"Dr. Fisher, there's this middle-aged person in the Emergency Room with a funny EKG who's short of breath and pretty tachycardic. Would you mind looking at it?"
"No," I said, taking a moment from the surgery I was performing. Here's what I saw:
Click image to enlarge
"Hmmm. Boy that's strange. Did you ... ?"
What did I ask? How would you sort this EKG out?
-Wes
19 comments:
mcg
said...
It looks to me sinus tachycardia with alternating conduction down the AVN and down an AP; I'd ask if they gave the guy any AVN blocking agent, maybe...
With the rigid regularity @ 150, I don't think it's sinus, but the P-wave orientation (appears upright in II, III) doesn't support a reentrant rhythm...
Well, I'll throw my hat in with a calcium-channel blocker!
So, I guess you did not want to post my response of atrial flutter and RVOT competing against one another.....tangoing....so to speak, because it would have undermined the interesting discussion and other comments....
The question is, is whether you ablate just the flutter or do you ablate both?
The flutter, with its rapid rates could have been the stimulant for the RVOT VT and you may not need to go after it.
My preference would be to do the flutter first, and then only after I demonstrated persistent VT on extended monitoring, would I go after that one as well.
I'm thinking MAT with alternating sources on each atria as the beats alternate from left to right axis. And the wider beats seem to have an accessory pathway due to the shortened PR interval.
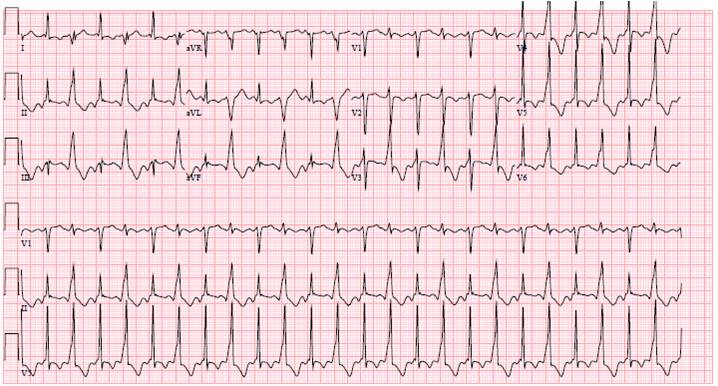
The EKG here contains a narrow-complex rhythm alternating with a wide complex rhythm. While there are similarities to "biventricular ventricular tachycardia," the lack of two alternating WIDE complex rhythm excludes this in the differential.
Most interesting are the negative P waves in leads II, III, and aVF that precede the narrow-complex beats. The wide complex beats obscure more careful analysis of the rhythm, so additional information can be gained if the rhythm is "disturbed" by varying the AV node conduction a bit.
My question was "Did you perform carotid massage or Valsalva on the patient?" The cardiologist who brought me the EKG had not performed either of these manuevers, but when they were attempted, no change to the rhythm occurred. It was elected to administer adenosine 6 mg IVP instead.
With adenosine, the rhythm stopped briefly, but then immediately reinitiated. The EKG, however, changed considerably to this EKG. (Beta blockers were administered and had little affect on the patients tachycardia rate. Note that the 5th and 7th beats of the subsequent EKG have the same morphology as the wide complex beats seen in the first EKG, except the 7th beat is somewhat narrower, making it consistent with a fusion beat between the narrow-complex rhythm and a PVC. Hence, the wide complex beats in the original EKG are from a ventricular source (ventricular bigeminy) and the narrow-complex beats are being driven by a long-RP supraventricular tachycardia (the second rhythm of the "tango").
The differential of the long-RP supraventricular tachycardia is fairly short: ectopic atrial tachycardia, atypical AV nodal reentrant tachycardia, or PJRT (paroxysmal junctional reentrant tachycardia from a decrementally-conducting retrograde-only accessory pathway). On EP study, the patient was found to have an incessant atrial tachycardia arising from the posteroseptal tricuspid annular area that was successfully ablated.
Of interest, the patient presented in congestive heart failure and was found to have an ejection fraction (post-ablation) of 18% with severe MR. The patient was discharged with a LifeVest and medical therapy for her cardiomyopathy thought to be induced by the tachycardia. Two months after ablation, both the the EF and mitral insufficiency had improved and the LifeVest never fired.
