This morning the American Board of Medical Specialties' (ABMS) Maintenance of Certification (MOC) program debate reached a larger mainstream media audience when the Wall Street Journal published their article by Melissa Beck entitled "Skill Reviews Upset Doctors."
While it is certainly nice to see an article reaching the main stream media concerning doctors' concerns with the MOC program, the issue with the MOC debate is not that doctors are upset. The real issue is that doctors have been enslaved by special interests and crony capitalism to complete a MOC process that robs patients of more time with their doctors so that regulators and payers can enrich themselves.
One only has to see how certain aspects of the Wall Street Journal article were highlighted to see how Ms. Beck framed the debate toward business interests. For instance, she quoted Ms. Lois Nora, president of American Board of Medial Specialties who said:
"Many practicing physicians have not had formal courses in patient safety or quality improvment."
Ahem. I wonder if Ms. Beck or Ms. Nora have ever heard of the Hippocratic Oath? Doctors spend their entire careers (not to mention many sleepless nights) worrying about their patients' safety and care. Their livelihoods depend on it!
Yet there is never a moment of serious reflection regarding the sweeping hubris of Ms. Nora's statement. As spokesperson for the American Board of Medical Specialties, Ms. Nora suggests that without oversight, doctors are lax, uninterested in research or updating their techniques, inattendant to patient safety and unwilling to update their skills. Instead, the ABMS welcomes the tripling of patient volumes, the cameo roles that doctors are increasingly asked to play in patient care, the refocusing of one third to one half of every patient visit staring into an electronic medical record so the ABMS can watch for flinches in quality of care. The overseer who allowed this untenable health care scenario to transpire is effectively positioning themselves to patients that they are their last best hope.
Ms. Beck's piece also ignored the existing CME requirements that physicians already must perform each year to remain licensed and the value of such truly voluntary learning. Instead, Ms. Beck chose to highlight a quote from Richard Armstrong, MD - a board certified surgeon clearly without formal media training - who said: "No one wants to come out and say we're against quality, but most physicians find these modules to be cumbersome and, frankly, a joke."
When doctors are quoted calling any quality process "a joke," it really doesn't matter what the doctor actually said, for few will take him seriously. Let's be clear: the MOC process is not a joke, it's more like the twisted controlling strategy of the Hunger Games.
Ms. Beck also ignored that some MOC requirements now involve enrolling patients into study groups without their consent, doing the study and then reporting the data back to the boards. According to one doctor, "there are nearly 400 research projects being done on children through part 4 of the ABMS MOC program. Not only is performing research on children without consent immoral, it is costly in both time and money for the patient." Isn't this consideration important for patients?
Finally, Ms. Beck's article ends with the ABMS's claim that "500,000 of the more than 800,000 board-certified physicians have enrolled in MOC programs to date" implying that the majority of doctors support the program. Yet this statistic completely ignores the fact that doctors had no choice but to sign up for MOC despite their better judgement. As Ms. Beck hesitantly acknowledges in her article, this unproven physician metric is now increasingly tied to measures of physician "quality," hospital privileges, legal standing in court, and insurance panels. This unproven MOC program that was created by a self-appointed, private organization that is completely unaccountable to the public has also been indelibly etched into our new health care law.
No, it's better not to mention these unethical and extortionary tactics by the ABMS that threaten patient care.
Instead, it's far better to call doctors "upset."
-Wes
Showing posts with label media. Show all posts
Showing posts with label media. Show all posts
Tuesday, July 22, 2014
Wednesday, May 14, 2014
What's Wrong With This Picture?
A US medical conference opening plenary session:
A European medical conference opening plenary session:
Just sayin' -
-Wes
 |
| Heart Rhythm Society Meeting 2014 (Click to enlarge) From https://twitter.com/HugoOC/status/464204486576058368 |
A European medical conference opening plenary session:
 |
| NICE Annual Conference 2014 (Click to enlarge) From https://twitter.com/LockOn_Tweets/status/466514188521598976 |
-Wes
Wednesday, April 10, 2013
Being Schooled
An interesting phenomenon is occurring in media circles these days. No doubt others have seen it, too.
Lately, doctors are being schooled by the media.
From how to learn empathy, to improving communication with patients, the breadth and depth of what we should do for our patients is endless. Why, some even have our own colleague "experts" tell us how we should really do things.
These efforts, while probably well-intentioned, are patronizing. Do doctors tell journalists how to write or what to print?
Why are doctors seeing these main stream media efforts? Is it because most doctors are really incapable of the ability to listen and communicate with our patients? Is it because we must keep a stiff upper lip for what's coming in 2014? Or is this not-so-subliminal agenda of social engineering underway for some other reason?
It goes without saying that all of us should communicate better. (Think how many wars or family fights we could have avoided if we had, for instance.) And every doctor should turn their head away from computer screens and toward their patients, hold the patient's hands, look into their eyes, listen to their concerns, put ourselves in their place, do a thorough physical exam, have constant empathy and insight, read back medications, write out written instructions in 5th grade English, escort our patients back to the waiting room, or utilize highly skilled and educated assistants with all of these tasks, too. But the reality is this: time and ancillary resources are limited these days for doctors. Helpers cost money. Productivity must occur before new helpers are hired. More people than ever are entering health care thanks to intense marketing campaigns and new mandates for care. And there are so many doctors with only so many minutes in the day.
