I write on Saturday morning March 28, and right now there are two contrary strains about to collide. On the one hand, you have scientists reducing their death-rate predictions further and further, lopping off zeros by the day. On the other hand, this is accompanied by appalling levels of despotism, even to the point of National Guard checkpoints at state borders and restrictions on what you can buy even at “essential” stores. This gigantic gap between emerging professional medical consensus and appalling policy ignorance is revealing as never before the practical impossibility of scientific public policy.-Wes
Then you have the cascade of unintentional and unexpected outcomes of the rush to coerce. It began with Trump’s disastrous block on flights from Europe that sent millions scrambling for tickets and led to an unspeakable crush of people standing shoulder-to-shoulder at our nations’ airports, contradicting the demand that people social distance just when the virus was revealing itself as highly contagious. The very opposite of intended results!
That’s just the beginning. I doubt seriously that the political class in this country, as low a regard I have it, set out to destroy all that we call civilized life, instantly generating millions of unemployed workers and bankrupt businesses all around, not to mention a pandemic of utter hopelessness on the part of vast swaths of the world’s population. Still, this is what they have managed to achieve. This is what their pretense of knowledge – as opposed to actual wisdom – has unleashed on the world, with incalculable human cost.
As for economics, are we talking recession? Depression? Those words indicate cyclical changes in business conditions. My friend Gene Epstein suggests another term for what we are going through. The Great Suppression. There will be months, years, and decades in which to more clearly observe the countless ways in which the supressors piled error upon error, blockage upon blockage, to add to the grotesquery.
What truly should inspire us all right now are the grocers, pharmacists, truck drivers, manufacturers, doctors and nurses, construction workers, restaurant workers, service station attendants, webmasters, volunteers of all sorts, philanthropists, and specialists in a huge variety of essential professions who keep life functioning more or less. And let us not forget the “unessential” people (it’s an incorrect and vicious term) who have innovated ways around the Great Suppression to continue to serve others, keep the rent being paid, and food on their tables. They are the means of salvation out of this mess.
The market, hobbled and bludgeoned, still loves you.
As for the politicians, Andrew Cuomo has admitted some of the error. In a much-welcome change, he has even deregulated medical services. There’s just a hint of humility and humanity embedded in these statements and actions. We need more of that, vastly more, if only to contribute to calming things down long enough to gain some perspective, and, hopefully, some eventual realization that in the “land of the free and the home of the brave” a virus should be regarded as a disease to mitigate and cure, not an excuse to bludgeon life on earth as we know it.
Monday, March 30, 2020
The Great Suppression
Interesting opinion piece from the American Institute for Economic Research appeared online framing the "Great Suppression:"
Saturday, March 28, 2020
Adjusting to Our "New Normal"
It's hard to image what life was like a month ago since so much has changed. The world seems surreal right now: little to no traffic, the hustle and bustle of our cities gone, and the quiet. So much quiet.
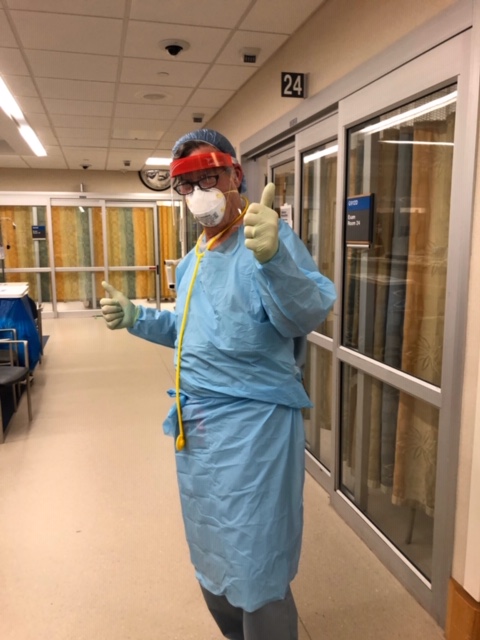
Life has changed significantly in our home, as I attempt to strip at my backdoor after returning from work, wash my hands, wipe my keys, phone, and wallet down, then head up stairs for a shower and change of clothes before familial reentry. I sleep in a different bedroom, shower in a different bathroom, and wonder (like a worker after the Chernobyl accident) what my viral "load" is at any point in time. Every accidentally-aspirated chicken noodle soup noodle and results in a coughing spree clears a room. I scratch my nose: "do I need to wash my hands again?"
Life as a physician is really weird now. We are healers and potential vectors all at the same time.
Yet so far we are lucky. Italy announced 969 deaths in a single day yesterday. Many, if not all of them, died alone. The ripple effect on their families must be enormous. And the poor doctors, nurses, health care workers there. New York is starting to feel this too. Will it get this bad here?
Our hospital system has been very proactive and open about the situation with us. They acknowledge the worldwide shortage of personal protective equipment (PPE). They are conserving necessary supplies for those most likely to confront new patients or those with suspected or confirmed COVID-19. All OR's and emergency procedures require full PPE, which is awkward when a non-COVID-19 patient enters: where is the transition to full PPE made? In the holding area? The lab itself? It's all a work in progress. Ventilators? Enough now, but later? Sands shift.
Still, it's impressive to see an ambulance bay converted to a negative flow screening area. Separate hospital's ICU and inpatient ward adapted for designated for COVID-19 patients. Contignecy plans for overflow are already in place. Outpatient drive-thru testing established for people who are most likely to warrant testing and have taken an online screening questionnaire. Six-foot markers are on the floor in the cafeteria, meetings, if they occur at all, are via Zoom or teleconference. Nearly all patient visits are virtual. Elective cases are a thing of the past. 425 physician volunteers are on standby - for extra duty - sometime.
At first, then percentage of people tested with positive coronavirus tests in 24 hrs was 15.8%, then 17.2%, and this AM was 19.1%. 7% of those hospitalized. Lots and lots of testing, planning, wondering, waiting. Today we admitted more people in a single day than everyone that was admitted when we started monitoring a week ago. It's coming.
The preparation seems so logical, but I wonder: will we be overwhelmed? We really don't know. But the non-COVID patients are still out there too: the LVAD patients with ICD shocks, the kids with broken bones, the baby deliveries, heart attacks, cancer patients, and patients with complete heart block, and more. They haven't stopped coming but they, too, are scared.
It's reassuring to see so many good folks giving it their all: from the doctors, nurses, administrative staff, clerical workers, laboratory staff, environmental workers, engineers and transporters. We work together - we have to - and with that effort comes the rekindling of respect for the special skills of everyone.
Once relatively simple things to treat take much more strategic coordination now. Atrial flutter w/rapid rate in a patient with fever and cough just a month ago would get a TEE/cardioversion without a moment's hesitation. Now, that patient is COVID-tested, isolated, procedures performed in full personal protective equipment, and tensions between colleagues heightened. The truth is, the vast majority of us that contract the disease will recover, but no one wants to be that other statistic. Patients need us. Families need us. So we wear a mask, we wash our hands, we wipe our tools, keys, keyboards, phones, then strip, wash and reenter. Are we effective? Honestly, I have no idea, but what else can we do?
Thanks to everyone who have sent prayers, words of encouragement, and support by staying home. We will all get thorough this.
Take care out there and take comfort in the fact that you're not alone.
 -Wes
-Wes
Life has changed significantly in our home, as I attempt to strip at my backdoor after returning from work, wash my hands, wipe my keys, phone, and wallet down, then head up stairs for a shower and change of clothes before familial reentry. I sleep in a different bedroom, shower in a different bathroom, and wonder (like a worker after the Chernobyl accident) what my viral "load" is at any point in time. Every accidentally-aspirated chicken noodle soup noodle and results in a coughing spree clears a room. I scratch my nose: "do I need to wash my hands again?"
Life as a physician is really weird now. We are healers and potential vectors all at the same time.
Yet so far we are lucky. Italy announced 969 deaths in a single day yesterday. Many, if not all of them, died alone. The ripple effect on their families must be enormous. And the poor doctors, nurses, health care workers there. New York is starting to feel this too. Will it get this bad here?
Our hospital system has been very proactive and open about the situation with us. They acknowledge the worldwide shortage of personal protective equipment (PPE). They are conserving necessary supplies for those most likely to confront new patients or those with suspected or confirmed COVID-19. All OR's and emergency procedures require full PPE, which is awkward when a non-COVID-19 patient enters: where is the transition to full PPE made? In the holding area? The lab itself? It's all a work in progress. Ventilators? Enough now, but later? Sands shift.
Still, it's impressive to see an ambulance bay converted to a negative flow screening area. Separate hospital's ICU and inpatient ward adapted for designated for COVID-19 patients. Contignecy plans for overflow are already in place. Outpatient drive-thru testing established for people who are most likely to warrant testing and have taken an online screening questionnaire. Six-foot markers are on the floor in the cafeteria, meetings, if they occur at all, are via Zoom or teleconference. Nearly all patient visits are virtual. Elective cases are a thing of the past. 425 physician volunteers are on standby - for extra duty - sometime.
At first, then percentage of people tested with positive coronavirus tests in 24 hrs was 15.8%, then 17.2%, and this AM was 19.1%. 7% of those hospitalized. Lots and lots of testing, planning, wondering, waiting. Today we admitted more people in a single day than everyone that was admitted when we started monitoring a week ago. It's coming.
The preparation seems so logical, but I wonder: will we be overwhelmed? We really don't know. But the non-COVID patients are still out there too: the LVAD patients with ICD shocks, the kids with broken bones, the baby deliveries, heart attacks, cancer patients, and patients with complete heart block, and more. They haven't stopped coming but they, too, are scared.
It's reassuring to see so many good folks giving it their all: from the doctors, nurses, administrative staff, clerical workers, laboratory staff, environmental workers, engineers and transporters. We work together - we have to - and with that effort comes the rekindling of respect for the special skills of everyone.
