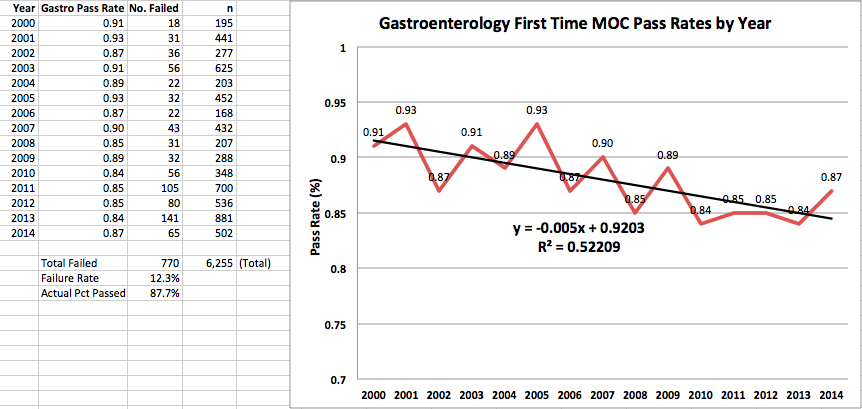
By now, most specialty boards in medicine appear to have "heard" practicing doctors over their displeasure over the American Board of Medical Specialties' (ABMS) proprietary MOC® program. They understand. They agree with us. They want to play nice. Really. They know how much we really don't like that secure examination every ten years that makes sure about 10-15% of experienced physicians fail because, well, someone has to fail. They understand that the busywork created by the ABMS MOC® program is time-consuming, duplicitous,
expensive and
meaningless for assuring quality care. A few of them even acknowledged, by golly, that
they got it wrong and promise to make things better by setting up new "
design principles" for further MOC® development.
But our ABMS Specialty Boards really don't seem to get the big problem: fraud.
Instead, some keep asking doctors to
cough up $2100 for "new and improved" exercises that
excludes the old MOC® secure examination and replaces them with annual "mini-assessments."
Fortunately, there's a small group of specialty societies that want change, but appear a bit too nervous about ridding themselves of the term "MOC®." They include the
American Gastroenterological Association, the
American Association of Clinical Endocrinologists, the
American College of Rheumatology, and (maybe) the
Heart Rhythm Society (although this statement is a greatly toned down version of an
earlier one).
But these Specialty Boards and professional organizations are relatively small fry compared to the much larger and richer specialty boards like the American College of Cardiology and the American College of Physicians who remain surprisingly quiet on the controversy.
"It's complicated," I'm told.
No, it's not.
***
The American Board of Medical Specialties (ABMS) has a problem. A big problem.
