A truly remarkable video demonstrating a lightning fast robotic hand with incredible implications for the disabled:
-Wes
h/t: Boingboing.net
Monday, August 31, 2009
Doctors: The Electronic Log Jam
With the increasing push for medical records to go electronic, I continue to be amazed at the ability and speed that information gets pushed my way.
I have already mentioned the multiple servers that we must interact with daily, and today learned that soon our pacemaker checks will soon become "paperless," permitting me the ability to log on to yet another server so I can sign my pacemaker checks electronically! Whooo Hooo!
Not that this is bad, mind you. I think it's great that all of this information will eventually be added on-line for all to see. There is no doubt that communication will be improved.
But despite the gleeful enthusiasm of the information technology gurus, I find that I am increasingly becoming the log jam that prevents the information from flowing to the electronic medical record. As more and more results and reports require the electronic signature, it is becoming increasingly difficult for some of us who do not spend the day at the computer screen to promptly sign our results and move them to the chart. The IT specialists and administrators realize that someone has to take the fall if there is a problem amongst all those results, so all of them pass before the doctor. But few of these technology people realize how long it takes to scroll down to find the results of a test that appears below a tiny pop-up window or the time it takes to decompress a pdf file on each test result reported. Multiply those times by hundreds of results or reports a day and it's no wonder doctors remain skepical of a computer's ability to save us time. The more tests and electronic signature requirements must pass beneath my typing fingers, there is a limit as to how fast it can find its way to the patient's chart.
Of course the IT specialists are all to happy to point out that you can highlight all of the results at once and click "Sign-'Em-All" and, presto, they're on the chart. But doesn't that defeat the purpose of checking and reviewing the results? Sadly, I fear that human nature will do just that as doctors look for ways to relieve the log jam that appears in their result inbasket each day.
But then again, since the computer will get its "signature" with the click of a button, we'll have 100% compliance with reviewing all our test results results, won't we?
-Wes
I have already mentioned the multiple servers that we must interact with daily, and today learned that soon our pacemaker checks will soon become "paperless," permitting me the ability to log on to yet another server so I can sign my pacemaker checks electronically! Whooo Hooo!
Not that this is bad, mind you. I think it's great that all of this information will eventually be added on-line for all to see. There is no doubt that communication will be improved.
But despite the gleeful enthusiasm of the information technology gurus, I find that I am increasingly becoming the log jam that prevents the information from flowing to the electronic medical record. As more and more results and reports require the electronic signature, it is becoming increasingly difficult for some of us who do not spend the day at the computer screen to promptly sign our results and move them to the chart. The IT specialists and administrators realize that someone has to take the fall if there is a problem amongst all those results, so all of them pass before the doctor. But few of these technology people realize how long it takes to scroll down to find the results of a test that appears below a tiny pop-up window or the time it takes to decompress a pdf file on each test result reported. Multiply those times by hundreds of results or reports a day and it's no wonder doctors remain skepical of a computer's ability to save us time. The more tests and electronic signature requirements must pass beneath my typing fingers, there is a limit as to how fast it can find its way to the patient's chart.
Of course the IT specialists are all to happy to point out that you can highlight all of the results at once and click "Sign-'Em-All" and, presto, they're on the chart. But doesn't that defeat the purpose of checking and reviewing the results? Sadly, I fear that human nature will do just that as doctors look for ways to relieve the log jam that appears in their result inbasket each day.
But then again, since the computer will get its "signature" with the click of a button, we'll have 100% compliance with reviewing all our test results results, won't we?
-Wes
Friday, August 28, 2009
Saving Money: B.Y.O.P.
* bleeeeep bleeeeep bleeeeep *
It was 11:57PM on the alarm clock last night. I peeled my head from the pillow and felt my heart racing from the adrenaline surge that usurped by Stage IV REM sleep. I fumbled for the pacer and pressed the button. Glorious silence ensued as I caught my breath. Reading the pager, I noticed it was the nurse caring for my patient calling. I dialed the phone.
"This is Doctor Fisher. I'm returning Sally's call (not her real name)."
"Just a moment."
Some cheesy commercial played in the background with some canned music that I had heard a thousand times before. 'Damn, why don't they just play some soft classical music?' I thought to myself. Just then, a voice answered.
"This is Sally..."
"Sally, Dr. Fisher, returning your call..."
"Yes, Mr. Faachamatacheesedip is having trouble sleeping. Can he have a sleeping pill?"
My heart raced again, but I kept my composure and acquiesced. Sure." Then I prescribed a sleeping pill as requested and the nice nurse thanked me and I was back to lying an bed, staring at the ceiling, thinking about ways to cut health care costs. I do that sometimes. Especially when I've been awakened for a sleeping pill.
Every day, countless times across the country, thousands of doctors prescribe tylenol and sleeping pills and countless other "preventative" medications just so they don't get these calls at night. I wondered how many millions of dollars could be saved, but realized with the savings comes a price: the need to make another call to the doctor. Would this really save money? Hard to tell. Would doctors sleep worse? Probably.
Better still, what if we allowed patients to take their own chronic medications that they have been using for years when they have already paid for when they come in the hospital for routine procedures? These medications could be registered on the patient's electronic medical record and designated as "self-adminstered" to assure that the nurses and doctors caring for the patient knew which medications they were actively taking during their medication reconcilation process performed when they enter the hospital.
But alas, the hospital would lose money. "Patient safety might be compromised," they'll say!
But I say, maybe some simple ideas like this could save real money in the long run for our over-priced health care system. Call it "B.Y.O.P.:" Bring Your Own Pills.
And then maybe, just maybe, our system could save some real money, bit by bit. And patients could take their OWN sleeping pills so the doctor could get another wink of sleep each night.
-Wes
It was 11:57PM on the alarm clock last night. I peeled my head from the pillow and felt my heart racing from the adrenaline surge that usurped by Stage IV REM sleep. I fumbled for the pacer and pressed the button. Glorious silence ensued as I caught my breath. Reading the pager, I noticed it was the nurse caring for my patient calling. I dialed the phone.
"This is Doctor Fisher. I'm returning Sally's call (not her real name)."
"Just a moment."
Some cheesy commercial played in the background with some canned music that I had heard a thousand times before. 'Damn, why don't they just play some soft classical music?' I thought to myself. Just then, a voice answered.
"This is Sally..."
"Sally, Dr. Fisher, returning your call..."
"Yes, Mr. Faachamatacheesedip is having trouble sleeping. Can he have a sleeping pill?"
My heart raced again, but I kept my composure and acquiesced. Sure." Then I prescribed a sleeping pill as requested and the nice nurse thanked me and I was back to lying an bed, staring at the ceiling, thinking about ways to cut health care costs. I do that sometimes. Especially when I've been awakened for a sleeping pill.
Every day, countless times across the country, thousands of doctors prescribe tylenol and sleeping pills and countless other "preventative" medications just so they don't get these calls at night. I wondered how many millions of dollars could be saved, but realized with the savings comes a price: the need to make another call to the doctor. Would this really save money? Hard to tell. Would doctors sleep worse? Probably.
Better still, what if we allowed patients to take their own chronic medications that they have been using for years when they have already paid for when they come in the hospital for routine procedures? These medications could be registered on the patient's electronic medical record and designated as "self-adminstered" to assure that the nurses and doctors caring for the patient knew which medications they were actively taking during their medication reconcilation process performed when they enter the hospital.
