For $812,000 a year and countless lost hours of patient care and financial mismanagement, you would think he could do better than that.
Instead, Dr. Baron justifies the ABIM's actions on the basis that the ABIM was "preserving and protecting self-regulation at a time of change... otherwise it will be people, not physicians, who drive what all the expectations are for physicians." He claims the ABIM helps physicians "communicate to the public ways in which they communicate to the public that they have skills and that they have knowledge that other people don't have." As if physician's degree and training and countless years of experience and nights on call aren't enough.
According to Baron's own words, it appears the ABIM is little more than an exceedingly expensive marketing team working on our behalf.
But the real evidence of whom the ABIM has been working for can be found in the financial, political, and strong-man tactics used by the ABIM over the past forty years since "continuous" certification was conceived.
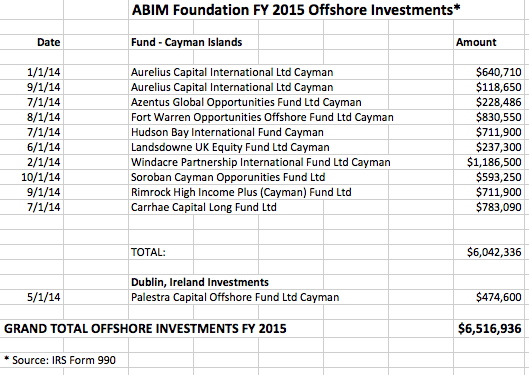
Dr. Baron never mentions the ABIM's secret transfer and cover-up of $55 million dollars taken from working physicians' test fees from 1990 to 2008 to create the ABIM Foundation and how the Foundation has moved a portion of those funds offshore.
Dr. Baron never mentions that the ABIM spent hundreds of thousands of dollars lobbying Congress to assure a perpetual money flow to the organization and hid these actions from the IRS to avoid paying taxes.
Dr. Baron never mentions that within all of their propaganda research the ABIM or ABIM Foundation never (once) studied the negative psychosocial effects of failing even one of their unjustified MOC examinations, nor the potential negative effects of cost saving initiatives promoted by the Foundation's "Choosing Wisely" campaign for the individual patient. He never mentions that 13.2% of clinically experienced physicians tested by their unproven metric failed their examination on their first try to the financial benefit of the ABIM and their partner professional societies.
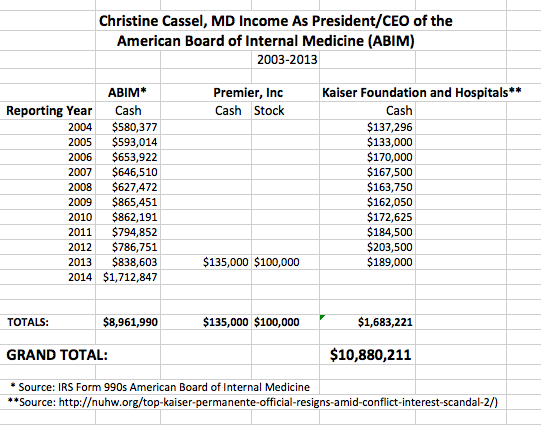
Dr. Baron never mentions the his predecessor, Christine Cassel, MD, earned $10.88 million (nearly $9 million of that amount from ABIM diplomats and an amount that included spousal travel fees) during her 11-year leadership at the ABIM and ABIM Foundation. Nor does Dr. Baron mention Dr. Cassel's long-standing conflicts of interest with Premier, Inc or Kaiser Foundation Healthcare and Hospital system. Nor does Dr. Baron mention Robert Wachter, MD's conflicts of interest with IPC Hospitalist company that is now under federal investigation for overbilling Medicare.