So doctors have to triage. Sickest first. We move as fast as we can to remain productive, because that's what's REALLY valued in healthcare these days. So is patient loyalty because that's what keeps them coming back. But in the process of growing loyalty, we increasingly have to document everything or other payers think it doesn't happen. So we type. And click. And type. And click. And print. To get paid. Talk about a communication and empathy buzz-kill!
Yet for those looking in, we must communicate better! "Listen to our "experts!" they proclaim.
Medicine was once considered a place where patients could confide in their doctors about their most intimate concerns and doctors had time to listen. Notes were one- or two-line jots in a chart. We'd spend the extra time because we were valued for our skills and for our knowledge and there was more to it than just pay. We had skin in the game. We got paid in chickens. We knew our patients. Back then, seven-minute appointments didn't exist. Now, doctors are cultivated as shift workers. Patients have Google. Everyone has information at their fingertips. Our new story line has become there are no limits to what patients can have in health care. Perfect data. Perfect health care access. Error-free health care with perfect delivery. Perfect communicating doctors. Always. We're building our medical Utopia.
But this effort to school doctors on our path to Nirvana has a serious downside for health care workers on the front lines.
As I've said before, there's a growing culture of hostile dependency that continues to grow toward doctors these days. The theme is like an adolescent who realizes his parents have feet of clay. He comes out of his childhood bubble and realizes his parents have failures and limitations because they are human beings. This results in the adolescent feeling unsafe, unprotected and vulnerable. Since this is not a pleasant feeling, narcissistic rage is triggered toward the people he needs and depends on the most. None of this occurs at a conscious level. Most of us understand this behavior simply as "adolescent rebellion," not understanding the powerful issues at play. So when we spotlight one side of what doctors should do for patients, be it improve communication or empathy (or whatever) without acknowledging the realities health care workers face like looming staffing shortages and pay cuts, we risk fanning the flames of narcissistic rage against the very caregivers whom we depend on the most - the very caregivers who are striving to communicate, do more with less, check boxes while still looking in the patient's eyes, meet productivity ratios, all while working in a highly litigious environment.
So be careful. Maybe we should school doctors less and value them more.
Who knows? Such a move might make things better for everyone in the long run.
-Wes
Lately, doctors are being schooled by the media.
From how to learn empathy, to improving communication with patients, the breadth and depth of what we should do for our patients is endless. Why, some even have our own colleague "experts" tell us how we should really do things.
These efforts, while probably well-intentioned, are patronizing. Do doctors tell journalists how to write or what to print?
Why are doctors seeing these main stream media efforts? Is it because most doctors are really incapable of the ability to listen and communicate with our patients? Is it because we must keep a stiff upper lip for what's coming in 2014? Or is this not-so-subliminal agenda of social engineering underway for some other reason?
It goes without saying that all of us should communicate better. (Think how many wars or family fights we could have avoided if we had, for instance.) And every doctor should turn their head away from computer screens and toward their patients, hold the patient's hands, look into their eyes, listen to their concerns, put ourselves in their place, do a thorough physical exam, have constant empathy and insight, read back medications, write out written instructions in 5th grade English, escort our patients back to the waiting room, or utilize highly skilled and educated assistants with all of these tasks, too. But the reality is this: time and ancillary resources are limited these days for doctors. Helpers cost money. Productivity must occur before new helpers are hired. More people than ever are entering health care thanks to intense marketing campaigns and new mandates for care. And there are so many doctors with only so many minutes in the day.
So doctors have to triage. Sickest first. We move as fast as we can to remain productive, because that's what's REALLY valued in healthcare these days. So is patient loyalty because that's what keeps them coming back. But in the process of growing loyalty, we increasingly have to document everything or other payers think it doesn't happen. So we type. And click. And type. And click. And print. To get paid. Talk about a communication and empathy buzz-kill!
Yet for those looking in, we must communicate better! "Listen to our "experts!" they proclaim.
Medicine was once considered a place where patients could confide in their doctors about their most intimate concerns and doctors had time to listen. Notes were one- or two-line jots in a chart. We'd spend the extra time because we were valued for our skills and for our knowledge and there was more to it than just pay. We had skin in the game. We got paid in chickens. We knew our patients. Back then, seven-minute appointments didn't exist. Now, doctors are cultivated as shift workers. Patients have Google. Everyone has information at their fingertips. Our new story line has become there are no limits to what patients can have in health care. Perfect data. Perfect health care access. Error-free health care with perfect delivery. Perfect communicating doctors. Always. We're building our medical Utopia.
But this effort to school doctors on our path to Nirvana has a serious downside for health care workers on the front lines.
As I've said before, there's a growing culture of hostile dependency that continues to grow toward doctors these days. The theme is like an adolescent who realizes his parents have feet of clay. He comes out of his childhood bubble and realizes his parents have failures and limitations because they are human beings. This results in the adolescent feeling unsafe, unprotected and vulnerable. Since this is not a pleasant feeling, narcissistic rage is triggered toward the people he needs and depends on the most. None of this occurs at a conscious level. Most of us understand this behavior simply as "adolescent rebellion," not understanding the powerful issues at play. So when we spotlight one side of what doctors should do for patients, be it improve communication or empathy (or whatever) without acknowledging the realities health care workers face like looming staffing shortages and pay cuts, we risk fanning the flames of narcissistic rage against the very caregivers whom we depend on the most - the very caregivers who are striving to communicate, do more with less, check boxes while still looking in the patient's eyes, meet productivity ratios, all while working in a highly litigious environment.