But alas, the hospital would lose money. "Patient safety might be compromised," they'll say!
But I say, maybe some simple ideas like this could save real money in the long run for our over-priced health care system. Call it "B.Y.O.P.:" Bring Your Own Pills.
And then maybe, just maybe, our system could save some real money, bit by bit. And patients could take their OWN sleeping pills so the doctor could get another wink of sleep each night.
-Wes
Wednesday, August 26, 2009
EKG Du Jour #18 - The Fax
The 47 year-old patient had suffered a cardiac arrest months ago, had a prolonged hospital stay and recovery, and was now being referred for consideration for implantation of a cardiac defibrillator. The doctor faxed ahead this patient's EKG, which arrived distorted and skewed:
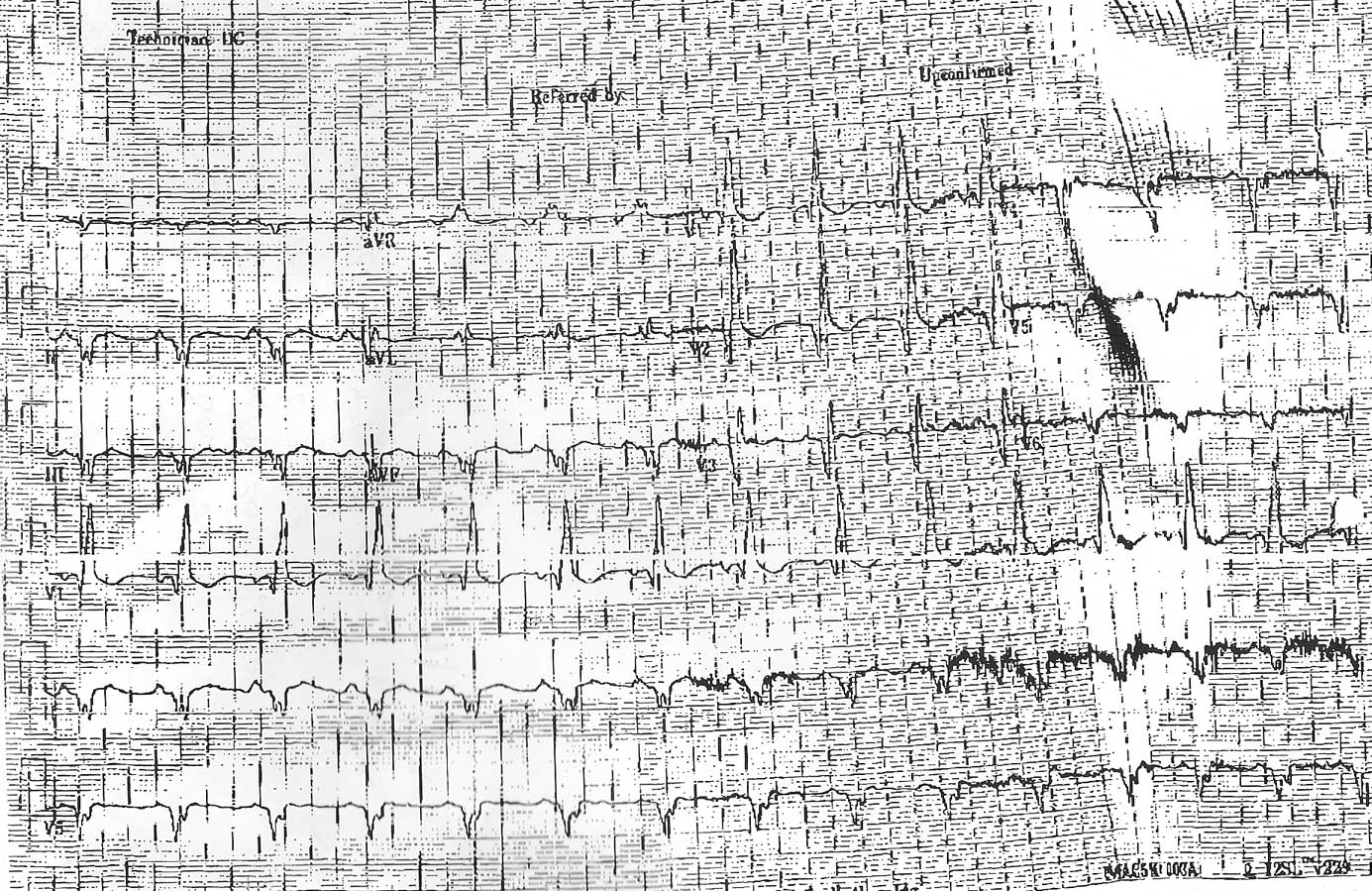
Your mission, should you decide to accept it my dear EKG aficionados, is to describe the findings as best you can. Because the patient has not yet arrived in your clinic and the referring doctor did not have access to an echocardiogram machine (theirs was broken), you must also estimate this patient's left ventricular ejection fraction based on this EKG alone. (Guesses are okay).
Good luck.
-Wes
Click image to enlarge
Your mission, should you decide to accept it my dear EKG aficionados, is to describe the findings as best you can. Because the patient has not yet arrived in your clinic and the referring doctor did not have access to an echocardiogram machine (theirs was broken), you must also estimate this patient's left ventricular ejection fraction based on this EKG alone. (Guesses are okay).
Good luck.
-Wes
A Heart Icon is Gone

Sad. Call it the largest broken heart ever. The old walk-through heart at the Museum of Science and Industry here in Chicago is gone:
The old, walk-through heart -- an iconic object that looms vividly in the memories of generations of museum visitors -- is gone.The heart, with its cheesy "lub dub" heart sounds and carvernous interior certainly made an impression on this fourth grader the first time he saw it.
Built of plaster around a building-support pillar, it could not be dismantled intact. It had to be broken into pieces, Ward said. Several families of workers who built the old heart got pieces as mementos, she said.
"It was very popular for many decades," Ward said, "but it was static, and we have so many new technologies now to make something like that come alive."
-Wes
PS: The old heart's replacement.
Monday, August 24, 2009
The Stephen Colbert Treadmill Heads to Space
... and it's not just any treadmill:
-Wes
The COLBERT, once simply known as T-2, is no ordinary treadmill. Engineers started with a medical treadmill available to anyone on Earth. NASA asked Wyle to nickel plate the parts and make some other modifications, including elastic straps that fit around the shoulders and waist to keep the runner from rocketing across the space station with the first hard step.Heh.
Engineers also faced the serious problem of keeping the treadmill from shaking the whole station with every step taken since the ISS is floating just like the astronauts and wants to react against any movement. Even small actions can shake up delicate microgravity experiments taking place inside the station's laboratories.
While another, older treadmill on the ISS relied on a powered system of gyroscopes and mechanisms to reduce vibrations, the COLBERT's Vibration Isolation System was designed to work without power and be more reliable than its predecessor. The COLBERT rests on springs that are hooked to dampeners. That unit is connected to a standard-sized rack that has been extensively reinforced to handle the power produced by COLBERT users. The rack alone weighs 2,200 pounds.