Their credibility bloom with practicing physicians is off the rose. Once an icon for assuring ethical, quality specialty medical education, the ABMS and their fellow member boards of the ACGME needed more. Much more. So they over-reached. They
paid themselves handsomely despite the
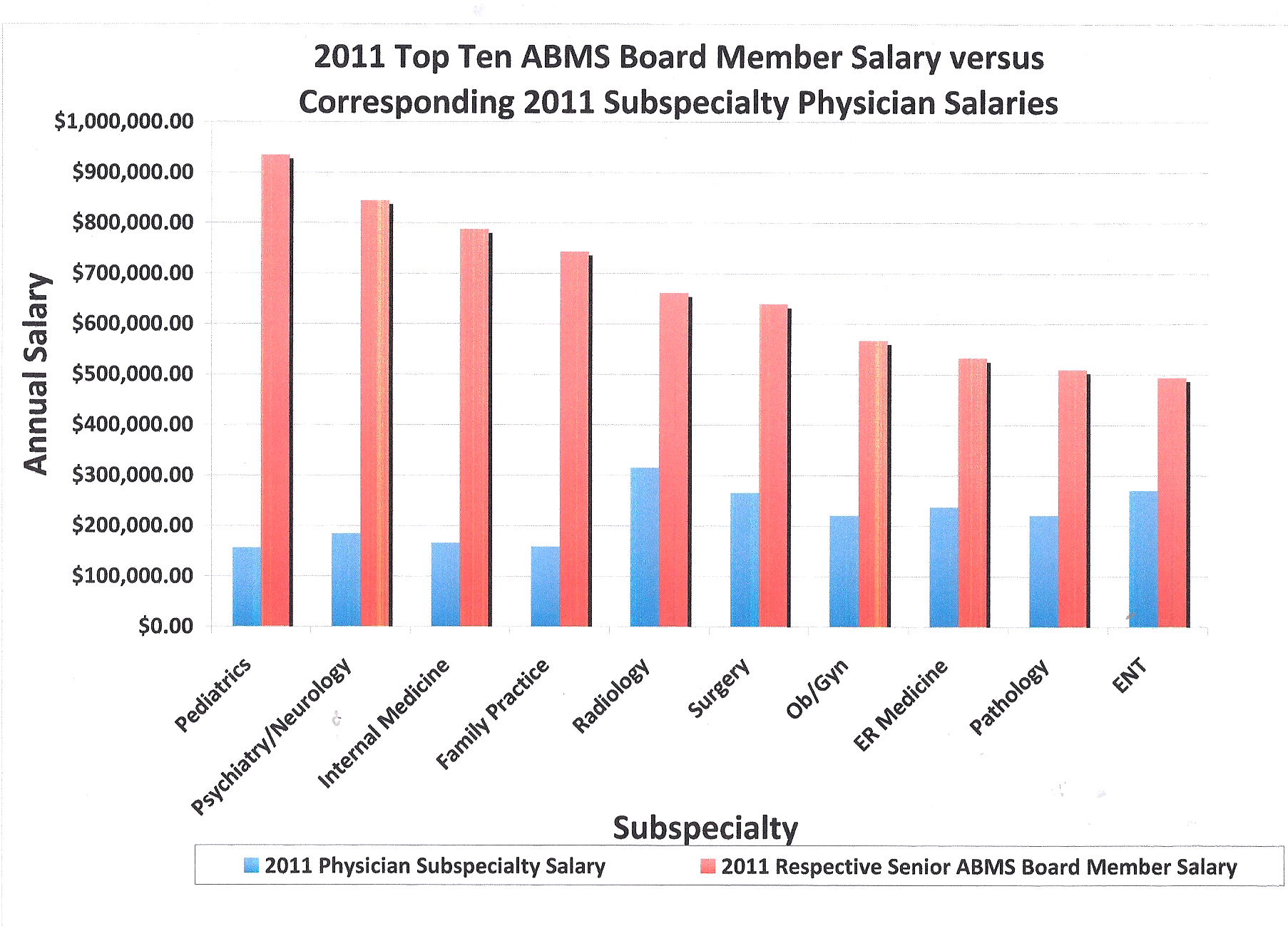
origins of the Specialty Boards being frugal. Almost without exception, the leadership of every ABMS specialty board has Presidents and CEOs that make far more income than their contemporary practicing colleagues -
way more. They fly first class (or have until 2000), commonly have expensive dinners at the finest five-star hotels, some of which even
overlook the Pacific Ocean,
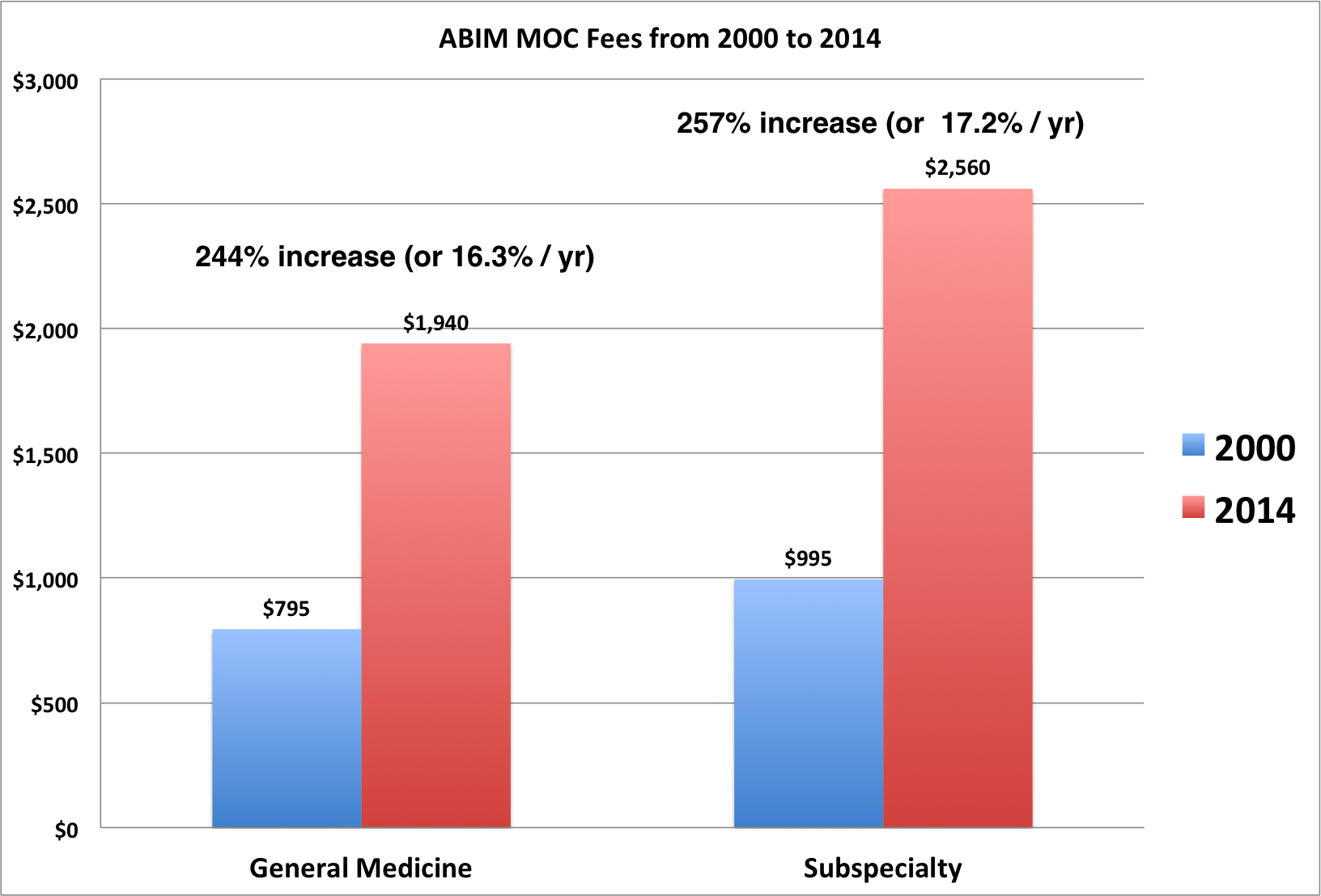
travel overseas to spread their regulatory gospel, all because they can. After all, they are special and they are unregulated. Meanwhile, residents and fellows making $50,000 a year are wondering where they'll come up with the $3000 or so it takes to become "certified" by the ABMS in their specialty.
The result? Practicing doctors don't trust our ABMS specialty boards any longer. Worse still, the more recent transgressions have prompted a look back at history, and history has shown the ABMS non-clinical specialty board leadership
stumping for corporate interests for personal gain instead of stumping for patients' best interests. Is this what the Boards call "professionalism?" The ABMS member boards also continue to allow their Presidents and CEOs to lead their organizations far past the usual maximum one-, two- or three-year term limits of the original boards, all while these executives earn lavish salaries and benefits as they
appoint new "Chairs" and "Directors" to make each organization seem "fresh."
The ABMS's largest member board also happens to be the American Board of Internal Medicine (ABIM).
