For their 80th Anniversary Jubilee Year (assuming they're still in existence), maybe ABIM can reinstate the 1936 fees for all ABIM diplomates and the ABIM officers and staff can accept the same compensation as the ABIM principals did in 1936. Since "Professionalism" is a key characteristic that ABIM wishes to promote among practicing physicians, they could start by improving their own.
Regarding the MOC pass fail rate study: it is better to publish on a reputable site like "Dr Wes" than in a journal that may or may not have some conflicts of interest involving folks at the ABIM and ABMS.
That's my opinion after looking at the other 'outfits' who seem to keep the seal on talking transparently about corruption in 'medical bureaucracy land'.
It's a shame that the historical founders, i.e., the membership societies like the ACP and AMA, have not presently admitted seeing any irregular behavior or conflicts of interest at the ABIM; or even that they might exist.
Or that serious wrongdoings may have occurred within any of the offshoot "membership societies" of the ABMS.
I mean, for this discussion the ABIM in particular, but coi and compensation excesses should be on the lips of all executives and in all the medical journals as a full page ad by now.
Put your money to work on ads in papers and digital media sites; it will be money well spent. Or ask that they be placed for free as a public service announcement.
It is much more important to make coi and excessive financial inurement a poster child issue rather than just hand washing, as coi and excessive inurement represent the essence of having dirty hands.
Thank you for publishing the pass/fail results here, although I found them extremely disturbing.
We would like to read an expanded discussion of the MOC pass/fail rate study sometime. Perhaps you can add a hyperlink.
The only folks who did as well or slightly better during 2000-2014 are behind bars now. They were Wall Street insiders who not-so-cleverly broke trading laws and Ponzi scheme scam artists.
One prosperous offshore hedge fund manager that is not behind bars is George Soros. He did very well with his Quantum Fund but we only have data through 2011 on him. I'll explain why in a moment.
Soros has some strange unexplained link to the ABIM and its Foundation. That's why I mention him here. One (or more)of his foreign/domestic NGO's received grants from the ABIMF. Odd that an organization associated with Soros would need money from the newly formed ABIMF.
I challenge the ABIM to publicly explain this Soros affair.
George Soros' who created the Quantum Fund in 1973 did quite well for his undisclosed list of world elites, names like Roth****** and the Queen of E******. Managing this fund from 1973 to 2011, Soros returned roughly 20% to his highly elite client investors annually.
He did this by manipulating markets or acting only when he had insider knowledge.
Soros allegedly ravaged markets in Eastern Europe and often influenced events in vulnerable emerging markets to benefit his investments. Soros' Quantum Fund decided to shut down based on "new financial regulations requiring hedge funds to register with the Securities and Exchange Commission."
That meant transparency and disclosure, which would put severe limitations on cheating--if there was any.
The only ABIM person I track with even better results (because they benefitted in tandem with ABIM's increased fees during this time period was the ABIM's own CEO/President/lobbyist Christine Cassel.
The ABIM has a top-heavy executive overhead with most of the money being sucked out of the ABIM and ABIMF bank accounts by a handful of executives and about 50-60 other principal players.
All salaries were high six-figure salaries approaching a million on down the pyramid. Cassel left ABIM in 2014 with a surprisingly large amount of deferred compensation just in time for her 70th birthday, which is distribution age.
1.7 million 'smackers' if I recall.
Great timing and financial planning on the part of the Board Chairman/CEO/President, namely Cassel herself.
More examples of ABIM corruption at its finest?
With ABIM pass/fail rate in the dumpster y over y, cheating on tax filings, sky-rocketing legal fees, and at the same time increasing all executive compensation and giving a golden parachute to Cassel! Ugh.
Was the 1.7 deferred check and multi-million ABIM(F)payday totally excessive?
Or was it justified compensation?
Or was Cassel cheating on her hard-working physicians?
Was the Kaiser Permanente/Premier, Inc. high board seats collecting millions of $ at the same time a conflict of interest?
The Jubilee year 1986 should have been spent celebrating the dissolution of the organization.
It is stated in the 1936 bylaws that ABIM would be administratively dissolved in 1986 or sooner.
That should speak volumes about the original mission and the integrity of the founders.
The entire ABMS group of specialty boards should understand the original mission as well. It was a time-bound mission to establish a society of scientific medical subspecialists--physician investigators, if you will, serving the public and creating a certification process.
That is all. An initiation into a society of medical scientists and a certification for life.
The ABMS Today
ABMS is now comprised of strangers creating a strange land out of the medical landscape. Whatever is said or presented by the ABIM one must understand that the truth is really in the opposite of what they say.
Truth is a lie and a lie is their truth. Choosing Wisely is not what it says it is. It is the opposite. That is one of the crudest forms of lies imaginable.
It was never intended to be like this with executive positions, huge bureaucracy, and huge money expectations. It was truly voluntary in the beginning and should be today. Let's move back in that direction.
To be of the profession and for the patient. That implies lifelong learning and CME. The ABMS just gets in the way of it. The are creating a big shadow from their towers of wealth. They are not towers of health. The profession is diseased by bad heads teaching nothing except about their greed and avarice. Raw power. Politics.
Yes, let executives work for the original compensation, which stated no personal inurement.
Zilch!
How's this for a new direction and a new way of thinking?
"I would be glad to serve just for the honor of serving; but only for a year as was originally intended."
Or just dissolve the organization if too much time is spent denying and defending fresh lies heaped on the old till the end of time (in perpetuity).
Presidential hopeful reading from his new tax plan. -Page 4.
Item 216. "A nut is a nut and will cost no more than a nut!"
Item 217. "Cost Reductions in Government and the 'Quality Assurance' Medical Bureaucracy."
"I'll take questions now."
Q. I was just reading your new tax plan. If you are elected president of the United States what would you do about the ABIM and ABMS mess?
A. "Did I hear you correctly...the executives make how much at the American Board of...?"
Q. Yes sir, the CEO makes nearly $x,xxx,xxx for a 35-hour work week!
A. "Oh, yes, those ABIM folks with the luxury condo and chauffeur! I know those political phonies well and they're bogus Choosing Wisely BS.
