when the process is continually expanded with such unrealistic and grandiose ideas? Isn't medicine and real life already an "open book test" for today's physicians? Why do we need the pleasure of paying $750 or even more for a another secure exam in a videotaped office building that prides itself on cavity searches? This whole process is already out of hand. Cut it back and make it manageable, don't expand it.
Why should anyone care about all of this? Yesterday morning, my good friend John Mandrola, MD sent a prescient tweet my way:
Yet another of Louisville's finest docs sends letter of resignation. Experienced docs are leaving in droves. No one is secure. @doctorwesSenior doctors are getting tired of all the nonsense in medicine these days. And nowhere is there more nonsense that the ABIM's complicated Maintenance of Certification program. Their continuing education program is far too cumbersome, onerous, and expensive and supplies little to no marginal utility for patients relative to the care that their physicians provide. As a result, the ABIM's MOC process is causing more harm than good to patient care while also compromising physician retention. Unless this is horrible mess is greatly simplified or stopped all together, look for more and more doctors to move on to other less hostile work environments or to simply retire.
— John Mandrola, MD (@drjohnm) August 5, 2014
After all, actions speak louder than words.
-Wes
Addendum: If you've failed a recent Maintenance of Certification examination, I am still confidentially collecting stories from affected physicians. Please consider contributing yours.
Wednesday, July 30, 2014
Fail Maintenance of Certification? I Need Your Help
With the increasing failure rate of first-time test takers of the American Board of Medical Specialties' Maintenance of Certification program, no study of the impact of failing the examination upon physicians (and the patients they serve) has occurred. Specifically, I am interested in the economic, professional and psychologic consequences of failing the Maintenance of Certification examination for previously board-certified practicing physicians.
To that end, I'd like to compile the stories of people who have FAILED their Maintenance of Certification examination. I would like to know the cost in both time, money and consequences that was impacted by the failure, whatever they were or were not. I hope to publish a paper in a major medical journal on my findings. Commentary can be sent to me one of two ways: (1) private e-mail (wes -at- medtees dot com) or (2) by placing a comment to this post (since all comments are moderated, I will only publish those that I am granted specific permission to publish) here.
I would like to know the following:
(1) A bit about you: your age, gender, specialty, years in practice, practice setting
(2) Number of patients you treat annually
(3) A description of what it was like to learn you failed, actions taken (re-score request, additional review course, repeat testing, retirement), loss of income.
(4) Impact to ability to practice, if any (loss of privileges, etc)
(5) Cost, but in time and money spent for the various parts of the process.
(6) Did your results appear on the website "CertificationMatters.org"
(7) Willingness to co-author a manuscript
(8) THIS ONE'S IMPORTANT: Willingness to have your name mentioned publically. ALL RESPONSES WILL BE KEPT STRICTLY CONFIDENTIAL otherwise.
(Any other data you think is important and I have missed and would like included or NOT mentioned)
I will compile the data I receive, both as discrete variables and comments that allow publication.
It is quite possible that many academic journals will not publish the results obtained in this survey and, if so, I will co-publish the composite data on this blog for all to review.
I appreciate any and all feedback I might be able to obtain. The face of the dark side of Maintenance of Certification needs to be understood and reported.
Thanks for your coooperation in this effort.
Sincerely,
Wes Fisher, MD
To that end, I'd like to compile the stories of people who have FAILED their Maintenance of Certification examination. I would like to know the cost in both time, money and consequences that was impacted by the failure, whatever they were or were not. I hope to publish a paper in a major medical journal on my findings. Commentary can be sent to me one of two ways: (1) private e-mail (wes -at- medtees dot com) or (2) by placing a comment to this post (since all comments are moderated, I will only publish those that I am granted specific permission to publish) here.
I would like to know the following:
(1) A bit about you: your age, gender, specialty, years in practice, practice setting
(2) Number of patients you treat annually
(3) A description of what it was like to learn you failed, actions taken (re-score request, additional review course, repeat testing, retirement), loss of income.
(4) Impact to ability to practice, if any (loss of privileges, etc)
(5) Cost, but in time and money spent for the various parts of the process.
(6) Did your results appear on the website "CertificationMatters.org"
(7) Willingness to co-author a manuscript
(8) THIS ONE'S IMPORTANT: Willingness to have your name mentioned publically. ALL RESPONSES WILL BE KEPT STRICTLY CONFIDENTIAL otherwise.
(Any other data you think is important and I have missed and would like included or NOT mentioned)
I will compile the data I receive, both as discrete variables and comments that allow publication.
