Asking the system to fix the system in regards to physician and nursing burnout is like asking the fox to watch the henhouse.
They have no clue.
Case in point: the recent article published online before print in the Journal of the American Medical Association (JAMA) (where else?) preaching a "systems-based approach to clinician well-being and provide better patient care."
What "system" is recommending this "approach? None other than the Accreditation Council for Graduate Medical Education comprised of the American Medical Association (AMA), the American Hospital Association (AHA), and the American Board of Medical Specialties (ABMS), among others, with work performed by a committee comprised of friends from Blue Cross Blue Shield.
Most concerning, however, is this report was co-authored by one of the most conflicted authors in the health care business, Christine K. Cassel, MD. Recall that Dr. Cassel failed to disclose her board seats (and income) with Kaiser Hospitals and Health Systems and Premier (the largest health care Group Purchase Organization for the nation's hospitals) while serving as President and CEO of the American Board of Internal Medicine.
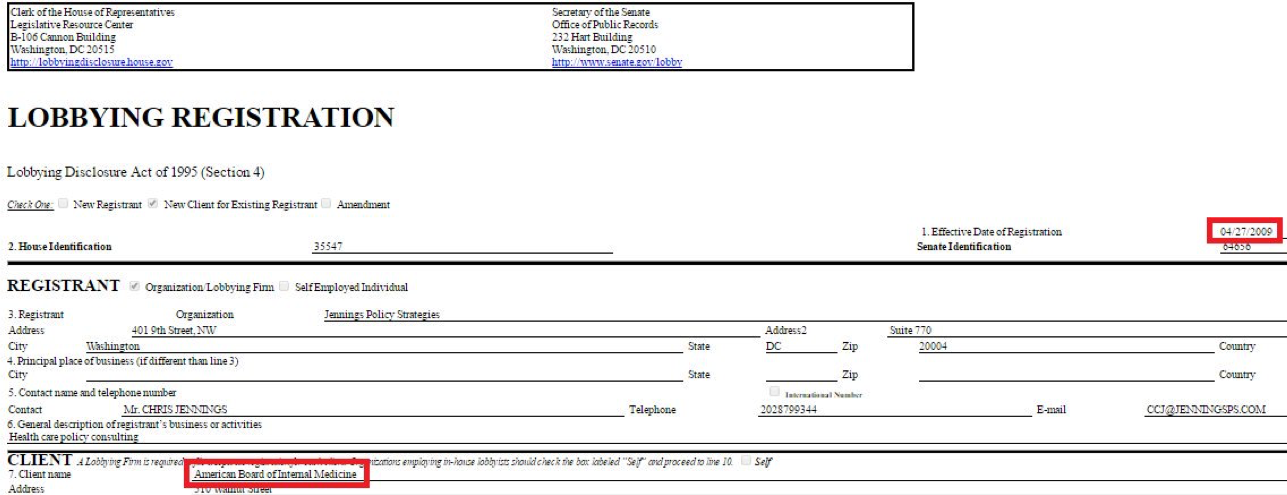
Christine K. Cassel, MD was President and CEO of the ABIM from 2004-2014. During her tenure at the ABIM, Dr. Cassel received a highly influential political appointment on the President's Council of Advisors for Science and Technology under President Obama in April 2009, just before the Affordable Care Act was signed into law in 2010.
The same day she announced that political appointment, the ABIM contracted with Washington lobbying firm Jennings Policy Strategies, Inc. yet never publicly disclosed this relationship. Instead, ABIM tax forms from 2010 listed this firm as hired for "consulting services." It appears to this lay physician that these "services" were in direct violation of IRS regulations concerning lobbying, especially given Dr. Cassel's substantial non-disclosed financial ties to Premier, Inc., one of the nation's largest Group Purchase Organizations for the nation's hospitals. At least one other lobbying firm was retained by ABIM (named Mehlman Castagnetti Rosen Bingel and Thomas, Inc.) until June 30, 2015, and this relationship was never publicly disclosed to ABIM's physician diplomates, the IRS, or the public either.