If I were president right now, I can guarantee you they'd be paying taxes--big taxes and fines for that kind of criminal lie...and they'd be paying back those docs from behind prison bars."
Q. Isn't that a harsh penalty for their type of fraud?
A. "You've never heard of the ABIM Foundation apparently! Don't get me started. Those stupid bozos will be crying for mercy in front of a Federal Judge of the Eastern District before the week is out...they've had their chance to...just slash all the executive positions! They're fired. And keep 'em out of my sight! We'll find real good jobs for the rest of them and make our country great again...
Q. But do you have the authority to fire them, sir?
the whole world of CME scam starts on the basis of premise that the time spent by a physician on books / researching while treating a patient cannot be counted as CME . WHY ? who promoted this stupid idea. the best a physician can do to the world of medical education and patient care is read and research when it matters the most. it is time to bring that truth back into medicine. Count the CMEs for what matters the most. make the insurance companies pay for what time we spend on reading and patient care both. STOP. the scam in medical education is over. the whole world of AMA/ACP/ABMS is finished. it is time to expose that one line which destroyed the definition of Continuing medical education. it time to reimburse the physicians and all other professions like the lawyers are reimbursed.
This is ready for press in the New York Times, Wall Street Journal, Washington Post and on the TIMES SQUARE NASDAQ TICKER SCREEN
The War Has Ended. Let the parade begin.
"The scam in medical education is over!
The whole world of AMA, ACP, and ABMS is finished."
The Surgeon General has spoken.
In other news...in an ideal world... The CMS has agreed to pay for physicians' time spent on the phone counseling patients and writing prescriptions. The CMS has decided that phone consults and prescription services (for patients who claim they cannot make it in to the doctor's office or UC) is a form of telemedicine and will reimburse providers at an appropriate rate.
The CMS also declared it will no longer be wasting physicians' precious time with preauthorization and denials. MD means making decisions and medicine should be left to the physician not insurers to decide. This bad practice complicates patient visits, creates confusion, delay, increases morbidity, death, and decreases quality of care overall.
Healthcare systems will run much better and the patient will be safer. There will be tremendous cost savings from ending this pre-emptive approach to managing fraud and overspending on medications. It simply does not work and puts patients health in jeopardy.
CMS recommends the same to all insurers. No more bureaucratic red tape which only creates time constraints and costs taxpayers additional money to administer the policy. The savings will bring much needed revenue for other much more important work in providing increased quality of coverage and care to seniors (and veterans) where it counts.
Formularies will be fully populated with all medications and made available. Studies have shown that highly trained physicians as we have today need to have the right tools when they need them to keep pace with advances in science and the increasing demands to administer medications and care when needed not after the patient condition has deteriorated, become frustrated to hell, or deceased.
(Insurance companies who create any such onerous additional burdens on providers creates a bottleneck in national health care. Offenders can be reported via the CMS.StateHealthCommission.gov or our hotline directly connected to your state insurance commissioners office with call-back and follow up calls provided as a public service to patient and physician.)
Recommendations made by the Surgeon General in his war against bureaucratic fraud and real waste in medicine caused by the corrupt quality assurance racket. The SG is looking to recover a quarter of a trillion dollars by 2020 in eliminating these robber barons.
Questions: Topic: Who created/signed off on ABIMF originally in 1989/1999? Where did the money come from and so on. How was it invested. Who formed the relationship with 1838 Investment Advisors.
Who actually transferred funds to the ABIMF? Who was ultimately responsible for decisions and who acted.
Who personally was involved in the momentum equity trades for over a decade using surplus physician fees? This money was actively traded to look like less equity trading took place than actually was the case. Yearly window dressing? Or something else?
Did 1838 Investment Advisors do this high risk/high gain investing as a courtesy for their non-profit clients? There was more than one specialist involved in non-profit portfolio management at 1838. Which one handled ABIM's account according to documents you have? Who sought out this arrangement with 1838?
As you may know 1838 Investment Advisors was founded in 1988. What part did 1838 Investments have in guiding the financial planning of the ABIM and ABIMF? What percentage of money was transferred over time to ABIMF from profits/winnings involving their risky bets that paid out big for the period up until the circa 2001 collapse of the markets? Especially bloody were many tech stocks that ABIMF held since at least 1991/1992, with new positions being acquired quarterly over a decade. According to more recent ABIM tax documents when 1838 was still a viable enterprise managing money for ABIM, you can clearly see the trading of tens of millions and you can see the heavy losses over three and four million dollars in consecutive years..
These losses were mitigated somewhat by selling longer term holdings with large gains. This buffered the accounts glaring losses, which were substantially more than the realized gains. Then the trading stopped abruptly when 1838 Investment Advisors went belly up bleeding at the gills.
Did the ABIM's CFO or any other officer have any direct handling of the account and the manner or style in which it was managed?
Was there attempted intervention to preserve capital by the ABIM CFO at any time and halt the heavy trading of risky stocks? Mutual fund holdings were also managed by 1838 Inv Adv and were traditionally a trading vehicle as well for the firm.
Why did ABIM officers allow investing in risky stocks with negative PE's or in the low to high hundreds like JDSU, AOL, CSCO, etc. They lost big in the early 2000's on these trades. They were caught with their pants down and rode the equities down realizing losses of nearly a million dollars each on TYC and JDSU. Half a million on CSCO. They lost big on MSFT, TI, MU, INTC, AIG. The losses were staggering.
Covering over some of the losses on the tax forms are the substantial gains of shares acquired from the previous decade. Trades are a bit difficult to follow due to the trading style of 1838. The trades go on for page after page with the statements added to tax filings. Has anyone audited these forms from the 1990's and early 2000's for irregularities beside the trading?
Did 1838 utilize a stop-loss order/policy on the ABIM investments or did ABIM request to have any safety net when riding such wild stocks in emotionally exuberant markets?