The one tradeoff? Perhaps fitting for a treadmill named after Stephen Colbert, it is loud.
-Wes
The $1 EKG
Are you a nerd? If so, you'll love this super-simple single-lead EKG design, facilitated by digital filters from a computer sound card and three pennies for electrodes.
Estimated cost?
About $1.
-Wes
h/t: BoingBoing.net.
Estimated cost?
About $1.
-Wes
h/t: BoingBoing.net.
Wine and Heart Disease
This review from Michael Apstein, MD, a gastroenterologist at Beth Israel Deaconess Medical Center in Boston and an assistant professor of medicine at Harvard Medical School, is one of the better reviews I've seen in a while regarding the associations, and proof, of wine's effects on the heart.
-Wes
-Wes
Making Progress on Health Care Reform
From the Chicago Tribune today:
The half-dozen leading proposals in Congress would require all citizens to have health insurance, guaranteeing insurers tens of millions of new customers, many of whom would get government subsidies to help pay the companies' premiums. At the same time, these proposals would limit government's potential role as competitor and regulator.While frustrating, this story misses another even more powerful lobby than the insurance industry: AARP. We should not forget that AARP made $497.6 million (43% of its $1.17 billion in revenues) from royalties in 2007 (the last year 'non-profit' tax data are published), much of it garnered by attaching their name to insurance products for people over the age of 50.
"The insurers are going to do quite well," said Linda Blumberg, a health policy analyst at the non-partisan Urban Institute, a Washington-based think tank. "They are going to have this very stable pool, they're going to have people getting subsidies to help them buy coverage and ... they will be paid the full costs of the benefits that they provide, plus their administrative costs."
UnitedHealth Group, the top U.S. insurer by sales, last month reported that revenue grew to $21.7 billion in the three months ended in June, compared with $20.3 billion from the year-ago period.
No wonder we're making such real progress on health care reform.
-Wes
Sunday, August 23, 2009
Unprecedented Realism
“There are few people who are not ashamed of their love affairs when the infatuation is over.”
- François, Duc De La Rochefoucauld
The end of an infatuation is always rather sad – we have many expressions for it, “the bloom is off the rose” comes to mind. Falling out of love is often a moment of maturity, a moment of coming out of an illusion – never wholly welcome.
We have had many decades of uncritical, wholesale adolescent-style adoration, heartbreak and hate towards our politicians. We have been capable of sustaining illusions and uncritical thought with support from a similarly dazzled media. This has been done for years on both sides of the aisle. This kind of idealism says that we have finally found the man (party) who will (choose one) solve our problems, understand us, have complete integrity, be able to function in a trustworthy and honest fashion. This idealism comforted us by putting some in black hats and some in white. The comforts of certainty, zeal and clarity, even if untrue, are hard to resist. How long we can sustain this with any one politician or party depends on the filter we have, and how much attention we are paying. This is how crushes are sustained, in romance and in politics.
There are signs on the ground that we are beginning to grow up. We are beginning to understand that the corruption, self-interest, special interests and spin exist symbiotically on both sides of the aisle. With the deeply personal debate on health care and its associated reform costs, our need for honesty and successful policy to save our country is suddenly more important to us than the comfort of bedtime stories. This is political maturity.
What are the signs of this? Take for example, the publics’ realization that our representatives have not read a bill in its entirety. This conversation did not even occur as little as ten years ago – we assumed a level of expertise by our elected officials, or we didn’t care, but somehow, and this is the point, the illusion was maintained. In retrospect, I would imagine few bills were ever read page by page – and that the fact that they are not now is nothing new. What is new is that we now care about this. What is new is that we now see that legislation has a direct impact upon us. What is new is that we realize this congressional neglect shelters corruption in the form of deals, earmarks and policy that the public would not support if there was transparency. And we now see that there is transparency not provided by a beneficent body of elected officials or trusted news sources, but rather there is transparency because of the internet. It is unprecedented that we can summon chapter and verse of any bill onto our own computer – almost in real time.
This is a game-changer.
We are now (as voters) in a position to demand that legislation (including I daresay health-care reform) occur in incremental, transparent, understandable terms that voting citizens can vet themselves. Not thousands of pages of nearly incomprehensible gobbledygook. Anything short of that has become unacceptable, in part because we are also now able to contact our representatives at a moments notice. In years to come, we will now look back and see the final lipstick-on-the-collar moment in our relationship with Congress as the ramming through of the unread, un-vetted Stimulus Package.
The bloom is off the rose. It’s time for a new kind of politics: a mature, unprecedented realism.
Politicians should dismiss the public as “not ready for this” at their own risk.
"When patterns are broken, new worlds can emerge."-Tuli Kupferberg
Saturday, August 22, 2009
Robin Williams Discusses his Aortic Valve Replacement
He's an exerpt from a candid video where Robin Williams discusses his rationale for choosing the type of valve replacement he received:
-Wes
"... here are your choices:The video provides a very real (and, yes, humorous) glimpse into the emotional and physical impact of aortic valve surgery as only Robin Williams can portray.
- pig valve, which is great, you can find truffles,
- mechanical valve, which clicks and you know, weird, (eds note: that also requires chronic anticoagulation)
- and bovine - great, 'I'll go bovine, Bob, for 20!'"
-Wes
Saturday, August 15, 2009
EP Lab Crasher
One last thing before I leave on my trip, I wanted to be first to cash in on the latest internet craze: the Crasher Squirrel:

Heh.
-Wes
Heh.
-Wes
Friday, August 14, 2009
A Summer Blog Break
Dr. Wes will be traveling overseas beginning tomorrow afternoon and will be taking a rather lengthy blog break until next weekend. As such, I regret I will be unable to moderate comments on this blog during that time.
Unlike Dr. Rich who manages to deduct such trips as he parlays new entrepreneurial endeavors or like Congressional "fact-finding" missions that use other people's money, I have chosen to take my personal vacation trip when the currency exchange rate is the least favorable to support the local economies and assure that I can't retire any time in the forseeable future.
So as I depart, I thought I'd link to a few of my favorite posts from year's gone by for your reading pleasure. I look forward to my resuming this project when I return during the last week in August.
Weekend Fun
Perfecting Social Graces
Spiders on Drugs (Video)
An Open Letter to Patients Regarding Health Reform
Why Medical Errors Are Good for You
The Concertos
I Didn't Practice Evidence-Based Medicine Today
Imagine a World Without Medicare
Mine's Bigger
More on Doctors and Lawyers
HIPAA's Worthless and Here's Why
Our Healthcare Hindenburg
Still Smoking? Look At This
Doubling Down
The Tim Russert Fallout
The Quiet Hero
Why You Should Be a Doctor
The Health Information Legacy Problem
Med Schools Fail at the Business of Medicine
-Wes
Unlike Dr. Rich who manages to deduct such trips as he parlays new entrepreneurial endeavors or like Congressional "fact-finding" missions that use other people's money, I have chosen to take my personal vacation trip when the currency exchange rate is the least favorable to support the local economies and assure that I can't retire any time in the forseeable future.
So as I depart, I thought I'd link to a few of my favorite posts from year's gone by for your reading pleasure. I look forward to my resuming this project when I return during the last week in August.