According to a Newsweek reporter, the ABIM used obfuscatory accounting techniques during and after Dr. Cassel's tenure: "I had an easier time figuring out the compensation of officials at Enron, WorldCom and Adelphia—all famous for lying on financial filings—than I did for those at the ABIM, where enormous effort seems to have been taken to make murky what should be crystal clear." The ABIM reportedly paid Dr. Cassel $1.7 million in her final year.
Some things never change: Dr. Cassel once again claimed "no conflicts" in the disclosures to this most recent JAMA article on physician burnout either.
Gaslighting physicians and nurses is not the way to fix burnout.
It would be far better for the members of the ACGME to hold a mirror before themselves to understand how their conflicts of interest have systematically done more to harm our profession over the years. Our current house of Medicine has gleefully created the world's most expensive typing pool with physicians and nurses as little more than data entry clerks clicking away whether home or at work. Our current non-transparent health care system has evolved this way thanks in large part to the AMA's behind-the-scenes business model dependent on licensing its ever-changing "Current Procedural Terminology" (CPT) codes for use by the electronic medical record companies and insurance companies to covertly ration care. At the same time, the ACGME supported and promoted the transition from lifetime ABMS board certification to an unproven and wasteful "continuous board certification" by insisting on lifetime testing and payments from physicians for themselves, the lucrative publishing and testing industries, and a vast network of physician specialty societies without ever examining the harms this extortion has caused physicians and the patients they care for. It is telling there was no mention in the recent JAMA article of the "Maintenance of Certification" (MOC) controversy that has led to multiple ongoing federal class action antitrust and racketeering lawsuits, deprives physicians of personal and family time, and steals any semblance of self-educational autonomy from physicians for the benefit of the ACGME members and their collaborators.
To fix burnout we need doctors and nurses looking up at patients rather than looking down at computer screens. We don't need hand-holding wellness exercises, life coaches, and yoga classes. We especially dont need them right after witnessing the unfortunate death of a child or having a patient die beneath our hands despite our best efforts.
Doctors and nurses are not babies or widgets in an assembly line.We entered into this real-life drama of medicine with eyes wide open knowing full well that medicine and health care can be challenging. Yet much of corporate medicine has taken on its role to push our limits to make the system more "productive" for the system at the expense of its caregivers. Medicine is hard damn work that is both emotionally draining yet exhilarating all at the same time. We take the ultimate responsibility for our patients. The ACGME and their protected bureaucratic workshop do not. We risk falling prey to this exploitation if we fail to expose these many undisclosed conflicts of interest with the authors and "committee" wrote and published this paper in JAMA.
This is not to say I see a day where medicine will occur without the use of computers. But computers and secret sharing of data health care data can have its consequences if patients and physicians are kept in the dark. The depersonalization that computers bring to medicine has a nasty side effect on the care we provide: physicians and nurses need face-to-face, hand-to-hand, and heart-to-heart time with patients and their colleagues, not computers, procedure codes, and recommendations from people who foisted MOC upon us, stood to gain financially from it, but never participated in MOC themselves.
Distrust of our self-imposed corporate overlords is a large part of why we're where we are currently, particularly when they insult us with their self-serving "mission" to have physicians help themselves. What do these physician-bureaucrat posers know what's really happening on the front line of health care today?
Humility at admitting mistakes would go a lot further at curing physician burnout than beating the same corporate drum that wedges itself between what really matters: doctors and nurses caring for patients without the self-appointed, politically- and industry-funded National Academy of Medicine and their cronies telling us how to do our jobs. It would be far better if they took off the chains they bind us with and let us do what we do best.
-Wes
{kind=link}
19 comments:
The chains are there for a reason. They built an entire pyramid on our shoulders. Countless bureaucrats of multiple calibers depend on our work to get their paychecks. They have no other skills other than analyze our performance and intensify our days. They sell their own value to the public as if they keep the public safer. Because we have to feed this army, the cost of healthcare gets progressively higher, while our incomes go down. If we rebel, this pyramid will fall apart.
I was moved by what you wrote. The truth has a strange effect like that when you listen with your mind and heart. Thank you for continuing to care.
To me it is crystal clear that MOC is a self-enrichment program. That's why they don't want to mention it.