It is quite possible that many academic journals will not publish the results obtained in this survey and, if so, I will co-publish the composite data on this blog for all to review.
I appreciate any and all feedback I might be able to obtain. The face of the dark side of Maintenance of Certification needs to be understood and reported.
Thanks for your coooperation in this effort.
Sincerely,
Wes Fisher, MD
Monday, July 28, 2014
Should Cardiologists Boycott the 2014 TCT/ACC Conference?

In reality, most cardiologists couldn't care less about Ms. Clinton. They'll oversleep or consider her address as nothing more than marketing theater. But to dismiss Ms. Clinton's presence at this event misses some important considerations.
Is the purpose of the TCT conference to hobnob and aggrandize politicians, especially one who could become President, or is to educate and inform physicians? Is the purpose of paying Ms. Clinton's hefty speaking fee about gaining her ear, or to make a political contribution from Big Business and the crony capitalism that pervades health care now? Is the real purpose to of her presence as keynote speaker to address cardiologists real concerns or so that ACC leadership can position their proprietary NCDR databases and "Appropriateness Criteria" as quality metrics to permanently pad their bottom line? Suddenly, Ms. Clinton's appearance takes on more cardiovascular gravitas.
Every cardiologist sitting in that hall will have just come through a year experiencing less time with their patients, less clinical autonomy, intrusions on their practice, while increasingly being coerced to perform bureaucratic tasks that mean little to patients yet everything to corporate interests. What do we imagine will, in fact, be addressed by Ms. Clinton as we buy our plane tickets and carefully pack our suitcases? Do we think for one moment that Ms. Clinton or the ACC will have the slightest compunction to address the serious concerns of the cardiology community? What do we imagine the ACC will address about these concerns in the rest of the meeting?
ACC should wake up to a new reality. Recall that it was a small group of cardiologists who started the anti-Maintenance of Certification (MOC) petition against the new, more onerous MOC program devised by the privately held American Board of Medical Specialties and the American Board of Internal Medicine. Over 18,000 doctors of all types have signed that petition now. In response to that petition, the ACC performed a survey of their member chapters nationwide. The anti-MOC sentiment from this survey was overwhelming. Many senior doctors even mentioned it might make them consider early retirement. In turn, the ACC's response was lukewarm at best. This was likely because the ACC's history has been to support the lucrative review courses this program requires. These courses are so important to the ACC's bottom line that they even devoted an entire "MOC Complex" hall at their last scientific session to promote the MOC program and still aggressively market the program on their website. This is hardly a show of solidarity with their member cardiologists'.
{kind=link}
It is time front line cardiologists put action behind their anger over the MOC process and the ACC's indifference. It is time to consider a boycott of the ACC/TCT meeting in Washington.
To that end, the ACC leadership needs to stop pandering to politicians and corporations eager to profit on doctors and instead start advocating for their own members. The preeminent assumption in program planning at events such as these appears to be that physicians are passive, apolitical, and unaware. Why would the ACC or any other physician membership organization feel the need to change? For this reason, the time to boycott is now. If the boycott is successful, perhaps the ACC leadership will take the concerns of the member cardiologists' more seriously than the politics of creating public-private partnerships that threaten to compromise, rather than promote, the care of our patients. Does the ACC really believe they can remain relevant without physician participation? We should note that alternative professional organizations are beginning to evolve.
Whether the ACC has realized this or not, they are coming to a juncture where they will have to decide whether they represent physicians and their patients or the Iron Triangle. Physicians are not lawyers, they are uncomfortable acting collectively or politically, much to their detriment in this era of rapidly morphing health care regulation and intrusion. I can still hope that the ACC and other organizations such as state medical societies will have the capacity to represent the real interests of their physician members. But increasingly I am concerned they won't.
But we should be clear: physicians' actions mean something. So this doctor will not be attending this year's meeting because it's one of the only ways I have left to send a message.
I hope others will consider the same.
-Wes
Saturday, July 26, 2014
MOC Points: The New Physician Currency
"Oh my God, I can't believe how complicated the American Board of Medical Specialties and the American Board of Internal Medicine has made this whole Maintenance of Certification (MOC) process!"
"Yeah, pretty amazing, isn't it? 10 points here, 10 points there, 20 points for a (required) Practice Improvement Module, then another 10 points if you complete another module online. And after all that, you're only half way there!"
"Where am I going to find the time? They need to make this process easier!"