Weekend Fun
Perfecting Social Graces
Spiders on Drugs (Video)
An Open Letter to Patients Regarding Health Reform
Why Medical Errors Are Good for You
The Concertos
I Didn't Practice Evidence-Based Medicine Today
Imagine a World Without Medicare
Mine's Bigger
More on Doctors and Lawyers
HIPAA's Worthless and Here's Why
Our Healthcare Hindenburg
Still Smoking? Look At This
Doubling Down
The Tim Russert Fallout
The Quiet Hero
Why You Should Be a Doctor
The Health Information Legacy Problem
Med Schools Fail at the Business of Medicine
-Wes
Wireless Home Monitoring of Pacemakers is Here
No, it's not a wireless pacemaker.
Rather, it's a pacemaker with a small radio transmitter inside that can talk to a base station that's attached to a phone line, much like many cordless phones we find at home. We call this "wireless telemetry." This same technology has been around for quite a while with our sister devices that treat both fast and slow heart rhythms: defibrillators. (Recall the recent firestorm of media attention that was created when researchers hacked the communication protocol while their antenae within 6 inches of the device.)
No doubt the new pacemakers with wireless telemetry will have the capability to upload information if pacing parameters like lead impedances readings (too low - there's an insulation break; too high - there's a lead fracture) and remaining battery voltage, as well as other cool tidbits of information that might be added to new sensors and the like. The hope, of course, is that through the use of this technology, the number of patient visits to device clinics (to assure proper functioning) will reduce the number of doctor visits a patient will have to make and therefore reduce costs.
But there is a potential downside to this technology. It is not lost on any engineer that the telemetry circuit for these pacemakers will use considerable battery energy to function. What we don't know is how much this added feature will reduce the device's longevity, especially if used frequestly. I would suspect we'll see slightly larger battery sizes to offset this higher energy demand of the device. Still, this feature will become the de facto standard for most new devices as we move from in-clinic pacemaker follow-up to home-based patient follow-up.
That is, of course, as long as no one wants to hack granny's pacemaker.
-Wes
Rather, it's a pacemaker with a small radio transmitter inside that can talk to a base station that's attached to a phone line, much like many cordless phones we find at home. We call this "wireless telemetry." This same technology has been around for quite a while with our sister devices that treat both fast and slow heart rhythms: defibrillators. (Recall the recent firestorm of media attention that was created when researchers hacked the communication protocol while their antenae within 6 inches of the device.)
No doubt the new pacemakers with wireless telemetry will have the capability to upload information if pacing parameters like lead impedances readings (too low - there's an insulation break; too high - there's a lead fracture) and remaining battery voltage, as well as other cool tidbits of information that might be added to new sensors and the like. The hope, of course, is that through the use of this technology, the number of patient visits to device clinics (to assure proper functioning) will reduce the number of doctor visits a patient will have to make and therefore reduce costs.
But there is a potential downside to this technology. It is not lost on any engineer that the telemetry circuit for these pacemakers will use considerable battery energy to function. What we don't know is how much this added feature will reduce the device's longevity, especially if used frequestly. I would suspect we'll see slightly larger battery sizes to offset this higher energy demand of the device. Still, this feature will become the de facto standard for most new devices as we move from in-clinic pacemaker follow-up to home-based patient follow-up.
That is, of course, as long as no one wants to hack granny's pacemaker.
-Wes
Thursday, August 13, 2009
Medicine's New Car Pricing
One of the most distasteful moments in life is walking in to a car dealership and knowing that the prices on the vehicles mean nothing relative to the purchase price you must "negotiate."
Once you decide on a car (and your heart's set on it), you are immediately ushered to a nice desk and a polite salesman types on a computer, adds a few numbers to a spreadsheet, lets the speadsheet add in a little extras sales tax and numerous "fees," and then swivels the monitor your way to show you what the real cost of ownership. You smile politely, knowing he's padded the amount with his commission and dealer mark-up, then start negotiating.
At first the dealer is appauled that you would do such a thing. You threaten to leave. Magically a few thousand dollars disappears. You're still not impressed. He asks if you have a trade-in. You say, "No." He offers you dealer financing. You decline and offer cash. He gets his manager. His manager, looking like "Slick Willy," turns up the heat. They walk away. They return and remove a few hundred more. You know other dealerships can do it cheaper. They say best of luck. You walk out, thoroughly pissed. The salesman runs out to the parking lot and offers a final price two thousand cheaper. You stop, and wonder, "who the hell are these guys?" and drive off.
Such is the case with health care pricing, too.
The only problem is, of course, that you're dealing with your health at a very vulnerable moment in life. "List price" in medicine means nothing any longer. Whether your insured or uninsured, the prices that appear initially on your bill mean nothing. You must haggle.
Insured folks have agreed to let most of the haggling be done for them by the insurer, since the prices insurers pay for health care are pre-negotiated with hospital systems beforehand. You, in accepting a particular policy plan, get to "pick" your deductible and co-pay amounts, knowing full well that the negotiators are taking their piece. But that's the price the War Lords of health care system have exacted on the common man in the name of "transparency."
Noninsured folks have it much tougher. They get the list price sent to them after their care and get to feel the impending doom of realizing they've bought a Mercedes when they could only afford a Hyundai. So they make an appointment with the financial assistance office at the hospital. The nice lady there determines your ability to pay. If your "lucky" enough to be unemployed and have little income, you might get a flat 35% off. If not, no worries, an easy payment plan will be arranged. Never mind the bills will continue for years. Never mind that you have to have another operation and another admission in three months.
But even worse are to poor saps who have insurance and come from out of state, or those with tons of cash and don't want the world to know about their illness. They pay full fee. That's how the game goes. And that's why hospitals inflate their prices: "there's money in the thar' hills!" That extra money pays for lots of little extras at hospitals.
To be fair, hospitals aren't the only ones to blame. Like a co-dependent spouse of an alcoholic, the payment system that only pays only 80% of costs and leaves the rest to be paid by secondary insurers or the patient (as Medicare does) further enables this dysfunctionality. The lack of price transparency for our entire health care system is staggering. No wonder no one knows what things really cost in health care and no wonder ANY attempt to estimate costs always underestimates reality (poor CBO).
And so, when we see survey's from the New York Times finding that there are high fees in medicine, I can only say, "Duh!"
Welcome to the world of obfuscation and new car pricing.
Real reform would require no-haggle CarMax pricing but none of the current proposals require this.
If they did, then maybe we'd get somewhere in the health care debate.
-Wes
Once you decide on a car (and your heart's set on it), you are immediately ushered to a nice desk and a polite salesman types on a computer, adds a few numbers to a spreadsheet, lets the speadsheet add in a little extras sales tax and numerous "fees," and then swivels the monitor your way to show you what the real cost of ownership. You smile politely, knowing he's padded the amount with his commission and dealer mark-up, then start negotiating.
At first the dealer is appauled that you would do such a thing. You threaten to leave. Magically a few thousand dollars disappears. You're still not impressed. He asks if you have a trade-in. You say, "No." He offers you dealer financing. You decline and offer cash. He gets his manager. His manager, looking like "Slick Willy," turns up the heat. They walk away. They return and remove a few hundred more. You know other dealerships can do it cheaper. They say best of luck. You walk out, thoroughly pissed. The salesman runs out to the parking lot and offers a final price two thousand cheaper. You stop, and wonder, "who the hell are these guys?" and drive off.