MOC causes stress and burnout and that's why the elites like Christine Cassel don't waste their time on it. They avoid it like the plague, but give it plugs for their ABMS business cronies.
Surely Chris (Cassel) knows the ABMS encourages executives and professional medical bureaucrats to participate in MOC.
It is questionable if any of the executives at the ABMS or their medical board leadership could describe the inside of a Pearson Vue high stakes testing center.
I have to do it again next year. It has already began disrupting my life, work, making plans, seeing patients.
MOC is longitudinal distraction not lifetime education.
Agree 100% with Dr. Wes and the above commenter.
I feel like physicians and nurses have completely lost their autonomy. As a retired nurse, I did NOT sign up for 12 hrs shifts which never got me out of the hospital unit til 13-14 hrs of time working. I did not sign up to go through endless screens on a computer. I DID sign up to provide the best possible care to every patient and help promote their return to an improved life or a peaceful ending if they were closing the final chapters of their life. It was hard to devote the time to our patients who needed us far more than the non stop computer IT screens for many of the same questions the patient, family members have already answered a 100 times.It's all about bottom lines and shove the patients out the door in no time and hope patient satisfaction scores will pass the mustard!
As the industry has captured the regulators and our professional organizations, the only paths forward are outside the system.
Direct primary care
Telemedicine as an independent contractor/practitioner
Cash only practice
non-clinical careers.
An employed position is tantamount to self-abuse.
Recently on linkedIN, I commented on a thread dripping with "Mayo love."
In it, mayo docs were espousing the benefit of salary only clinician positions and a clinic design where "all the specialists a patient would need are in close proximity."
They seemed unable to grasp the idea that , "He who pays the piper calls the tunes."
The idea that the patient isn't "sophisticated" enough to purchase their own healthcare is simply an influence tactic to promote the opacity needed for self-dealing and overcharging.
With the assistance and curation of their own personal clinician, whom they pay directly, the patient can make healthcare purchases just fine.
Such a system gores too many oxen however, so it will not be allowed until the "Great Reset."
Until then, work outside the system---you'll be much happier
None of these administrators care. These are professional politicians pushing around emails speaking corporate happy talk. They do not care about clinicians. They are sociopaths skilled at lying, cheating and stealing up the corporate ladder. This is Medical Jenga. The first Jenga bottom piece pulled out is the old school clinicians who gut it out in 72 hour shifts are disappearing.
The tour of duty begins Friday at 5PM and doesn't end until 8A Monday. Folks coming out of training nowadays want to punch a clock cloning Epic notes and punch out. Working under duress was part of the experience back in the day. Perhaps a class action lawsuit against a large hospital system for sleep deprivation will awaken these hospital administrators.
We are still engineered to gulp that stale cup of coffee and stumble back home to a family already fast asleep. How dumb are we?
The second Jenga piece is the fast disappearing hospital facility fee. Any hospital system derived care gets a Federally approved "facility fee" charge. The hospital executives went on a spending spree acquiring assets, practices and most nauseatingly dispensed billions of dollars in bonuses to THEMSELVES. For every patient who got suckered into paying their 20% co-insurance/deductible/balance billing and then got SUED by the hospital for an overdue bill, you are getting ripped off by the hospitals.
On November 1st, 2019 the first cuts to facility fees will be enacted putting massive financial pressure on the hospitals. You can expect underperforming physicians and cost centers to be eliminated. The debt burden hospitals have acquired to fund new buildings, ORs, and more middle managers will crush any growth projections. You can't grow when you are servicing corporate debt with a coupon of 4-5%+. The only way out of it is more consolidation and massive austerity plans.
The third and last piece d'resistance is of course human resource management of doctors. This is also known as how to quell physicians from noticing this House of Cards is built on a foundation of wet mud and quicksand. That's where Cassel, Baron et al thought they were clever enough to bamboozle us into blind compliance. It is clear they made a massive miscalculation and the data are manifest. Clearly you can build a career based on treachery, lying and stealing from our profession.
So the powerful forces of change will now show up where the rubber meets the road.