As I mentioned, in the 1990's they purchased equities and made large gains, what was the level of risk specified by the non-profit managers and what discussion took place with ABIM officers about this momentum trading? What did ABIM state as to their risk tolerance as is required by brokers/managers.
Does ABIM retain discussion of these financial decisions and other discussions related to it?
Do they keep records of their board meetings and private decision-making in general?
Past president Kimball signed nothing related to the ABIMF registration document in 1999. Why? Only Christine Cassel the Chairman of the ABIMF signed it. It is strange to me that Kimball would not sign also. Documents as important as that and he did not sign draws up my hackles. Anybody have any personal stories to relate about past president Kimball?
Neither did the past ABIM president Benson in 1989 as I will show below.
The 1989 ABIMF registration document bears the name and address of the incorporator: Henry F. Strozeski C/O American Board of Internal Medicine 3624 Market Street, 2nd floor Philadelphia, Pa. 19104
What are the implications of the above formation/registration document when a financial officer's name appears on the document in this manner and he is the only officer named. Strozeski is named as the incorporator with and in care of address at the ABIM's past offices on Market Street?
It strikes me as odd that the president would not also take credit or bear responsibility in any transparent company dealing with revenue and a good deal of profit.
Is the ABIM or ABIMF engaged in any document destruction routinely. What is kept from the past and how far back are documents preserved? What is required legally?
Seemingly in constant litigation, is ABIM required to retain and not destroy documents?
Hi Wes, Your data analytics continue to amaze everyone I share the data with and it continues to cement the notion that this entire cottage industry is rife with obvious corruption, nauseating cronyism and worst of all professional cannabalism. It is obviously clear that the ABIM and their MOC process are woefully flawed and the leaders in charge of that organization have lost their stature. The simmering rage at the ABIM will lead to more formal forms of conflict resolution- official complaints with the Federal and State Governments, defunding of their operations etc. Keep up the great work shining a blinding white light into the dark corners of one of the most corrupt Medical institutions in recent history. And let this be a loud warning to those organizations that pretend to hold a monopoly on altruism and morale behavior but hypocritically behave just like the ABIM.
I often wonder if organizations like the ACC, HRS, ABMS, AHS would stand up to the moral stress test imposed on the ABIM. Do we think that the ACC and the HRS can hold its head up high when it comes to fiscal responsibility and financial modesty? Aren't the conflicts of interest at the ACC truly disturbing? Harlan Krumholz MD FACC is a leader at the ACC and at the ABIM 2020 working group. Does anyone else feel this is hypocrisy and morally wrong? Why such a lukewarm rejection of the ABIM by the ACC? Why do any of us support a dour organization like the ABIM? They have never supported clinicians and have lived off our sweat equity for too long.
I just received notice to pay my ACC membership fees that I have annually forked over for the last 17 years. I wonder where all this money goes and who gets to spend all of it. I wonder if I am getting my money's worth. I wonder if we looked into the ACC's books, would we find lavish spending such as condos, limo service, trips to the Four Seasons?
Such behavior cannot stand the scrutiny of the Internet. I hope I am wrong about the ACC and the HRS.
Wes, if there is a Lasker Award equivalent for a physician who has forever changed the way we look at professional administrator physicians, you would be immediately nominated. I hope we look back at folks like you, Charlie Cutler, Ron Benhasset and realize that courage, morality, and a ethical compass pointed at true North are underappreciated qualities.
Bravo to you and all of us who continue to insist on accountability and transparency in a massively disappointing era of American Medicine.
If we could only exchange the benevolent paternalism of the ABIM for the AFL-CIO or Teamsters. Of course, we'd have to put up with the same corruption and all, but at least we'd get great benefits and leadership that actually looks out for us.
S on assignment in Chicago and Asia Field Office
said...
The Globalization of Medicine, ABMS International (You are invited to visit their 'current' website.) http://www.abms-i.org/
Using their 'ethical compass' pointed at true North the ABMS is looking to increase revenue with a wholly-owned subsidiary called ABMS International. They are hoping to spin it off someday, but growth is spindly as the franchise meets a lot of global resistance so far.
It appears to be a trust and stress issue regarding anything that demands more time, money, and extra busywork spreading the 'quality assurance' word according to the..."what do you 'guys' call your medical assurance firm again?"
According to the kind organization spokesperson ABMS has only established their important work in Singapore so far. Mostly in education and initial certification after residency. "MOC may be coming next we hope."
But they related they have high hopes for other areas like the Middle East, as well. "Maybe Qatar; they have expressed an interest. We have projects elsewhere in the works, but perhaps Qatar will hopefully listen and be adopting soon."
According to fairly recent and 'reliable intelligence' there are a number of training camps and suitable apartments still available for MOC training programs in Qatar.
But note right now the AMBS is warning its international teams to watch their backs closely for 'friendly fire' as they engage the Middle East in the global war against medical chaos and unprofessional behavior. It is also written in the overseas training manuals that they are engaged in risky business in trying to improve the quality of medical care through cost reduction plans, such as "Choosing Wisely".
Europe for now has expressed doubt about American assurance programs and MOC US, because they have had enough of US bullying in international affairs to last a decade according to some "weak political crybabies" in the European Union (who wish remain anonymous).
"Just stay out of medicine; you already control everything else, they say."
Now let's fly to Singapore and stay at a luxury hotel and shake hands with Asia and spend a lot of greenbacks in the process. It's a reasonable cost for doing business.
Here's an update from the Singapore Journal of Medicine as of April 2015! (excerpts: three paragraphs, with full article link below)
"The regulatory climate in Singapore currently does not require recertification through participation in an MOC programme or sitting for an examination – yet. However, similar to the requirements of most state medical boards, documentation of participation in accredited continuing medical education sessions is required for renewal of practice certificates (licensure) by the Singapore Medical Council (www.smc.gov.sg). Unlike in the United States (US), medical boards and credentialing committees of Singapore-based hospitals and clinical institutions currently do not require staff physicians to undergo MOC programmes or pass recertification examinations. However, the institution of residency training programmes, along the lines of the US programmes and certification examinations modelled on ABMS, may result in future Singapore-specific MOC programmes. Generally, academic medical institutions require staff physicians to be current with their specialty certifications in order to have practice privileges. Moreover, physician-educators are also usually required to be current with their certifications.