Once relatively simple things to treat take much more strategic coordination now. Atrial flutter w/rapid rate in a patient with fever and cough just a month ago would get a TEE/cardioversion without a moment's hesitation. Now, that patient is COVID-tested, isolated, procedures performed in full personal protective equipment, and tensions between colleagues heightened. The truth is, the vast majority of us that contract the disease will recover, but no one wants to be that other statistic. Patients need us. Families need us. So we wear a mask, we wash our hands, we wipe our tools, keys, keyboards, phones, then strip, wash and reenter. Are we effective? Honestly, I have no idea, but what else can we do?
Thanks to everyone who have sent prayers, words of encouragement, and support by staying home. We will all get thorough this.
Take care out there and take comfort in the fact that you're not alone.
Tuesday, March 17, 2020
The "Risk and Distraction" of MOC
We did not come to this decision lightly, but we believe removing the potential risk and distraction of sitting for a spring exam is the right thing to do for our diplomates and for the country at this time. Learn more: https://www.abim.org/media-center/Coronavirus-Updates.aspxPhysicians can help make sure this risky, unproven, and "distracting" ABMS board "maintenance of certification" (MOC) requirement never returns by supporting the plaintiffs working to end this monopolized program here.
-Wes
Saturday, February 08, 2020
MOC's Sword of Damocles and the Platinum Rule

It is clear that MOC has morphed into a money-making endeavor for legions of third parties, including insurance companies, hospitals, and a myriad of other corporate interests eager to capitalize on the control and sharing of physician data. While the concept of using the "Platinum Rule" to guide the evolution of MOC is a step in the right direction, the "MOC existential crisis" will not end until the "Sword of Damocles" (as the authors aptly put it) is removed from working physicians' heads. We simply cannot work with the threat of the loss of our professional careers if we fail to purchase the unproven MOC (and any other required "continuous certification" product).
The ABMS MOC paradigm will only survive if becomes truly voluntary and its lack of purchase will not affect our right to earn a living.
-Wes
P.S. (Updated 9 Feb 2020 @ 13:45PM CST) As we have seen time and time again, the physician influencers and apologists of the American Board of Medical Specialties (ABMS) have historically abandoned their moral imperative to working physicians and their patients to “first, do no harm.” Corporate interests invariably supersede this ethic. It should come as no surprise, then, that the lead author of this piece has a similar track record working for the National Football League.
Physicians wishing to support the plaintiffs in their ongoing effort to end Maintenance of Certification are encouraged to contribute here.
Tuesday, February 04, 2020
PA Medical Society and MOC
In 2016, the Pennsylvania Medical Society (PAMed) issued a strongly-worded "Vote of No Confidence" against the American Board of Internal Medicine (ABIM).
Good luck finding that earlier statement on PAMed's webpage concerning MOC now.
Instead, we see the following soothing pablum regarding PAMed's MOC position:
PAMED PositionThe accusations in PAMed's original 2016 Vote of No Confidence against the ABIM were significant:
Supports efforts to:
- Improve MOC
- Prohibit MOC as a condition of licensure, insurer credentialing and reimbursement, or hospital admitting privileges
" Through their marketing efforts, the ABIM has worked hard to give the impression that their recertification exam demonstrates competency. However, despite numerous calls to substantiate this assertion, the ABIM has been unable to provide reliable independent evidence that a secure, high-stakes exam, taken every 10 years by some and for which other are "grandfathered" and therefore exempt - leads to better patient care. This is because while the overwhelming majority of practicing physicians pass the ABIM recertification secure, high-stakes computer exams, this test and the MOC process have no correlation to how well a doctor can take care of a patient. Shockingly, countless medical leaders. numerous national mainstream publications, and several forensic accounting reviews have published information which suggests the ABIM's motivation for their recertification process was primarily driven by little more than financial mismanagement."In 2017, a resolution was passed by the AMA House of Delegates demanding an independent audit of the ABIM. This lead to the following response from the ABIM to James Madara, MD, President of the AMA. In that response by the ABIM, the American College of Cardiology was quoted as vouching for the ABIM's financial statements because of this statement issued to their membership:
In addition, the ACC's accounting staff have reviewed and discussed the ABIM’s publicly available financial statements with an outside accounting firm and have found the statements to be in compliance with Generally Accepted Accounting Principles, as utilized by not-for-profit organizations in the United States.The problem is, the AMA and the ACC have interests in selling physician data and each organization has representatives on the board of PCPI.org alongside representatives from UnitedHealthcare. PCPI and the ABMS share the same office address. Therefore, the financial "audit" demanded by the AMA House of Delegates in 2017 and accepted by the AMA's President Madara was never "independent."
Pennsylvania physicians represented by PAMed need to confront their medical society's current leadership concerning MOC and the lack of independent financial audit demanded by the AMA House of Delegates. One thing working physicians in Pennsylvania (and elsewhere) don't need: corporate physician shills more interested in themselves and their political aspirations than the support of front-line physicians who care for their citizens.
-Wes
Sunday, January 26, 2020
The Certified Deceit and Exploitation of US Physicians
For the past seven years, I have devoted a significant amount of my time to investigating and telling the true story of US physician "board certification." That story has been one of deceit, private back-room deals, profiteering, and (worst of all in my humble opinion), the exploitation of working physicians and the patients for whom they care.
This writing has not come without its personal and professional costs, but when the story is one that affects the corruption of the largest single contributor to the US economy, what else should I have expected?
As I reflect on what this side job has exposed, it would be naive and dishonest to suggest that physicians are exempt from bearing some responsibility for rising healthcare costs in America. But it may go much further than that: our medical profession and its hallowed physician education regulatory system comprised of the unchecked Accreditation Council for Graduate Medical Education (ACGME) might be the very reason things were allowed to become so out of control. Our non-profit tax laws with their opaque reporting requirements have allowed huge "non-profits" to go unchecked in America - and most of those "non-profits" are in healthcare. (Just take a stroll by the American Medical Association (AMA) building in downtown Chicago sometime to get a feel for the magnitude of the problem.)
Why should the physician education and credentialing systems in America be exempt from such corruption?
Well, they are not.
From the earliest reports of a multi-million dollar condominium purchase by the same non-profit organization that created the "Choosing Wisely®" campaign to promote health care cost savings, the hypocrisy of US board certification was laid bare. With not-so-difficult internet Google searches, it was just a matter of time before the multiple deep-pocketed corporate ties between US physician board certification and Big Tobacco, Big Insurance, Group Purchase Organizations, and the Health Care Quality and Safety Industry became evident. Even our most widely respected health care journals, many of which were owned by state medical societies or physician specialty societies, published innumerable articles with an editorial blind eye to these financial conflicts. Even the Chief Medical Officer of the American Board of Internal Medicine is just a hired corporate consultant. To that end, is it any wonder that the so-called "voluntary" ABMS board certification product is now anything but voluntary for physicians, as trillions of health care dollars exchange hands in hospitals and insurance companies whose corporations believed the published propaganda?
This is why the "Maintenance of Certification" (MOC) story must be told and understood. Continuing the cover-up only serves to fan the flames of physician burnout and risks loss of more frontline highly-trained physicians to other professions.
Thankfully, the true history of AMBS board certification was recently published online. But it was not published in a medical journal. It was published in the public Siva v. American Board of Radiology antitrust lawsuit case docket.
And what a complicated and tortuous story it tells.
It is a story of public deception.
It is a story of physician exploitation.
It is a story of greed.
It is a story of trying to use Maintenance of Certification to control state's sovereignty over medical licensure.
It is a story of money for bureaucrats, hospitals, and numerous corporate interests at the expense of the youngest and most vulnerable physicians.
It is a story of a sophisticated self-serving physician education and credentialing racket.
And now, you can read the 79-page story here.
Let's hope Judge Jorge Alonso (who initially dismissed the case against the American Board of Radiology) reads it, too.
-Wes
P.S.: Please consider supporting the Plaintiffs in their ongoing David vs Goliath MOC legal battles.
This writing has not come without its personal and professional costs, but when the story is one that affects the corruption of the largest single contributor to the US economy, what else should I have expected?
As I reflect on what this side job has exposed, it would be naive and dishonest to suggest that physicians are exempt from bearing some responsibility for rising healthcare costs in America. But it may go much further than that: our medical profession and its hallowed physician education regulatory system comprised of the unchecked Accreditation Council for Graduate Medical Education (ACGME) might be the very reason things were allowed to become so out of control. Our non-profit tax laws with their opaque reporting requirements have allowed huge "non-profits" to go unchecked in America - and most of those "non-profits" are in healthcare. (Just take a stroll by the American Medical Association (AMA) building in downtown Chicago sometime to get a feel for the magnitude of the problem.)
Why should the physician education and credentialing systems in America be exempt from such corruption?
Well, they are not.
From the earliest reports of a multi-million dollar condominium purchase by the same non-profit organization that created the "Choosing Wisely®" campaign to promote health care cost savings, the hypocrisy of US board certification was laid bare. With not-so-difficult internet Google searches, it was just a matter of time before the multiple deep-pocketed corporate ties between US physician board certification and Big Tobacco, Big Insurance, Group Purchase Organizations, and the Health Care Quality and Safety Industry became evident. Even our most widely respected health care journals, many of which were owned by state medical societies or physician specialty societies, published innumerable articles with an editorial blind eye to these financial conflicts. Even the Chief Medical Officer of the American Board of Internal Medicine is just a hired corporate consultant. To that end, is it any wonder that the so-called "voluntary" ABMS board certification product is now anything but voluntary for physicians, as trillions of health care dollars exchange hands in hospitals and insurance companies whose corporations believed the published propaganda?
This is why the "Maintenance of Certification" (MOC) story must be told and understood. Continuing the cover-up only serves to fan the flames of physician burnout and risks loss of more frontline highly-trained physicians to other professions.
Thankfully, the true history of AMBS board certification was recently published online. But it was not published in a medical journal. It was published in the public Siva v. American Board of Radiology antitrust lawsuit case docket.