Think I am wrong? Fully 50% of EP fellowships cannot fill their training positions. The EP fellowship Match goes unfilled. Why? Would any sane trainee want to work long hours doing risky procedures just so they can be employed by a financially failing hospital system?
Do the math. Complete your training at age 33+ and work for peanuts under the thumb of Rich Baron and the ABIM. Just so you can service your medical school debt and struggle to feed your family. The smart medical students are voting with their feet- Anesthesiology, Dermatology, General Cardiology, Ophthalmology. They are walking away from perpetual fellowships. Smart move.
If the training programs are half empty. And the older folks are slowing down and retiring. And the younger people who are left in the lab are going home exactly at 5PM. And the hospital based services are consolidating so there is less geographic choice. And salaries are being cut because the middle managers need to service their corporate bond debt. And no one will do the high risk procedures as they used to because the system is deincentivized.
Who will take care of the patient at 2AM on Thanksgiving Day?
Baron?
Cassel?
Luke: "Ten thousand??? We can almost buy our own ship for that!!!"
Han: "But who's gonna fly it, kid? You?"
THe hubris with which Christine Cassel blithely states that the burnt out doctors need more of her bureaucracy to soothe their frayed nerves, is totally abhorrent. Actually Dr Cassel, we need LESS of you and your clones screaming for more regulation, more MOC question and answers sessions paid for with my overworked credit card, more meetings, more hot air. MOC is killing doctors and healthcare and health insurance is at the breaking point. I’m seeing doctors retire, hospitals and clinics closing, and the CVS minute clinic staffed by a NP is multiplying like weeds. A race to the bottom is occurring and the over credentialed and over fellowship trainees are being decimated and left unemployed. As others have said, who’s left at 2am to tend to your Vtach? Nobody. The herd will be thinned, both the physicians and nurses and patients. Is this the goal? Is population replacement and a race to mediocrity what is planned?
I have the same reaction to all these new "physician wellness" programs. Addressing physician burnout is the flavor of the month. These programs will be put in place so the hospitals and the corporations that run them can SAY that they are "doing something about the physician burnout problem". It won't work. Physicians burn out because they have no more control and are called "providers". We are forced to spend a ridiculous percentage of our time entering data instead of caring for patients (the EMR that was going to make care more efficient and save time). The vast majority of EMR upgrades have nothing to do with making the data entry/user interface more efficient and pertinent--they are designed to more easily EXTRACT DATA that is useful for big data analysis, billing, adherence to quality improvement initiatives, and physician surveillance. The focus IS NOT on the patient physician interface. Which is after all the whole point of health care.
When we are not entering data and caring for patients, we are paying for and doing ridiculous MOC part 4 "Quality improvement" points. Just typing about this gives me such agida. I am 58 and will be leaving this behind relatively soon. I feel for the upcoming physicians.
Now available on the NASDAQ courtesy of the ABMS MOC® CORPORATION
MOC has physicians and patients in blockchains
That study is not even about burnout, it's about how corporations and government can manipulate the burnout crisis they created in order to monitor and control the "labor force" (patients and physicians) more efficiently. "They" put the foxes in the hen houses on purpose for their own evil purposes to erode the already diminished rights and privacy of physicians and patients. I repeat the study is not about physician well-being, it's about machine learning technology, AI, blockchain, surveillance and how corporations can make more money from less by fine tuning their systems.
Invisible chains
"The chains are there for a reason. They built an entire pyramid on our shoulders. Countless bureaucrats of multiple calibers depend on our work to get their paychecks. They have no other skills other than analyze our performance and intensify our days. They sell their own value to the public as if they keep the public safer. Because we have to feed this army, the cost of healthcare gets progressively higher, while our incomes go down. If we rebel, this pyramid will fall apart."
Banking, defense, healthcare, law enforcement
"You look fatigued. Come here and let us help you," said the foxes to the hens.
The same fluffy noses that brought us burnout are now going to fix it?
