Especially when their intent appears to be to change therapy recommendations based on conclusions from a retrospective meta-analyses. Meta-analyses are nothing more than selectively-pooled studies aggregated by statistical pseudoscientific hand-waving and data manipulation fraught with so many examples of bias that we have to wonder if the intent of the lead author's comments about such a study to the media were not focused on whether their hypothesis was an appropriate topic for future study, but rather if some just had another axe to grind.
Repeatedly this week we have seen the lead author of the meta-analysis that attempts to determine if QRS width can predict future responders to cardiac resynchronization therapy (CRT) promulgate opinion in the name of science. In fact, the study's lead author, Ilke Sipahi, MD leaps to such amazing conclusions about the study's findings that the mind just boggles. From the Wall Street Journal, to Consumer Reports and now, that bastion of scientific reporting, the New York Times, his comments resulted in a main stream media feeding frenzy on the technology. His conclusion?
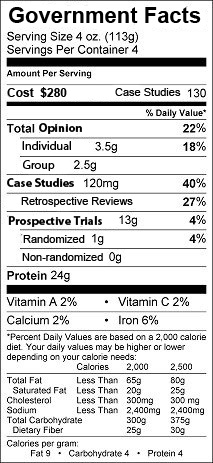
"In this in-depth analysis, we found that pacemaker patients with less severe electrical disturbance in their hearts did not receive any benefit whatsoever from these expensive and potentially risky implants. Given the abundance of data showing lack of efficacy in this patient population, current treatment guidelines should be changed."Wow. I'm speachless. Cause and effect to change medical practice from a meta-analysis! Since when?
Since never.
And how did the mainstream media interpret the study?
Here's a sample comical passage from a Consumer Reports article entitled "Many Heart Failure Patients Don't Benefit from Pacemakers:"
Current American Heart Association guidelines say that patients with a QRS (the measurement of the activity of the heart's left and right ventricles) of greater than 120 milliseconds should be treated with CRT (Cardiac Resynchrtonization Therapy). But the study found that patients with a QRS between 120 ms and 150 ms—38 percent of the participants—received little to no benefit from CRT. In contrast, the 60 percent of people who had a QRS of 150 or higher did benefit.Said another way, 38% (about 40%) of patients with QRS widths between 120-150 had no benefit to CRT pacing, and 40% of patients with QRS widths greater than 150 also had no benefit to CRT pacing. (Yet a remarkably large 60% of these very sick patients with or without wide QRS complexes - most NYHA Functional Class III - benefitted from the therapy.)
Yep. That's the real data: pre-procedure QRS width does not predict who will respond to biventricular pacing therapy clinically. Some will. Some will not. Truth is, we can't predict a priori which patients will respond to this form of pacing therapy for heart failure. To suggest (suddenly and miraculously) that QRS width can predict response from these poor data aggregations when numerous other studies have failed to show such an effect is an irresponsible leap.
Now, please guys, can we stop bashing the best form of heart failure therapy for patients with wide QRS complexes above and beyond our maximal medical therapy and move on to more important issues like bathing salt bans extolled by our AMA leadership today?
Now there's science!
-Wes
P.S.: (For a much calmer evaluation of the trial and the media's response, see Dr. John Mandrola's blog.)
Reference: Sipahi I, Carrigan TP, Rowland DY, Stambler B, Fang JC.
Impact of QRS Duration on Clinical Event Reduction With Cardiac Resynchronization Therapy - Meta-analysis of Randomized Controlled Trials
Archives of Internal Medicine Published online June 13, 2011.
Disclaimer: Dr. Fisher is on the speaker's bureau for the medical device companies Medtronic and Boston Scientific and earned $2000 from each company in the past year for that teaching. Also, he often cares for real patients with heart failure and, yes, earns a portion of his living implanting CRT devices as a board-certified cardiac electrophysiologist.






{kind=link}