And what a complicated and tortuous story it tells.
It is a story of public deception.
It is a story of physician exploitation.
It is a story of greed.
It is a story of trying to use Maintenance of Certification to control state's sovereignty over medical licensure.
It is a story of money for bureaucrats, hospitals, and numerous corporate interests at the expense of the youngest and most vulnerable physicians.
It is a story of a sophisticated self-serving physician education and credentialing racket.
And now, you can read the 79-page story here.
Let's hope Judge Jorge Alonso (who initially dismissed the case against the American Board of Radiology) reads it, too.
-Wes
P.S.: Please consider supporting the Plaintiffs in their ongoing David vs Goliath MOC legal battles.
Wednesday, January 15, 2020
Who Is the ABIM Chief Medical Officer?
 |
| Drs. Richard G. Battaglia and Richard Baron (Image from the ABIM Blog) |
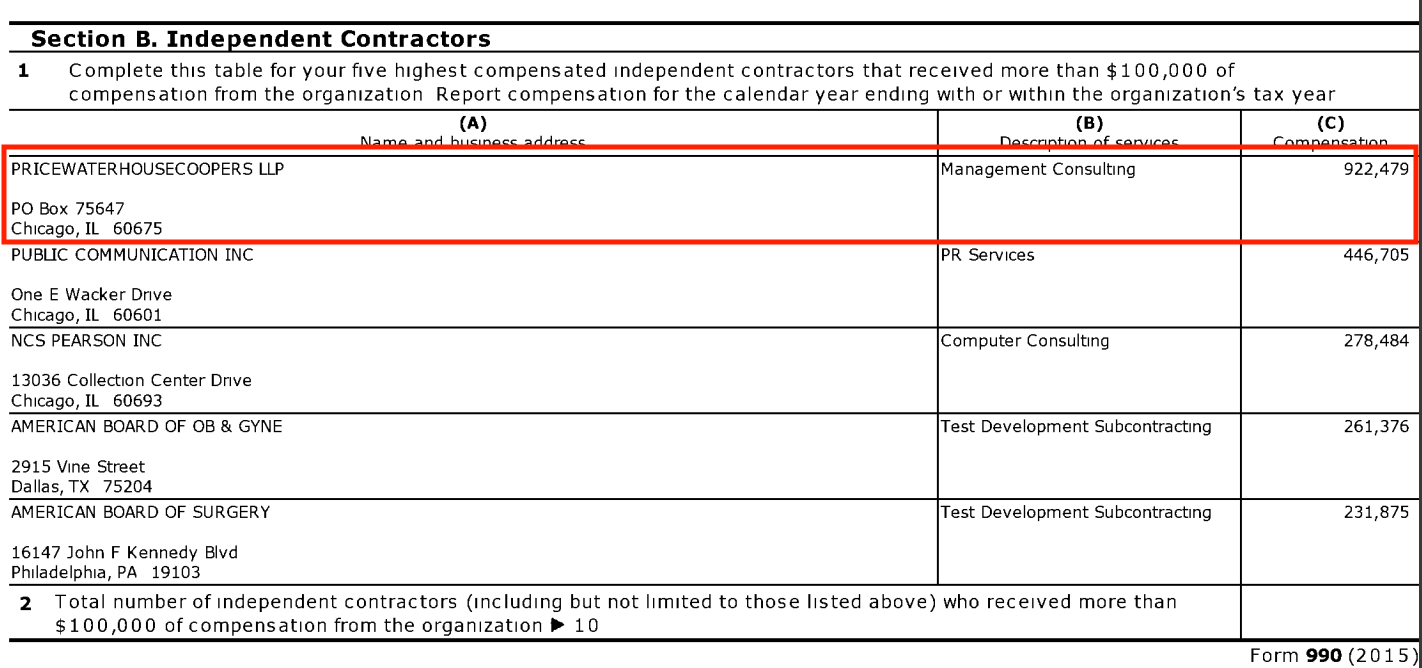
In 2015, the American Board of Internal Medicine (ABIM) announced Richard G. Battalgia, MD as their new Chief Medical Officer (CMO). This was the same year the American Board of Medical Specialties (ABMS) paid $922,479 to PriceWaterhouseCooper LLP (PwC) for "Management Consulting:"
Is Dr. Battaglia, the ABIM CMO, concerned about medical education of physicians or merely a consultant purchased by the American Board of Medical Specialties to "clean up" the ABIM Maintenance of Certification (MOC) mess?
The ABIM website only says this about their CMO:
"Dr. Battaglia, a board certified internist, is Chief Medical Officer (CMO) of the American Board of Internal Medicine (ABIM). There, he leads ABIM's effort to incorporate feedback from practicing physicians and key stakeholders into clinical aspects of all of ABIM activities, including Certification and Maintenance of Certification (MOC).Maybe PwC's "Unifying Thread" of using (physician) data is the real reason Dr. Battalia promotes "continuous certification" and MOC:
Previously, Dr. Battaglia served as a primary care internist with Health Care Plan/Univera, a multi-specialty, staff model practice in Western New York before transitioning into leadership roles, including Medical Director of the Medical Centers Division and Senior Vice President, Medical Affairs/Corporate Medical Director. He also served as Medical Director/Chief Medical Officer of large multispecialty medical groups in Western New York. He has participated in national quality initiatives focused on physician group practice and health maintenance organizations. For more than 10 years, he devoted time to The National Committee for Quality Assurance, including a term as Chairman of the committee charged with accreditation decision-making. Most recently, he was a consultant (emphasis mine) for national and international organizations, including academic medical centers, health systems, community hospitals, medical groups, payers and national physician certification organizations.
Dr. Battaglia received a biochemistry degree from Canisius College, a Jesuit institution in Buffalo, NY. He obtained his medical degree from the University of Rochester School of Medicine and Dentistry. Dr. Battaglia completed his residency through the University of Rochester Primary Care Program in Internal Medicine and also served as Chief Resident."
Data is the unifying thread across seven policy areas we highlight here. Privacy, antitrust, tax, regulation of artificial intelligence, and trade are converging around the collection, sharing and security of data.Physicians subjected to lifelong payments to ABMS member boards for Maintenance of Certification (MOC) and Continuous Certification (CC) should know about
When considering patient safety and care quality, a corporate, non-clinical, damage-control medical consultant for a Fortune 500 accounting firm should not be Chief Medical Officer of the American Board of Internal Medicine.
-Wes
Tuesday, January 14, 2020
Visible Cracks
it was a clinic day like all the rest
until it wasn't
she was there with her son and granddaughter
winded
legs swollen "for a month"
afib, fast rate despite cardizem CD 300 mg daily, diabetic meds, norvasc.
EKG with LVH, RBBB, LAFB.
BP 178/84, HR 124
rales
meds to be started, but help?
EMR->no doctor
a nurse practitioner?
4:45 pm-> all gone
see you in two days
no appointments.
i wake too early
staring up
mind swirling
cases ahead
remembering her
and me
alone.
-Wes
until it wasn't
she was there with her son and granddaughter
winded
legs swollen "for a month"
afib, fast rate despite cardizem CD 300 mg daily, diabetic meds, norvasc.
EKG with LVH, RBBB, LAFB.
BP 178/84, HR 124
rales
meds to be started, but help?
EMR->no doctor
a nurse practitioner?
4:45 pm-> all gone
see you in two days
no appointments.
i wake too early
staring up
mind swirling
cases ahead
remembering her
and me
alone.
-Wes
Monday, January 13, 2020
The Study We Weren't Supposed to See
Most US physicians are well-acquainted with the American Board if Internal Medicine's (ABIM) breathless claims of ABIM board certification and Maintenance of Certification's benefits. These have included:
These are their words, not mine.
Where are these results published on the ABIM or ABIM Foundation website?
Shouldn't U.S. physicians who paid for such poorly conducted/self-promotional "research" be entitled to disclosure of (1) how much granbt money was paid to USUHS, (2) why the funding agency was allowed authorship of this "research," and (3) why the data contained in this work were not disclosed to ABIM diplomates on the ABIM website?
-Wes
Please contribute to help support the legal effort to end Maintenance of Certification nationwide.
- The Public Expects It
- Physicians Value It
- Amount of clinical experience does not necessarily lead to better outcomes or improvement of skills
- Certification is Associated with Better Care
- "lead to higher measures of depersonalization and emotional exhaustion."
- "may be an important source of medical errors related to clinical reasoning tasks in practice."
- yet are considered the "Gold Standard of physician performance."
These are their words, not mine.
Where are these results published on the ABIM or ABIM Foundation website?
Shouldn't U.S. physicians who paid for such poorly conducted/self-promotional "research" be entitled to disclosure of (1) how much granbt money was paid to USUHS, (2) why the funding agency was allowed authorship of this "research," and (3) why the data contained in this work were not disclosed to ABIM diplomates on the ABIM website?
-Wes
Please contribute to help support the legal effort to end Maintenance of Certification nationwide.
Monday, December 30, 2019
ABIM Antitrust/RICO Lawsuit Notice of Appeal Filed

Working physicians can help the plaintiffs in their David-versus-Goliath effort to end the unproven American Board of Medical Specialties' MOC program by contributing to Practicing Physicians of America's GoFundMe page created on their behalf. We have almost reached our $400,000 goal. (Your contribution may be tax deductible before year's end - please consult your tax advisor.)
-Wes
Thursday, December 12, 2019
Just In Time for Christmas: The MOC Legal Juggernaut Intensifies
With the recent back-to-back announcements that the class action antitrust and racketeering lawsuit against the American Board of Internal Medicine (ABIM) and the antitrust lawsuit against the American Board of Radiology were dismissed (e.g., the ABIM announcement and ABR announcement), doctors everywhere - both young and old - seemed resigned to the fact that they will have to be subjects to lifelong extortion of private American Board of Medical Specialties member boards and their affiliates if they wanted to practice medicine in the United States.
