An important article by Paul Martin Kempen, MD, PhD that critically reviews the American Board of Internal Medicine (ABIM) and American Board of Medical Specialty's (ABMS) Maintenance of Certification (MOC) process recently appeared in the Journal of Anesthesia and Analgesia. Unfortunately, the article resides behind a pay wall. As such, I can only publish a small sampling of the article for discussion here, but I think the points raised are important ones to bring to the public's attention for discussion ( I have also included the appropriate references at the end of the excerpt):
If you have the time, be sure to read the whole thing. I welcome responsible comments and encourage doctors so moved to sign the petition to roll back the MOC process.MOC: RESEARCH VERSUS MARKETINGThe ABMS emphatically stresses that multiple articles support MOC. A quick review of these proffered ABMS articles readily identifies the authors as overwhelmingly ABMS paid executives and/or hired paid consultants.(4,c)These corporate authorships mitigate scientific validity and introduce significant bias into these retrospective data-base interpretations, as would occur for any proprietary medical device or drug.(5) At best, they can statistically substantiate only associations and not causality. Negative studies may never be published. Publication further occurs in journals owned, edited, managed or supported by organizations strongly influenced by ABMS senior staff or national societies, otherwise exhibiting significant financial interests in proprietary and endorsed products associated with recertification programs.(4,c) Executive members of ABMS boards are frequently found to serve as executives of all national medical societies, associated journal editorial boards, and many academic departments. Corporately sponsored/authored publications of both FSMB and ABMS affiliates, financed with the $374 million in ABMS’ gross annual receipts, repeatedly support a significant corporate advertising campaign, without significant opportunity for opposing views from practicing physicians.(6,7)In 2002, the ABMS unsuccessfully attempted to validate board certification itself, via meta-analysis coauthored by 2 ABMS (executive and associate) vice presidents documenting, “Few published studies (5%) used research methods appropriate for the research question,” and “Perhaps one lesson to be learned from this review is the need to thoughtfully examine this recertification process to document its value.”(8) Cochrane Collective Database Review (another quality indicator) also fails to support MOC or board certification validity. The only ABMS-funded prospective randomized study found in the Cochrane database (yet missing from ABMS listing), however, did document “no benefit regarding primary outcome” from the specifically studied practice improvement module.9 These facts together emphasize significant scientific limitations supporting validation of the ABMS program, despite ABMS insistence to the contrary.PRACTICE IMPROVEMENT MODULES—BREACHING ETHICAL RESEARCH STANDARDS?MOC practice improvement modules require physicians to define subset populations in their practice, where patient care might be improved. A plan is introduced for selectedpatients, and changes in care are introduced. Data are collected to specifically demonstrate quality improvements in one’s own practice to the ABMS to enable recertification. This practice improvement modules method is initiated to facilitate the individual physician’s personal certification, that is, personal gain.Practice improvement modules constitute an experiment: changing practice to demonstrate a positive result. This experimentation occurs without any institutional review or written informed consent. Patients unknowingly assume the costs and risks of the practitioner’s experiment. Without IRB oversight, review, and approval, practice improvement modules violate the Nuremberg Code of 1947(d) (safeguarding humans from experimentation) and the Declaration of Helsinki.