"Face it. That isn't going to happen. Look at the ineffectual ideas the member board members are telling the ABIM leadership in their precious '3-5 minutes' of feedback: making sure physicians can get 'credit' for patient surveys and quality assurance projects they already do, making the ABIM website 'easier-to-navigate,' making patient surveys 'more flexible,' lowering costs, and 'providing more transparency from ABIM on how requirements are created.' I'm not seeing any cuts to any of this, I'm just seeing different versions of the same old same-old."
"Dude, you just completed your MOC process, how did you do it?"
"I'll tell you a secret, but you have to promise TOTAL secrecy."
"I promise! I'll do ANYTHING to get this MOC monkey off my back!"
"Okay, here's what you do. Remember that research project you wanted to do on kids but never could get off the ground because the IRB stonewalled you, claiming lack of consent in minors and all that red tape regarding research in minors?"
"Yeah."
"Well, just call your work a 'quality assurance project' you have to do for your MOC points! No one would dare question your intent, after all, it's to improve quality care and patient safety!"
"I can't do that."
"Sure you can! No one dares question the lofty ideals of the ABMS/ABIM's MOC program. After all, they interconnected with the ACGME, the Joint Commission, American Medical Association, the American Hospital Association, the whole works! You just do your thing and no one will think anything of it except 'you're the MAN!' I mean these MOC points are our new hall pass to do anything you like on people in the name of quality of care! It just has to sound reasonable. And man, you need those points, don't you? You'd be killing two birds with one stone and potentially get a publication out of it to boot! Better yet, you can claim "no conflicts of interest" because you never receive a dime for your efforts. Your IRB will never look, trust me. Paraphrasing a former famous politician: 'I've got this MOC thing, and it's f*%^in' golden!"
"I see. And if we do it your way, we can even get paid more, thanks to that CMS incentive they've created!"
"Now you're catchin' on. It's our new currency. I'm telling you, it's f*%^in' golden!"
-Wes
h/t: IP4PI blog
"Yeah, pretty amazing, isn't it? 10 points here, 10 points there, 20 points for a (required) Practice Improvement Module, then another 10 points if you complete another module online. And after all that, you're only half way there!"
"Where am I going to find the time? They need to make this process easier!"
"Face it. That isn't going to happen. Look at the ineffectual ideas the member board members are telling the ABIM leadership in their precious '3-5 minutes' of feedback: making sure physicians can get 'credit' for patient surveys and quality assurance projects they already do, making the ABIM website 'easier-to-navigate,' making patient surveys 'more flexible,' lowering costs, and 'providing more transparency from ABIM on how requirements are created.' I'm not seeing any cuts to any of this, I'm just seeing different versions of the same old same-old."
"Dude, you just completed your MOC process, how did you do it?"
"I'll tell you a secret, but you have to promise TOTAL secrecy."
"I promise! I'll do ANYTHING to get this MOC monkey off my back!"
"Okay, here's what you do. Remember that research project you wanted to do on kids but never could get off the ground because the IRB stonewalled you, claiming lack of consent in minors and all that red tape regarding research in minors?"
"Yeah."
"Well, just call your work a 'quality assurance project' you have to do for your MOC points! No one would dare question your intent, after all, it's to improve quality care and patient safety!"
"I can't do that."
"Sure you can! No one dares question the lofty ideals of the ABMS/ABIM's MOC program. After all, they interconnected with the ACGME, the Joint Commission, American Medical Association, the American Hospital Association, the whole works! You just do your thing and no one will think anything of it except 'you're the MAN!' I mean these MOC points are our new hall pass to do anything you like on people in the name of quality of care! It just has to sound reasonable. And man, you need those points, don't you? You'd be killing two birds with one stone and potentially get a publication out of it to boot! Better yet, you can claim "no conflicts of interest" because you never receive a dime for your efforts. Your IRB will never look, trust me. Paraphrasing a former famous politician: 'I've got this MOC thing, and it's f*%^in' golden!"
"I see. And if we do it your way, we can even get paid more, thanks to that CMS incentive they've created!"
"Now you're catchin' on. It's our new currency. I'm telling you, it's f*%^in' golden!"
-Wes
h/t: IP4PI blog
Tuesday, July 22, 2014
What Main Stream Media Misses in the MOC Debate
This morning the American Board of Medical Specialties' (ABMS) Maintenance of Certification (MOC) program debate reached a larger mainstream media audience when the Wall Street Journal published their article by Melissa Beck entitled "Skill Reviews Upset Doctors."