But fear not, dear colleagues. I bring you tidings of great joy. The first great Supplemental Opposition to the Motion to Dismiss the lawsuit against the American Board of Psychiatry and Neurology (ABPN) was filed yesterday that promises to renew the call for justice on the basis of proper legal procedural grounds:
We can anticipate that the multitude of moneyed interests behind Maintenance of Certification will stop at nothing to assure this unlawful program continues unchecked.
Still, a bit of hope and cheer is always welcome for working physicians this time of year.
Merry Christmas!
-Wes
P.S.: On a separate legal note:
Remember the Puerto Rican physician, Jaime Salas Rushford, MD, whom the ABIM revoked his board certification and dragged him through the court system since 2012 with a dismissed time-barred cheating claim while the President and CEO of the ABIM simultaneously failed to disclose her conflicts of interest with Kaiser and Premier Inc? Yesterday, the judge issued the following order to expedite the counterclaim suit filed against ABIM by Salas Rushford:
Readers wishing to support the brave physician plaintiffs involved in these lawsuits trying to end the unlawful Maintenance of Certification program are encouraged to contribute to their GoFundMe campaign.
But fear not, dear colleagues. I bring you tidings of great joy. The first great Supplemental Opposition to the Motion to Dismiss the lawsuit against the American Board of Psychiatry and Neurology (ABPN) was filed yesterday that promises to renew the call for justice on the basis of proper legal procedural grounds:
Defendant American Board of Psychiatry and Neurology (“ABPN”) illegally ties its initial certification product, which it sells to new doctors to demonstrate completion of their medical education and assess the quality of their residency program, and its MOC product, which it requires some older doctors, but not all, to purchase throughout their careers to demonstrate lifetime learning or forfeit their initial certification. ABPN brings to the court’s attention Kenney v. American Board of Internal Medicine, No. 18-5260, 2019 U.S. Dist. LEXIS 164725 (E.D. Pa.Sept. 26, 2019) (“Kenney”), and Siva v. American Board of Radiology, No. 19 C 1407, 2019 U.S. Dist. LEXIS 200645 (N.D. Ill. Nov. 19, 2019) (“Siva”). Kenney came first, followed by Siva which “agree[d] with the reasoning in Kenney.” Id. at *11.1The supplemental opposition to the ABPN motion to dismiss then outlines multiple legal reasons why the plaintiffs believe the decisions were wrongly decided. In essence, the attorneys are arguing that the facts in this case were not even allowed to be considered past the judges' chambers.
Nothing in those opinions changes ABPN’s unlawful conduct. A critical reading of the opinions and application of the universally accepted rule that well-pleaded factual allegations and all reasonable inferences therefrom must be taken as true compels the conclusion that Kenney and Siva were, respectfully, wrongly decided.1 The tying claims in Kenney were dismissed with prejudice without plaintiffs being allowed to amend, the court finding as a matter of law that separate products could never be alleged. Plaintiffs are appealing that ruling. The claims in Siva were dismissed without prejudice and plaintiff is filing an amended complaint on January 10, 2020.
We can anticipate that the multitude of moneyed interests behind Maintenance of Certification will stop at nothing to assure this unlawful program continues unchecked.
Still, a bit of hope and cheer is always welcome for working physicians this time of year.
Merry Christmas!
-Wes
P.S.: On a separate legal note:
Remember the Puerto Rican physician, Jaime Salas Rushford, MD, whom the ABIM revoked his board certification and dragged him through the court system since 2012 with a dismissed time-barred cheating claim while the President and CEO of the ABIM simultaneously failed to disclose her conflicts of interest with Kaiser and Premier Inc? Yesterday, the judge issued the following order to expedite the counterclaim suit filed against ABIM by Salas Rushford:
The American Board of Internal Medicine may file its motion for judgment on the pleadings no later than December 18, 2019. Dr. Salas-Rushford will respond no later than January 2, 2020. The Board may reply no later than January 9, 2020. The case schedule will be discussed at the scheduling conference to be held on January 31, 2020. Signed by Judge Francisco A. Besosa on 12/11/2019. (brc) (Entered: 12/11/2019)It seems that case will soon be coming to a head, too.
Readers wishing to support the brave physician plaintiffs involved in these lawsuits trying to end the unlawful Maintenance of Certification program are encouraged to contribute to their GoFundMe campaign.
Wednesday, December 04, 2019
ABIM's Dark Side Needs More Light
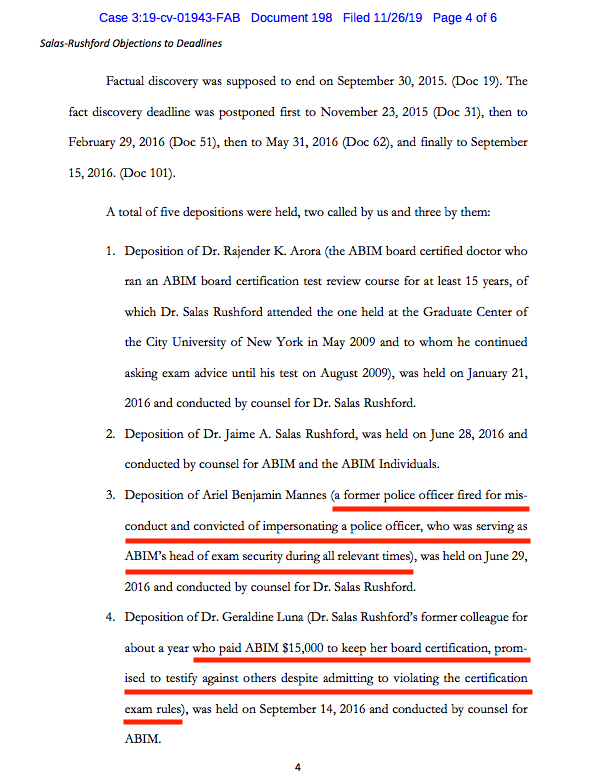
From the recently filed "Objections to Deadlines due to Completion of Discovery" by Plaintiff Jaimie Salas Rushford, MD in Puerto Rico Federal Court comes public evidence of mafia-like tactics used against physicians by the American Board of Internal Medicine (ABIM) to protect their certification testing monopoly:
So to summarize some of what has transpired at the ABIM to maintain their physician testing monopoly:
 |
| (Click image to enlarge) |
So to summarize some of what has transpired at the ABIM to maintain their physician testing monopoly:
- The ABIM secretly created the ABIM Foundation in 1989 for the purpose of laundering over $70 million of physician testing fees from 1990-2007 for various personal and political agendas, including the purchase of a 2-bedroom luxury condominium, art collection, and offshoring of Cayman Island retirement funds.
- They published a white paper in 2002 in two major medical journals, the Annals of Internal Medicine and the Lancet, entitled "Medical Professionalism in the New Millennium: A Physician Charter" (which, given these revelations, should both be retracted in my opinion).
- They used a strongman convicted of impersonating a police officer and carrying an unregistered firearm as their Director of Test Security with access to physicians' most sensitive personal information.
- They forced a physician who admitted to wrongdoing to pay $15,000 to remain board certified on the condition that physician also serve as an informant.
- They continue to drag a vulnerable physician through the court system for what will be at least eight years to maintain their monopoly and hide the truth.
The American Board of Internal Medicine needs to be held accountable to working US physicians and the public for their actions. I believe their irresponsible and undisclosed financial and political dealings, paired with these mafia-like tactics, deserve full transparency and appropriate judicial scrutiny.
Physicians deserve better. The public deserves better.
It's past time we shine a bright light on this racket.
-Wes
Saturday, November 30, 2019
Watching Our Healthcare Hindenburg Burn
Just before Thanksgiving, 15 physicians were notified they will be replaced by less-experienced and cheaper nurse practitioners at the nearly $1 billion Edwards-Elmhurst healthcare system here in Chicago. Doctors, the article says, were "broadsided," perhaps because they were naive to events that occurred in Springfield, IL earlier this year. Thanks to aggressive lobbying, recent legislation was unanimously passed in both the House and Senate Illinois legislature allowing nurse practitioners to practice independently of physicians in any capacity except surgery. Working doctors likely missed this since they don't populate legislative halls - they populate clinics and hospitals caring for patients - or at least most did.
This trend of using more and more nurse practitioners in lieu of physicians appears to be accelerating nationwide as large hospital systems or consolidated primary care clinics with bloated numbers of midlevel administrators look to cut costs. Nurse practitioners are everywhere now: staffing ICUs, Emergency Rooms, and yes, primary care clinics. Some nurse practitioners are used to preferentially fill lucrative surgical pipelines armed with little other knowledge than what a routine case for surgery requires. And while advanced practice nurse practitioners do treat common ailments like earaches and sore throats, often quite well, how many can recognize the warning signs of a case of epiglottitis? What happens to patients then?
Is compromising years of physician training and care experience for cost efficiency really about patient care or cost savings or a facility's bottom line? Is the inevitable pitting of nurses against doctors in the patient's best interest or the institution's? Who sees the costs supposedly saved by hiring cheaper advanced practice nurses? Will Edward-Elmhurst Healthsystem suddenly stop spending millions on collection agents who served as second-largest contractor for Edward-Elmhurst Healthsystem in Fiscal Year 2018?
Working physicians aren't without some blame either. Where were the physicians on the Medical Executive Committee of Edward-Elmhurst Healthsystem with this announcement? Did they approve replacing 15 physician-colleagues for lesser-trained nurse practitioners or fearful of losing their jobs if they didn't "align" themselves with this administrative move? Who is advocating for patients at Edward-Elmhurst Healthsystem (or any other large non-physician run hospital system) now? Anyone?