So be careful. Maybe we should school doctors less and value them more.
Who knows? Such a move might make things better for everyone in the long run.
-Wes
Friday, September 28, 2012
The Growing Culture of Hostile Dependency Toward Caregivers
Not long ago in this blog, I wrote about one of my colleague's tears as she hung up the phone after a bitter patient berated her for making a surgical schedule change. Tired and exhausted and still with consults and pacemaker checks to perform, she was returning a series of phone calls at the end of the day long after most people had already headed home. She tried to maintain control, but after that call, the damage was done.
I have seen this happening over and over again recently. The stress is palpable in our profession that cares for people's most prescious commodity, their health, while under extreme pressure to do more with less.
For businesses everywhere, the balance of costs with productivity to assure profit is nothing new. But in health care where people's lives are in the balance, the stress to health professional personnel is particularly palpable, especially now as huge transformative shifts are underway in how health care is being delivered in America.
So it was from this background that I struggled to understand why an exerpt from a heavily promoted book on patient safety appeared recently in the Wall Street Journal. Why should an article about five simple steps to "keep hospitals from killing us" bother me so? After all on the surface, it's such an important concept.
Perhaps I was bothered that "killing" was used in the byline when there are so many of us trying to prevent harm or do good for patients. Perhaps it was because some of the insinuations made in the book lacked a national perspective. Perhaps it was because some of the suggestions made were just more top-down Big Brother ideas that detract from actual patient care. Perhaps it was all of these. But after considerable reflection, I realized there was something else: a another overriding phenomenon that I was having a hard time putting my finger on.
I submitted the following letter to the Wall Street Journal Wednesday. They elected not to publish it. This really did not come as a surprise since it was quite critical of their coverage of the patient safety issue. But after showing the letter to a number of well-respected colleagues, they all encouraged me to publish it here. Hopefully it will make people think about the complicated psychology of what's happening on the front line of health care these days.
Holding the Wall Street Journal Accountable
Since when does a book promotion get a full page and a half of prime news print in one of the most respected business newspapers in the world? Usually a story that commands that much newsprint in the Wall Street Journal is written by one or more seasoned journalists to make sure all sides of the story are reported.
 |
| Full-page WSJ Story 21 Sep 2012 |
Doctor versus doctor: it just doesn't get any better for Main Stream Media.
But did anyone think to ask Dr. Makary if maybe the reason those older doctors don't use laparoscopic techniques is because they work at an inner city hospital with a limited budget without all the trappings of an academic medical center?
No. That would be reporting.
I am trying to understand the Wall Street Journal's motivation for their recent move. It is both puzzling and concerning. But at its core, it's probably quite simple to understand. I should probably follow the money. After all, we're all aware of the problems print media is having these days.
My bet is there's Big Business behind the Wall Street Journal's journalistic move.
And who's Bigger Business or Bigger Money than the insurance industry or the hospital industry? After all, medicine is the Biggest of Businesses in America.
Now before you go laughing at my conspiracy theory, ask yourself if there might be a problem with the perfectly even 98,000 number of deaths caused by medical errors touted by the Institute of Medicine in 1999 and highlighted in the Wall Street Journal's patient safety piece. Ask yourself why a professionally-produced book trailer promoting Dr, Makary's book that HAD to cost upwards of a quarter million dollars to produce winds its way on to the Internet. Ask yourself why no one would research the background of the players in that video and their motivations to appear in it. Was their motivation truly altruistic? Or in this era of the creation of Big Box medical care delivery, might there be another reason?
These days, the majority of today's American doctors are in the unenviable position of trying to be true patient advocates while promoting a Big Box medical model that has been foisted upon them and, for the majority of us, serves as our employer. The world loves idealists and none more so that Big Box Medical Center administrators and thought-leaders. Getting a physician
But is this new paradigm of journalistic reporting and wholesale promotion of one doctor's five ideas for patient safety without consequences? Can we afford perfect safety and all of the costs it entails while throwing our doctors under the documentation bus (or Big Brother camera) as they are asked to take incredible risks on behalf of their patients, be omnipresent, omni-available, impeccably skilled, omni-credentialed, omni-sympathetic all while seeing more patients in less time? Must we be made to believe, without reservation, that doctors (or any of the hundreds of people who work on each doctor's behalf) aren't human and subject to error?