CONCLUSION
It is inevitable that continuous professional competence assessment, recertification, re-licensure or revalidation will come to Singapore. While we continue to debate the relative merits, I think it is more important to determine the methodology of doing so, without duplication of efforts. Singapore is a small country and the professional community is small in number, even smaller when considering specialties and subspecialties. It is clear that the professional societies and regulatory agencies will not be able to implement credible and non-controversial programmes. To increase efficiency and productivity, and reduce costs to the Singapore society, it would be better to outsource this process or work with larger professional bodies. Physicians should be able to choose a programme that best fits their scope of practice. However, it is likely that, besides the efforts put in by physicians themselves as a commitment to professionalism, the economic price will be borne by patients in the name of public assurance of medical competence and safety. If the burden becomes too onerous, one can always become a banker.
Endnote: The ABIM programme changed slightly from January 2014. It now reports certification status and 'meeting MOC requirements'. Diplomates have to continuously achieve MOC points to meet the requirements."
ABMS International, LLC, a wholly-owned subsidiary of the American Board of Medical Specialties, provides international services relating to physician certification. The American Board of Medical Specialties is a not-for-profit organization and has assisted its Member Boards in developing standards for physician certification in the United States since 1933.
Dr Fisher- I am not a physician, but I have read much of your blog. It is a rare compendium of medical news with references to research that you and others have engaged in.
The worst bits have been the news about how the ABMS has gained so much power in such a short period of time--a few decades only--and how they continue to dictate such onerous policies. I really can't understand why this has not been stopped immediately by authorities.
I can tell from reading your blog that you are a family man with strong values and that you love your country and profession. You seem fair and honest to me.
I sometimes wondered why you spent so much time on the ABIM. I'm not sure they are worth it.
Then I happened upon a blog where you introduced your daughter to an average workday. It was splendid to meet such a bright caring person coming to witness your world as a physician. That one blog and many other blogs here helped me also to see and have a taste of all the changes in medicine.
I understood something clearly at that point. I'll try to explain. I was touched by your daughter's comments about all the typing you do (I remember the days of dictation and paper charts in offices and hospitals). Then the emotion struck home to me that we must stand up for what is right, good, and true for our children. Strive for it in medicine and in life. Not let them inherit a world that is less than what they deserve (or we deserve today)
You might not understand what I mean, because it was a dual perception of how things are and how we would like them to be. I wish the people at the ABIM would just talk to all of you openly. But I understand the complicated nature of the organization and so many things I can't even imagine that are involved.
Anyone with children can understand why you persist in trying to bring to light the embedded culture at the ABIM, ABMS, and the other organizations I never knew existed before. No one even knows about the ABIM, for goodness sake.
I don't want to say it is like a shadow government exactly, but it certainly appears to have been doing things beneath the radar without any oversight. I would say that medicine has a shadow bureaucracy that I don't agree with at all.
And all the executive compensation is ridiculous when most of us struggle on a small fraction. I won't address the corruption, because it was not my point in writing, but I would hope that it is investigated and cleaned up.
Please, I hope others in medicine will stand up and not let this inequity of money, power and politics to continue.
I saw a video of Dr Cutler(?), someone mentioned. He has very valid points and people should see it. No vetting for conflicts of interest stood out, cost of buying condo and maintaining versus renting an apartment with pool. So many good points. I'll bet you my daughter could run it better with complete transparency, and completely fairly. She is bright and looking for work.
I am a property manager, by the way, with a masters in business. A neighbor who is a doctor showed me your site.
Thanks for your nice note. I think the reason I persist in this endeavor is because, like you, I care about medicine being a profession of integrity and honesty, not lies and half-truths. We are talking about a system of re-certification that uses fear to exact large sums of money from physicians, has the ability to destroy careers, has (in my view) stolen from vulnerable practicing physicians to fund a shadow organization that purports to impart "social justice" imperatives and re-distributes grants to groups that promise to "teach physicians" about cost savings and some skewed definition of "professionalism" that ignores honesty, transparency and integrity. I'm not sure I've ever seen such corruption by a group of (supposedly) peer physicians. It's deplorable and inexcusible, IMO.
Granted, not all physicians in these organizations are bad people, but our specialty board system has become bloated and self-serving - full of unaccountable burned-out academic and practicing physicians that no longer see patients but are more than happy to criticize the colleagues with whom they have no idea of their scope of practice and coerce them into paying handsomely into their scheme of quasi-quality in the name of "public good."
I train residents and fellows and like to think I lead by example. I'll be damned if the profession of medicine is going to go down some financial/busy-work rabbit hole in the name of a funding this broken, bloated, and self-serving ABMS/ACGME/JCAHO/FSMB bureaucracy. We are better than this and these bureaucrats need to wake up to the fact that their methods are now understood and bright shining lights will continue to illuminate their activities.
Like you, I have no idea why the IRS, state Attorney Generals, or OIG of the Department of Health and Human Services has allowed such transgressions to occur for so long and only hope that a formal investigation of these organizations will be forthcoming by the authorities. I eagerly await the anti-trust suit ruling by the AAPS against the ABMS as well, for this might be the stake in the heart of our Specialty Board monopoly that is a deplorable example of what physicians should become.
Here's to physicians and patients waking up together! Thanks again for taking the time to noctice and comment.
Thank you for keeping the pressure on the ABIM. However, we are fighting a hydra. For every head you try to battle, there are many others.
1. Witness the new ICD-10 incarnation. This has been a horrible disrupter of clinic flow this week. It adds NOTHING to patient care and only serves the bureaucrats with their databases who can sell their information to CMS.
2. No matter how you feel about planned parenthood, seeing a political operative (bureaucrat de jour) from Nancy Pelosi's office paid $600k is upsetting. As an interventional cardiologist who is paid less, I would feel better about her salary if she had to get out of bed in the middle of the night to perform an abortion and only had 20 minutes to be in the office. Don't forget the press ganey scores to boot. Does anyone remember Obama criticizing cardiologists (vascular) who cut the legs off diabetics for a buck. Here is the CEO who is paid handsomely from government funds for ending lives--pure hypocrisy.