While it is certainly nice to see an article reaching the main stream media concerning doctors' concerns with the MOC program, the issue with the MOC debate is not that doctors are upset. The real issue is that doctors have been enslaved by special interests and crony capitalism to complete a MOC process that robs patients of more time with their doctors so that regulators and payers can enrich themselves.
One only has to see how certain aspects of the Wall Street Journal article were highlighted to see how Ms. Beck framed the debate toward business interests. For instance, she quoted Ms. Lois Nora, president of American Board of Medial Specialties who said:
"Many practicing physicians have not had formal courses in patient safety or quality improvment."
Ahem. I wonder if Ms. Beck or Ms. Nora have ever heard of the Hippocratic Oath? Doctors spend their entire careers (not to mention many sleepless nights) worrying about their patients' safety and care. Their livelihoods depend on it!
Yet there is never a moment of serious reflection regarding the sweeping hubris of Ms. Nora's statement. As spokesperson for the American Board of Medical Specialties, Ms. Nora suggests that without oversight, doctors are lax, uninterested in research or updating their techniques, inattendant to patient safety and unwilling to update their skills. Instead, the ABMS welcomes the tripling of patient volumes, the cameo roles that doctors are increasingly asked to play in patient care, the refocusing of one third to one half of every patient visit staring into an electronic medical record so the ABMS can watch for flinches in quality of care. The overseer who allowed this untenable health care scenario to transpire is effectively positioning themselves to patients that they are their last best hope.
Ms. Beck's piece also ignored the existing CME requirements that physicians already must perform each year to remain licensed and the value of such truly voluntary learning. Instead, Ms. Beck chose to highlight a quote from Richard Armstrong, MD - a board certified surgeon clearly without formal media training - who said: "No one wants to come out and say we're against quality, but most physicians find these modules to be cumbersome and, frankly, a joke."
When doctors are quoted calling any quality process "a joke," it really doesn't matter what the doctor actually said, for few will take him seriously. Let's be clear: the MOC process is not a joke, it's more like the twisted controlling strategy of the Hunger Games.
Ms. Beck also ignored that some MOC requirements now involve enrolling patients into study groups without their consent, doing the study and then reporting the data back to the boards. According to one doctor, "there are nearly 400 research projects being done on children through part 4 of the ABMS MOC program. Not only is performing research on children without consent immoral, it is costly in both time and money for the patient." Isn't this consideration important for patients?
Finally, Ms. Beck's article ends with the ABMS's claim that "500,000 of the more than 800,000 board-certified physicians have enrolled in MOC programs to date" implying that the majority of doctors support the program. Yet this statistic completely ignores the fact that doctors had no choice but to sign up for MOC despite their better judgement. As Ms. Beck hesitantly acknowledges in her article, this unproven physician metric is now increasingly tied to measures of physician "quality," hospital privileges, legal standing in court, and insurance panels. This unproven MOC program that was created by a self-appointed, private organization that is completely unaccountable to the public has also been indelibly etched into our new health care law.
No, it's better not to mention these unethical and extortionary tactics by the ABMS that threaten patient care.
Instead, it's far better to call doctors "upset."
-Wes
While it is certainly nice to see an article reaching the main stream media concerning doctors' concerns with the MOC program, the issue with the MOC debate is not that doctors are upset. The real issue is that doctors have been enslaved by special interests and crony capitalism to complete a MOC process that robs patients of more time with their doctors so that regulators and payers can enrich themselves.
One only has to see how certain aspects of the Wall Street Journal article were highlighted to see how Ms. Beck framed the debate toward business interests. For instance, she quoted Ms. Lois Nora, president of American Board of Medial Specialties who said:
"Many practicing physicians have not had formal courses in patient safety or quality improvment."
Ahem. I wonder if Ms. Beck or Ms. Nora have ever heard of the Hippocratic Oath? Doctors spend their entire careers (not to mention many sleepless nights) worrying about their patients' safety and care. Their livelihoods depend on it!
Yet there is never a moment of serious reflection regarding the sweeping hubris of Ms. Nora's statement. As spokesperson for the American Board of Medical Specialties, Ms. Nora suggests that without oversight, doctors are lax, uninterested in research or updating their techniques, inattendant to patient safety and unwilling to update their skills. Instead, the ABMS welcomes the tripling of patient volumes, the cameo roles that doctors are increasingly asked to play in patient care, the refocusing of one third to one half of every patient visit staring into an electronic medical record so the ABMS can watch for flinches in quality of care. The overseer who allowed this untenable health care scenario to transpire is effectively positioning themselves to patients that they are their last best hope.
