Click image to enlarge
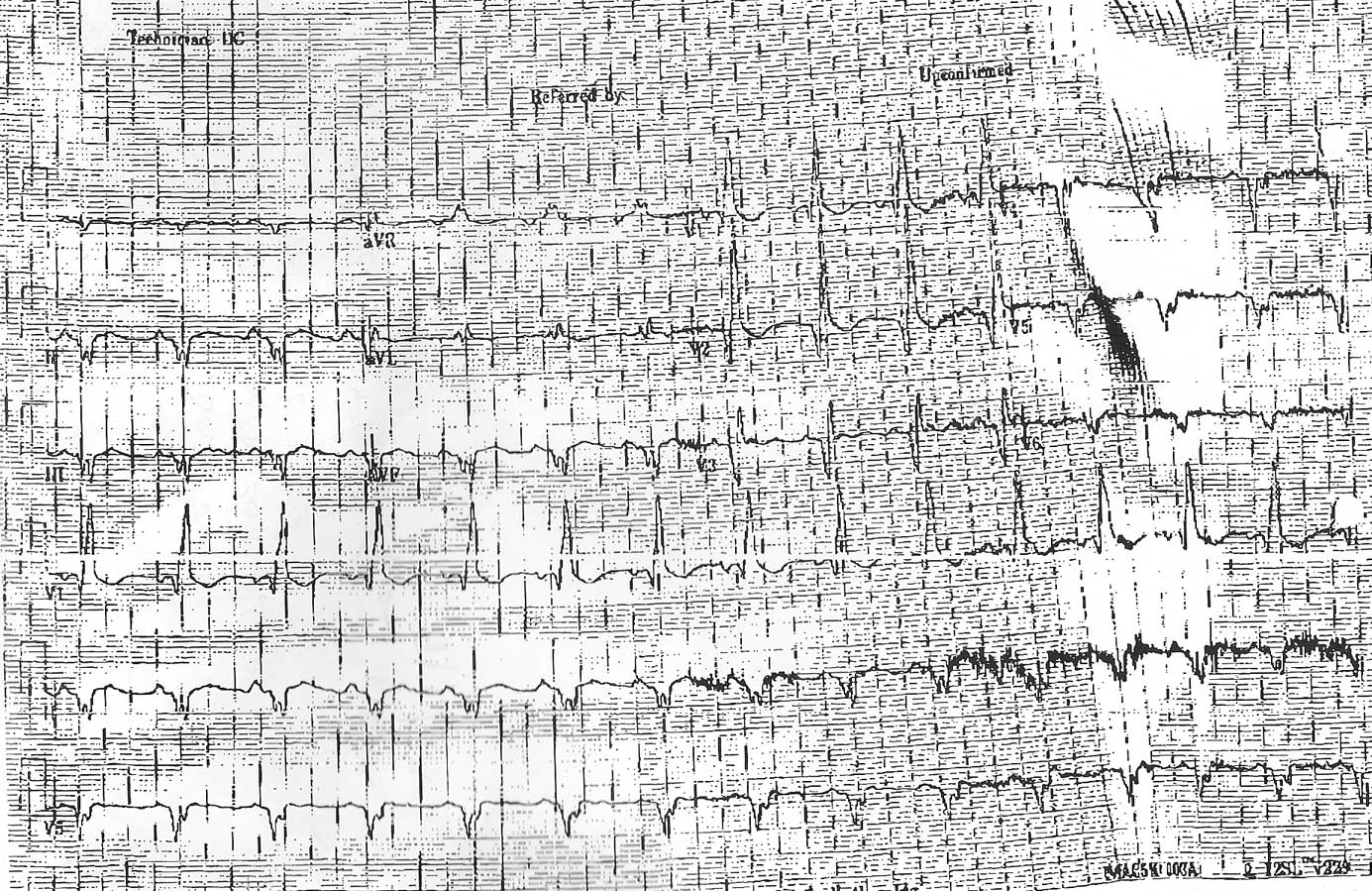
Your mission, should you decide to accept it my dear EKG aficionados, is to describe the findings as best you can. Because the patient has not yet arrived in your clinic and the referring doctor did not have access to an echocardiogram machine (theirs was broken), you must also estimate this patient's left ventricular ejection fraction based on this EKG alone. (Guesses are okay).
Good luck.
-Wes
8 comments:
. The tall R waves in V1 and deep, narrow Q waves in leads 1, aVL, and V4-6 are typical of Duchenne Muscular Dystrophy and are related to the characteristic posterolateral left ventricular involvement in this condition.Baseed on the history his ejection fraction is probably less than 30%
Anony 11:01PM-
While there are tall waves in V1, it is preceeded by a very large Q wave, which is uncharacteristic for Duchenne's muscular dystrophy. Duchenne's usually has a more characteristic "left rabbit ear larger than the right rabbit ear pattern consistent with an atypical RBBB-type appearance and fairly narrow Q waves (example here courtesy Medscape).
I would agree that the EF is likely less than 30%, but any guess how much less?
I'm not a trained physician and took a few graduate courses in lead field theory so don't mock my answer too much :-)
To my untrained eye it seems like the patient has large areas of infarct in the left anterior and left lateral free wall. My guess is an ejection fraction of about 20%?
I'm just a 'tern, but:
The patient's r-wave axis is, like, 240 in the frontal plane. That's not normal.
The initial precordial vector is pretty posterior, even though the terminal part of the QRS in those leads is pretty anterior, with a wide QRS.
Good news: sinus rhythm!
This patient seems to have an pretty absent anterior/lateral wall. Given that that's a pretty important part of the heart, I'm putting their EF at 15%. Depending on whether hey may have had some recovery from their initial event, it could, maybe, be more).
Extensive anterior and inferior infarction. Complicated RBBB. Probably left atrial abnormality. EF 10-15%.
I would guess that the patient had suffered a large anteroseptal infarct with Q waves v1-v6 as well as in the inferior leads and probable posterior infarct manifested with tall R waves v1. Poor R wave progression with extreme axis deviation. Widened qrs also portends poorer prognosis for severe cardiomyopathy. I would guess EF 15%.
I'm gonna' say his EF is about 0h-crappy-percent. Maybe around 10-15% would be my totally uneducated ballpark guess. But I like crappy...it's so much more descriptive.
Once again, thanks to all who ventured a "guess" on this case. As usual, the observations made on this EKG were great.
First, the patient is in sinus rhythm, but an extreme right axis deviation is noted with negative QRS complexes in I and II. I agree with Dr. Donnell that the P wave morphology in V1 is not quite negative enough to warrant a designation of left atrial enlargement, but certainly "left atrial abnormality" would be reasonable to describe on the EKG interpretation.
Right bundle branch block is present. Recall that Q waves that appear in the first 0.04 sec of RBBB can be interpreted as infarction. This EKG is remarkable for the presence of Q waves in nearly all leads except aVL and aVR (and perhaps lead I, but this is difficult to see).
The patient had undergone left heart catheterization and attempted proximal LAD stent placement in a large transapical vessel in the past, but this stent thrombosed, resulting in a massive anterior wall myocardial infarction that included an extensive portion of the inferior wall. The only wall moving at all was the posterolateral left ventricular wall, and the ejection fraction was calculated at 8%.
Post a Comment