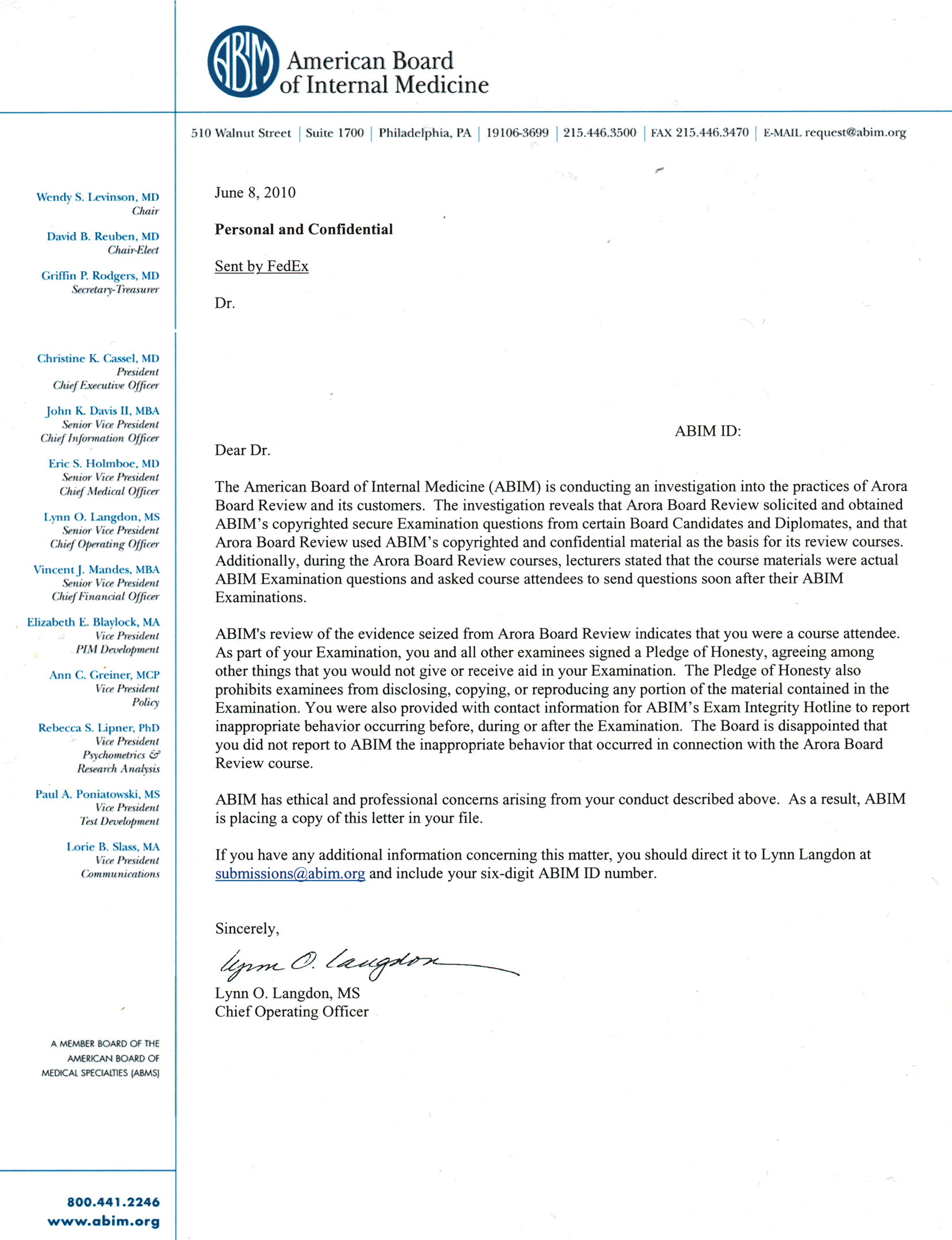
Dr. Baron also fails to mention how serious they are about protecting their monopoly - that they even use Federal Marshals to raid homes and seize assets, call physicians cheaters, then collect an amount estimated to be $3 to $4.5 million in hush money to justify their program that has "no robust evidence." He fails to mention have 139 physicians were sanctioned because the ABIM felt doctors were the one cheating. He also fails to mention that the ABIM continues to track down and hunt physicians from as far away as Puerto Rico some four years later after publishing their one-sided account of details of their raid in the Wall Street Journal for their benefit "as a message and a deterrent."
But not all of the blame for the acceptance of MOC as a facade for physician competency rests with just the ABIM. The American Board of Medical Specialties (ABMS) and the Accreditation Council on Graduate Medical Education (ACGME) that has quietly insisted on this credential for hospital and graduate training programs just so they can assure they receive more money from Medicare deserves blame as well. Their lack of leadership to expose the egregious behavior of the ABIM is at least as concerning, if not more so, for our profession and society.
-Wes
* Note, it appears this ABIM video was published in 2014, not 2016 as I first published. I regret the error and have corrected the post. Thanks to the anonymous commenter to corrected the date. Hopefully that same commenter will address the other issues brought up in this blog post as well.


.jpg)
{kind=link}
{kind=link}
{kind=link}
{kind=link}