Ms. Beck's piece also ignored the existing CME requirements that physicians already must perform each year to remain licensed and the value of such truly voluntary learning. Instead, Ms. Beck chose to highlight a quote from Richard Armstrong, MD - a board certified surgeon clearly without formal media training - who said: "No one wants to come out and say we're against quality, but most physicians find these modules to be cumbersome and, frankly, a joke."
When doctors are quoted calling any quality process "a joke," it really doesn't matter what the doctor actually said, for few will take him seriously. Let's be clear: the MOC process is not a joke, it's more like the twisted controlling strategy of the Hunger Games.
Ms. Beck also ignored that some MOC requirements now involve enrolling patients into study groups without their consent, doing the study and then reporting the data back to the boards. According to one doctor, "there are nearly 400 research projects being done on children through part 4 of the ABMS MOC program. Not only is performing research on children without consent immoral, it is costly in both time and money for the patient." Isn't this consideration important for patients?
Finally, Ms. Beck's article ends with the ABMS's claim that "500,000 of the more than 800,000 board-certified physicians have enrolled in MOC programs to date" implying that the majority of doctors support the program. Yet this statistic completely ignores the fact that doctors had no choice but to sign up for MOC despite their better judgement. As Ms. Beck hesitantly acknowledges in her article, this unproven physician metric is now increasingly tied to measures of physician "quality," hospital privileges, legal standing in court, and insurance panels. This unproven MOC program that was created by a self-appointed, private organization that is completely unaccountable to the public has also been indelibly etched into our new health care law.
No, it's better not to mention these unethical and extortionary tactics by the ABMS that threaten patient care.
Instead, it's far better to call doctors "upset."
-Wes
An Insider's Guide to a Health Care Policy White Paper
Do you want to "raise awareness" of how physician quality and value information impacts health care decision making? Do you want to spin your data via the Associated Press internationally?
Just have the Robert Wood Johnson Foundation pay for a survey!
We all know how great surveys are, especially when you design it to "raise awareness" for the low, low price of $604,454!
For that price, you get:
(1) A nice glossy white paper that contains a concerned patient looking away while she's being examined by a doctor on the cover
(2) Lots and lots of numbers and scientific-looking charts.
(3) An NORC Press release (After all, it was laundered through the Associated Press-NORC Center for Public Policy Research!)
(4) A republishing of your "key points" by a few business-minded online health care journals eager to demonstrate relevance of using "quality measures" to determine health care "value."
(5) An opportunity to collaborate "on all aspects of the study!"
See how easy it is to make sure you get your major points out there to the decision makers! (Never mind that a quality physician means many different things to many different people - stop being a perfectionist, okay?)
Look, these guys did a survey with 25% response rate that totaled a whopping 1002 people - or about 0.000000317 of the current US population! Heck, no bias there, right? Then they add a few "sampling weights" and calculate the survey response rate using the important sounding American Association of Public Opinion Research's Method 3!
What's that? You're not familiar with Method 3? What kind of scientist ARE YOU????
Here. Let me help: If Method 1,2, or 4 doesn't get you the desired number, you use Method 3! The survey response rate for Method 3 is calculated from the handy, dandy Response Rate Method Calculator where:
I = Complete Interviews
R = Refusal and Break Offs
NC = Non-contacts
O = Other
e = the estimated cases of unknown eligibility that are eliglible! (In other words, a guess)
UH = Unknown Household
UO = Unknown Other
Using these definitions , the "Method 3" calculation for the survey response rate becomes:
I / (( I+P) + (R + NC + O) + e(UH + UO))
See? And that response rate, according to the white paper, after applying "sampling weights" had "an overall margin of error" of "+/- 4.0 percentage points, including the design effect resulting from the complex sample design."
Heck ya, I'm seeing accuracy there, aren't you?
These days, it's really important that lots of people see these data so policy makers (who have about as much scientific wattage as an LED), can turn to them to create controlling policy and regulations that benefit those who make - you got it - the policy and regulations! Especially in US health care. That's because doctors are getting a bit unruly and need to understand why they must fall in line on all this physician quality measurement stuff. Perhaps one of the introductory paragraphs of the published white paper says it best:
It's important that we all understand just how critical these surveys paid for by political organizations will be to health care in the years ahead. Spin, you see, is everything. Thank goodness the Robert Wood Johnson Foundation (who's CEO, by the way, has also partnered on other publications about patient safety and medical professionalism with members of the American Board of Internal Medicine and National Quality Forum) can show us the way!