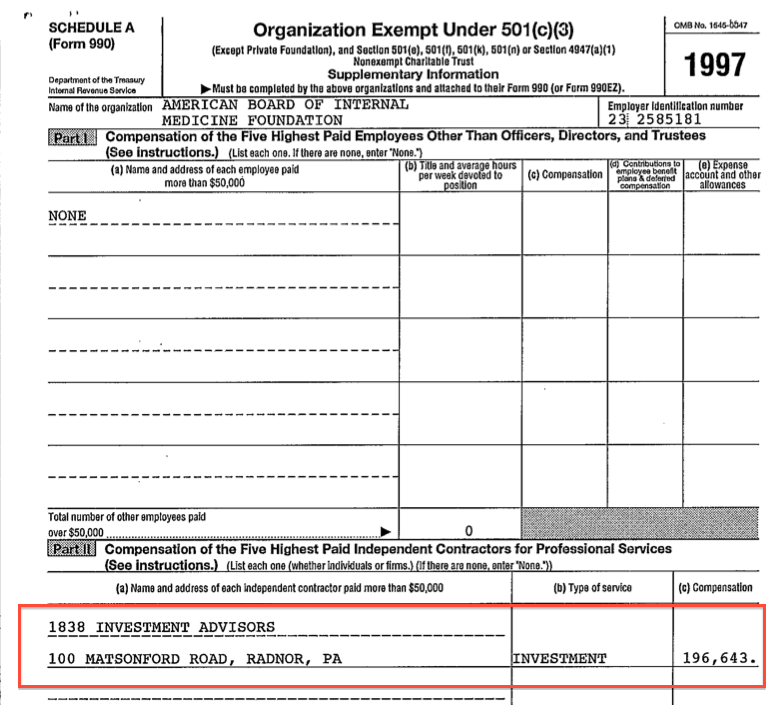
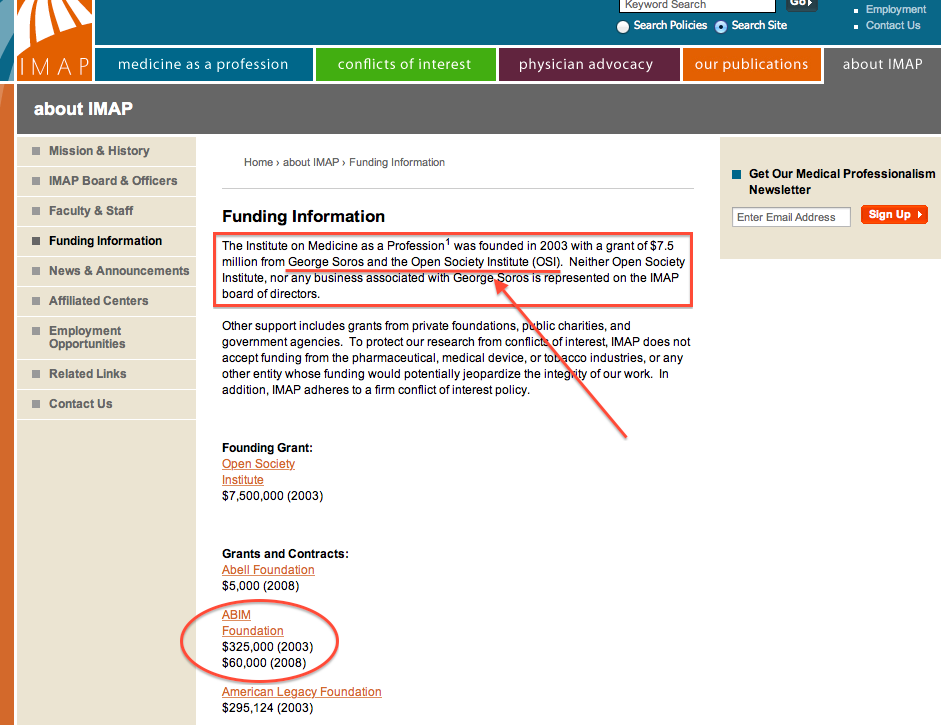
The ABIM still has the sizable problem of their ABIM Foundation that no one wants to mention: that "secret society" without a credible public mission other than "to support the ABIM" when it was created in 1989. The only logical reason for its creation was to accumulate money from the pockets of practicing physicians to fund an investment portfolio
created by the now defunct 1838 Investment Advisors (which were
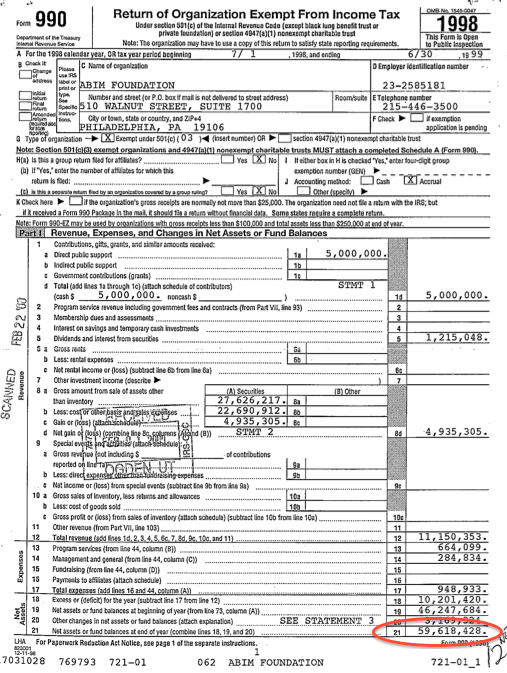
paid handsomely each year to do so). The ABIM leadership did very well using practicing physicians' money for this purpose, accumulating a bankroll of
over $59 million without concern of IRS intervention. They also