Can Dr. Google and inexperienced physician posers safely replace the highly trained, experienced physician? No one really knows. This latest move is little more than a grand experiment promoted by healthcare consultants with patients' lives on the line. Which leads us to ask: is touting a shortage of US physicians really a concern of the Association of American Medical Colleges or just a ploy by other member organizations of Accreditation Council for Graduate Medical Education (like the American Hospital Association) to justify these physician firings so hospitals can pad their bottom line?
Our Healthcare Hindenburg is burning: a bubble of excessive prices, high middleman salaries, a rapidly accelerating physician shortage, competition of healthsystems and patients increasingly unable to pay even basic co-pays for healthcare, medications, and procedures, as they are left to take the financial hit to maintain the health care industrial complex's status quo.
In healthcare, it's "Winner Takes All" with the likes of PriceWaterHouseCooper, McKinsey, and the Advisory Board at the helm. The competition is fierce.
Patients (and their better-trained frontline physicians) be damned.
-Wes
This trend of using more and more nurse practitioners in lieu of physicians appears to be accelerating nationwide as large hospital systems or consolidated primary care clinics with bloated numbers of midlevel administrators look to cut costs. Nurse practitioners are everywhere now: staffing ICUs, Emergency Rooms, and yes, primary care clinics. Some nurse practitioners are used to preferentially fill lucrative surgical pipelines armed with little other knowledge than what a routine case for surgery requires. And while advanced practice nurse practitioners do treat common ailments like earaches and sore throats, often quite well, how many can recognize the warning signs of a case of epiglottitis? What happens to patients then?
Is compromising years of physician training and care experience for cost efficiency really about patient care or cost savings or a facility's bottom line? Is the inevitable pitting of nurses against doctors in the patient's best interest or the institution's? Who sees the costs supposedly saved by hiring cheaper advanced practice nurses? Will Edward-Elmhurst Healthsystem suddenly stop spending millions on collection agents who served as second-largest contractor for Edward-Elmhurst Healthsystem in Fiscal Year 2018?
Working physicians aren't without some blame either. Where were the physicians on the Medical Executive Committee of Edward-Elmhurst Healthsystem with this announcement? Did they approve replacing 15 physician-colleagues for lesser-trained nurse practitioners or fearful of losing their jobs if they didn't "align" themselves with this administrative move? Who is advocating for patients at Edward-Elmhurst Healthsystem (or any other large non-physician run hospital system) now? Anyone?
Can Dr. Google and inexperienced physician posers safely replace the highly trained, experienced physician? No one really knows. This latest move is little more than a grand experiment promoted by healthcare consultants with patients' lives on the line. Which leads us to ask: is touting a shortage of US physicians really a concern of the Association of American Medical Colleges or just a ploy by other member organizations of Accreditation Council for Graduate Medical Education (like the American Hospital Association) to justify these physician firings so hospitals can pad their bottom line?
Our Healthcare Hindenburg is burning: a bubble of excessive prices, high middleman salaries, a rapidly accelerating physician shortage, competition of healthsystems and patients increasingly unable to pay even basic co-pays for healthcare, medications, and procedures, as they are left to take the financial hit to maintain the health care industrial complex's status quo.
In healthcare, it's "Winner Takes All" with the likes of PriceWaterHouseCooper, McKinsey, and the Advisory Board at the helm. The competition is fierce.
Patients (and their better-trained frontline physicians) be damned.
-Wes
Sunday, November 24, 2019
The AMA and ABMS Member Boards: Banking on the Promise of Private Equity
Recently, I was sent a prospectus for a medical device company that caught the eye of a local Venture Capital funding group. On that prospectus was this paragraph for a "vision" of future of a "clinical decision support system:"
In short, this is what health care market investors see now: a vision where fewer staff, more data entry, and less humanity and human touch are sold as better health care. Worse still, working physicians who remain are being grown and matured in a muzzled petri dish where dissent is openly discouraged by employers and "certifying" bodies.
This data-driven model didn't work out so well for Boeing.
And it won't work so well for health care either.
But don't tell that to the American Medical Association. Because to the AMA, working physicians in the US are little more than data entry ports "Moving Medicine" toward the AMA's latest vision for a business-oriented private equity-driven health care model for tomorrow.
-Wes
Collects data from the electronic medical record, medical literature, regulatory warnings and other internet-based public information. Provides analysis of intra-procedural progress that integrates this data with procedural imaging and patient status. Includes predictive analytics with the use of cognitive computing to support optimal clinical decision making."This pitch was little more than a marketed promise of artificial intelligence, of instant processing of black-box algorithms, of equity funding to solve healthcare's less-than optimal patient outcomes using the internet, numbers, cut-copy-and-paste data entry, physician testing scores, in one big algorithmic, dehumanized, robotic mess.
In short, this is what health care market investors see now: a vision where fewer staff, more data entry, and less humanity and human touch are sold as better health care. Worse still, working physicians who remain are being grown and matured in a muzzled petri dish where dissent is openly discouraged by employers and "certifying" bodies.
This data-driven model didn't work out so well for Boeing.
And it won't work so well for health care either.
But don't tell that to the American Medical Association. Because to the AMA, working physicians in the US are little more than data entry ports "Moving Medicine" toward the AMA's latest vision for a business-oriented private equity-driven health care model for tomorrow.
-Wes
Friday, November 15, 2019
Timeline for Justice: ABIM v Salas Rushford

Over three years later, he received a letter from Ms. Lynn O. Langdon, Chief Operating Office of the ABIM at the time, that his board certification was suddenly, indefinitely revoked because of claims he "collected and compiled hundred of ABIM examination questions from multiple sources" and that he "sent hundreds of ABIM examination questions" from his email to Arora Board Review. The letter implied he did "not maintain moral, ethical, or professional behavior satisfactory to the Board," engaged in "misconduct adversely affecting " his integrity, and engaged in "behavior that subverts the examination process."
Because the ABIM felt he violated their "Pledge of Honesty," the Board elected to "indefinitely revoke" his certification and "notify the Medical Board in every jurisdiction" that he was licensed.
He had 10 days to appeal that decision through a never-disclosed ABIM "three-stage appeal process" that lasted two years. Following this, he later discovered the ABIM had filed a copyright infringement lawsuit against him.
He describes the ordeal in detail here. In that description, he notes the additional reprimanding of some "2700 physicians," the use of a "spy" sent to the board review course he attended, the secret funneling of millions of dollars of ABIM Diplomate testing fees to create the ABIM Foundation, the raid using federal Marshals of Dr. Arora's home to copy computer files and secure physician's email addresses, and the undisclosed conflicts of interest of Christine Cassel, MD, former President and CEO of the ABIM, none of which were known to Diplomates of the ABIM at the time.
Instead, the ABIM issued a press release that was picked up by the Wall Street Journal and shocked the medical community on June 9, 2010, detailing the sanctioning of 139 physicians for claims of "cheating:"
"Any high-school kid knows that cheating is unfair," said Dr. Christine Cassel, president and chief executive of the ABIM, who called the sanctions "a message and a deterrent."The ABIM subsequently lost the copyright infringement lawsuit against Salas Rushford, but his counterclaim lawsuit filed against the ABIM goes on after being recently moved to Puerto Rico Federal District Court.
The ABIM's move springs from a case involving test-prep firm Arora Board Review, which it sued last year. The ABIM's suit alleged that Arora instructors told class members the review questions were from the actual exam and solicited them to supply the company with additional questions they remembered after taking certification exams.
The ABIM and an attorney for Livingston, N.J.-based Arora both said they are in settlement talks. Arora's website says it has "put [its] business on hold until a settlement is reached in the near future."
Materials seized from Arora in December as part of the case included 2,000 emails and audio and other communications from physicians disclosing exam questions, according to the ABIM.
Based on these materials, the ABIM sued Monica Mukherjee of Washington, D.C.; Anastassia Todor of Aurora, Colo.; Pedram Salehi of Los Angeles; Sarah Von Muller of Tulsa, Okla.; and Frederick Oni of Warner Robins, Ga.
Dr. Mukherjee couldn't be reached for comment. Dr. Todor and Dr. Salehi had no comment. Dr. Oni said he didn't know the questions he purchased were from previous tests.
Dr. Von Muller said courses like Arora's are necessary for busy physicians attempting to get their optional board certification.
Dr. Cassel said she doesn't believe sharing or selling actual questions is common. "We have a great deal of confidence that most people don't cheat on this exam," she said, adding that there are "legitimate board-review programs that continue to function." (The ABIM doesn't offer its own review courses.)
The "hundreds" of allegedly infringing questions used by the course were removed from the pool of questions used on the computerized tests starting in 2009. Doctors who took the Arora course but weren't sanctioned or sued will get letters of reprimand, the ABIM said.
On 7 Nov 2019, the case management order for this lawsuit was published by the federal judge Francisco A. Besosa with the following timeline:
- 29 Nov 2019 - Objections to Case Management Deadlines and all outstanding pleadings due.
- 3 Dec 2019 - Motions to amend the pleadings or add parties to be filed.
- 31 Jan 2020 - initial Case Management and Settlement Conference
- 29 May 2020 - Motions to Dismiss must be filed
- 30 Dec 2020 - All discovery must be completed
- 9 Apr 2021 - Pretrial and Settlement Conference
- 19 Apr 2021 - Trial Shall Begin (09:00AM)
Perhaps now light will shine on the inner dealings of the so-called "voluntary" US Physician Board Certification process that has harmed practicing physicians without accountability or means of due process for years.
-Wes
Tuesday, November 12, 2019
Is CMS's Value-Based Healthcare System Already Being Gamed?