I feel so reassured that this is the caliber of science being used to shape US health care now.
Seriously.
What could go wrong?
-Wes
Just have the Robert Wood Johnson Foundation pay for a survey!
We all know how great surveys are, especially when you design it to "raise awareness" for the low, low price of $604,454!
For that price, you get:
(1) A nice glossy white paper that contains a concerned patient looking away while she's being examined by a doctor on the cover
(2) Lots and lots of numbers and scientific-looking charts.
(3) An NORC Press release (After all, it was laundered through the Associated Press-NORC Center for Public Policy Research!)
(4) A republishing of your "key points" by a few business-minded online health care journals eager to demonstrate relevance of using "quality measures" to determine health care "value."
(5) An opportunity to collaborate "on all aspects of the study!"
See how easy it is to make sure you get your major points out there to the decision makers! (Never mind that a quality physician means many different things to many different people - stop being a perfectionist, okay?)
Look, these guys did a survey with 25% response rate that totaled a whopping 1002 people - or about 0.000000317 of the current US population! Heck, no bias there, right? Then they add a few "sampling weights" and calculate the survey response rate using the important sounding American Association of Public Opinion Research's Method 3!
What's that? You're not familiar with Method 3? What kind of scientist ARE YOU????
Here. Let me help: If Method 1,2, or 4 doesn't get you the desired number, you use Method 3! The survey response rate for Method 3 is calculated from the handy, dandy Response Rate Method Calculator where:
I = Complete Interviews
R = Refusal and Break Offs
NC = Non-contacts
O = Other
e = the estimated cases of unknown eligibility that are eliglible! (In other words, a guess)
UH = Unknown Household
UO = Unknown Other
Using these definitions , the "Method 3" calculation for the survey response rate becomes:
I / (( I+P) + (R + NC + O) + e(UH + UO))
See? And that response rate, according to the white paper, after applying "sampling weights" had "an overall margin of error" of "+/- 4.0 percentage points, including the design effect resulting from the complex sample design."
Heck ya, I'm seeing accuracy there, aren't you?
These days, it's really important that lots of people see these data so policy makers (who have about as much scientific wattage as an LED), can turn to them to create controlling policy and regulations that benefit those who make - you got it - the policy and regulations! Especially in US health care. That's because doctors are getting a bit unruly and need to understand why they must fall in line on all this physician quality measurement stuff. Perhaps one of the introductory paragraphs of the published white paper says it best:
"Major investments are being made in health care systems like Accountable Care Organizations and in tools like Physician Compare. Similarly, health insurers and employers are exploring new benefits designs that incentivize consumers to select providers and hospitals that provide the highest-quality care while reducing costs through value-based provider networks and tiered health plans."So there you have it!
It's important that we all understand just how critical these surveys paid for by political organizations will be to health care in the years ahead. Spin, you see, is everything. Thank goodness the Robert Wood Johnson Foundation (who's CEO, by the way, has also partnered on other publications about patient safety and medical professionalism with members of the American Board of Internal Medicine and National Quality Forum) can show us the way!
I feel so reassured that this is the caliber of science being used to shape US health care now.
Seriously.
What could go wrong?
-Wes
Sunday, July 13, 2014
The Game of Numbers
The dark underbelly of health care is becoming all too visible now.
Fresh faces in neatly pressed white coats are in the halls. Eager. Enthusiastic. Clearly very bright. All hoping for a moment, an experience, an encounter that makes all their hard work worth it. Surely they'll have one, but not before the thousands of keyboard clicks, the mandatory lectures, rounds and lots of lengthy, lonely call nights.
He was a doctor from another time, well into his 80's. Lovely man with an infectious smile, mesmerizing foreign accent, and almost regal presence. An authority in his time and still attends lectures to stay engaged, a question passed his way from time to time out of respect for his experience and insights.
But he kept nearly falling at night and became concerned; even confused once. This was not like him. So he was admitted, observed and had a heart rhythm that was not normal. Blood thinners were started cautiously. Surely he could manage them. His wife, ever-present at his side, was equally engaging, concerned. And so, as fate would have it, after hundreds of thousands of keyboard clicks, I came to know them and realize his heart beat was too slow at times, dangerously so.