(e) This represents a significant moral concern. No individual rigorous review of methods, adverse outcomes, risks, or costs is mandated or occurs.As a physician working for an internationally recognized center of medical excellence, I should not be allowed to tamper with proven protocols merely to meet ABMS requirements for my very personal recertification needs. For example, perhaps I want to change my practice to improve (reduce) hemoglobin A1c levels. Thus, I become more aggressive with insulin management to achieve this worthy goal. However, we know that tight control of insulin can be extremely dangerous and the burden of treatment associated with therapeutic complexity and risk of harms increases with lower targets.(11,12) Such experimentation with changing insulin management to meet personal recertification needs may result in fatalities. Is such tinkering with standard practice worthwhile, ethical, or even likely to improve quality?REGULATORY CAPTURE OF PHYSICIANS
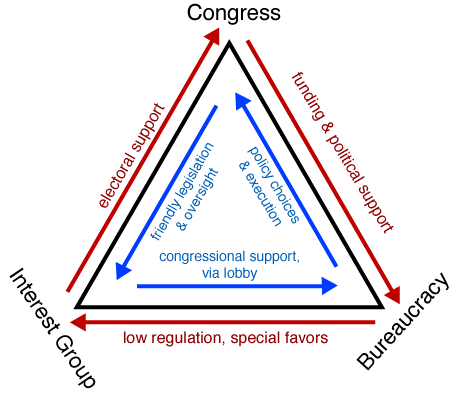
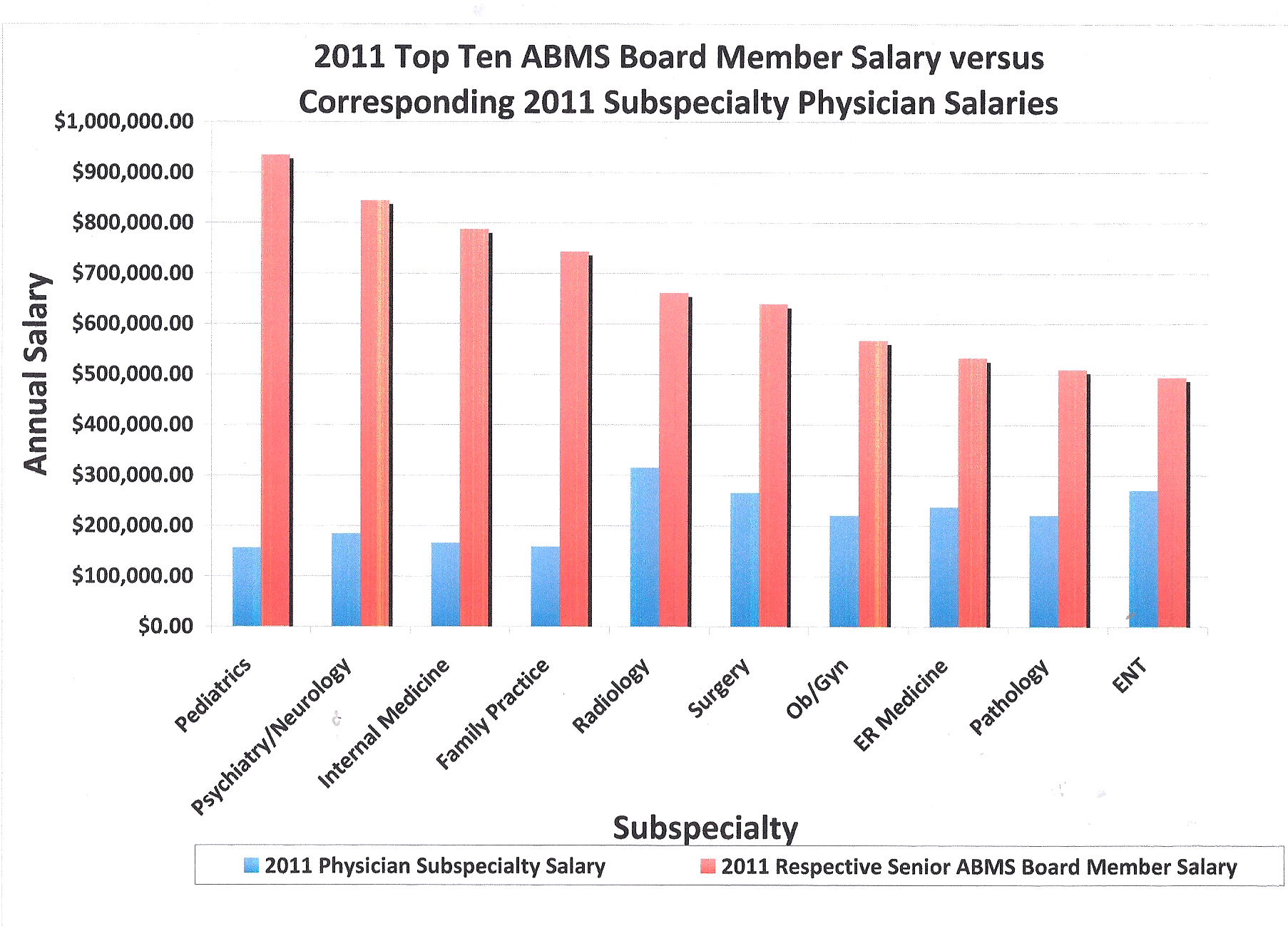
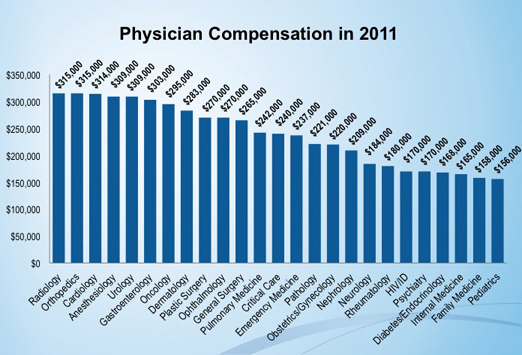
Recent attempts by the testing/regulatory corporation, the FSMB Inc., to legally mandate MOC nationally with testing every 5 years exemplify regulatory capture: monopolies or special interest groups co-opting policymakers, or political bodies (e.g., regulatory agencies), to further their own ends.(13,14) While current board certification is generally a prerequisite for hospital privileges and applicant hiring, informed physicians are now proactively pushing to prohibit bylaws that require recertification compliance as documented by resolutions passed at the 2013 annual meeting of the American Medical Association (AMA) in Chicago, IL. Passage of anti–MOC-MOL resolutions in New York, New Jersey, Iowa, Michigan, North Carolina, Oklahoma, and recently Florida followed Ohio’s State Medical Society’s lead in recent years. These are specific examples of the rising concern among working physicians that unproven certification restrictions and costs are becoming mandated by private and corporate interest groups. These efforts strive to place time-limited certificate holders on equal ground with grandfathered lifelong certified physicians. Nationally, the Association of American Physicians and Surgeons and Doctors for Patient Care have led the opposition, followed by AMA actions at the annual meeting in Chicago, IL, in 2013. Examples of physicians losing hospital privileges and/or the ability to participate with insurance programs including Medicare over recertification have been noted. This led the Association of American Physicians and Surgeons to file a lawsuit on behalf of the national membership against the ABMS in April of 2013 seeking redress on multiple issues regarding conspiracy and restraint of trade (see United States District Court for the District of New Jersey Docket No. 3:13-cv-2609-PGS-LHG). While the FSMB’s MOL program (linking participation to the ability to practice) goes further than the ABMS currently voluntary certification proposals, neither protects against lawsuits nor insures competence, while both limit competition from noncertified physicians and intimidate physician compliance with ABMS programs.(15) The ABA has now expanded testing, which requires mandatory passage of their part 1 test before allowing completion of any residency training program. This undermines any appearance of voluntary participation and provides a clear trend for the future.Renowned contemporary medical leaders simply never need MOC to secure their newest or next position, their reputation suffices. Thus, certification is mostly a marketing mechanism for employment, required by industry insiders and overwhelmingly ignored and unappreciated by the general population. Multiple ABMS executives themselves have published statements indicating long-term failure to recertify or participate in MOC, complying only when it has become a recent job requirement as ABMS officers, individual chief executive officers (CEOs) having been paid 6 and 7 figure salaries (Table 1).