Such is the case with health care pricing, too.
The only problem is, of course, that you're dealing with your health at a very vulnerable moment in life. "List price" in medicine means nothing any longer. Whether your insured or uninsured, the prices that appear initially on your bill mean nothing. You must haggle.
Insured folks have agreed to let most of the haggling be done for them by the insurer, since the prices insurers pay for health care are pre-negotiated with hospital systems beforehand. You, in accepting a particular policy plan, get to "pick" your deductible and co-pay amounts, knowing full well that the negotiators are taking their piece. But that's the price the War Lords of health care system have exacted on the common man in the name of "transparency."
Noninsured folks have it much tougher. They get the list price sent to them after their care and get to feel the impending doom of realizing they've bought a Mercedes when they could only afford a Hyundai. So they make an appointment with the financial assistance office at the hospital. The nice lady there determines your ability to pay. If your "lucky" enough to be unemployed and have little income, you might get a flat 35% off. If not, no worries, an easy payment plan will be arranged. Never mind the bills will continue for years. Never mind that you have to have another operation and another admission in three months.
But even worse are to poor saps who have insurance and come from out of state, or those with tons of cash and don't want the world to know about their illness. They pay full fee. That's how the game goes. And that's why hospitals inflate their prices: "there's money in the thar' hills!" That extra money pays for lots of little extras at hospitals.
To be fair, hospitals aren't the only ones to blame. Like a co-dependent spouse of an alcoholic, the payment system that only pays only 80% of costs and leaves the rest to be paid by secondary insurers or the patient (as Medicare does) further enables this dysfunctionality. The lack of price transparency for our entire health care system is staggering. No wonder no one knows what things really cost in health care and no wonder ANY attempt to estimate costs always underestimates reality (poor CBO).
And so, when we see survey's from the New York Times finding that there are high fees in medicine, I can only say, "Duh!"
Welcome to the world of obfuscation and new car pricing.
Real reform would require no-haggle CarMax pricing but none of the current proposals require this.
If they did, then maybe we'd get somewhere in the health care debate.
-Wes
Wednesday, August 12, 2009
Surgeons Set Obama Straight
From the American College of Surgeons' press release:
-Wes
The American College of Surgeons is deeply disturbed over the uninformed public comments President Obama continues to make about the high-quality care provided by surgeons in the United States. When the President makes statements that are incorrect or not based in fact, we think he does a disservice to the American people at a time when they want clear, understandable facts about health care reform. We want to set the record straight.Amen.•Yesterday during a town hall meeting, President Obama got his facts completely wrong. He stated that a surgeon gets paid $50,000 for a leg amputation when, in fact, Medicare pays a surgeon between $740 and $1,140 for a leg amputation. This payment also includes the evaluation of the patient on the day of the operation plus patient follow-up care that is provided for 90 days after the operation. Private insurers pay some variation of the Medicare reimbursement for this service.We agree with the President that the best thing for patients with diabetes is to manage the disease proactively to avoid the bad consequences that can occur, including blindness, stroke, and amputation. But as is the case for a person who has been treated for cancer and still needs to have a tumor removed, or a person who is in a terrible car crash and needs access to a trauma surgeon, there are times when even a perfectly managed diabetic patient needs a surgeon. The President's remarks are truly alarming and run the risk of damaging the all-important trust between surgeons and their patients.
•Three weeks ago, the President suggested that a surgeon's decision to remove a child's tonsils is based on the desire to make a lot of money. That remark was ill-informed and dangerous, and we were dismayed by this characterization of the work surgeons do. Surgeons make decisions about recommending operations based on what's right for the patient.
We assume that the President made these mistakes unintentionally, but we would urge him to have his facts correct before making another inflammatory and incorrect statement about surgeons and surgical care.
-Wes
To AMA or Not AMA - That is the Question
"Dear Colleague:And so begins a recent e-mail sent to electrophysiologists around the country from the Heart Rhythm Society.
In this era of health care reform, it has been said that when it comes to reimbursement issues, “you are either at the table or on the menu.” President Obama has said that he would like to cut Medicare costs by more than 300 billion dollars in the next 10 years. The Heart Rhythm Society needs to be at the table, and we need your help. To strengthen the Society's ability to represent your interests, we need to gain a seat in the American Medical Association (AMA) House of Delegates. This is one of the “tables” where the critical medical policy decisions are being made.
We know that many of you believe that AMA does not always represent your interests. You are not alone. Many physicians across all medical societies struggle with this, including those from societies who are already in the AMA House of Delegates. But it is critical that the Society is in all policymaking arenas to influence the future of EP practice. The AMA House of Delegates opens important doors for us — especially those entities who are in control of identifying Medicare procedures that will be reimbursed and performance measures that will be the basis for Medicare reimbursement in the future."
I find myself at a critical crossroad. Any society that has gone "all-in" as the AMA did with the recent H.R. 3200 because they simply wanted a "seat at the negotiating table" without evaluating the legislation has me deeply concerned. It was clear from the recent AMA House of Delegates meeting that physicians were NOT in agreement with a single payer system, and yet the AMA leadership decided unilaterally in under 24 hours after the first house bill was released to side with the legislation: legislation created more from special interests needs than those of the physicians and patients long term.
And like the push to approve the House Bill before the August recess, I have until 31 August to join the AMA so the Heart Rhythm Society can have a representative at the House of Delegates.
Problem is, it didn't matter for the societies that HAD delegates there before, what makes me think it'll matter now?
-Wes
Tuesday, August 11, 2009
Saving the Jewels
No, these things below are not Mickey Mouse ears. Designed by Pam Krieg, RN, a neonatal ICU nurse, I saw these little radiation shields in our neonatal unit recently and was happy to see they're using them on our little ones:
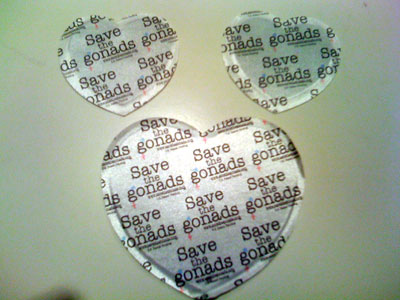
As a cardiologist and cardiac electrophysiologist who gets way too much radiation, I can appreciate their importance and loved their shape. But it wasn't until I read their instructions for use that I realized why their shaped that way. It seems the shape is used differently for boys vs. girls.
Cool. You learn something new every day.
-Wes
Reference: More info from SavetheGonads.com.
Neonatal and newborn radiation shields for the "jewels."
As a cardiologist and cardiac electrophysiologist who gets way too much radiation, I can appreciate their importance and loved their shape. But it wasn't until I read their instructions for use that I realized why their shaped that way. It seems the shape is used differently for boys vs. girls.
Cool. You learn something new every day.
-Wes
Reference: More info from SavetheGonads.com.
Grand Rounds with a Health Reform Theme is Up
Head on over to Dr. Rich at the Covert Rationing blog and enjoy this week's best of the blog-o-sphere!
-Wes
-Wes
Poland's Syndrome: A Friendly Amendment
I read the excellent review of Poland's Syndrome recently published by Ramona Bates, MD over at the Suture For a Living blog. I encourage all of you to head over there and enlighten yourself.