After lengthy discussions of the good and bad, the options, the data, he agreed a pacemaker made sense. Trustingly, he wanted it performed soon, eager to return to the lectures he loved. So the next morning after a night of worry, we assembled. His smile greeted me as I came to his bedside to obtain written consent, answer any last-minute questions, and silence the noise of concern. He was ready to go.
So I left his bedside to change into my scrubs, trying to hang my newly pressed shirt and tie to the side to preserve it for later behind a changing room curtain, when I heard a voice.
"Dr. Fisher, I'm so sorry..."
"What's up?"
"We can't bring your patient in the room."
"Why not?"
"We didn't know he's UnitedHealthCare. He's Medicare Part C!"
"Wha...?"
"You placed your order after 4PM, and we didn't see it until this morning. We have to get pre-approval from UnitedHealthCare for his pacemaker. They said it would be two or three hours..."
"Seriously?"
"Yes. It's his insurance. If you don''t get pre-approval, you won't get paid and he might have to pay for the procedure."
I stood, pants in hand, dumfounded. So I finished changing and exiting the changing area to clear my head. I called our administrator. She said, "Let me see what I can do. I'll call you right back." Within minutes a reply was sent: "You have to wait."
I thought of my frightened patient lying there vulnerable, so I went to his bedside to explain. He looked at me as a fellow physician, and he shook his head in disbelief, all the while naked beneath the covers. He agreed to wait - he had no choice. I left to get a cup of coffee and to collect my thoughts. What else could I do? I put a detailed note, an order, a consent order last night, and a pre-anesthetic note this morning. All keyed in, all according to protocol.
Then a nurse appeared with a note.
"If you call this number, hit "3" on the menu selection, and enter this case number, you can do a peer-to-peer."
"A what?"
"Peer-to-peer approval. You talk to a medical director and they might be able to expedite the approval for the pacemaker."
I looked for a moment at the "800" number, sighed, and called.
The woman who eventually answered after I heard "all attendants are busy" was pleasant enough, full of "good morning, doctor" and "what can I do for you." I explained the situation and wanted the ordering physician's name. I spelled my name to her. Keyboards were heard in the background.
"I see that his is for a CPT code 33208, correct?" She must have known that I knew my codes. But I knew that was wrong. He was not getting a dual chamber pacemaker, he just needed a single chamber, VVIR pacemaker.
"No, that's not correct. It should be 33207," I replied.
"Oh."
I heard more clicking.
"I'm sorry but I've tried to change that code under this case number and it seems I don't have authorization to do that. Can I put you on hold while I speak with the medical director to see if he can make the change?"
"Sure," I said. What choice did I have?
So I waited, listening to some nondescript melody in the background as I was placed on hold. A few minutes later, the same voice returned.
"Doctor?"
"Yes?"
"It seems the medical director couldn't change the information on this case number either, but I'm going to try to make a new number based on the CPT code you gave me, then I'll have the right information to give to the medical director, okay?"
So we proceeded to build a new case number. Lots of clicks interspersed with silence, then more clicks in the background, a few more statements like, "Sorry, I'm new to this" and "could you spell your name again," then finally:
"There. I think I've done it. Let me transfer you to our medical director...."
A click, some music, then a pleasant official-sounding woman's voice. "This is Doctor Frigamafrats. I'm sorry about the delay, I hope you didn't have to wait too long..."
A conversation ensued. I explained the rationale for the pacemaker, then finally was granted approval. Case number 2342343240 and approval number A321232451, or something like that. I notified the staff and handed the numbers to our clerk, knowing full well that pre-approval does not guarantee payment. Forty minutes rather than 120.
It's the game we play now. A new game. The Game of Numbers. Of money. Clinical doctors as agents for others who call themselves a "doctor" yet are unfamiliar with the patient and unexposed while they make the call.
As I adjusted my headlamp before scrubbing, I thought about those new interns and residents on our wards upstairs, eager, willing, able. Bustling about, yearning to make a difference, waiting for their first chance...
... yet all being groomed to play the game.
-Wes
Fresh faces in neatly pressed white coats are in the halls. Eager. Enthusiastic. Clearly very bright. All hoping for a moment, an experience, an encounter that makes all their hard work worth it. Surely they'll have one, but not before the thousands of keyboard clicks, the mandatory lectures, rounds and lots of lengthy, lonely call nights.
He was a doctor from another time, well into his 80's. Lovely man with an infectious smile, mesmerizing foreign accent, and almost regal presence. An authority in his time and still attends lectures to stay engaged, a question passed his way from time to time out of respect for his experience and insights.