3. Can you graph the inflation adjusted reimbursement for cardiac cath or stent implantation during AMI vs. ABIM charges over the last 20 years? We know that opening an artery during AMI saves lives whereas MOC has never been proven to save a life. In addition, the Choose Wisely guidelines from ABIM actually killed numerous Americans.
PROPOSED IAC (Intersocietal Accreditation Commission) CARDIAC ELECTROPHYSIOLOGY STANDARDS Another production fostered by C Cassel, et al.
Interested parties should visit the IAC website and advise against limiting their certification to ABIM/ ABOIM certificate holders. There may be lab staff who wish to comment upon their credentialing requirements as well. I submitted mine tonight.
Into the Streets (of DC) http://www.c-span.org/video/?320749-5/washington-journal-conspiracy-theories
Mr. Eichenwald. This is a great video. On another occasion can we get the ABIM questions on C-span somehow with some live callers from physicians, legislators and the public? Or another venue on the MSM.
Also could you and Dr. Fisher arrange for a series of questions on c-span with an interview with Senator Grassley, who could be briefed on the ABIM/ABMS related issues to get his take on the problems of ABMS excesses, quality assurance racket, and conflict of interests. I am concerned about the clandestine political activism, corruption, fraud, MOC and so on. Grassley is familiar with the NQF's Christine Cassel and most likely has a keen interest in the ABIM's finances as Senator from the state of domicile and principal on the finance committee. He is on another key Senate committees as well as you know. Perhaps open it up for a few questions from physicians and general voting public as well.
Elizabeth Warren is another legislator that has a sub-committee regarding health of our aging populations. Consider another interview with her for c-span and your you-tube channel.
Since Dr. Baron refuses to speak with you, could you get a few presidential candidates to weigh in with key questions and responses so the issue can be a part of our healthcare reform and debate.
I think it is time to take the case to the legislators and let voters know of the excesses under their noses. Ben Carson, Hillary Clinton, etc would be a very interesting mix of views so we can consider our choices. I would like to get Joe Biden's views on how things could be improved to help physicians serve the public better free of onerous red tape and bureaucrats that only seem to have self interests on the agenda.
I appreciate your interest and welcome a civil rights march out into the public. Arm and arm with democrat and republican and independents. This truly is a bipartisan issue that affects so many lives. I am a democrat who wishes for the pursuit of fairness for patient and physician in the medical arena. And time for health and happiness in life.
I am totally opposed to MOC and Choosing Wisely part of the ABIMF. The latter initiative has no place at the ABIM. I would like to have a chance to state the case and present it more to the public well in advance of our upcoming elections.
I would like to have a referendum in which physicians could vote on MOC and Choosing Wisely as well. It is time for phycians and the patient to have a voice again.
This is truly a socially responsible way to proceed and I believe corruption in the medical bureaucracy constitutes a crisis in broad terms, but also the violation of civil rights of US physicians and patients.
We must debate it openly on a larger scale in order to be heard.
There has never been an issue which has united the ACC membership like the opposition of MOC. The ACC membership has spoken loudly against MOC and the ABIM racket. Sadly, the ACC is replete with physicians in powerful positions who have an allegiance to the ABIM. The one physician/board of Trustees/former president at the ACC and serving on ABIM is Dr. John Harold.
This is clearly a conflict of interest. How can a person have a fiduciary responsibility to ACC and ABIM at the same time? It is obvious that we have traitors in our ranks. Until these turncoats are exposed and deposed, the ACC does not represent me.
Here here! Get the debate out into the public. Look at how they debate in the British Parliament. It's a bloody intellectual brawl. IN YOUR FACE AND VOCAL TO THE EXTREME. Get this debate going where it counts with the voter and your real advocate representatives. Pick the legislators with known integrity and who want to clean things up. Let's get it all on the 'tube' presses, and digital media.
Hey Kurt Eichenwald! Don't just go to the Trump rally. Bring Trump, Carson, Clinton, Sanders, and all the rest of the presidential wannabes into YOUR RALLY for US physicians against MOC and corruption. Create a Physician and Patient RALLY FOR JUSTICE in the medical system. Make it a fun, fair and clean fight to be a part of. You can do it!
Get Joseph Biden to break ranks and start distinguishing himself as someone who will fight against the special interests that dominate medicine and the rest of American society.
Get one of the Dwight Eisenhower family to weigh in on the medical industrial complex and how we got here today.
Fisher, get a publicist, media backing. You deserve to be on 60 minutes with Kurt or on your own. Do the Sunday rounds making the case with a few physicians, legislators and a non-profit tax specialist.
Kurt, write a song about it! Too much talk and not enough action. Get creative and go public for real. Get the democrats, republicans, independents to see the vital problems in medicine today. Problems that need to be addressed and fixed. Study it completely and objectively. Do it. Save the many who don't see the truth, not the few who already see and suffer.
