The Hippocratic Oath. Most medical students in America recite some version of this oath at their medical school graduation. Its text implies a sacred and overriding respect (ethic if you will) for the individual."I swear by Apollo the physician and AEsculapius and Health (Hygieia) and All-Heal (Panacea) and all the gods and goddesses, that, according to my ability and judgment, I will keep this oath and this stipulation—to reckon him who taught me this art equally dear to me as my parents, to share my substance with him, and relieve his necessities if required; to look upon his offspring in the same footing as my own brothers, and to teach them this art, if they shall wish to learn it, without fee or stipulation; and that by precept, lecture, and every other mode of instruction, I will impart a knowledge of my art to my own sons, and those of my teachers, and to disciples bound by a stipulation and oath according to the law of medicine, but to none others. I will follow that system of regimen which, according to my ability and judgement, I consider for the benefit of my patients, and abstain from whatever is deleterious and mischievous.
I will give no deadly medicine to anyone if asked, nor suggest any such counsel; and in like manner I will not give to a woman a pessary to produce abortion.
With purity and with holiness I will pass my life and practice my art.
(I will not cut persons labouring under the stone, but will leave this to be done by men who are practitioners of this work.)
Into whatsoever houses I enter, I will go into them for the benefit of the sick, and will abstain from every voluntary act of mischief and corruption, and, further, from the abduction of females or males, of freemen and slaves. Whatever, in connection with my professional practice, or not in connection with it, I see or hear, in the life of men, which ought not to be spoken of abroad, I will not divulge, as reckoning that all such should be kept secret.
While I continue to keep this Oath unviolated, may it be granted to me to enjoy life and the practice of the art, respected by all men, in all times! But should I trespass and violate this Oath, may the reverse be my lot!"
(Adams, II, 779, cf. Littre, IV, 628.)
Doctors are currently witnessing the profession of medicine moving from the ethic of the individual to the ethic of the collective. The passage of the Affordable Care Act has solidified this treatment ethic and, as a consequence, often creates conflicts between the treating physician and their individual patients.
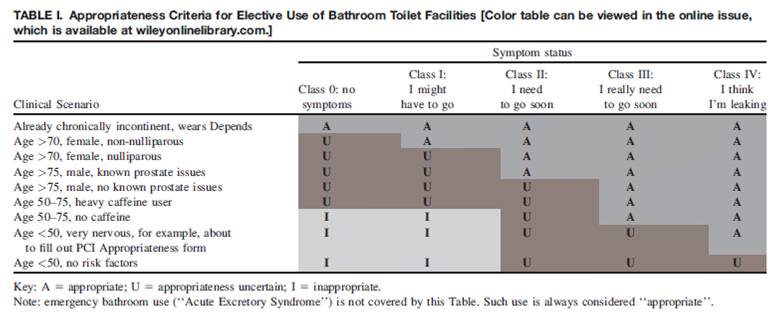
Nowhere is this shift to the ethic of the collective clearer than our expanding attempt to determine treatment "appropriateness" using a look-up chart of euphemistically-scored clinical scenarios owned and trademarked as "Appropriateness Criteria®" or "AUC®" by our own medical professional organizations. For those unfamiliar, these "criteria" label the care rendered in hypothetical clinical situations as "appropriate", "uncertain" or "inappropriate." (ed's note: oops, this year's update labels these "appropriate," "may be appropriate," or "rarely appropriate"). While touted as "evidence-based," these criteria simply are not - they are a consensus opinion of a collection of physicians for clinical scenarios unrelated to any real patient.
What happened to doctors serving as advocates for their patients? Are doctors really turning to these tables to decide which clinical care to render? Or do we really use them to make sure their EMR note reflects aspects that will assure third-party payment for care?
As we wallow in this latest unfortunate mandate being served to doctors, perhaps there is some use in investigating the origins of these ridiculously-complex criteria, for it is telling.
A few clicks of a computer will show the idea of "appropriateness" came from the Europeans via the RAND corporation. The organization quickly spread abroad and is now RAND Health in Santa Monica, California, USA and RAND Europe in Leiden, the Netherlands. Most of all, it is telling who now sits on the RAND Health Advisory board (ed note: Vice President, Global Affairs for Anheiser-Busch, really?). Not surprisingly, it is those who stand to gain from the business of medicine, the vast majority of whom are not even doctors. It is also worth noting that this is the same RAND organization that promoted unrealistic estimates of cost-savings to our health system afforded by Electronic Medical Records subsidized and promoted by the government today; the same business interests who make billions upon billions on Wall Street.
Our professional subspecialty societies, often funded by these very same organizations who sit as board members of the RAND Corporation, have turned a blind eye to this conflict of interest. They have adopted the process "in response to the imperative for improving the utilization of cardiovascular procedures in an efficient and contemporary fashion" and few have ever questioned its downside. In turn, doctors who use these methods collude with our well-meaning professional society colleagues to perpetuate a health care delivery model that prioritizes business interests on behalf of the "collective" above those of the individual patient. Why are we allowing trademarked intellectual properties like "Appropriateness Criteria®" to substitute for clinical judgment about our patient's individual clinical circumstance? Could our societal self-appointed gurus ever know anything about the constellation of complicated medical and social circumstances that patients bring before us in the private confines of our office? Of course not.
Yet here we are.
It seems a day never ends that physicians aren't being instructed on what else we must do to massage a chart for the good of the collective without a moment's consideration of what their "criteria" might mean for our patient's best care.
This is our new ethic, our new reality.
Speak out against this practice and the doctor is instantly labeled "non-evidence-based," "greedy," "self-serving," and "unconcerned" about the "patient collective." So doctors actively put their heads down and care for their patients as best they can. Daily, doctors experience the angst of this movement. We don't want to admit what has happened. Time and again we find ourselves constrained by these "guideline"- or "appropriateness use"-directed care that has been authorized by our own "physician collective" as "appropriate" when, by its very nature, is outdated by the time the guidelines are published, static and fail to incorporate newly-vetted therapies, and conflict with our patient's actual medical needs. Our field of medicine has become so complicit with this movement that we've even allowed our political and justice systems to threaten or impugn those who step outside these or other outdated care guidelines.
When doctors abandon our most basic ethic of caring for the individual for that of the collective, we are served our just desserts. Perhaps writing something like this will open our eyes. Or perhaps, as we've been so quick to do, we'll choose to keep them closed and not admit that this has happened.
Remember this when others say no to the care your patient needs.
-Wes
{kind=link}