________________________________________________________________________________________
How independent* is your news? https://www.mdedge.com/internalmedicine/article/210818/career/nam-offers-recommendations-fight-clinician-burnout
Reported above by MDEdge a subsidiary of Frontline Medical Communications
https://www.frontlinemedcom.com/about/
Frontlind Medical Communications was recently bought out by WebMD.
https://www.mmm-online.com/home/channel/media-news/webmd-acquires-frontline-medical-communications/
WebMD is owned by Internet Brands, which is gobbling up many health-tech companies
https://www.prnewswire.com/news-releases/internet-brands-webmd-acquires-qxmd-300898932.html
Internet Brands has some controversies
https://en.wikipedia.org/wiki/Internet_Brands
Internet Brands is owned by private equity company KKR
https://en.wikipedia.org/wiki/Kohlberg_Kravis_Roberts
WebMD was acquired by Internet brands in 2017.
https://media.kkr.com/news-releases/news-release-details/webmd-be-acquired-kkrs-internet-brands
Inerenet Brands was acquired by KKR in 2014
https://www.reuters.com/article/us-internetbrands-deals-kkr-idUSKBN0EE12V20140603
*When they say a company will remain independent after being acquired, how independent do they mean?
Thanks Dr. wes. A systemic approach to burnout requires an overhaul of the health system but neither the health systems nor the insurance companies have any interest in changing anything....the only solution is physicians coming together to boycott the system...
This is the best read of my week so far. Couldn't agree more and I've shared this on FB (I hope that's ok). Excellent post and supporting facts.
As always, spot on. What wouldn't I give to listen to Cassel try to respond to these comments? Can someone PLEASE invite her?
FSMB and the Politics of Physician Control - Burnout and Wellness the Last Frontiers
"Widescale reduction of administrative redundancies has been identified in the 2018 FSMB Report on Physician Wellness and Burnout as a recommendation that would improve physician wellness, a patient safety issue.7" -FSMB
How will they in part achieve this?
"Adoption of new technologies to build the trust framework for a regulated environment."
- FSMB
Why MOC is never mentioned in any of the so-called studies and reports.
MOC is a liability issue and cannot be specifically named. To do so would be like a car manufacturer admitting that their "safety devices" did not work and in fact produced the opposite effect. The constraints were the cause of injury. But this is exactly what MOC does. It casues unspeakable harm. The reason tobacco and car manufactures do not study anything related to product safety is not until there is an outcry about it. The ABMS has done no studies on MOC's deleterious effects. Instead they are controlling the narrative and spinning a false reality as is typical of propagandist corporations and governments.
The ABMS public safety constraints (the MOC of all 24 franches) produce a faulty and harmful product that only generates a great deal of income for them. In fact the constraints and demands MOC places on physicians and patients invariably puts lives at risk.
MOC does cause harm. All ABMS member boards and their associations in the "quality cartel" have been instructed not topeak aobut lawsuits or liability issues. The executives and staff have bee coached not to mention MOC's links with burnout. They cannot speak out about what a bane to wellness maintenance of certification is. This is obviously because the organizations involved in the proliferation and profiteering from MOC could be sued on product safety issues.
What is hidden between every line of the FSMB study on burnout is that MOC does cause harm and we can't state it. The whole of the FSMB study points to physicians harm and patient harm from burnout.
MOC is a leading cause, if not arguably the major cause of burnout, because it is the hinge pin for the kingpin executives at the ABMS umbrella, the medical boards and their associates' myriad forms of administrative redundancies. This is the truth. MOC is a conspiracy to defraud patients through deceiving physicians and the public. (Certification matters. Phone people are instructed to talk about MOC when someone calls to verify a physician's ABMS certification.)
The ABMS, FSMB, AMA, NAM, ACP, NCQA, etc are trying to make physician burnout an issue, not because they want to end the root causes of burnout, but primarily to control physicians by increasing administrative burdens/redundancies not decreasing them. They are literally investing in technologies to create a work atmosphere of continuous surveillance, monitoring, analysis and reporting.
The ABMS/FSMB/ACGME circus - MOC product liability - covering up the root causes of burnout
The conscious and deliberate harm MOC does to physician/patient relationship and deleterious effect MOC has on the wellness of both
There is a delicate tightrope balancing act the various organizations are engaged in as they control the MOC/burnout narrative. In essence they want to lick the icing off the heavy MOC cake without falling into the quality chasm they created themselves with the enormous liability the quality/testing cartel faces.