I am seeing a culture of hostile dependency growing toward caregivers. The theme is like an adolescent who realizes his parents have feet of clay. He comes out of his childhood bubble and realizes his parents have failures and limitations because they are human beings. This results in the adolescent feeling unsafe, unprotected and vulnerable. Since this is not a pleasant feeling, narcissistic rage is triggered toward the people he needs and depends on the most. None of this occurs at a conscious level. Most of us understand this behavior simply as "adolescent rebellion," not understanding the powerful issues at play. So when we spotlight one side of the patient safety story without acknowledging the realities health care workers face like looming staffing shortages and pay cuts, we risk fanning the flames of narcissistic rage against the very caregivers whom we depend on the most - the very caregivers who are striving to do more with less, check boxes while still looking in the patient's eyes, meet productivity ratios, all while working in a highly litigious environment. Why would we do this and why would we allocated money as Dr. Makary suggests, for punitive top-down solutions instead of spending that same money on supporting and educating our frontline providers?
A good journalist would investigate all sides of the story and understand its impact. A one-sided full-page book promotion by a non-journalist in the well-respected Wall Street Journal that reduces the serious patient safety issues in today's Big Box medical organizations to "5 simple steps" is nothing more than a cheap shot at the majority of doctors who choose to carefully and tirelessly treat their patients as safely as they can without basking in the glow of Main Stream Media.
-Wes
Tuesday, January 03, 2012
Tough Guy Does CPR Hard and Fast
While it might not be quite as funny as the Portugese Cardiology Foundation's Big Belly People video which takes a stab at the obesity epidemic, the British Heart Foundation does a pretty good job getting the "hard and fast" message out for "hands-only CPR" using British tough-guy Vinnie Jones in its new TV ad:
Heh.
-Wes
Heh.
-Wes
Tuesday, December 13, 2011
Be Wary of Press Releases
Why we need to be wary of press releases, especially when they contain so-called "scientific" content that "pushes the envelope," courtesy of Conan O'Brien:
-Wes
h/t: my brother-in-law on Facebook.
-Wes
h/t: my brother-in-law on Facebook.
Monday, October 24, 2011
Big-Time Medical Blogging
First, there was O Magazine, now Reader's Digest (next to Hugh Laurie, no less):

Yes, Virginia, it's medical blogging at its best!
(Thanks to my patient who clipped this for me!)
:)
-Wes
Yes, Virginia, it's medical blogging at its best!
(Thanks to my patient who clipped this for me!)
:)
-Wes
Saturday, April 02, 2011
On Yesterday's Blog Post
... and the deconstruction of the 23-blog April Fool's Day conspiracy.
It was lot's of fun and had two over-arching lessons from my standpoint:
(1) Be critical of what you read: not all news that fit to print is fit to read, and
(2) it really is possible for lawyers and doctors to work together.
-Wes
It was lot's of fun and had two over-arching lessons from my standpoint:
(1) Be critical of what you read: not all news that fit to print is fit to read, and
(2) it really is possible for lawyers and doctors to work together.
-Wes
Friday, April 01, 2011
Orson Welles: Meet the New York Times
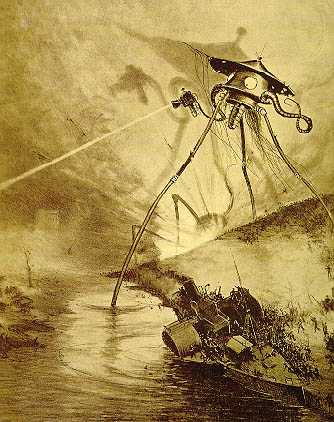
The news grows more frequent and increasingly ominous as a cylindrical meteorite lands in Grover's Mill, New Jersey. A crowd gathers at the site and events are related by reporter Carl Phillips. The meteorite unscrews, revealing itself as a rocket machine, and onlookers catch a glimpse of a tentacled, pulsating, barely mobile Martian before it incinerates the crowd with Heat-Rays. Phillips' shouts about incoming flames are cut off in mid-sentence. (Later surveys indicate that many listeners heard only this portion of the show before contacting neighbors or family to enquire about the broadcast. Many contacted others in turn, leading to rumors and confusion.)
This 1938 coupe was a classic example of how mainstream media can manipulate their audience. As we all know, these examples continue today and should serve as a powerful reminder to medical students, residents, doctors, nurses and ancillary health professionals how all sorts of instantaneously-available information, be it health care information or otherwise, can be shaped, manipulated, processed and pureed.
Want an example?
How about this: once again, the mainstream media's darling, The New York Times, gets punked.
-Wes
Friday, February 25, 2011
Doctor-Bashing Headlines
While I know it grabs the eye, it really didn't matter what the article was about:

... the headline says it all: doctors are the problem, not the system, right?
-Wes

Click image to enlarge
... the headline says it all: doctors are the problem, not the system, right?
-Wes
Monday, October 04, 2010
Uh-"O"
... Saw a little tidbit, courtesy Sitemeter: it seems this blog was mentioned in "O" magazine as a "Four Doctor Blogs to Read Now", along with surgeon Jeffrey Parks, MD of Buckeye Surgeon, Lucy E. Hornstein, MD from Musings of a Dinosaur, and Kimberly D. Manning, MD of GradyDoctor.com.
Man, and I haven't even put up a post today...
Ouch!
(Welcome to all three of my new readers! Hope my sidebar samplings will do for now.)
-Wes
Man, and I haven't even put up a post today...
Ouch!
(Welcome to all three of my new readers! Hope my sidebar samplings will do for now.)