lied about their government lobbying activity that likely helped
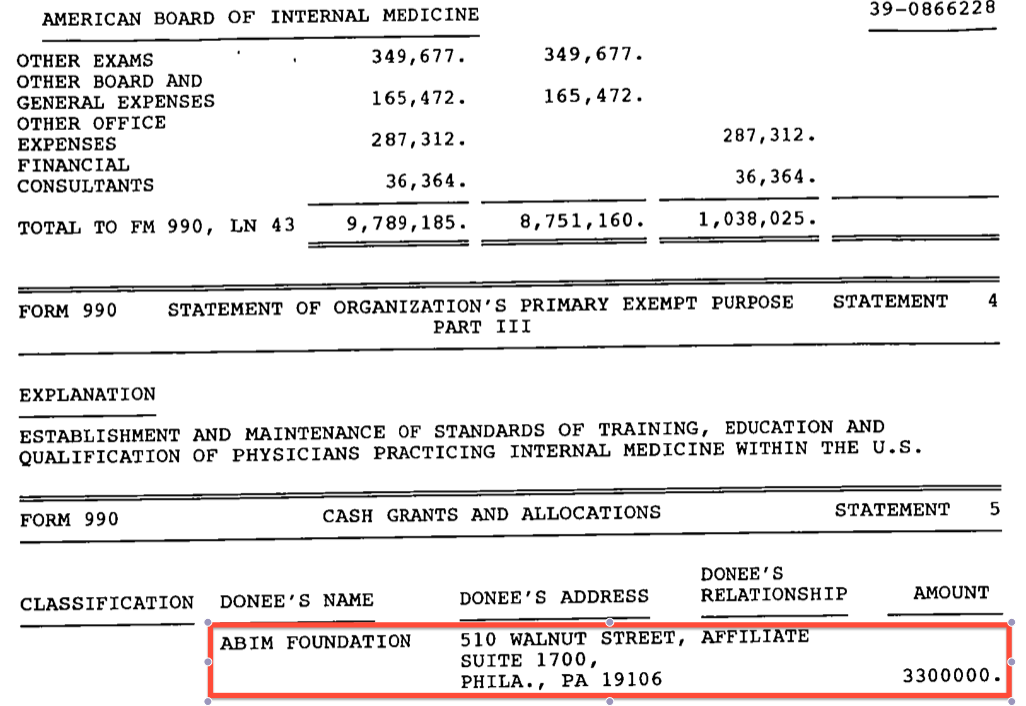
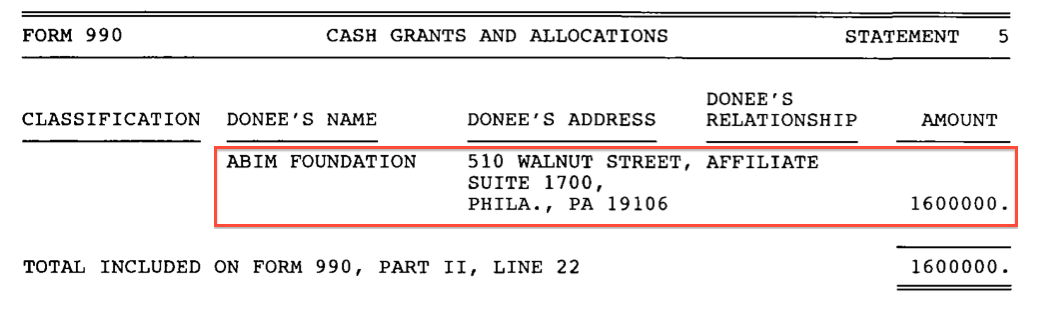
cement the ABMS MOC® program in the Affordable Care Act. Then, in what can only be considered (at best) an incredible lapse of judgment, they bought their infamous
luxury condominium (complete with chauffeur) with some of their colleagues' testing fees they "granted" to the Foundation.
What a deal.
But it's hard to shelter that a profit motive for a non-profit from the IRS unless you have a plan, and who is smarter than the folks and lawyers at the ABIM?
First, for
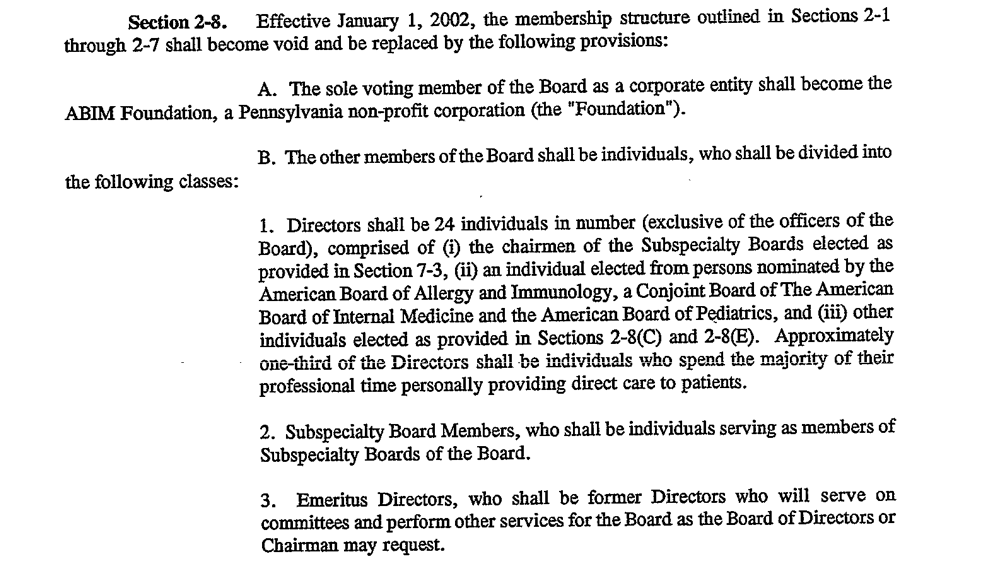
Deception #1, you have to
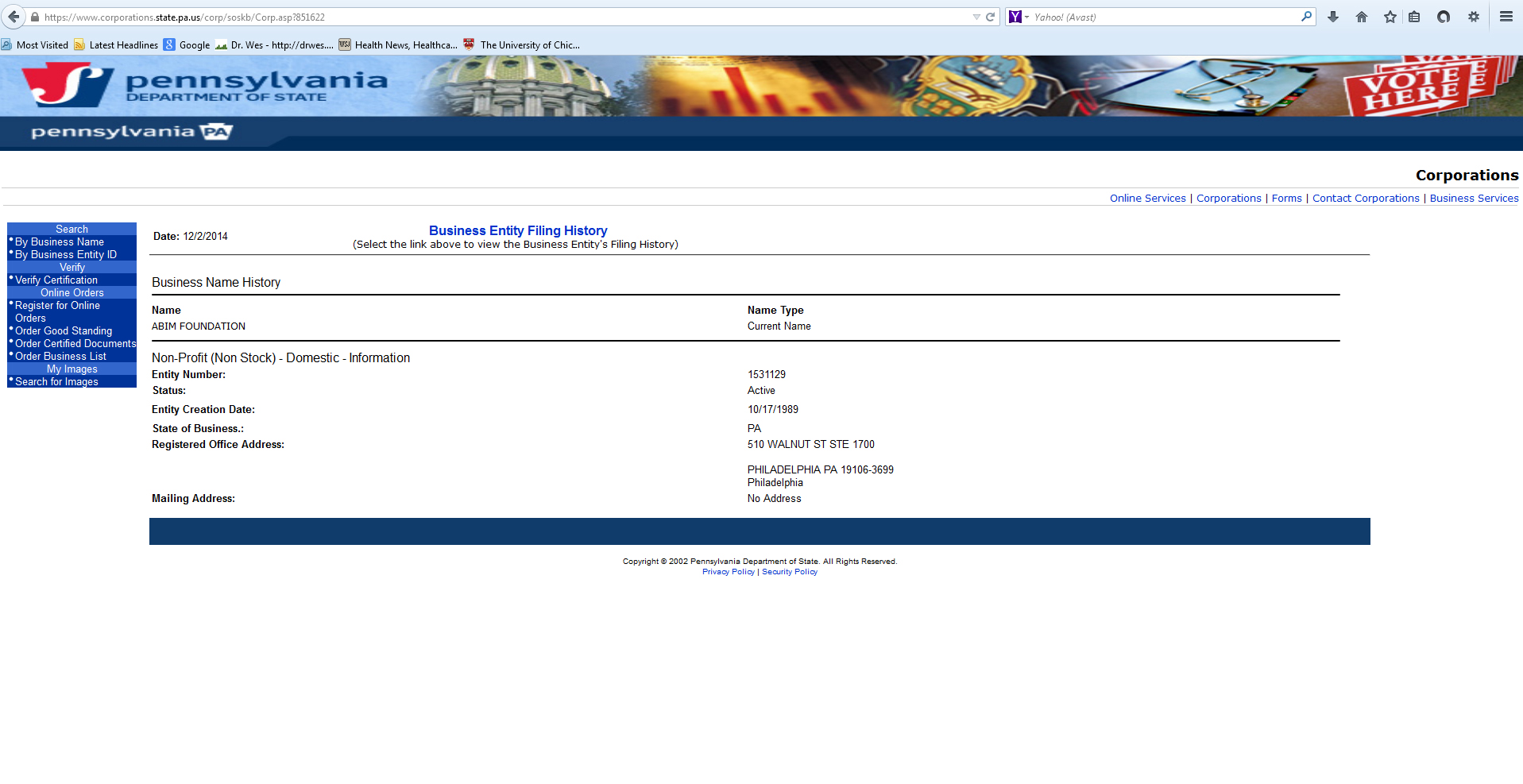