For those unfamiliar, this syndrome involves the absence of sternal head of the pectoralis major, hypoplasia and/or aplasia of breast or nipple, deficiency of subcutaneous fat and axillary hair, abnormalities of rib cage, and upper extremity anomalies. The upper extremity anomalies include short upper arm, forearm, or fingers (brachysymphalangism). Remarkably, I had never seen one of these cases in my clinic before, but met a nice gentleman recently who thought his syndrome was called "Pol's Syndrome, or something like that," and with the quick help of Google, he and I quickly surfed the web together in my office and discovered he actually had "Poland's Syndrome."
I was referred to see him for non-sustained asymptomatic ventricular tachycardia noted on a recent stress test. Consequently, an EKG was performed. Before I get to that, my patient was nice enough to permit me to include the photos of his chest and upper extremities and share them here:

The Chest of a Patient With Poland's Syndrome

Hands of a Patient With Poland's Syndrome
So now, in the spirit of collegiality in medicine, I'd like to add one more thing to the syndrome: possible "pseudo-ventricular hypertrophy on the EKG when the left pectoral muscle is absent." Here's the patient's EKG:
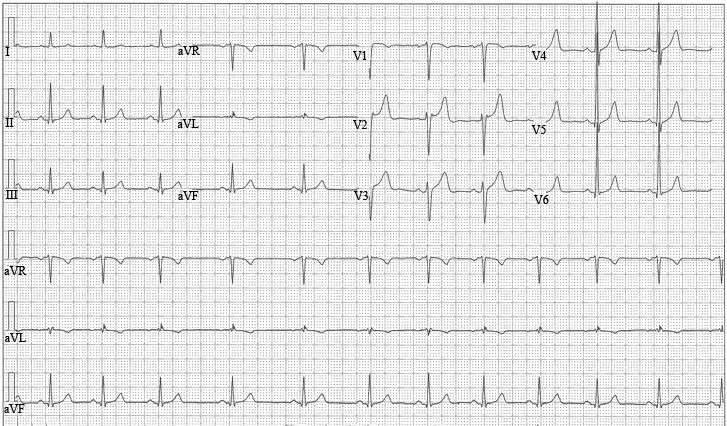
EKG of a Patient With Poland's Syndrome - Click to Enlarge
There. This modification to the syndrome is now etched in the highly scientific ether of the blog-o-sphere. Of note, his echocardiogram failed to demonstrate any left ventricular hypertrophy or cardiac anomaly.
-Wes
For those unfamiliar, this syndrome involves the absence of sternal head of the pectoralis major, hypoplasia and/or aplasia of breast or nipple, deficiency of subcutaneous fat and axillary hair, abnormalities of rib cage, and upper extremity anomalies. The upper extremity anomalies include short upper arm, forearm, or fingers (brachysymphalangism). Remarkably, I had never seen one of these cases in my clinic before, but met a nice gentleman recently who thought his syndrome was called "Pol's Syndrome, or something like that," and with the quick help of Google, he and I quickly surfed the web together in my office and discovered he actually had "Poland's Syndrome."
I was referred to see him for non-sustained asymptomatic ventricular tachycardia noted on a recent stress test. Consequently, an EKG was performed. Before I get to that, my patient was nice enough to permit me to include the photos of his chest and upper extremities and share them here:
The Chest of a Patient With Poland's Syndrome
Note the congenital abscence of the left nipple and pectoralis muscle.
Hands of a Patient With Poland's Syndrome
The left hand has gone under significant reconstruction to permit an opposable thumb and individual digits.
So now, in the spirit of collegiality in medicine, I'd like to add one more thing to the syndrome: possible "pseudo-ventricular hypertrophy on the EKG when the left pectoral muscle is absent." Here's the patient's EKG:
EKG of a Patient With Poland's Syndrome - Click to Enlarge
Note the present of large precordial voltage suggestive of left ventricular hypertrophy due to proximity of the EKG leads to the heart.
There. This modification to the syndrome is now etched in the highly scientific ether of the blog-o-sphere. Of note, his echocardiogram failed to demonstrate any left ventricular hypertrophy or cardiac anomaly.
-Wes
Monday, August 10, 2009
The Med Student's Pockets: Then and Now
In case you've forgotten what medical students' pockets looked like:
This was then:

And this is now:

-Wes
This was then:
And this is now:
-Wes
Metamorphosis
It’s the kind of thing you don’t expect.
It starts with a bit of reluctance, peppered with a reservation, knowing that things will take a bit longer this day.
And there you are, contemplating the day ahead, when a soft voice interrupts the reverie:
“Uh, are you Dr. Fisher?”
You turn and see not a colleague, but a stranger, a young stranger much more fit than you, smiling. You admire the crispness of their lab coat, the gleam in their eye, the enthusiasm that seems to exude from their pores. Not that anything has happened, mind you, but still, for a brief moment, you see yourself in the same place many years ago. Eager, anxious, awestruck and clueless, all blended together in a complicated emotional goulash.
Years ago it was you, entering a different lab. You knew no one, knew nothing and barely had an idea how to tie a facemask so your chin was not permanently touching your chest. Surrounded by instruments and tech-speak you watched. You had no idea how in the hell you’d ever be able to do this, but never dared to admit it.
But time passed.
Slowly, gradually, carefully, your mentor introduced you to your new home away from home. See one, do one. Bit by tiny bit. Hundreds of hours, thousands of anecdotes. Each meant to shape you, scare you, and guide you. “Here, feel what 1500 psi feel like in your hand” as the pigtail spewed contrast in my palm. “How many cc’s are in that catheter?” “This is the image intensifier.” “Gotta hold longer.” Tons of iterations, plenty of mistakes. “It’s okay to make a mistake once,” they’d say, “but not twice.” Papers. Research. Presentations. Fewer inefficiencies. You taught the first- and second-years, but still were the student.
And then they said you were done.
But you quickly realized you hadn’t even started. Going alone is different. Very different. So you learned some more. You kept watching, absorbing, getting faster, safer, yet always losing sleep over tough cases. Again and again and again. Soon you realize you're growing weary, growing old.
Until in the din of a back room a fresh face walks in and asks who you are.
And suddenly you realize it's good to slow down again, if for just a moment, since the student is the teacher in more ways than one.
It starts with a bit of reluctance, peppered with a reservation, knowing that things will take a bit longer this day.
And there you are, contemplating the day ahead, when a soft voice interrupts the reverie:
“Uh, are you Dr. Fisher?”
You turn and see not a colleague, but a stranger, a young stranger much more fit than you, smiling. You admire the crispness of their lab coat, the gleam in their eye, the enthusiasm that seems to exude from their pores. Not that anything has happened, mind you, but still, for a brief moment, you see yourself in the same place many years ago. Eager, anxious, awestruck and clueless, all blended together in a complicated emotional goulash.
Years ago it was you, entering a different lab. You knew no one, knew nothing and barely had an idea how to tie a facemask so your chin was not permanently touching your chest. Surrounded by instruments and tech-speak you watched. You had no idea how in the hell you’d ever be able to do this, but never dared to admit it.
But time passed.