But he kept nearly falling at night and became concerned; even confused once. This was not like him. So he was admitted, observed and had a heart rhythm that was not normal. Blood thinners were started cautiously. Surely he could manage them. His wife, ever-present at his side, was equally engaging, concerned. And so, as fate would have it, after hundreds of thousands of keyboard clicks, I came to know them and realize his heart beat was too slow at times, dangerously so.
After lengthy discussions of the good and bad, the options, the data, he agreed a pacemaker made sense. Trustingly, he wanted it performed soon, eager to return to the lectures he loved. So the next morning after a night of worry, we assembled. His smile greeted me as I came to his bedside to obtain written consent, answer any last-minute questions, and silence the noise of concern. He was ready to go.
So I left his bedside to change into my scrubs, trying to hang my newly pressed shirt and tie to the side to preserve it for later behind a changing room curtain, when I heard a voice.
"Dr. Fisher, I'm so sorry..."
"What's up?"
"We can't bring your patient in the room."
"Why not?"
"We didn't know he's UnitedHealthCare. He's Medicare Part C!"
"Wha...?"
"You placed your order after 4PM, and we didn't see it until this morning. We have to get pre-approval from UnitedHealthCare for his pacemaker. They said it would be two or three hours..."
"Seriously?"
"Yes. It's his insurance. If you don''t get pre-approval, you won't get paid and he might have to pay for the procedure."
I stood, pants in hand, dumfounded. So I finished changing and exiting the changing area to clear my head. I called our administrator. She said, "Let me see what I can do. I'll call you right back." Within minutes a reply was sent: "You have to wait."
I thought of my frightened patient lying there vulnerable, so I went to his bedside to explain. He looked at me as a fellow physician, and he shook his head in disbelief, all the while naked beneath the covers. He agreed to wait - he had no choice. I left to get a cup of coffee and to collect my thoughts. What else could I do? I put a detailed note, an order, a consent order last night, and a pre-anesthetic note this morning. All keyed in, all according to protocol.
Then a nurse appeared with a note.
"If you call this number, hit "3" on the menu selection, and enter this case number, you can do a peer-to-peer."
"A what?"
"Peer-to-peer approval. You talk to a medical director and they might be able to expedite the approval for the pacemaker."
I looked for a moment at the "800" number, sighed, and called.
The woman who eventually answered after I heard "all attendants are busy" was pleasant enough, full of "good morning, doctor" and "what can I do for you." I explained the situation and wanted the ordering physician's name. I spelled my name to her. Keyboards were heard in the background.
"I see that his is for a CPT code 33208, correct?" She must have known that I knew my codes. But I knew that was wrong. He was not getting a dual chamber pacemaker, he just needed a single chamber, VVIR pacemaker.
"No, that's not correct. It should be 33207," I replied.
"Oh."
I heard more clicking.
"I'm sorry but I've tried to change that code under this case number and it seems I don't have authorization to do that. Can I put you on hold while I speak with the medical director to see if he can make the change?"
"Sure," I said. What choice did I have?
So I waited, listening to some nondescript melody in the background as I was placed on hold. A few minutes later, the same voice returned.
"Doctor?"
"Yes?"
"It seems the medical director couldn't change the information on this case number either, but I'm going to try to make a new number based on the CPT code you gave me, then I'll have the right information to give to the medical director, okay?"
So we proceeded to build a new case number. Lots of clicks interspersed with silence, then more clicks in the background, a few more statements like, "Sorry, I'm new to this" and "could you spell your name again," then finally:
"There. I think I've done it. Let me transfer you to our medical director...."
A click, some music, then a pleasant official-sounding woman's voice. "This is Doctor Frigamafrats. I'm sorry about the delay, I hope you didn't have to wait too long..."
A conversation ensued. I explained the rationale for the pacemaker, then finally was granted approval. Case number 2342343240 and approval number A321232451, or something like that. I notified the staff and handed the numbers to our clerk, knowing full well that pre-approval does not guarantee payment. Forty minutes rather than 120.
It's the game we play now. A new game. The Game of Numbers. Of money. Clinical doctors as agents for others who call themselves a "doctor" yet are unfamiliar with the patient and unexposed while they make the call.
As I adjusted my headlamp before scrubbing, I thought about those new interns and residents on our wards upstairs, eager, willing, able. Bustling about, yearning to make a difference, waiting for their first chance...
... yet all being groomed to play the game.
-Wes
Subscribe to:
Posts (Atom)