Rothman D. Leadership by example: saying no to health industry board membership. BMJ. 2015 Sep 29;351:h5065. http://www.ncbi.nlm.nih.gov/pubmed/?term=26419423 Prohibition is the best way to safeguard scientific and clinical integrity. Although medicine came late to managing conflict of interest and promoting transparency, well after law, finance, and government, it now confronts many of the critical issues. Part of the impetus to change was externally driven, with state and federal legislation playing a key role in the United States. For example, US senator Charles Grassley led the initiative to compel drug and device companies to disclose all payments over $10 (£6.47; €8.95) to physicians and teaching hospitals, with the data accessible, name by name, on a public website.1 But part of the impetus also came from within medicine. Several medical school deans believed that cozy ties between industry and faculty violated professional standards.2 At the same time, medical researchers documented the extent and impact of these relations. In a linked paper (doi:10.1136/bmj.h4826) a study of this problem by Anderson and colleagues is an excellent case in point.3
The research into physician-industry ties helped alter attitudes and practices. Dozens of well designed articles refuted some physicians’ self serving claims that “you can’t buy me for a steak dinner,” or for stays in lavish resorts, or sizeable payments to promote a new drug or device. As the researchers found, recipients of company gifts were much more likely to prescribe and use the company’s products. Indeed, the company expended its funds to gain market share.4 5
Investigators also illuminated institutional conflicts of interest that had remained obscure. One study found that 60% of medical department chairs had financial relations with industry.6 A commentary on these and other findings noted that academic health centres and industry have different missions. Academic medical institutions seek to expand knowledge through research and to deliver effective patient care; industry looks to enlarge markets and profits to benefit shareholders. Boston’s not for profit health system, Partners, did limit the sums its administrators could receive from serving on a healthcare company board of directors, to $5000 a day. Even so, much more needs to be done to curb industry influence over academic institutions.7
The study by Anderson and colleagues strengthens the case for more stringent policies, by documenting the extent of these ties. In total, 279 academically affiliated directors, including chief executive officers, presidents, trustees, provosts, deans, and department chairs from 85 non-profit academic institutions received in aggregate $55m in compensation for serving on for profit health industry boards; on average they received annual payments of $193 000 and, in addition, stock options. The sums are unsettling—hardly a steak dinner—but effective institutional guidelines have yet to be agreed upon or widely implemented....
Non-profit Triple Dipping at the ABMS, et al. The Theft of Billions of Tax Dollars
Medical bureaucrats at the "not-for-profit" NGO's have stolen from physicians. They have stolen from their foundations; and they steal huge sums from the 'common pool' by placing a huge burden on the United States taxpayer.
It's time the profiteers at the ABIM and ABMS who skim the cream start paying their fair share of the tax burden.
Physicians and patients need a raise; and the fat cat bureaucrats need a haircut and a shave to help pay for it. And physicians and patients need more time.
There's plenty of fast and free cash out there going to waste. Organization in the quality assurance racket such as the ABMS and ABIM. They ABIM claims a motto of "of the profession, for the patient".
But their real motto is "wasting money and wasting lives."
We have seen clearly and sufficiently that the ABIM and its parasol apparatus the ABMS hide from the sun of truth preferring to languish in their tax-free dens. They see nothing wrong with inequity, but hypocritically make it their professional creed.
How strange how the fat cat bureaucrats live behind secure gates in "luxury land" casting lordly shadows on the common physicians, the common woman and man - who can barely pay for their travel and parking to and from the place where they give or receive their medical care.
And that point of care is getting further and further from the consumer and provider.
The ones who decide the fate of hundreds of millions - whether that consumer enjoys health and success, or poverty and morbidity - are living aloof in their plush penthouses in the sky.
Why is that Mr. and Ms. fat cat bureaucrat get to live under the tax umbrella of the non-profit NGO?
I think it is time to recognize these organizations have changed. They have changed so far from the voluntary humanitarian missions for which they were conceived that it's time we recognize and applaud all the progressive success and wealth at the ABMS by clapping our hands and uplifting their status as well with the IRS.
Let's get real. Let's get the tax codes changed to reflect reality. These fat cat bureaucrats cast their long shadows over us while dwelling in luxury on their "flying islands."
Let's tax the troublemaking quality assurance NGO's and tack on a luxury tax so that others can afford the precious luxury of being able to eat, see a doctor and live.
Now we are starting to understand where the rest of the missing money to pay for health care is going to come from.
ABIM, ABMS, the free ride is over. The Triple dipping ends here where the people draw a red line.
What does it mean, the professionalism and equity?
It means waking up to the common reality, which summons you and your organizations to pay their fair share of the tax burden to help us all out.
No more hoarding and consuming the better part of the American pie.
The taxpayer has won. Now the common citizen can go out and enjoy a hot dinner and they can save up for insulin.
The fat cat bureaucrat can still have his/her steak dinner, but the consumer will no longer pick up the tab.
24 comments:
For their 80th Anniversary Jubilee Year (assuming they're still in existence), maybe ABIM can reinstate the 1936 fees for all ABIM diplomates and the ABIM officers and staff can accept the same compensation as the ABIM principals did in 1936. Since "Professionalism" is a key characteristic that ABIM wishes to promote among practicing physicians, they could start by improving their own.
Regarding the MOC pass fail rate study: it is better to publish on a reputable site like "Dr Wes" than in a journal that may or may not have some conflicts of interest involving folks at the ABIM and ABMS.
That's my opinion after looking at the other 'outfits' who seem to keep the seal on talking transparently about corruption in 'medical bureaucracy land'.
It's a shame that the historical founders, i.e., the membership societies like the ACP and AMA, have not presently admitted seeing any irregular behavior or conflicts of interest at the ABIM; or even that they might exist.
Or that serious wrongdoings may have occurred within any of the offshoot "membership societies" of the ABMS.
I mean, for this discussion the ABIM in particular, but coi and compensation excesses should be on the lips of all executives and in all the medical journals as a full page ad by now.
Put your money to work on ads in papers and digital media sites; it will be money well spent. Or ask that they be placed for free as a public service announcement.
It is much more important to make coi and excessive financial inurement a poster child issue rather than just hand washing, as coi and excessive inurement represent the essence of having dirty hands.
Thank you for publishing the pass/fail results here, although I found them extremely disturbing.
We would like to read an expanded discussion of the MOC pass/fail rate study sometime. Perhaps you can add a hyperlink.