file a request for tax-exempt status for your newly-created "American Board of Internal Medicine Foundation" with the IRS. Note that this was a very different name from the "ABIM Foundation" that was
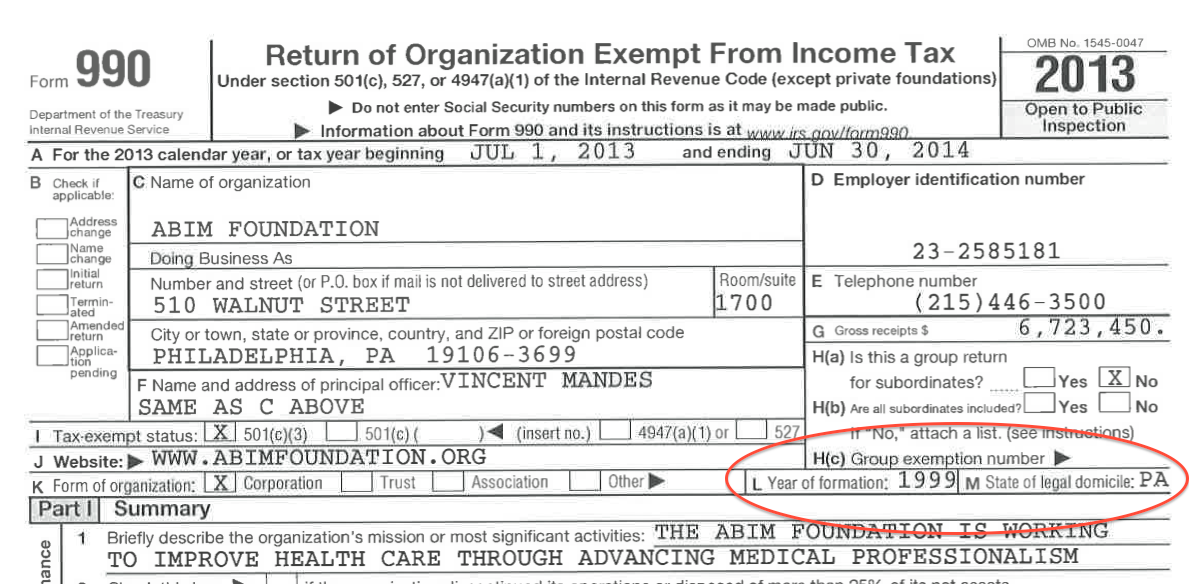
filed with the state of Pennsylvania in 1989. That way, the "American Board of Internal Medicine Foundation" never had too many dollars in its coffers to be tracked by the Internal Revenue Service (IRS).
Next, to avoid the tax consequences of accumulating a lot of money in a non-profit, you have to deflect. Unfortunately for the ABIM,
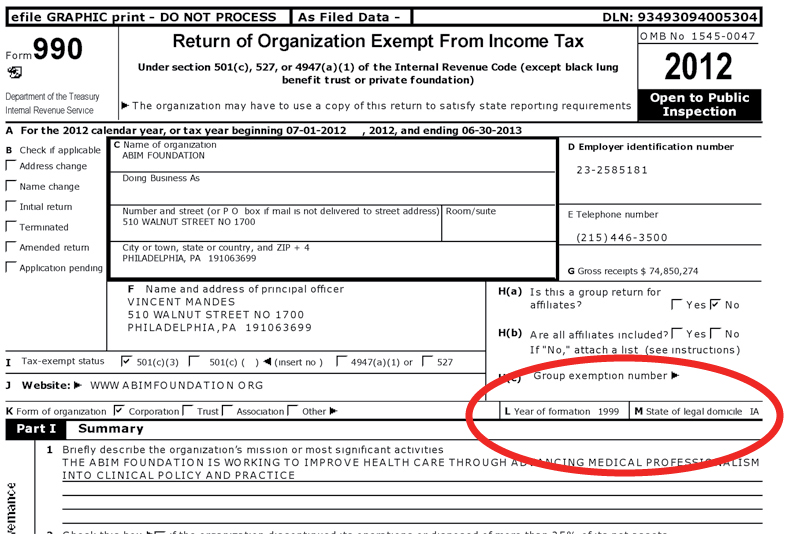
changes in the IRS Form 990 made in 2008 required them to start reporting a "state of domicile."