-Wes
Tuesday, August 24, 2010
The 10 Most Powerful People In Health Care
In case you haven't seen it, the media's list of the 100 Most Powerful People in Health Care was published yesterday. In thinking about this list I realized that in reality, these people had little to do with my patients' health care delivery. So how did they became the most powerful people in health care? Quite simply, they are not the 100 most powerful people in health care, but rather they are the 100 most powerful people overseeing the funding of health care - at least for the moment. In as little as 11 months, many of the people on this list will be gone or have moved on to their next money-making venture.
So who are the most powerful people in health care?
Well, I'd like to propose my list - maybe not of a 100 people (frankly, nothing gets done if you have a committee of 100 people anyway) - but rather my own list of the Top 10 Most Powerful People in Your Health Care today:
So who are the most powerful people in health care?
Well, I'd like to propose my list - maybe not of a 100 people (frankly, nothing gets done if you have a committee of 100 people anyway) - but rather my own list of the Top 10 Most Powerful People in Your Health Care today:
10. The Doctor - They consider the differential, write the orders, follow-up on tests, and move the health care ball forward throughout your hospitalization or stay with a rehab facility. As such, they should be given their power due, even if many other members of the health care team are actually are the ones that make sure the care happens. Still, because the doctor gets most of the liability risk if things don't happen or happen incorrectly, they just make my power list.-Wes
9. The Food Service Personnel - These folks are powerful. They have the ability to make even a clear liquid diet look like real food - especially when they mix the colors and flavors of jello. Further, proper parenteral nutrition for an ICD patient greatly shortens the sickest patient's hospitalization. Get it right and everyone benefits. Power personified.
8. The Physical Therapist - If you can't eat your food, sit up, keep your muscles toned, maintain the range of motion of your limbs when sick, the chances of returning to independent living are limited. Physical therapist have come of the most helpful techniques to get going - both physically and mentally - like turkey bowling. Their power over our patients should definitely be appreciated more.
7. The Social Worker - Want to negotiate the complex Medicare and Medicaid rules for placement in an assisted living facility? Need to get a patient to rehab? Want to arrange transportation for a patient that doesn't have a penny to their name? Make something from absolutely nothing? Call the Social Worker - but call them early in the hospital stay. (They're never at their best with last-minute consults.)
6. The Nursing Supervisor - Trust me on this. No one has more power to assure adequate staffing on each patient care ward each day than the Nursing Supervisor. Medical students and residents that cross the directives issued by this individual do so at their own peril.
5. The Bed Coordinator - If you need to admit a patient to a hospital, they must first get a bed. With many hospitals working at or near capacity, no single person has more influence over the patients admitted to a hospital facility. They find beds when no one else can. After all, it's their job.
4. The Hospital Operator - Name one person who can activate a Code Blue (cardiac arrest), find the obscure specialist in the middle of the night when they're most needed, or mobilize a trauma team faster. Can't do it? That, my friends, is power.
3. The Night Shift Nurse - At three in the morning when you're lying there in the hospital bed and need something - anything - who's the most important person in the hospital who will assure you're needs are tended to? Need I say more? If the night shift nurse is inattentive, unresponsive, irresponsible for that 8-hour shift - you're screwed. On the other hand, if she's attentive, knows when to call for help, or provides pain relief when you need it most after surgery, or - most important - gives you that laxative at 3AM - his or her power in medicine pales in comparison to any bureaucrat, politician, or hospital system CEO.
2. The Patient's Family - Often forgotten, family members have huge influence over the care provided to their loved one - especially at times where their loved one might not be able to communicate. This power should not be ignored, but it cuts both ways, too. While family members can facilitate the treatment and rehabilitation of their loved one because they know them better than anyone else, they can also prolong undue suffering if they do not comprehend the limits of care that their loved one desires in the end-of-life setting. Families that communicate their needs and wishes before anyone gets sick avoid much of the confusion during this difficult time and serve as powerful allies to the health care team.
1. You, The Patient - No one has more influence and power over their care than you. Don't want care? Leave. No one can stop you. Want care and don't have a penny? Come to the Emergency Room. You won't be turned away. Wonder what all the big buildings, waterfalls, and fancy technology were built and bought for? You. Every single person involved in health care is there because of you. So make the most of it. Come prepared. Know your medical history, medicines and allergies. If you can't remember, keep a list with you. Ask questions. Insist on clear answers. Work with your care givers, don't fight them. If you're not sure, get a second opinion. Write a letter acknowledging those that made the extra effort and scolding those that didn't. Your constructive criticism makes the system better. And know that hospitals understand the importance of your word-of-mouth referral - it's the most powerful marketing strategy a health care system can generate. Finally, remember that you can vote for politicians that don't forget who's in charge. You are the ultimate power broker in health care. Don't forget it.
Wednesday, March 03, 2010
Coffee and the Heart - Good or Bad?
This week, it seems to be good:
But a quick Google search on Dr. Klatsky's earlier studies using the same questionaire database shows the problems with using questionaire data to make such sweeping conclusions. Take, for instance, these findings from 1973:
What they say is:
-Wes
h/t: The Happy Hospitalist for the story idea.
“People who are moderate coffee drinkers can be reassured that they are not doing harm because of their coffee drinking,” said Arthur Klatsky, the study’s lead investigator and a cardiologist at Kaiser’s Division of Research.These "surprising" data are to be presented at the AHA meeting March 5th. (You'll have to wait until then to get the REAL scoop, it seems.)