Slowly, gradually, carefully, your mentor introduced you to your new home away from home. See one, do one. Bit by tiny bit. Hundreds of hours, thousands of anecdotes. Each meant to shape you, scare you, and guide you. “Here, feel what 1500 psi feel like in your hand” as the pigtail spewed contrast in my palm. “How many cc’s are in that catheter?” “This is the image intensifier.” “Gotta hold longer.” Tons of iterations, plenty of mistakes. “It’s okay to make a mistake once,” they’d say, “but not twice.” Papers. Research. Presentations. Fewer inefficiencies. You taught the first- and second-years, but still were the student.
And then they said you were done.
But you quickly realized you hadn’t even started. Going alone is different. Very different. So you learned some more. You kept watching, absorbing, getting faster, safer, yet always losing sleep over tough cases. Again and again and again. Soon you realize you're growing weary, growing old.
Until in the din of a back room a fresh face walks in and asks who you are.
And suddenly you realize it's good to slow down again, if for just a moment, since the student is the teacher in more ways than one.
Sunday, August 09, 2009
Your Prescription Information For Sale
I wish this was hard to believe:
But with the pharmaceutical industry soon to release $150M dollars of ads promoting health reform as they cozy up to Congressional leaders, the conflicts of interest for patient's privacy are staggering. Further, the promotion of the electronic medical record, personal health records, and ultimately, cloud computing (where no one will know where health data resides), are firmly part of the health reform landscape.
Now before people think I'm totally against the EMR, let me be candid: I'm not. It does facilitate care and is an incredible means of communication between physicians and laboratories and pharmacies and the like. When used properly, they are miraculous.
But the risks of losing information remain huge. Certainly, the above referenced New York Times article notes that safeguards are supposed to be enacted to prevent this wholesale marketing of your health data.
But suddenly, we learn of a White House snitch line where they will collect e-mails of people who might be spreading "misinformation" about the health reform efforts underway. (Thanks to my previous blog post, I am happy to report I've been reported! ;)) But this occurs at a time when privacy issues in health care must be seen as paramount and electronic medical records prototed as secure.
Ooops.
So now we have a White House eager to build a snitch line as they cozy up to pharaceutical interests that are already selling personal information from prescription data, all while trying to promote the security of electronic medical records to the masses.
Who are they kidding?
But then, shucks, just think of the marketing possibilities for the government:
And lest people think I'm too partisan (who me?), the Republicans with their travel junkets aren't any better.
Sheesh!
-Wes
Reference: White House blog with snitch e-mail link at flag@whitehouse.gov .
Like many other people, Ms. Krinsk thought that her prescription information was private. But in fact, prescriptions, and all the information on them — including not only the name and dosage of the drug and the name and address of the doctor, but also the patient’s address and Social Security number — are a commodity bought and sold in a murky marketplace, often without the patients’ knowledge or permission.But given the money involved, I'm afraid it isn't.
But with the pharmaceutical industry soon to release $150M dollars of ads promoting health reform as they cozy up to Congressional leaders, the conflicts of interest for patient's privacy are staggering. Further, the promotion of the electronic medical record, personal health records, and ultimately, cloud computing (where no one will know where health data resides), are firmly part of the health reform landscape.
Now before people think I'm totally against the EMR, let me be candid: I'm not. It does facilitate care and is an incredible means of communication between physicians and laboratories and pharmacies and the like. When used properly, they are miraculous.
But the risks of losing information remain huge. Certainly, the above referenced New York Times article notes that safeguards are supposed to be enacted to prevent this wholesale marketing of your health data.
But suddenly, we learn of a White House snitch line where they will collect e-mails of people who might be spreading "misinformation" about the health reform efforts underway. (Thanks to my previous blog post, I am happy to report I've been reported! ;)) But this occurs at a time when privacy issues in health care must be seen as paramount and electronic medical records prototed as secure.
Ooops.
So now we have a White House eager to build a snitch line as they cozy up to pharaceutical interests that are already selling personal information from prescription data, all while trying to promote the security of electronic medical records to the masses.
Who are they kidding?
But then, shucks, just think of the marketing possibilities for the government:
And lest people think I'm too partisan (who me?), the Republicans with their travel junkets aren't any better.
Sheesh!
-Wes
Reference: White House blog with snitch e-mail link at flag@whitehouse.gov .
Saturday, August 08, 2009
All the President's Men: Lipstick Cost Control
Representative Michele Bachmann (R - Minnesota, 6th District) referred to a quote by Ezekiel J. Emanuel, MD, PhD on the floor of the House before the House recess:
Maybe rather than taking away physicians' discretion regarding end-of-life decisions and care (especially when tort reform is not and has not been part of the reform discussion) we should ask why are we being smeared with the "EMR-Prevention-Wellness-Waste Reduction" lipstick as a means to justify significant cost savings if it's all a ruse. Might all those non-intercommunicating computer systems, drugs, testing, and wellness initiatives actually increase the costs of care delivery due to the large number needed to treat to save one life? Have these things really saved costs to our "system" or merely made healthy patients sick?
But then, serious discussion wouldn't be feeding our political constituents, would it?
Here's the video of Bachmann's comments:
-Wes
Addendum: This from the New England Journal of Medicine - Prevention might not save costs. Who knew?
"Vague promises of savings from cutting waste, enhancing prevention and wellness, installing electronic medical records, and improving quality are merely lipstick cost control, more for show and public relations, than for true change."He's right, of course. But what he proposes instead is threatening to the doctor-patient relationship, especially when the government intervenes in end-of-life decisions. Could government bodies ever understand the nuances of a patient's illness and family dynamic when a loved one is near death? It is hard to conceive how any doctor could take the Hippocratic Oath, as Emanuel states, "too seriously" at that time.
Maybe rather than taking away physicians' discretion regarding end-of-life decisions and care (especially when tort reform is not and has not been part of the reform discussion) we should ask why are we being smeared with the "EMR-Prevention-Wellness-Waste Reduction" lipstick as a means to justify significant cost savings if it's all a ruse. Might all those non-intercommunicating computer systems, drugs, testing, and wellness initiatives actually increase the costs of care delivery due to the large number needed to treat to save one life? Have these things really saved costs to our "system" or merely made healthy patients sick?
But then, serious discussion wouldn't be feeding our political constituents, would it?
Here's the video of Bachmann's comments:
-Wes
Addendum: This from the New England Journal of Medicine - Prevention might not save costs. Who knew?
Back to Basics: The Cardiac Cycle
A nice introductory video appeared over at Not Nurse Ratched's blog that is worth sharing on the "plumbing" (blood flow) behind the cardiac cycle. It's worth viewing for anyone puzzled over how the heart pumps blood throughout the body:
How this mechanical pumping action is initiated by the heart's "electrical" system can be viewed on our introductory video about atrial fibrillation.
-Wes
How this mechanical pumping action is initiated by the heart's "electrical" system can be viewed on our introductory video about atrial fibrillation.
-Wes
Proof That Some Legislators Have Read the Health Reform Bill
And then it's scary what they found:
-Wes
When the bill got to the House Ways and Means Committee on July 16, it contained an especially audacious and egregious provision that could only be called a “trial lawyer earmark.” The 10-page measure would “open the door to massive liability that is neither in the public’s interest nor in the interest of the American healthcare system,” said Phil Goldberg, a lawyer who formerly served on the staff of the House Judiciary Committee and describes himself as a “lifelong Democrat.”Kudos to Walter Olson at Overlawyered.com for bringing this to the public's attention.