19 comments:
It looks to me sinus tachycardia with alternating conduction down the AVN and down an AP; I'd ask if they gave the guy any AVN blocking agent, maybe...
Are they on digoxin?
according to me, its ST with VES bygeminy,
With the rigid regularity @ 150, I don't think it's sinus, but the P-wave orientation (appears upright in II, III) doesn't support a reentrant rhythm...
Well, I'll throw my hat in with a calcium-channel blocker!
Atrial tachycardia
Start with Diltiazem 25mg slow IV push.
Is this electrical alternans from pericardial effusion?
ashman phenomen?
ashman phenomen
Christopher -
The patient was not on digoxin.
mcg and agus -
If it is sinus tachycardia, how do we explain the inverted P waves in II, III, aVF? (seen just before the narrow-complex beats)
Brooks Walsh -
I see the P waves inverted in those leads. Where are you looking?
Anony 11:25 PM -
Once you give diltiazem, it's hard to get back if the blood pressure drops. Any other ideas?
(Come back later today for follow-up info)
Are they on digoxin? Are they an electrician? On oxygen? How bout the left atrial enlargement.
Bidirectional VT, in the setting of dig toxicity?
Dang. I was seeing them a few milliseconds ahead, evidently. That makes for a short PRI in both types of complexes. Okay, I'm going with an AVRT.
I'll stick with the guess that the ED gave diltiazem, though, perhaps thinking they were looking at an AF before.
I'm concerned with the WPW like appearance In the V leads. I wouldn't not be giving cardizem here.
So, I guess you did not want to post my response of atrial flutter and RVOT competing against one another.....tangoing....so to speak, because it would have undermined the interesting discussion and other comments....
The question is, is whether you ablate just the flutter or do you ablate both?
The flutter, with its rapid rates could have been the stimulant for the RVOT VT and you may not need to go after it.
My preference would be to do the flutter first, and then only after I demonstrated persistent VT on extended monitoring, would I go after that one as well.
My bad. (Dang auto correct.) i meant above that regarding the WPW appearance in the V leads I would not consider Cardizem.
I'm thinking MAT with alternating sources on each atria as the beats alternate from left to right axis. And the wider beats seem to have an accessory pathway due to the shortened PR interval.
The EKG here contains a narrow-complex rhythm alternating with a wide complex rhythm. While there are similarities to "biventricular ventricular tachycardia," the lack of two alternating WIDE complex rhythm excludes this in the differential.
Most interesting are the negative P waves in leads II, III, and aVF that precede the narrow-complex beats. The wide complex beats obscure more careful analysis of the rhythm, so additional information can be gained if the rhythm is "disturbed" by varying the AV node conduction a bit.
My question was "Did you perform carotid massage or Valsalva on the patient?" The cardiologist who brought me the EKG had not performed either of these manuevers, but when they were attempted, no change to the rhythm occurred. It was elected to administer adenosine 6 mg IVP instead.
With adenosine, the rhythm stopped briefly, but then immediately reinitiated. The EKG, however, changed considerably to this EKG. (Beta blockers were administered and had little affect on the patients tachycardia rate. Note that the 5th and 7th beats of the subsequent EKG have the same morphology as the wide complex beats seen in the first EKG, except the 7th beat is somewhat narrower, making it consistent with a fusion beat between the narrow-complex rhythm and a PVC. Hence, the wide complex beats in the original EKG are from a ventricular source (ventricular bigeminy) and the narrow-complex beats are being driven by a long-RP supraventricular tachycardia (the second rhythm of the "tango").
The differential of the long-RP supraventricular tachycardia is fairly short: ectopic atrial tachycardia, atypical AV nodal reentrant tachycardia, or PJRT (paroxysmal junctional reentrant tachycardia from a decrementally-conducting retrograde-only accessory pathway). On EP study, the patient was found to have an incessant atrial tachycardia arising from the posteroseptal tricuspid annular area that was successfully ablated.
Of interest, the patient presented in congestive heart failure and was found to have an ejection fraction (post-ablation) of 18% with severe MR. The patient was discharged with a LifeVest and medical therapy for her cardiomyopathy thought to be induced by the tachycardia. Two months after ablation, both the the EF and mitral insufficiency had improved and the LifeVest never fired.
Without an ablation, what about Amiodarone?
Post a Comment