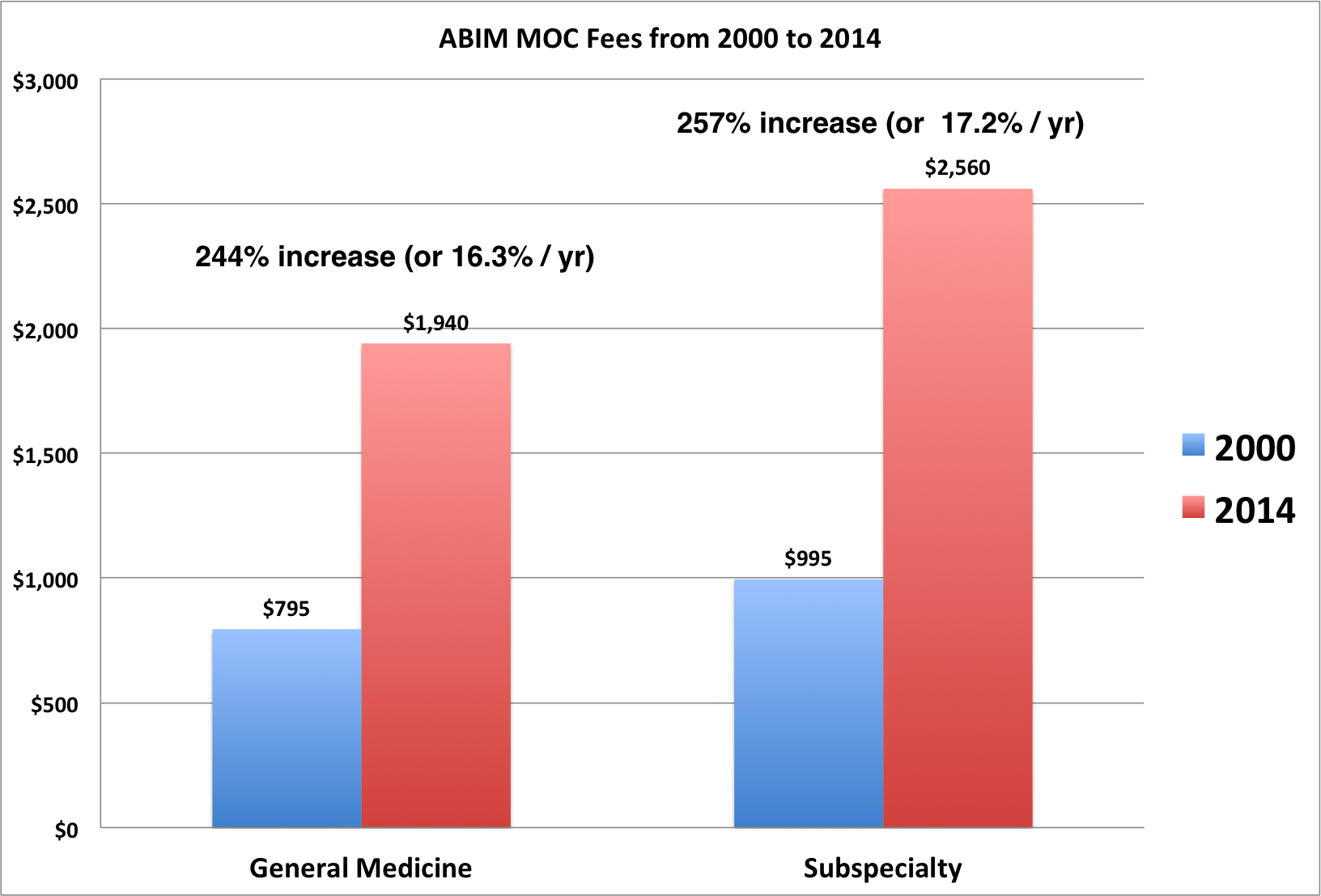
Concerning the ABIM wealth generation/fee graph:
The only folks who did as well or slightly better during 2000-2014 are behind bars now. They were Wall Street insiders who not-so-cleverly broke trading laws and Ponzi scheme scam artists.
One prosperous offshore hedge fund manager that is not behind bars is George Soros. He did very well with his Quantum Fund but we only have data through 2011 on him.
I'll explain why in a moment.
Soros has some strange unexplained link to the ABIM and its Foundation. That's why I mention him here. One (or more)of his foreign/domestic NGO's received grants from the ABIMF. Odd that an organization associated with Soros would need money from the newly formed ABIMF.
I challenge the ABIM to publicly explain this Soros affair.
George Soros' who created the Quantum Fund in 1973 did quite well for his undisclosed list of world elites, names like Roth****** and the Queen of E******. Managing this fund from 1973 to 2011, Soros returned roughly 20% to his highly elite client investors annually.
He did this by manipulating markets or acting only when he had insider knowledge.
Soros allegedly ravaged markets in Eastern Europe and often influenced events in vulnerable emerging markets to benefit his investments. Soros' Quantum Fund decided to shut down based on "new financial regulations requiring hedge funds to register with the Securities and Exchange Commission."
That meant transparency and disclosure, which would put severe limitations on cheating--if there was any.
The only ABIM person I track with even better results (because they benefitted in tandem with ABIM's increased fees during this time period was the ABIM's own CEO/President/lobbyist Christine Cassel.
The ABIM has a top-heavy executive overhead with most of the money being sucked out of the ABIM and ABIMF bank accounts by a handful of executives and about 50-60 other principal players.
All salaries were high six-figure salaries approaching a million on down the pyramid. Cassel left ABIM in 2014 with a surprisingly large amount of deferred compensation just in time for her 70th birthday, which is distribution age.
1.7 million 'smackers' if I recall.
Great timing and financial planning on the part of the Board Chairman/CEO/President, namely Cassel herself.
More examples of ABIM corruption at its finest?
With ABIM pass/fail rate in the dumpster y over y, cheating on tax filings, sky-rocketing legal fees, and at the same time increasing all executive compensation and giving a golden parachute to Cassel! Ugh.
Was the 1.7 deferred check and multi-million ABIM(F)payday totally excessive?
Or was it justified compensation?
Or was Cassel cheating on her hard-working physicians?
Was the Kaiser Permanente/Premier, Inc. high board seats collecting millions of $ at the same time a conflict of interest?
You make the call.
(50-year ABIM mission)
The Jubilee year 1986 should have been spent celebrating the dissolution of the organization.
It is stated in the 1936 bylaws that ABIM would be administratively dissolved in 1986 or sooner.
That should speak volumes about the original mission and the integrity of the founders.