But a quick Google search on Dr. Klatsky's earlier studies using the same questionaire database shows the problems with using questionaire data to make such sweeping conclusions. Take, for instance, these findings from 1973:
"Coffee drinking is not an established risk factor for myocardial infarction."And yet a bit later, in 1990, there's a flip flop:
Because of conflicting evidence about the relation of coffee use to coronary artery disease, the authors conducted a new cohort study of hospitalizations among 101,774 white persons and black persons admitted to Kaiser Permanente hospitals in northern California in 1978–1986. In analyses controlled for eight covariates, use of coffee was associated with higher risk of myocardial infarction (p=0.0002). (By the way, British researchers failed to find a similar correlation in instant coffee drinkers)So what, really, do these data from the Kaiser questionaire data regarding heavy coffee consumption and the heart say?
What they say is:
- Questionaire data crunched to suggest correlations are insufficient to mean causation, irrespective of how the media parses it.
- Questionaire data are subject to significant sampling and reporting biases.
- Rehashing the same old questionaires using the same samples with newer data can dramatically alter prior findings.
- Researchers are getting paid way too much to keep rehashing the same data for large health systems.
- On the lighter side, college undergrads and medical students should note that they could use these types of questionaire data to justify significant caffeine consumption along with alcohol to protect themselves from developing cirrhosis.
-Wes
h/t: The Happy Hospitalist for the story idea.
Sunday, February 07, 2010
How Technology Is Straining the Doctor-Patient Relationship
Technology is an incredible thing.
Technology is expensive.
Technology saves lives.
Technology can bankrupt.
When there's no technology, are you a "bad" doctor for not following guidelines?
When technology's used, are you a "bad" doctor because the patient has multiple comorbidities and the benefit for the implanted technology is questionable?
It's become the yin and yang of medicine. An inconvenient truth.
Medicine's technology is incredibly expensive, but incredibly valuable.
But if the struggle isn't enough, along comes the press to skew the debate by "raising awareness" with our patients.
Doctor, you need to "Get with the Guidelines." The subtitle with such an industry-sponsored trial and press report should be, "Oh, and business is off."
The journal article at the heart of the Chicago Tribune piece (referenced below) suggests the underpenetrated market of defibrillators (ICDs) was partially caused by three factors:
We must also place a jaded eye at the manufacturer's earlier press release about this trial that 35,000 charts had been reviewed, rather than less than half of that (15,381). Small error? Not so much.
Medicine is a complicated, non-linear profession. But as patients continue to shoulder more of their health care bills, doctors are finding themselves in the increasingly difficult position of recommending very expensive life-saving technology that might bankrupt their patients. Unless industry acknowledges that very real price pressures are straining this doctor-patient relationship, there will remain a reluctance to completely "Get With the Guidelines" and implant the technology, even when doing so stands to benefit the doctor.
-Wes
Ref: Evidence of clinical practice heterogeneity in the use of implantable cardioverter-defibrillators in heart failure and post–myocardial infarction left ventricular dysfunction: Findings from IMPROVE HF. HeartRhythm Dec 2009, 6(12), Pp 1727-1734.
Technology is expensive.
Technology saves lives.
Technology can bankrupt.
When there's no technology, are you a "bad" doctor for not following guidelines?
When technology's used, are you a "bad" doctor because the patient has multiple comorbidities and the benefit for the implanted technology is questionable?
It's become the yin and yang of medicine. An inconvenient truth.
Medicine's technology is incredibly expensive, but incredibly valuable.
But if the struggle isn't enough, along comes the press to skew the debate by "raising awareness" with our patients.
Doctor, you need to "Get with the Guidelines." The subtitle with such an industry-sponsored trial and press report should be, "Oh, and business is off."
The journal article at the heart of the Chicago Tribune piece (referenced below) suggests the underpenetrated market of defibrillators (ICDs) was partially caused by three factors:
Adjusted analyses revealed lack of adherence for ICD use most notably with advancing age (odds ratio: 0.87; 95% confidence interval: 0.82 to 0.93 per 10 years), black race (odds ratio: 0.75; 95% confidence interval: 0.60 to 0.94), and lack of insurance (odds ratio: 0.45; 95% confidence interval: 0.26 to 0.78).But other factors exist, they claim, like geography and available expertise:
Practices in the Northeast U.S. were more likely to adhere to guidelines (P <.001), as were those with a dedicated HF clinic (P = .004) and electrophysiologists on staff (P <.001).These data are indeed valuable, even for an industry-sponsored trial. But patients should be aware that six of these devices must be implanted to save one life in properly selected populations of patients. Not to say that the cost-effectiveness of this approach hasn't been extensively reviewed, it has. But referring doctors and patients have also been barraged with the problems with these technologies. No doubt the chart reviews in the study cited probably didn't account for the rash of recalls whose influence continues today.
We must also place a jaded eye at the manufacturer's earlier press release about this trial that 35,000 charts had been reviewed, rather than less than half of that (15,381). Small error? Not so much.