(16,17) The chairman of the American Board of Pediatrics received $1,241,588.00 as annual income, when, in 2009, the board’s corporate deficit (expenses-revenues per the 2009 filed Internal Revenue Service 990 forms) was documented at $2,713,406.00.(18)These salaries pale in comparison to the $374 million yearly expenditure for ABMS certifications. The current 2013 ABMS and FSMB physician CEOs were not enrolled in MOC and have never recertified as of January 2013, as verified by ABMS databanks found at the ABMS and ABIM Web pages to verify a physician’s certification. This strongly undermines any personal statement regarding conviction of certification’s personal value versus corporate profits from ABMS programs. One might argue that these CEOs are no longer practicing medicine. However, why should the many administrative physicians be required to submit to the MOL or MOC protocols and costs to maintain licenses necessary to work in administrative or research positions? On the contrary, executives in the certification industrial complex, along with our academic colleagues pushing for certifications, are typically not those practicing full time and maintaining their clinical skills. This push for certifications by executives in the certification industrial complex may be simply reflecting their myopic prejudice arising from their academic distance from practice, when often treating patients only several hours per day, week, or month, if at all. Those physicians near retirement may be economically and inappropriately forced to retire, rather than to maintain a full license and ABMS certification protocol. With the 10-year certification intervals, retirement may become an economic enticement at 10-year intervals from first certification.The ABMS has, nonetheless, actively and effectively lobbied Congress to pass Physician Quality Reporting System-MOC (PQRS-MOC) legislation, requiring ABMS MOC compliance for payment. The ABA openly disclosed that the 0.5% initial PQRS-MOC benefits would not cover the costs of MOC, which is soon slated to become a 2% penalty for nonparticipants. (f) Only 9 specialty boards had fulfilled PQRS-MOC requirements to become providers, leaving all other 15 physician specialist groups (ABA included) exposed to reap only PQRS-MOC’s future penalties, because 2013 is the prescribed index year required for such protections.(g) Only recently did the ABA attain provider status despite openly declining to do so in 2010, declaring then “Based on its understanding of the current CMS requirements, the ABA does not believe that the additional requirements for the MOC bonus will have a sufficient impact on patient care, nor will the reimbursement bonus justify the additional time and resource burden on its diplomates.”(f) Many individual ABMS specialty affiliates opposed transitioning to time-limited programs but succumbed to ABMS corporate directives to comply or lose ABMS accreditation and these exclusive franchise rights.While the ABMS argues that MOC is inexpensive, the ancillary cost of travel, study, time away from patient care, locums coverage, and busywork are quite significant. However, these minor costs are deemed insignificant, if the benefit is a measurable improvement in patient care. The burden of proof for any claim rests with the claimant. If the ABMS believes there is value to offset the costs, then it has the burden of proof to support this claim and this claim remains to be conclusively demonstrated by objective and reproducible means.