-Wes
Friday, August 07, 2009
Do NOT Try This at Home
I have no idea if this is real but, DANG, it sure looks cool:
Heh. Happy Friday.
-Wes
Heh. Happy Friday.
-Wes
Thursday, August 06, 2009
Hey, It's About ME!
It was a remarkable day in clinic yesterday.
Not because of the number of people I saw (12) or the clinical diversity seen, but rather how many people (4) asked me what I thought of the current health care reform bill before Congress.
The political spin being posed by Democrats is that people are staging town hall protests about their displeasure about the current health care reform efforts underway.
I don't think so.
Rather, I think people are finally realizing that the health care reform proposal on the table is no longer about the "47 million" uninsured, but rather, "Hey, this health care reform thing, why, it's about ME!"
-Wes
Not because of the number of people I saw (12) or the clinical diversity seen, but rather how many people (4) asked me what I thought of the current health care reform bill before Congress.
The political spin being posed by Democrats is that people are staging town hall protests about their displeasure about the current health care reform efforts underway.
I don't think so.
Rather, I think people are finally realizing that the health care reform proposal on the table is no longer about the "47 million" uninsured, but rather, "Hey, this health care reform thing, why, it's about ME!"
-Wes
Tuesday, August 04, 2009
Monday, August 03, 2009
On Package Inserts and Innovation
Every doctor knows of the package insert: the little paper with tons of fine print that is enclosed with medication bottles.
In short: package inserts are the formal "labeling" mandated by the the Food and Drug Administration (FDA) for new drugs.
Recently, I have had a chance to review a package insert in detail for one of the most common antiarrhythmic drugs I prescribe: amiodarone.
I was surprised to find that over my years as an electrophysiologist, that I have been prescribing amiodarone "off label" for every patient I treat with atrial fibrillation, an arrhythmia in the heart's upper chambers. That's because Amiodarone is technically only approved for use in treating lower chamber (ventricular) arrhythmias:
Not that this was a problem when the package insert was first developed. At that time, the original package contained the prevailing knowledge about the drug based on carefully developed clinical trials. The information was carefully reviewed by federal regulators to assure the prescribing information was as up to date and informative as possible. Every known problem with the drug was carefully mentioned to protect patients as much as possible. No doubt, that was a laudible goal.
But doctors later recognized the effectiveness of amiodarone to treat certain supraventricular arrhythmias like atrial fibrillation and quickly moved to adopt the drug into their therapeutic armamentarium. Case reports came first, then clinical trials - soon a new indication for the drug was born.
Cardiologists or electrophysiologists cannot follow the package insert recommendations for Amiodarone (or many other drugs) when they feel Amiodarone is the best drug to treat atrial fibrillation. But here we are years after the package inserts were developed, treating a huge number of patients with atrial fibrillation with a drug technically not approved for that indication by the FDA.
Fortunately, professional organizations have come to our support the cause by issuing clinical "guidelines" acknowledging the real world clinical use of amiodarone treatment:
Which leads me to several considerations:
1) It appears there is no incentive for government agencies to modify published package inserts or recommendations for therapy after market release despite safety and efficacy data to the contrary.
2) With compensation for cost-effective therapies increasingly tied to doctor "performance" using "state of the art information," will incentives for innovative new therapies diminish as a result?
3) Finally, if clinical innovation is somehow preserved, we can only wonder if government-controlled recommendations for therapies proposed in the immediate future by MEDPAC (that also reguire approval by Congress) will ever be updated once they become etched in policy stone - much like we see now with drug package inserts. Will we ever be able to advance care to our patients when new therapeutic recommendations surface without a literal act of Congress?
If our history with package inserts is any indication, it seems doubtful.
-Wes
In short: package inserts are the formal "labeling" mandated by the the Food and Drug Administration (FDA) for new drugs.
Recently, I have had a chance to review a package insert in detail for one of the most common antiarrhythmic drugs I prescribe: amiodarone.
I was surprised to find that over my years as an electrophysiologist, that I have been prescribing amiodarone "off label" for every patient I treat with atrial fibrillation, an arrhythmia in the heart's upper chambers. That's because Amiodarone is technically only approved for use in treating lower chamber (ventricular) arrhythmias:
Because of its life-threatening side effects and the substantial management difficulties associated with amiodarone use (seeThat's it. No indication for the treatment of atrial fibrillation or other supraventricular tachycardias (SVT's)... just ventricular fibrillation and ventricular tachycardia.
“WARNINGS” below), Pacerone® (Amiodarone HCl) Tablets are indicated only for the treatment of the following documented, life-threatening recurrent ventricular arrhythmias when these have not responded to documented adequate doses of other
available antiarrhythmics or when alternative agents could not be tolerated.
1. Recurrent ventricular fibrillation.
2. Recurrent hemodynamically unstable ventricular tachycardia.
Not that this was a problem when the package insert was first developed. At that time, the original package contained the prevailing knowledge about the drug based on carefully developed clinical trials. The information was carefully reviewed by federal regulators to assure the prescribing information was as up to date and informative as possible. Every known problem with the drug was carefully mentioned to protect patients as much as possible. No doubt, that was a laudible goal.
But doctors later recognized the effectiveness of amiodarone to treat certain supraventricular arrhythmias like atrial fibrillation and quickly moved to adopt the drug into their therapeutic armamentarium. Case reports came first, then clinical trials - soon a new indication for the drug was born.
Cardiologists or electrophysiologists cannot follow the package insert recommendations for Amiodarone (or many other drugs) when they feel Amiodarone is the best drug to treat atrial fibrillation. But here we are years after the package inserts were developed, treating a huge number of patients with atrial fibrillation with a drug technically not approved for that indication by the FDA.
Fortunately, professional organizations have come to our support the cause by issuing clinical "guidelines" acknowledging the real world clinical use of amiodarone treatment:
Although amiodarone is not approved for use in the treatment of atrial fibrillation (AF) by the FDA, it is the most commonly used antiarrhythmic drug for this purpose. This is based on 1 year efficacy rates for maintaining sinus rhythm of greater than 60%, compared to 50% or less for other antiarrhythmic agents.Yet we cannot help but note that the above FDA package insert for amiodarone (Pacerone) was revised "0508" (which I can only assume meant May, 2008), well after these non-FDA clinical guidelines were written.
Which leads me to several considerations:
1) It appears there is no incentive for government agencies to modify published package inserts or recommendations for therapy after market release despite safety and efficacy data to the contrary.
2) With compensation for cost-effective therapies increasingly tied to doctor "performance" using "state of the art information," will incentives for innovative new therapies diminish as a result?
3) Finally, if clinical innovation is somehow preserved, we can only wonder if government-controlled recommendations for therapies proposed in the immediate future by MEDPAC (that also reguire approval by Congress) will ever be updated once they become etched in policy stone - much like we see now with drug package inserts. Will we ever be able to advance care to our patients when new therapeutic recommendations surface without a literal act of Congress?
If our history with package inserts is any indication, it seems doubtful.
-Wes
Sunday, August 02, 2009
Subscribe to:
Posts (Atom)