Take a look at the address of the American Board of Medical Specialties (ABMS) that owns the Maintenance of Certification (MOC®) trademark that is the subject of at least six anti-trust lawsuits (see here, here, and here for instance) underway because MOC binds physicians to their hospital privileges and insurance payments to made to hospitals on behalf of their employed physicians:
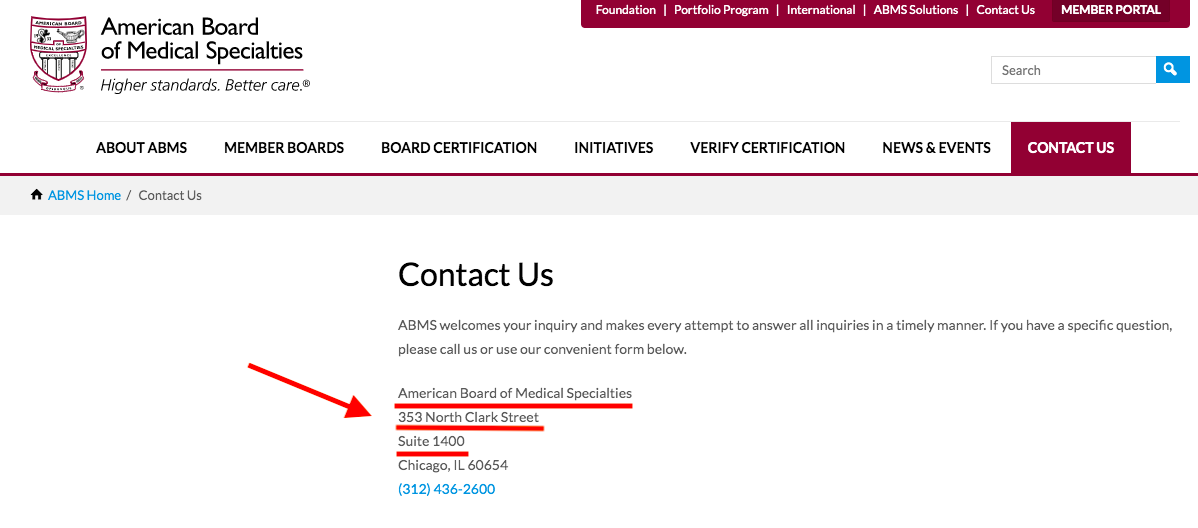
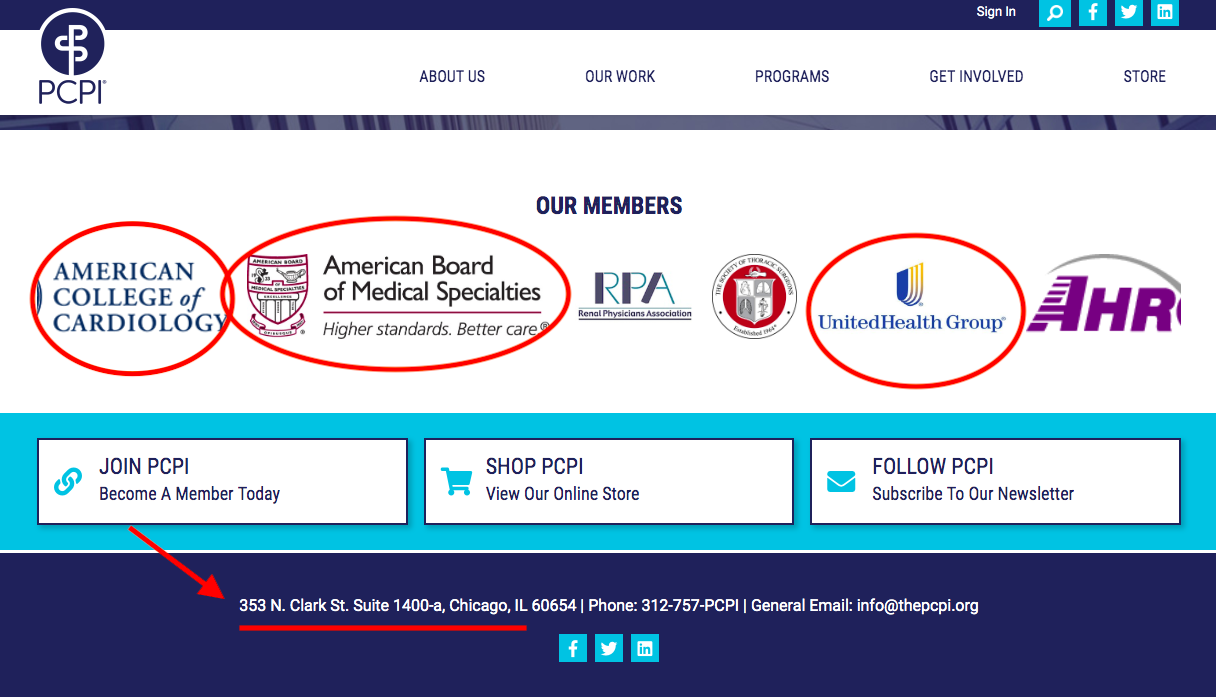
Now look at the address of the American Medical Association (AMA)-sponsored PCPI Foundation with board members from UnitedHealthcare, Premier, the American College of Cardiology, the American College of Physicians, several trustees of the AMA, and others:
Recall that the AMA maintains a monopoly on the procedure codes (CPT® codes) for every medical procedure performed in the United States and sells the rights to use that database to insurers and electronic medical record companies. Each of the AMA codes, then, have particular "value" to hospitals and insurers.
The AMA also determines the "relative value system" used by the government coding for weighting physician compensation that strongly incentivizes physician behavior. Some procedures, then, have more "value" to physicians than others. Hospitals know this, too.
Gee, I wonder, with all these codes and friends that stand to profit on the backs of working physicians and our patients, is the Affordable Care Act's value-based healthcare already being gamed?
-Wes
Now look at the address of the American Medical Association (AMA)-sponsored PCPI Foundation with board members from UnitedHealthcare, Premier, the American College of Cardiology, the American College of Physicians, several trustees of the AMA, and others:
Recall that the AMA maintains a monopoly on the procedure codes (CPT® codes) for every medical procedure performed in the United States and sells the rights to use that database to insurers and electronic medical record companies. Each of the AMA codes, then, have particular "value" to hospitals and insurers.
The AMA also determines the "relative value system" used by the government coding for weighting physician compensation that strongly incentivizes physician behavior. Some procedures, then, have more "value" to physicians than others. Hospitals know this, too.
Gee, I wonder, with all these codes and friends that stand to profit on the backs of working physicians and our patients, is the Affordable Care Act's value-based healthcare already being gamed?
-Wes
Saturday, November 09, 2019
MOC®: It's All About Physician Data

Because patients do not give consent for the use of their data, who better to target for access to sensitive patient-related information than those entrusted with their care? As details come to light about the American Board of Medical Specialties' (ABMS) Maintenance of Certification (MOC) program that has plagued physicians since 1990, many similarities to the Cambridge Analytica data-sharing scandal are appearing. The adhesion contract that forms the basis for MOC and is increasingly tied to physician hospital privileges and insurance reimbursements, assures this data pipeline remains open:
I also understand that ABIM may use my examination performance, training program evaluations, self evaluations of knowledge and practice assessment, and other information for research purposes, including collaboration with other research investigators and scientific publications."Unbeknownst to most physicians, the ABMS has been involved with the sale and sharing of physicians' demographic and sensitive MOC data with third parties for years. Each clinical physician in the United States may see 2000-3000 patient's each annually. Marrying physician data with their patient's data and targeting patient markets becomes possible with physician-specific MOC information. Procedural and pharmaceutical data allows medical suppliers, pharmaceutical companies, device companies, and others virtually unlimited opportunities to sell their products while optimizing most their bottom lines through increased sales and offering rebates to health care facilities (aka, kickbacks).
Group purchase organizations (GPOs) and Pharmacy Benefit Managers (PBMs) decide what equipment appears on a database for hospitals to purchase. Companies pay those GPOs and PBMs to be on the list. Doctors' equipment choices and pharmaceutical preferences influence that list. Companies want to know what doctors are using and who doctors are seeing. By knowing their patterns and knowing the procedures performed on patients, highly sensitive patient information can be deduced. Registries owned by procedurally-heavy specialty societies (like the American College of Cardiology) are a particularly ripe source of procedural data, particularly when it can be made doctor-specific (where MOC comes in). More data sales occur. Repeated MOC testing and demographic data entries required by physicians assures these physician-specific databases are kept current. Having the President and CEO of the American Board of Internal Medicine on the President's Council of Advisors for Science and Technology assured uninterrupted marketing access to physicians and their patients.
By using physician information and their patient care information for these corporate purposes, the ABMS/ABIM MOC® product looks more like Cambridge Analytica than a physician education tool and affects far more people's health care than the Cambride Analytica ever did.
So how how do all these organizations coordinate and connect their MOC data, registries, and corporate databases?
Through a virtually undisclosed tax-exempt AMA-funded private foundation shamelessly called the Physician Consortium for Performance Improvement (PCPI).
Reportedly formed in 2000 with the help of the AMA, the PCPI Foundation is located just blocks away from the AMA's corporate headquarters in downtown Chicago. The organization describes itself as follows:
The AMA-convened PCPI, in partnership with its members, has developed more than 350 measures, many of which are used in the Physician Quality Reporting System (PQRS) and Meaningful Use, as well as private health plan payment models. (emphasis mine)Not surprisingly, it's Board of Directors is lead by John S. McIntyre, MD of the American Psychiatric Association, who has never participated in MOC and is not required to do so:
In 2011, American Medical Association staff to the PCPI worked with a group of committed volunteer leaders to launch the NQRN®, a national, multi-stakeholder network of clinical registry stewards and others interested in registries. The NQRN has created tools and educational opportunities and increased the visibility and value of clinical registries as reporting and improvement systems. In 2016 NQRN was merged into the PCPI as a key program. In 2013, the AMA-convened PCPI launched the PCPI Quality Improvement Program to support its members improvement needs beyond measurement.
In 2014, the AMA and AMA-convened PCPI leadership undertook an evaluation to determine the optimal governance structure to meet the growing demand for value-based health care. The result of this evaluation was the adoption of new By-Laws in June 2015, which set the course for the PCPI Foundation (PCPI), an independent organization with an expanded membership.