ABMS and their business associates want to institutionalize burnout for their own benefit/profit - without taking responsibility for burnout. Burnout was never mentioned in "To Err is Human". Or the ABIM's manifesto on professionalism, which really was intended to gradually strip physicians of their rights. The whole of MOC is based on an error and the harm that error does. MOC is a patient/physicians safety issue and the courts need to issue an immediate injunction for relief.
From the FSMB 2018 report on physician burnout
"It has been widely reported for more than a decade that nearly 100,000 preventable
medical errors occur in the United States each year.
4 More recent findings suggest that between 210,000 and 400,000 deaths each year are associated with preventable harm.5
Many of these errors may be attributed to physician burnout and its drivers, such as
excessive caseloads, negative workplace culture, poor work-life balance, or perceived
lack of autonomy in one’s work.6 Burnout affects a significant proportion of the U.S.
physician workforce. A 2012 study conducted by Shanafelt and colleagues showed that
45.5% of surveyed physicians demonstrated at least one symptom of burnout.7 When this
study was repeated three years later with a different sample, the authors demonstrated
that burnout and work-life dissatisfaction had increased by 9% over the three year
period.8
In addition to obvious risks to patient safety, an alarming and extreme result of
physician burnout has been the disproportionate (relative to the general population) levels
of suicide in recent years by physicians, medical residents and even medical students.
9,10
One is hard-pressed to find a phenomenon that negatively affects a broader array of
stakeholders in health care than burnout. It impacts providers from all health professions.
State medical boards’ duty to protect the public, in this regard, also includes a
responsibility to ensure the wellness of its licensees."
FSMB tentative policy on physicians wellness and burnout
http://www.fsmb.org/siteassets/advocacy/policies/policy-on-wellness-and-burnout.pdf
FSMB Foundation Tax filings 2017
https://apps.irs.gov/pub/epostcard/cor/363071272_201804_990_2019042516241499.pdf
From FSMB digital credentials report 2019, June. (From their new DC mansion minus the Bogata surveillance bugs/devices.)
In their own words
"Digitization may foster a regulatory framework that is not only agile and automated but may also be a critical component in efforts to address other challenges within healthcare. The FSMB House of Delegates has repeatedly identified regulatory redundancies as an impediment to license portability5 and has called for enhancements to FSMB services that would expedite delivery of physician credentials to state medical boards and third parties.6 Widescale reduction of administrative redundancies has been identified in the 2018 FSMB Report on Physician Wellness and Burnout as a recommendation that would
improve physician wellness, a patient safety issue.7 Furthering the discussion of the digital transformation of credentialing through a vehicle such as this Report is another step forward towards the realization of these policy recommendations and aligns with the FSMB’s solid commitment to regulatory excellence.
As technology and healthcare evolve, so too does the ability of key stakeholders to provide a more efficient, secure, and verifiable trust framework without sacrificing the essential elements necessary to create a high level of trust between the patient and provider. In addition, there is a growing movement to disintermediate the creation and management of credentials and provide individual ownership of one’s own credentials. Digital credentials, in a variety of forms, can abstract the complexity of the licensing and credentialing process and reduce it to a seamless digital function which creates and maintains the trust
framework that is the necessary foundation for a modern healthcare system."
"Digitization may foster a regulatory framework that is not only agile and
automated but may also be a critical component in efforts to address other
challenges within healthcare." [In other words, burnout and wellness/patient safety.]
https://www.fsmb.org/siteassets/digital-credentials/digital-credentials-report-june-2019.pdf
The FSMB has bought themselves a permanent seat on K Street.
___________________
From the ABMS/AMA bureau of investigations and ministry of propaganda
Christine Sinsky's lengthy efforts to evade facts in behalf of the quality/testing cartel
Not to forget her own private investments in EHR technology that will make physicians more "agile". (AMA/ABIM/ABIMF/HealthFinch Advisor)
Describing the Harms of MOC - in their own words
http://www.annfammed.org/content/11/3/272.full
Post a Comment