-Wes
Addendum 2 JUN 2014: The full article has now been posted online here: http://www.changeboardrecert.com/documents/KempenANesAnalg.pdf
References:
(c ) ABMS Maintenance of Certification® (ABMS MOC®) Updated
March 20, 2013 Myths & Facts. Available at: http://www.abms.org/maintenance_
of_certification/pdfs/ABMS_MOCMythsFacts_3-20-13.pdf . See LISTS 1–5
(Qualidigm, Middletown, CT [Drs. Wang, Meehan, and Ho and Ms.
Tate]). Accessed January 16, 2014.
(d) The Nuremberg
Code. Available at: http://history.nih.gov/research/down-loads/nuremberg.pdf
. Accessed May 28, 2013.
(e) WMA Declaration of Helsinki—Ethical
Principles for Medical Research Involving Human Subjects. Available at: http://www.wma.net/en/30publications/10policies/b3/index.html
. Accessed May 28, 2013.
(f) The American Board Of Anesthesiology, Inc. Maintenance
of Certification and Physician Quality Reporting System Requirements. Available
at: http://www.theaba.org/pdf/MOC_PQRS.pdf
. Accessed February 28, 2013.
(g) Qualified Maintenance of Certification Program Incentive
Entities for 2012. Available at: http://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/PQRS/Downloads/Fully-Qualified-2012-MOC-Posting-Document-Rev-11282012.pdf
. Accessed February 28, 2013.
(4) Chaudhry HJ, Talmage LA, Alguire PC, Cain FE, Waters S,
Rhyne JA. Maintenance of licensure: supporting a physician’s commitment to
lifelong learning. Ann Intern Med 2012;157:287–9
(5) Lehman RS. Nullius in verba: don’t take anyone’s word
for it. JAMA Intern Med 2013;173:1049–50
(6) Kempen P. Maintenance of licensure. Ann Intern Med2013;158:219
(7) Chaudhry HJ, Talmage LA, Rhyne JA. Maintenance of licensure-Reply. Ann Intern Med2013;158:219
(8) Sharp LK, Bashook PG, Lipsky MS, Horowitz SD,
Miller SH. Specialty board certification and clinical outcomes: the missing
link. Acad Med 2002;77:534–42
(9) Simpkins J, Divine G, Wang M, Holmboe E, Pladevall M,
Williams LK. Improving asthma care through recertification: a cluster
randomized trial. Arch Intern Med 2007;167:2240–8
(10) Vollmann J, Winau R. Informed consent in human
experimentation before the Nuremberg
code. BMJ 1996;313:1445–9
(11) Finfer S, Liu B, Chittock DR, Norton R, Myburgh JA,
McArthur C, Mitchell I, Foster D, Dhingra V, Henderson WR, Ronco JJ, Bellomo R,
Cook D, McDonald E, Dodek P, Hébert PC, Heyland DK, Robinson BG; NICE-SUGAR
Study Investigators. Hypoglycemia and risk of death in critically ill patients.
N Engl J Med 2012;367:1108–18
(12) Lipska KJ, Montori VM. Glucose control in older adults
with diabetes mellitus–more harm than good? JAMA Intern Med 2013;173:1306–7
(13) Federation of State Medical Boards. Report from the
Maintenance of Licensure Implementation Group. Euless, TX:
Federation of State Medical Boards, 2011
(14) Dal Bó E. Regulatory capture: a review. Oxf RevEcon Policy 2006;22:203–25
(15) Wallace DA. Occupational licensing and certification:
remedies for denial. William Mary Law Rev 1972;14:46–127. Available at: http://scholarship.law.wm.edu/wmlr/vol14/iss1/3
(16) Johnson DH. Maintenance of certification: confession of
a grandfather. J Oncol Pract 2012;8:203–4
(17) Brennan TA. Recertification for internists–one
“grandfather’s” experience. N Engl J Med 2005;353:1989–92
(18) American Board of Pediatrics. 2009 IRS 990 form, part
VII. http://www.changeboardrecert.com/tax-returns.html
. Accessed January 16, 2014




{kind=link}