Medicine is a complicated, non-linear profession. But as patients continue to shoulder more of their health care bills, doctors are finding themselves in the increasingly difficult position of recommending very expensive life-saving technology that might bankrupt their patients. Unless industry acknowledges that very real price pressures are straining this doctor-patient relationship, there will remain a reluctance to completely "Get With the Guidelines" and implant the technology, even when doing so stands to benefit the doctor.
-Wes
Ref: Evidence of clinical practice heterogeneity in the use of implantable cardioverter-defibrillators in heart failure and post–myocardial infarction left ventricular dysfunction: Findings from IMPROVE HF. HeartRhythm Dec 2009, 6(12), Pp 1727-1734.
Wednesday, December 16, 2009
Scientific Medical Journals and the Media
The article appeared yesterday in the Wall Street Journal: "Study Shows Older Patients Benefiting From Defibrillators."
One would think a doctor might like to read the article, especially one dealing with defibrillators.
So I checked late last night and wouldn't you know, no such article was on-line. Then I checked again early this morning. Still no reference on line. I checked Google. I checked Circulation: Heart Failure's website. I checked for the press release on the American Heart Association's press release web page.
No such article.
But Reuters had seen it (I think) (or at least they saw the American Heart Association's press release about the article, I really don't know).
And so I waited and waited, only to find that the article was finally posted on-line publically on the Circulation: Heart Failure's website at about 12-1PM CST, almost a full 18 hours later the manuscript was reported upon by the main stream media.
The article certainly has plenty to comment upon, but I will forgo that for the moment and instead focus on this disturbing trend of media releases pitched to journalists before the scientific community.
Given that this study was funded by GlaxoSmith Kline and the journal Circulation: Heart Failure is published by the American Heart Association who acknowledges multimillion dollar funding from the pharmaceutical and medical device companies we have to wonder: why are physicians being left out of the opportunity to critically review scientific publications before mainstream media broadcasts information to our patients and the public? Might it be that the sponsors of these trials might not like what certain doctors might say about the study? Or are such press releases being more like classic TV ads hoping to prod patient's to "Ask Your Doctor" about study's findings? What potential implications might these press releases have on public policy mandating doctors to "Get With the Guidelines" for the treatment of heart failure going forward?
I find the feeding of jounalists these manuscripts before the very scientists who subscribe to the these journals troubling at best and potentially subversive and manipulative at worst.
-Wes
One would think a doctor might like to read the article, especially one dealing with defibrillators.
So I checked late last night and wouldn't you know, no such article was on-line. Then I checked again early this morning. Still no reference on line. I checked Google. I checked Circulation: Heart Failure's website. I checked for the press release on the American Heart Association's press release web page.
No such article.
But Reuters had seen it (I think) (or at least they saw the American Heart Association's press release about the article, I really don't know).
And so I waited and waited, only to find that the article was finally posted on-line publically on the Circulation: Heart Failure's website at about 12-1PM CST, almost a full 18 hours later the manuscript was reported upon by the main stream media.
The article certainly has plenty to comment upon, but I will forgo that for the moment and instead focus on this disturbing trend of media releases pitched to journalists before the scientific community.
Given that this study was funded by GlaxoSmith Kline and the journal Circulation: Heart Failure is published by the American Heart Association who acknowledges multimillion dollar funding from the pharmaceutical and medical device companies we have to wonder: why are physicians being left out of the opportunity to critically review scientific publications before mainstream media broadcasts information to our patients and the public? Might it be that the sponsors of these trials might not like what certain doctors might say about the study? Or are such press releases being more like classic TV ads hoping to prod patient's to "Ask Your Doctor" about study's findings? What potential implications might these press releases have on public policy mandating doctors to "Get With the Guidelines" for the treatment of heart failure going forward?
I find the feeding of jounalists these manuscripts before the very scientists who subscribe to the these journals troubling at best and potentially subversive and manipulative at worst.
-Wes
Friday, October 16, 2009
In Case You Were Wondering
... Kim has a nice run-down on what I've been up to over at Emergiblog. Yesterday's conference on medical blogging and the impact that social media will play in the future direction of health care was fascinating and well worth the trip. Issues discussed were far-reaching, including the legal issues facing physician and nurse bloggers, what new media means to hospital and the medical device/pharmaceutical industries, and the impact/influence medical bloggers can have upon mainstream media and patient communication.
Everyone had a great time and I would encourage anyone out there with an interest in this venue to join us next year!
-Wes
Everyone had a great time and I would encourage anyone out there with an interest in this venue to join us next year!
-Wes
Thursday, March 05, 2009
Socialism's Scientific Method
Thank God journalists in the United States can spew forth opinion in the name of self-righteousness and indignation free from interference from faceless bureaucrats. If bureaucrats were in charge, they might require that journalists make generalizations about a profession they know nothing about to push their socialist-leaning agenda in the name of readership. Oh wait, they are. I am so relieved that journalists can still breathlessly demonstrate why doctors hate science after never spending a day at a patient’s bedside.
Welcome to socialism’s scientific method.
Doctors, you see, make more money than journalists. Therefore, they are inherently evil since everything they do is about money.
Seriously.
For example, doctors use expensive hypertensive agents because all patients can be treated with simpler, much less expensive agents that have been “definitely shown” to be more effective. Why? Because they are easily corruptible by evil pharmaceutical and device companies that have added nothing to our pharmaceutical or therapeutic armamentarium in the last ten years.