The remainder of the Board of Directors include:
- Thomas Granatir, MD, Senior Vice President for Policy and "External Relations" of the ABMS (formerly from Humana)
- Lewis G. Sandy MD, FACP of the UnitedHealth Group
- Non-physician Nancy E. Lundebjerg, MPA of the American Geriatric Society (Vice Chair)
- Non-physician Laura J. Cranston, RPh of the Pharmacy Quality Alliance (Secretary)
- Non-physician Dianne V. Jewell PT, DPT, PhD, FAPTA of the American Physical Therapy Association (Treasurer)
- Larry A. Allen, MD, MHS of the American Heart Association
- Bruce S. Auerbach MD, FAECP of the American College of Emergency Physicians
- Arlene S. Bierman MD, MS of the Agency for Healthcare Research and Quality
- Claire Bradley, MD, MPH who oversees "Quality Improvement"
- Non-physician Carol A Cronin MA, MSW of the Informed Patient Institute
- Non-physician Melissa Danforth of the Leapfrog Group
- E. Scott Ferguson, MD - A radiologist on the AMA Board of Trustees and AMA representative to the National Quality Forum but does not appear to participate in MOC.
- Deeraj Mahajan, MD FACP, CMD, CIC, CHCQM ("Certified Medical Doctor, Certified Infection Control, Certified Health Care Quality Measures") of the Medical Specialty
- Lawyer Melanie G. Phelps JD of the North Carolina Medical Society who previously worked in the Government Affairs Department of Blue Cross Blue Shield
- Non-physician Aisha T. Pittman MPH of Premier, Inc, the largest hospital Group Purchase Organization
- Amir Qaseem MD, PhD, MHA, FACP of the American College of Physicians
- Martha J. Radford, MD FACC, FAHA of the American College of Cardiology
- David Shahian MD of the Society of Thoracic Surgeons
- Computer Scientist Kurt Skifstad, PhD CEO of ArborMetrix, a data analytics company
- Sandra Adamson Fryhofer, MD MACP from the Board of Trustees of the AMA
- Richard D. Zorowitz MD, FAAPMR of the American Academy of Physician Medicine and Rehabilitation
Members get to "access the latest tools and insights on performance measurement, clinical registries, and quality improvement" as well as "influence through representation on the PCPI board, committees, advisory and other, as well as expert panels and task forces."
Members of this organization, according to the revolving banner on the PCPI website, include:
AvaMed, FigMD (MOC data collectors), AMA, ACP, ACC, ABMS, Informed Patient Institute, CMSS, Am Society of Clinical Oncology, The American Health Quality Association, Am College of Occupational Medicine, Primaris (A healthcare consulting and data abstraction company), American Academy Foot and Ankle Orthopedics Society, UnitedHealth Group (Market cap: $262B), The Society of Thoracic Surgeons, Pharmacy Quality Alliance, American Gastroenterology Association, Health Care Services Platform, American Optometric Association, Academy of Nutrition and Dietetics, American Heart Association, American College of Radiology, and on, and on...
It's handsomely paid CEO and Executive Director, Kevin Donnelly, is a non-physician, too. Here's their latest 2017 IRS filing that confirms a cool $2.78M contribution from the AMA to the PCPI and contains this explanation why the organization is not a true public "charity" after all:
The organization is filing this 990PF after the extended due date of November 15, 2018 (extension was for Form 990). Upon completion of schedule it was determined that the public support test had not been met for the second year. Research into IRS code and regulations was done to determine the next steps, which took the organization past the due date. The organization did not intentionally disregard the filing requirement, but rather, took time to ensure that that (sic) the appropriate filings were being made. Going forward, now that the requirements are understood, all 990PF filings will be timely. Additionally the organization properly extended the 2018 return as fling a Form 990PF.I'm sensing some BS here, but I'll leave that to my readers (and the IRS) to decide.
Are UnitedHealth, Humana, Blue Cross Blue Shield, Premier, AvaMed (and all the medical device companies they represent), FigMD, and Primaris really about "quality" or their own bottom line?
Is there any wonder, then, that when a physician points out certain conflicts to medical editors of the Journal of the American Medical Association (JAMA) or the New England Journal of Medicine (owned by the Massachusetts Medical Society), he can't get a straight answer and is referred by the conflicted party to IRS tax filings?
One thing's for sure, to the best of my knowledge and belief, these multiple organizations are colluding with each other for their own best interests ("covert rationing" - a concept coined by the prescient Dr. Richard Fogoros) and using our physician MOC® data to drive their bottom lines while hiding behind non-profit tax law and the ruse of assuring the public it's all in the name of "quality."
-Wes
Wednesday, October 30, 2019
What Gives?
WHAT GIVES the American Board of Internal Medicine the ability to take away years of schooling, mountains of prior testing, sleepless nights of residency, and months of study for initial Board certification that we all had to pass?
WHAT GIVES the American Board of Internal Medicine the authority to magically un-certify physicians for not purchasing or their Maintenance of Certification program?
WHAT GIVES the American Board of Internal Medicine the right to take away over 25 years of my expertise with catheter ablation or pacemaker implantation when they've never once examined the quality of my work or spoken with my patients?
WHAT GIVES the American Board of Internal Medicine the right to tell insurance companies and hospitals when my board certification expires so those companies can suddenly refuse to issue payments or revoke my hospital privileges claiming by skills as a physician have expired?
The American Board of Internal Medicine says it is developing new strategies of physician testing in the name of improved patient care, but WHAT GIVES for those physicians it has de-certified and are now jobless?
Removing physicians with years of patient care experience because they refuse to pay a fee or perform needless computer tasks is not in the best interest of patient safety or quality of care.
So WHAT GIVES?
-Wes
PS: Please help support the legal efforts underway to end Maintenance of Certification for all subspecialties by contributing to at https://www.gofundme.com/practicing-physicians-of-america
(Every dollar helps. Please share this video with your colleagues, too.)
Friday, October 25, 2019
A Case Study in the Wrong Way to Fix Clinician Burnout
Asking the system to fix the system in regards to physician and nursing burnout is like asking the fox to watch the henhouse.
They have no clue.
Case in point: the recent article published online before print in the Journal of the American Medical Association (JAMA) (where else?) preaching a "systems-based approach to clinician well-being and provide better patient care."
What "system" is recommending this "approach? None other than the Accreditation Council for Graduate Medical Education comprised of the American Medical Association (AMA), the American Hospital Association (AHA), and the American Board of Medical Specialties (ABMS), among others, with work performed by a committee comprised of friends from Blue Cross Blue Shield.
Most concerning, however, is this report was co-authored by one of the most conflicted authors in the health care business, Christine K. Cassel, MD. Recall that Dr. Cassel failed to disclose her board seats (and income) with Kaiser Hospitals and Health Systems and Premier (the largest health care Group Purchase Organization for the nation's hospitals) while serving as President and CEO of the American Board of Internal Medicine.
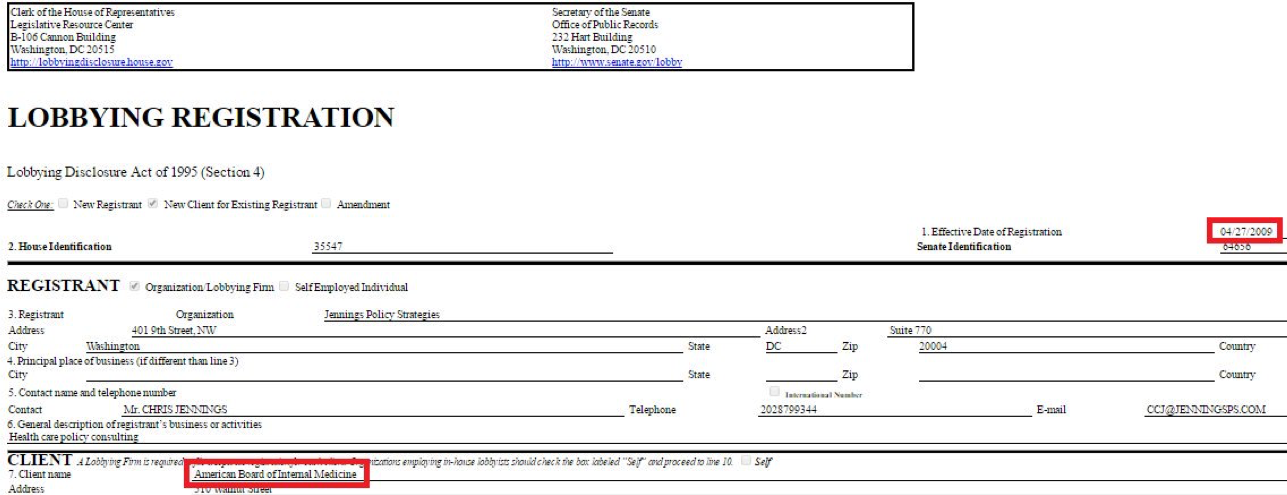
Christine K. Cassel, MD was President and CEO of the ABIM from 2004-2014. During her tenure at the ABIM, Dr. Cassel received a highly influential political appointment on the President's Council of Advisors for Science and Technology under President Obama in April 2009, just before the Affordable Care Act was signed into law in 2010.
The same day she announced that political appointment, the ABIM contracted with Washington lobbying firm Jennings Policy Strategies, Inc. yet never publicly disclosed this relationship. Instead, ABIM tax forms from 2010 listed this firm as hired for "consulting services." It appears to this lay physician that these "services" were in direct violation of IRS regulations concerning lobbying, especially given Dr. Cassel's substantial non-disclosed financial ties to Premier, Inc., one of the nation's largest Group Purchase Organizations for the nation's hospitals. At least one other lobbying firm was retained by ABIM (named Mehlman Castagnetti Rosen Bingel and Thomas, Inc.) until June 30, 2015, and this relationship was never publicly disclosed to ABIM's physician diplomates, the IRS, or the public either.
