What is remarkable (yet not the least bit surprising to those of us who have been in the business of medicine for a while) is how insurers dismiss the importance of discussions that are held by those of us who attempt to explain the pros and cons of the various new medications to our patients. We see these conversations completely invalidated as soon as the insurance industry renders their "coverage decision." Discussions are immediately invalidated, the pros and cons of each medication ignored. Meanwhile, these same insurers bear no reponsibility for potential safety issues that might arise when their made-up care process is implemented. And there is no accountability, no person ultimately responsible.
When a doctor tries to call and speak with someone about their policy, we meet hushed tones that promise to approve the prescribed medication if we just send a letter explaining our rationale. Yet despite this effort, they stick by their policy nonetheless.
What a waste.
So I'm sending a few questions to Aetna about their new "coverage decision" regarding the new oral anticoagulant, apixaban:
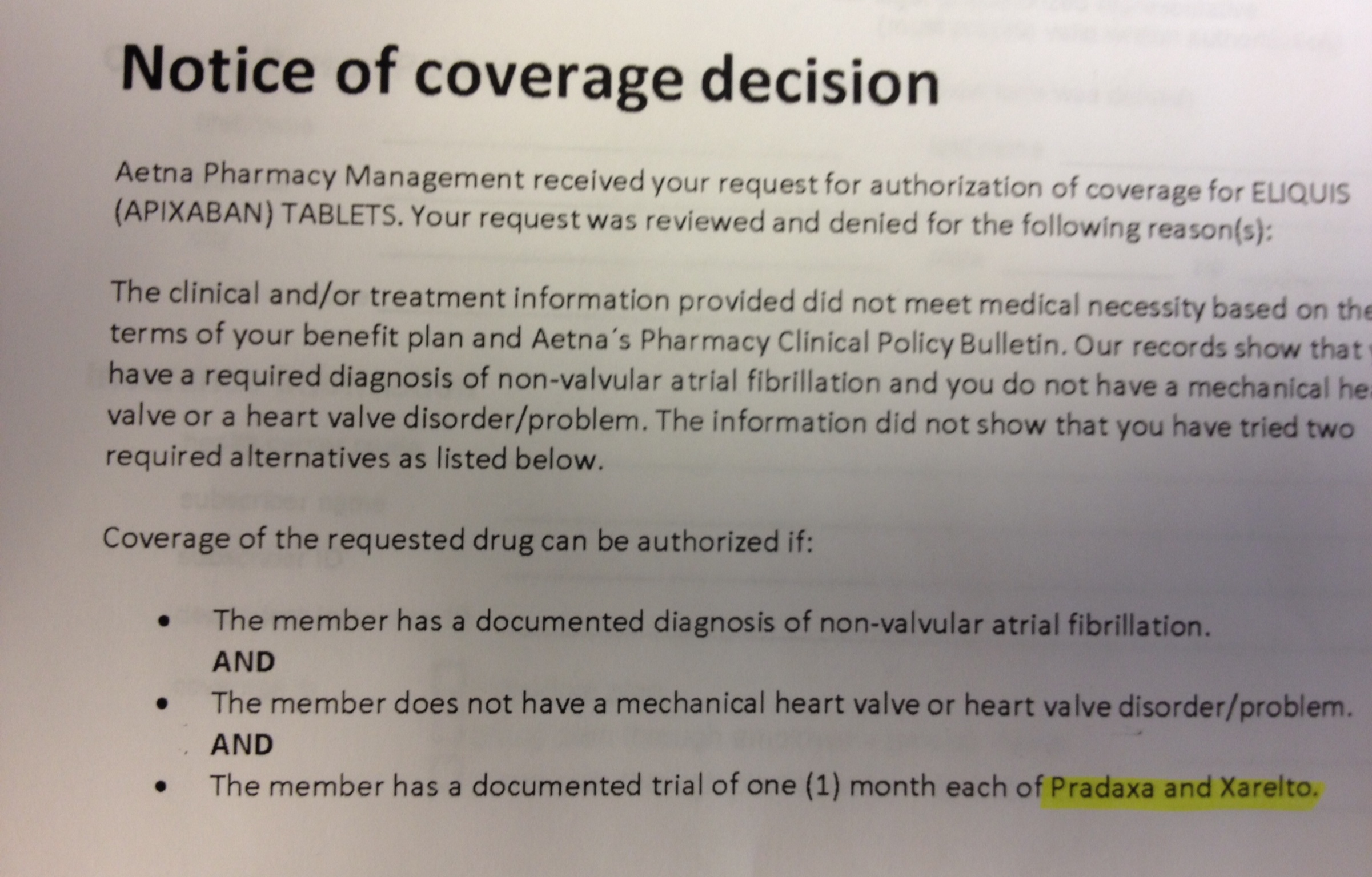 |
| An Aetna 'Coverage Decision' (click to enlarge) |
Dear Aetna Pharmacy Management:
- When my patient has a GI bleed from Pradaxa, will you explain to them why you insisted I start this medication?
- When my patient gets nauseated from Pradaxa, will you take the call at 3 am and write the new script for him or her?
- When my patient accidentally overdoses on Xarelto thinking it was a twice a day drug like Pradaxa, will you explain to the plantiff's lawyer the safety of your non-evidenced based practice of switching anticoagulants on a monthly basis?
- Along the same line of reasoning, where I might find data pertaining to the safety of monthly switches of anticoagulants in the world's literature?
- Is your effort to "manage" physician-prescribed medications in the patient's best interest or your stockholders'?
- Where can I send the bill for the wasted time spent by my staff and me to jump through your self-imposed hoops?
With sarcastic love of all you do -
-Wes
2 comments:
Interesting that you don't put your patient on warfarin, apixaban does not have a lower risk of GI bleed
"4. Compared with warfarin, apixaban does not significantly alter the risk of major GI bleeding. " www.thrombosis-online.com on 2013-07-30 | ID: 1000467415 | IP: 128.104.209.200. I am an anticoagulation Nurse Practitioner in the VA system which approves with very strict guidelines.
K. Moore -
Whether apixaban, rivaroxaban, dabigatran or warfarin, the risk of bleeding regardless of drug chosen is about 3%/year. Certainly intracranial bleeds are slightly less common with most of the NOACs, but only slightly so. Is that worth it to the patient? perhaps.
We spend the time to have careful discussions about cost and potential side effects of each of these drugs with patients.
My point here is that none of this matters to insurers who bear no responsibility for the care of our patients. More importantly, their drug denial policies may be exposing patients to serious safety issues when drug "equivalents" aren't so equivalent after all.
Post a Comment