Deception #2: tell the IRS and the public (repeatedly until this year) on their Form 990 that the
ABIM Foundation was domiciled in Iowa where
no financial audit is required.
Then, when you realize your Foundation (that's supposed to be supporting the ABIM) has made a lot of cash covertly from the wallets of ABIM diplomats and investments, you magically perform
Deception #3: ask the IRS to
change the name of your "American Board of Internal Medicine Foundation" to the "ABIM Foundation" yet
keep it 'domiciled' in Iowa. Oh, and be sure the "computer-generated notices" are "changed" and a new non-profit determination letter is re-issued in the new name because, gosh, they got it wrong when they first applied.
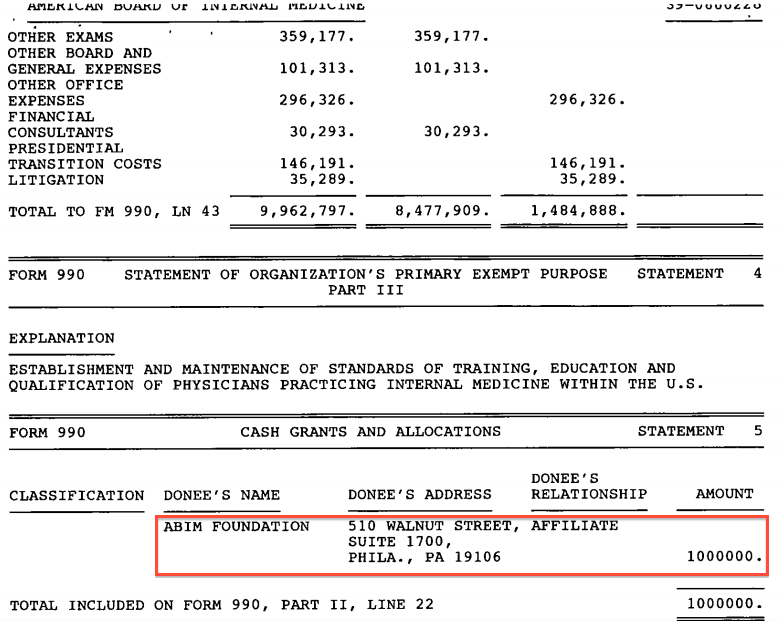
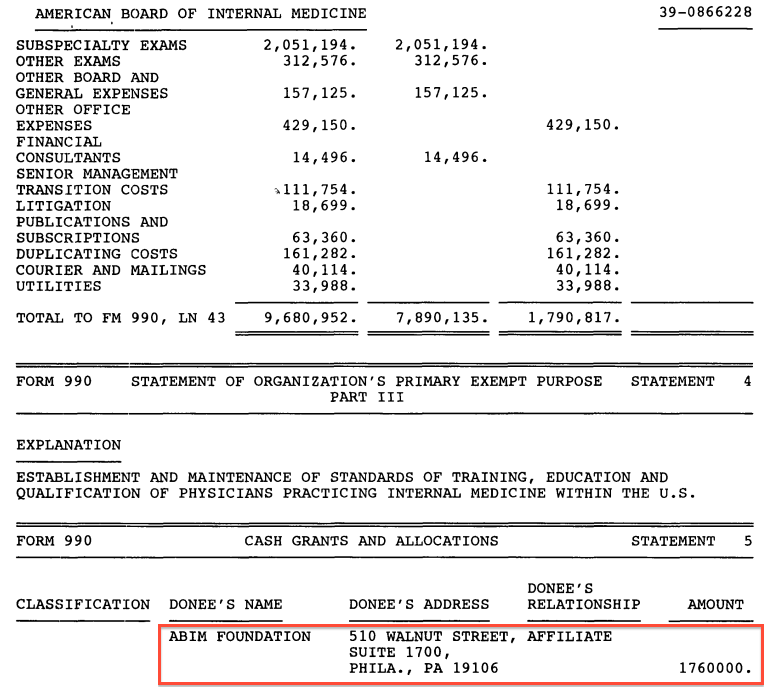
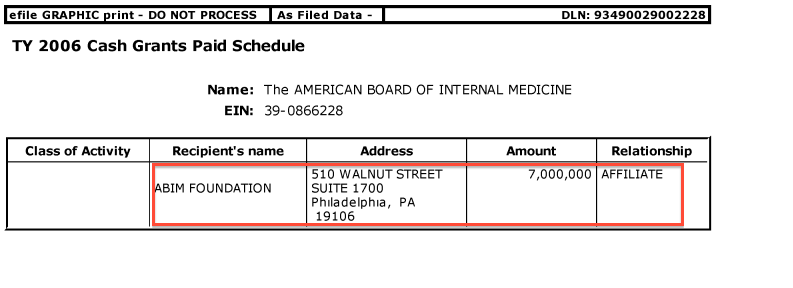
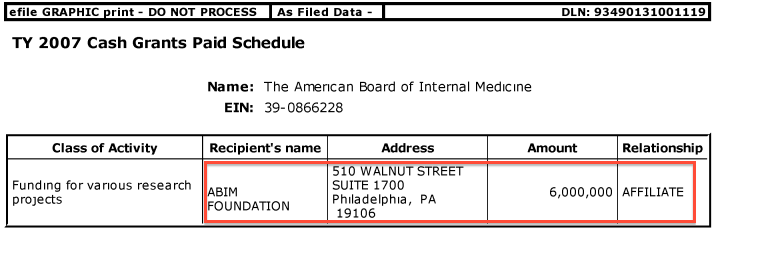
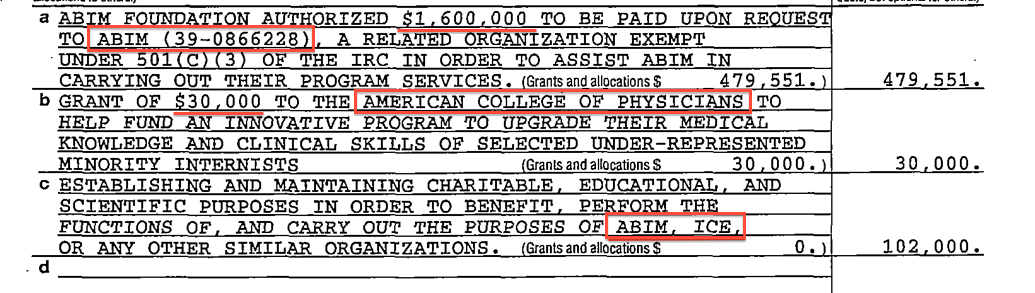
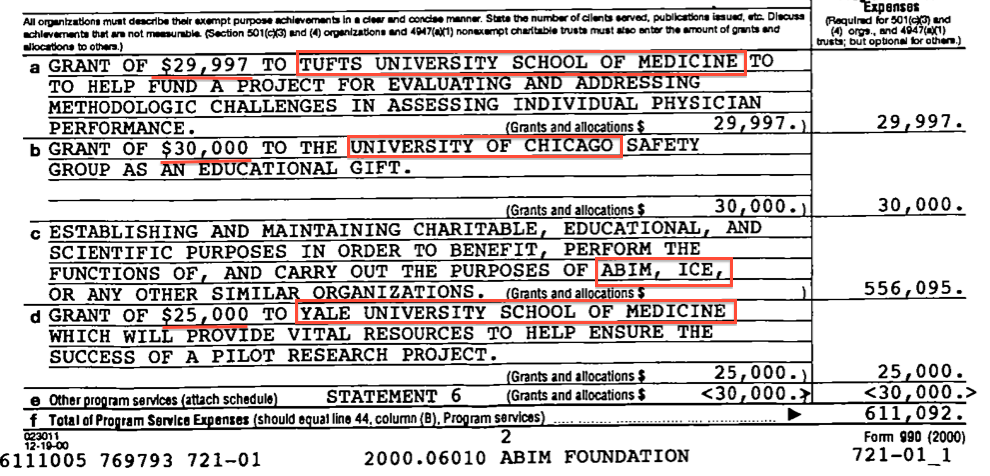