According to a Newsweek reporter, the ABIM used obfuscatory accounting techniques during and after Dr. Cassel's tenure: "I had an easier time figuring out the compensation of officials at Enron, WorldCom and Adelphia—all famous for lying on financial filings—than I did for those at the ABIM, where enormous effort seems to have been taken to make murky what should be crystal clear." The ABIM reportedly paid Dr. Cassel $1.7 million in her final year.
Some things never change: Dr. Cassel once again claimed "no conflicts" in the disclosures to this most recent JAMA article on physician burnout either.
Gaslighting physicians and nurses is not the way to fix burnout.
It would be far better for the members of the ACGME to hold a mirror before themselves to understand how their conflicts of interest have systematically done more to harm our profession over the years. Our current house of Medicine has gleefully created the world's most expensive typing pool with physicians and nurses as little more than data entry clerks clicking away whether home or at work. Our current non-transparent health care system has evolved this way thanks in large part to the AMA's behind-the-scenes business model dependent on licensing its ever-changing "Current Procedural Terminology" (CPT) codes for use by the electronic medical record companies and insurance companies to covertly ration care. At the same time, the ACGME supported and promoted the transition from lifetime ABMS board certification to an unproven and wasteful "continuous board certification" by insisting on lifetime testing and payments from physicians for themselves, the lucrative publishing and testing industries, and a vast network of physician specialty societies without ever examining the harms this extortion has caused physicians and the patients they care for. It is telling there was no mention in the recent JAMA article of the "Maintenance of Certification" (MOC) controversy that has led to multiple ongoing federal class action antitrust and racketeering lawsuits, deprives physicians of personal and family time, and steals any semblance of self-educational autonomy from physicians for the benefit of the ACGME members and their collaborators.
To fix burnout we need doctors and nurses looking up at patients rather than looking down at computer screens. We don't need hand-holding wellness exercises, life coaches, and yoga classes. We especially dont need them right after witnessing the unfortunate death of a child or having a patient die beneath our hands despite our best efforts.
Doctors and nurses are not babies or widgets in an assembly line.We entered into this real-life drama of medicine with eyes wide open knowing full well that medicine and health care can be challenging. Yet much of corporate medicine has taken on its role to push our limits to make the system more "productive" for the system at the expense of its caregivers. Medicine is hard damn work that is both emotionally draining yet exhilarating all at the same time. We take the ultimate responsibility for our patients. The ACGME and their protected bureaucratic workshop do not. We risk falling prey to this exploitation if we fail to expose these many undisclosed conflicts of interest with the authors and "committee" wrote and published this paper in JAMA.
This is not to say I see a day where medicine will occur without the use of computers. But computers and secret sharing of data health care data can have its consequences if patients and physicians are kept in the dark. The depersonalization that computers bring to medicine has a nasty side effect on the care we provide: physicians and nurses need face-to-face, hand-to-hand, and heart-to-heart time with patients and their colleagues, not computers, procedure codes, and recommendations from people who foisted MOC upon us, stood to gain financially from it, but never participated in MOC themselves.
Distrust of our self-imposed corporate overlords is a large part of why we're where we are currently, particularly when they insult us with their self-serving "mission" to have physicians help themselves. What do these physician-bureaucrat posers know what's really happening on the front line of health care today?
Humility at admitting mistakes would go a lot further at curing physician burnout than beating the same corporate drum that wedges itself between what really matters: doctors and nurses caring for patients without the self-appointed, politically- and industry-funded National Academy of Medicine and their cronies telling us how to do our jobs. It would be far better if they took off the chains they bind us with and let us do what we do best.
-Wes
They have no clue.
Case in point: the recent article published online before print in the Journal of the American Medical Association (JAMA) (where else?) preaching a "systems-based approach to clinician well-being and provide better patient care."
What "system" is recommending this "approach? None other than the Accreditation Council for Graduate Medical Education comprised of the American Medical Association (AMA), the American Hospital Association (AHA), and the American Board of Medical Specialties (ABMS), among others, with work performed by a committee comprised of friends from Blue Cross Blue Shield.
Most concerning, however, is this report was co-authored by one of the most conflicted authors in the health care business, Christine K. Cassel, MD. Recall that Dr. Cassel failed to disclose her board seats (and income) with Kaiser Hospitals and Health Systems and Premier (the largest health care Group Purchase Organization for the nation's hospitals) while serving as President and CEO of the American Board of Internal Medicine.
Christine K. Cassel, MD was President and CEO of the ABIM from 2004-2014. During her tenure at the ABIM, Dr. Cassel received a highly influential political appointment on the President's Council of Advisors for Science and Technology under President Obama in April 2009, just before the Affordable Care Act was signed into law in 2010.
The same day she announced that political appointment, the ABIM contracted with Washington lobbying firm Jennings Policy Strategies, Inc. yet never publicly disclosed this relationship. Instead, ABIM tax forms from 2010 listed this firm as hired for "consulting services." It appears to this lay physician that these "services" were in direct violation of IRS regulations concerning lobbying, especially given Dr. Cassel's substantial non-disclosed financial ties to Premier, Inc., one of the nation's largest Group Purchase Organizations for the nation's hospitals. At least one other lobbying firm was retained by ABIM (named Mehlman Castagnetti Rosen Bingel and Thomas, Inc.) until June 30, 2015, and this relationship was never publicly disclosed to ABIM's physician diplomates, the IRS, or the public either.
{kind=link}
According to a Newsweek reporter, the ABIM used obfuscatory accounting techniques during and after Dr. Cassel's tenure: "I had an easier time figuring out the compensation of officials at Enron, WorldCom and Adelphia—all famous for lying on financial filings—than I did for those at the ABIM, where enormous effort seems to have been taken to make murky what should be crystal clear." The ABIM reportedly paid Dr. Cassel $1.7 million in her final year.
Some things never change: Dr. Cassel once again claimed "no conflicts" in the disclosures to this most recent JAMA article on physician burnout either.
Gaslighting physicians and nurses is not the way to fix burnout.
It would be far better for the members of the ACGME to hold a mirror before themselves to understand how their conflicts of interest have systematically done more to harm our profession over the years. Our current house of Medicine has gleefully created the world's most expensive typing pool with physicians and nurses as little more than data entry clerks clicking away whether home or at work. Our current non-transparent health care system has evolved this way thanks in large part to the AMA's behind-the-scenes business model dependent on licensing its ever-changing "Current Procedural Terminology" (CPT) codes for use by the electronic medical record companies and insurance companies to covertly ration care. At the same time, the ACGME supported and promoted the transition from lifetime ABMS board certification to an unproven and wasteful "continuous board certification" by insisting on lifetime testing and payments from physicians for themselves, the lucrative publishing and testing industries, and a vast network of physician specialty societies without ever examining the harms this extortion has caused physicians and the patients they care for. It is telling there was no mention in the recent JAMA article of the "Maintenance of Certification" (MOC) controversy that has led to multiple ongoing federal class action antitrust and racketeering lawsuits, deprives physicians of personal and family time, and steals any semblance of self-educational autonomy from physicians for the benefit of the ACGME members and their collaborators.
To fix burnout we need doctors and nurses looking up at patients rather than looking down at computer screens. We don't need hand-holding wellness exercises, life coaches, and yoga classes. We especially dont need them right after witnessing the unfortunate death of a child or having a patient die beneath our hands despite our best efforts.
Doctors and nurses are not babies or widgets in an assembly line.We entered into this real-life drama of medicine with eyes wide open knowing full well that medicine and health care can be challenging. Yet much of corporate medicine has taken on its role to push our limits to make the system more "productive" for the system at the expense of its caregivers. Medicine is hard damn work that is both emotionally draining yet exhilarating all at the same time. We take the ultimate responsibility for our patients. The ACGME and their protected bureaucratic workshop do not. We risk falling prey to this exploitation if we fail to expose these many undisclosed conflicts of interest with the authors and "committee" wrote and published this paper in JAMA.
This is not to say I see a day where medicine will occur without the use of computers. But computers and secret sharing of data health care data can have its consequences if patients and physicians are kept in the dark. The depersonalization that computers bring to medicine has a nasty side effect on the care we provide: physicians and nurses need face-to-face, hand-to-hand, and heart-to-heart time with patients and their colleagues, not computers, procedure codes, and recommendations from people who foisted MOC upon us, stood to gain financially from it, but never participated in MOC themselves.
Distrust of our self-imposed corporate overlords is a large part of why we're where we are currently, particularly when they insult us with their self-serving "mission" to have physicians help themselves. What do these physician-bureaucrat posers know what's really happening on the front line of health care today?
Humility at admitting mistakes would go a lot further at curing physician burnout than beating the same corporate drum that wedges itself between what really matters: doctors and nurses caring for patients without the self-appointed, politically- and industry-funded National Academy of Medicine and their cronies telling us how to do our jobs. It would be far better if they took off the chains they bind us with and let us do what we do best.
-Wes
Saturday, October 12, 2019
Plaintiffs to Appeal ABIM Class-Action Lawsuit in Full
With the time to amend the earlier class action antitrust and racketeering lawsuit against the American Board of Internal Medicine (ABIM) past, this statement was issued by C. Phillip Curley, the Plaintiffs' lead attorney:
-Wes
Physicians wishing to support the plaintiffs in this unprecedented action are encouraged to contribute here.
“Plaintiffs plan to appeal in full the dismissal of their case. While we respect the district court, we believe it was wrong at this early stage of the litigation to dismiss Plaintiff’s case and deprive them of their day in court. Plaintiffs look forward to the vindication of their claims on appeal.”ABIM may have thought they won this case on dismissal, but it looks the plaintiffs' claims will get a second more critical review of the case with the 3rd Circuit Court of Appeals.
-Wes
Physicians wishing to support the plaintiffs in this unprecedented action are encouraged to contribute here.
Subscribe to:
Posts (Atom)