And doctors get MRI’s in patients with back pain when cheaper CT scans are just as effective because… well, I’m not sure, but I know there’s a reason. Oh, I know, to make money! (What’s that you say? The hospital owns the machine and the doctor doesn’t get paid the technical fee that covers the cost of the MRI – oh, come on now, don’t bore me with the details!)
It’s hard not to scream when journalists make such sweeping generalizations about doctors without any attempt at identifying the potential problems inherent to surrendering individualized care to a central governmental Politburo in the name of the “efficiencies and cost savings” of comparative effectiveness research. After all, what's $1.1 billion when we're talking trillions in government bailout?
But where has this $1.1 billion in your tax dollars already gone? Well, much of it has gone to the very “efficient” and “non-biased” bureaucratic Agency for Healthcare Research and Quality (AHRQ) or the National Insitute of Health. Please recall that it was the AHRQ that helped fund the “non-biased” research that advocated for adding cardiac resynchronization therapy (CRT) to hospital guidelines for the treatment of heart failure with barely acknowledging the investigators’ and the American Heart Association's deep ties to the device industry. (Hey, it was a sound scientific study based on chart reviews!) And of course, we can still thank the NIH for their bloated and hightly efficient National Center of Comparative and Alternative Medicine! Where would we be without their ongoing work on echinacea that showed it was worthless for the common cold? I feel relieved (don't you?) that because some critized their study that the echinacea dose was "too low" that they still accept proposals for continued work in this area!
And when the journalist needs a pacemaker, what does she say?
"You're not going to give me one of those old, recalled ones, are you? I want the best!"
Thank God the government and their left-leaning journalistic sycophants can provide us with all the answers. Certainly, us “doctor-scaremongers” and our patients have nothing to fear now that they’re in charge.
-Wes
Addendum: Also republished at MedPageToday. (Additional commentary there).
Welcome to socialism’s scientific method.
Doctors, you see, make more money than journalists. Therefore, they are inherently evil since everything they do is about money.
Seriously.
For example, doctors use expensive hypertensive agents because all patients can be treated with simpler, much less expensive agents that have been “definitely shown” to be more effective. Why? Because they are easily corruptible by evil pharmaceutical and device companies that have added nothing to our pharmaceutical or therapeutic armamentarium in the last ten years.
And doctors get MRI’s in patients with back pain when cheaper CT scans are just as effective because… well, I’m not sure, but I know there’s a reason. Oh, I know, to make money! (What’s that you say? The hospital owns the machine and the doctor doesn’t get paid the technical fee that covers the cost of the MRI – oh, come on now, don’t bore me with the details!)
It’s hard not to scream when journalists make such sweeping generalizations about doctors without any attempt at identifying the potential problems inherent to surrendering individualized care to a central governmental Politburo in the name of the “efficiencies and cost savings” of comparative effectiveness research. After all, what's $1.1 billion when we're talking trillions in government bailout?
But where has this $1.1 billion in your tax dollars already gone? Well, much of it has gone to the very “efficient” and “non-biased” bureaucratic Agency for Healthcare Research and Quality (AHRQ) or the National Insitute of Health. Please recall that it was the AHRQ that helped fund the “non-biased” research that advocated for adding cardiac resynchronization therapy (CRT) to hospital guidelines for the treatment of heart failure with barely acknowledging the investigators’ and the American Heart Association's deep ties to the device industry. (Hey, it was a sound scientific study based on chart reviews!) And of course, we can still thank the NIH for their bloated and hightly efficient National Center of Comparative and Alternative Medicine! Where would we be without their ongoing work on echinacea that showed it was worthless for the common cold? I feel relieved (don't you?) that because some critized their study that the echinacea dose was "too low" that they still accept proposals for continued work in this area!
And when the journalist needs a pacemaker, what does she say?
"You're not going to give me one of those old, recalled ones, are you? I want the best!"
Thank God the government and their left-leaning journalistic sycophants can provide us with all the answers. Certainly, us “doctor-scaremongers” and our patients have nothing to fear now that they’re in charge.
-Wes
Addendum: Also republished at MedPageToday. (Additional commentary there).
Sunday, February 22, 2009
Sunday, January 25, 2009
How to Scare a Reporter
Just show him an angioplasty with a little Bezold-Jarisch reflex and a brief bout of ventricular fibrillation then watch him bail into the control room.
Heh.
-Wes
PS: Note the size of the clot they aspirated from the artery. (Yes, Mr. President, it doesn't take much to bring a young smoker to his knees.)
Heh.
-Wes
PS: Note the size of the clot they aspirated from the artery. (Yes, Mr. President, it doesn't take much to bring a young smoker to his knees.)
Wednesday, August 06, 2008
You'd Better Not Watch the Olympics
... because the media thinks, just like the Super Bowl and World Cup Soccer, doing so might just kill you.
If anyone would like a defibrillator for primary prevention of sudden death... (heh)
... really, why do they print these stories?
-Wes
If anyone would like a defibrillator for primary prevention of sudden death... (heh)
... really, why do they print these stories?
-Wes
Subscribe to:
Comments (Atom)