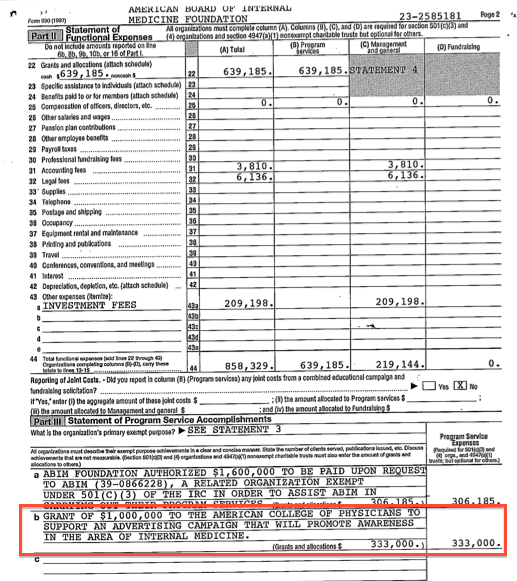
And guess what happens? The new ABIM Foundation magically has a boat-load of physician-supplied cash to give back to the ABIM (or their many cash-hungry friends who promise to spread the gospel of "Choose Wisely®") without an easily traceable trail because (as the
ABIM Foundation website and their
tax forms claimed) the ABIM Foundation really didn't exist (in the public or the IRS's eyes) before 1999!
Finally, it is
very important to perform
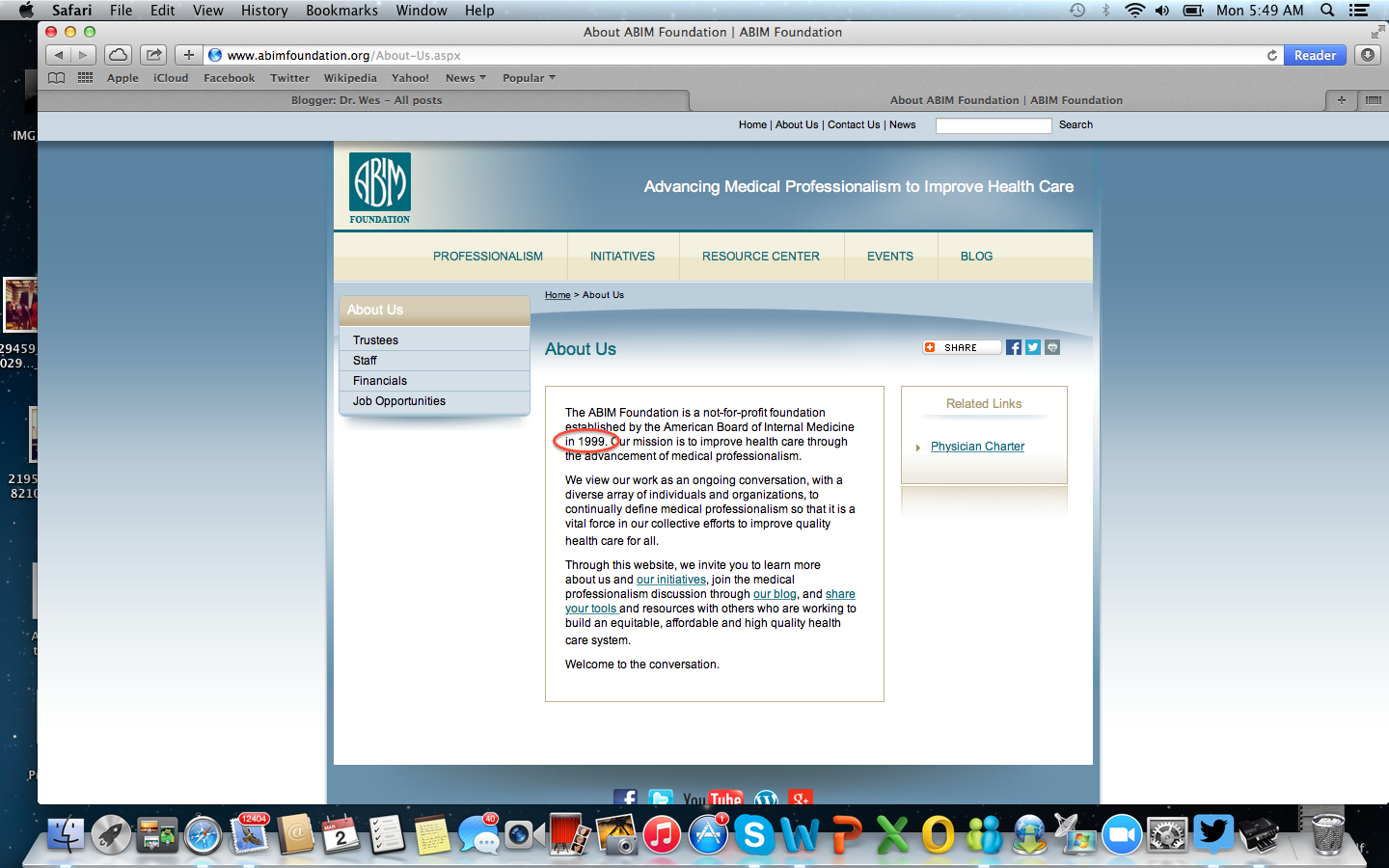
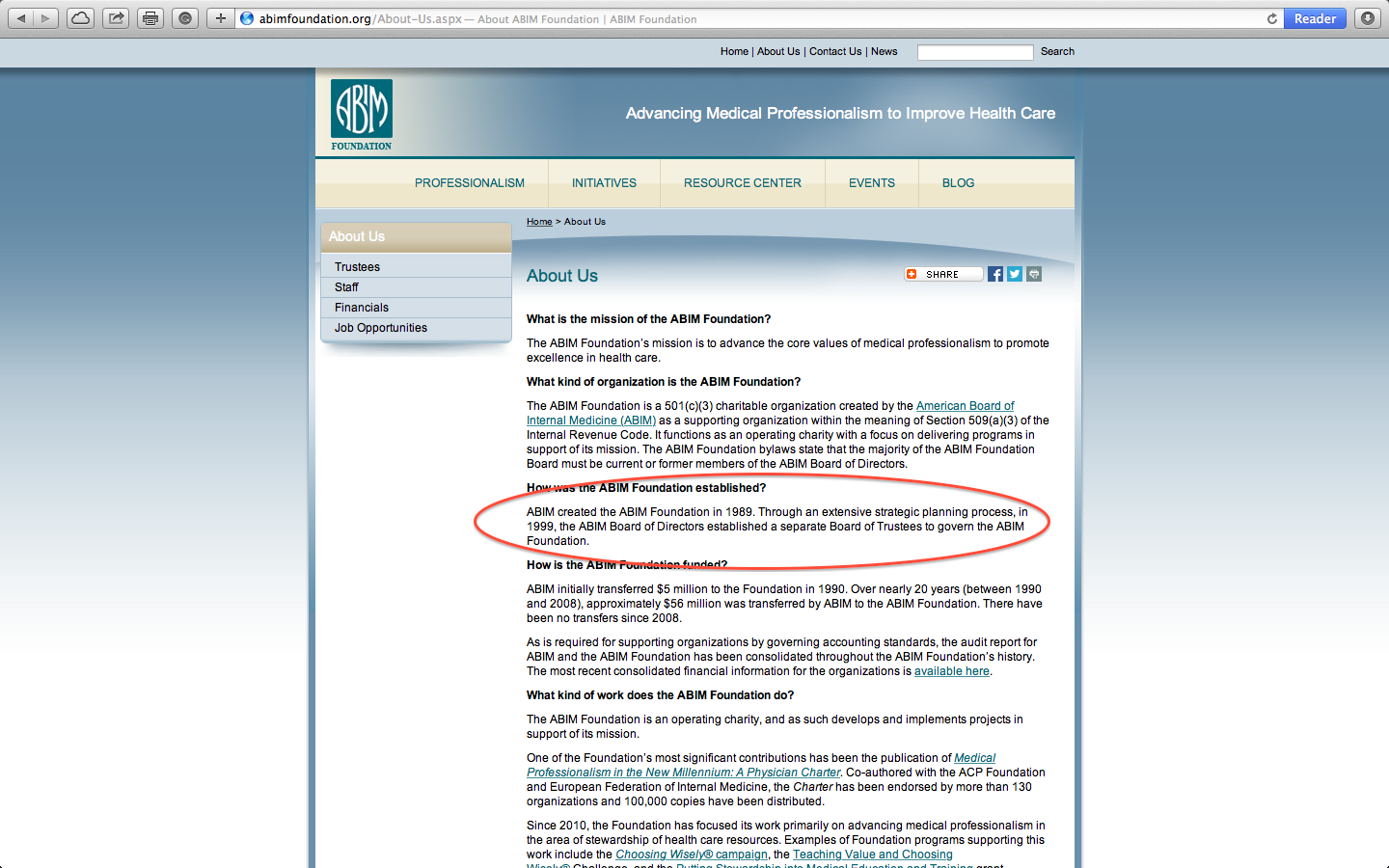
Deception #4: Make up a reason the ABIM Foundation was
"created" in 1999 and delete the web page the stated the ABIM Foundation was "
restructured" in 1999 as an operating Foundation to 'complement' the ABIM." Then be
sure the reason for the "new" Foundation sounds
really sincere - like "
to advance the core values of medical professionalism to promote excellence in health care." (Forget to mention you
created your own definition of "medical professionalism") Who could argue with such a "mission?" Also, make sure to create a
Physician Charter of all your best bureaucratic and academic friends so they can join you at really nice venues to talk about things. Then make sure doctors "Choose Wisely®" treatments that they must forego in the name of "social justice." Once you've done all of these things, no one will ever know (or have time to suspect) where all that ABIM Foundation money came from.
It's a clever way to hide the money trail to the ABIM, it's officers and membership fees paid by the ABIM to the ABMS, don't you think?
(No wonder "it's complicated.")
Now, let's
end the ABMS MOC® program entirely - every last bit of it - shall we?
That would be the truly professional thing to do and every ABMS specialty board today knows it.
-Wes


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}