The entire ABMS group of specialty boards should understand the original mission as well. It was a time-bound mission to establish a society of scientific medical subspecialists--physician investigators, if you will, serving the public and creating a certification process.
That is all. An initiation into a society of medical scientists and a certification for life.
The ABMS Today
ABMS is now comprised of strangers creating a strange land out of the medical landscape. Whatever is said or presented by the ABIM one must understand that the truth is really in the opposite of what they say.
Truth is a lie and a lie is their truth. Choosing Wisely is not what it says it is. It is the opposite. That is one of the crudest forms of lies imaginable.
It was never intended to be like this with executive positions, huge bureaucracy, and huge money expectations. It was truly voluntary in the beginning and should be today. Let's move back in that direction.
To be of the profession and for the patient. That implies lifelong learning and CME.
The ABMS just gets in the way of it. The are creating a big shadow from their towers of wealth. They are not towers of health. The profession is diseased by bad heads teaching nothing except about their greed and avarice. Raw power. Politics.
Yes, let executives work for the original compensation, which stated no personal inurement.
Zilch!
How's this for a new direction and a new way of thinking?
"I would be glad to serve just for the honor of serving;
but only for a year as was originally intended."
Or just dissolve the organization if too much time is spent denying and defending fresh lies heaped on the old till the end of time (in perpetuity).
Nobody has time for that kind of bull.
Just when you think they cant get any worse...
Professional Scamming.
THANK YOU for opening my eyes.
Trepidation Over the New Tax Plan
Presidential hopeful reading from his new tax plan.
-Page 4.
Item 216. "A nut is a nut and will cost no more than a nut!"
Item 217. "Cost Reductions in Government and the 'Quality Assurance' Medical Bureaucracy."
"I'll take questions now."
Q. I was just reading your new tax plan. If you are elected president of the United States what would you do about the ABIM and ABMS mess?
A. "Did I hear you correctly...the executives make how much at the American Board of...?"
Q. Yes sir, the CEO makes nearly $x,xxx,xxx for a 35-hour work week!
A. "Oh, yes, those ABIM folks with the luxury condo and chauffeur!
I know those political phonies well and they're bogus Choosing Wisely BS.
If I were president right now, I can guarantee you they'd be paying taxes--big taxes and fines for that kind of criminal lie...and they'd be paying back those docs from behind prison bars."
Q. Isn't that a harsh penalty for their type of fraud?
A. "You've never heard of the ABIM Foundation apparently! Don't get me started. Those stupid bozos will be crying for mercy in front of a Federal Judge of the Eastern District before the week is out...they've had their chance to...just slash all the executive positions! They're fired. And keep 'em out of my sight!
We'll find real good jobs for the rest of them and make our country great again...
Q. But do you have the authority to fire them, sir?
A. "I just did. It's that simple. Next question!
Yes, you with the Anti-MOC button..."
Q. Uh, you just answered all my questions, sir...
the whole world of CME scam starts on the basis of premise that the time spent by a physician on books / researching while treating a patient cannot be counted as CME . WHY ? who promoted this stupid idea. the best a physician can do to the world of medical education and patient care is read and research when it matters the most. it is time to bring that truth back into medicine. Count the CMEs for what matters the most. make the insurance companies pay for what time we spend on reading and patient care both. STOP. the scam in medical education is over. the whole world of AMA/ACP/ABMS is finished. it is time to expose that one line which destroyed the definition of Continuing medical education. it time to reimburse the physicians and all other professions like the lawyers are reimbursed.
This is ready for press in the New York Times, Wall Street Journal, Washington Post and on the TIMES SQUARE NASDAQ TICKER SCREEN
The War Has Ended. Let the parade begin.
"The scam in medical education is over!
The whole world of AMA, ACP, and ABMS is finished."
The Surgeon General has spoken.
In other news...in an ideal world...
The CMS has agreed to pay for physicians' time spent on the phone counseling patients and writing prescriptions. The CMS has decided that phone consults and prescription services (for patients who claim they cannot make it in to the doctor's office or UC) is a form of telemedicine and will reimburse providers at an appropriate rate.
The CMS also declared it will no longer be wasting physicians' precious time with preauthorization and denials. MD means making decisions and medicine should be left to the physician not insurers to decide. This bad practice complicates patient visits, creates confusion, delay, increases morbidity, death, and decreases quality of care overall.
Healthcare systems will run much better and the patient will be safer. There will be tremendous cost savings from ending this pre-emptive approach to managing fraud and overspending on medications. It simply does not work and puts patients health in jeopardy.
CMS recommends the same to all insurers. No more bureaucratic red tape which only creates time constraints and costs taxpayers additional money to administer the policy. The savings will bring much needed revenue for other much more important work in providing increased quality of coverage and care to seniors (and veterans) where it counts.
Formularies will be fully populated with all medications and made available. Studies have shown that highly trained physicians as we have today need to have the right tools when they need them to keep pace with advances in science and the increasing demands to administer medications and care when needed not after the patient condition has deteriorated, become frustrated to hell, or deceased.
(Insurance companies who create any such onerous additional burdens on providers creates a bottleneck in national health care. Offenders can be reported via the CMS.StateHealthCommission.gov or our hotline directly connected to your state insurance commissioners office with call-back and follow up calls provided as a public service to patient and physician.)
Recommendations made by the Surgeon General in his war against bureaucratic fraud and real waste in medicine caused by the corrupt quality assurance racket.
The SG is looking to recover a quarter of a trillion dollars by 2020 in eliminating these robber barons.
Questions:
Topic: Who created/signed off on ABIMF originally in 1989/1999? Where did the money come from and so on. How was it invested. Who formed the relationship with 1838 Investment Advisors.
Who actually transferred funds to the ABIMF? Who was ultimately responsible for decisions and who acted.
Who personally was involved in the momentum equity trades for over a decade using surplus physician fees? This money was actively traded to look like less equity trading took place than actually was the case. Yearly window dressing? Or something else?
Did 1838 Investment Advisors do this high risk/high gain investing as a courtesy for their non-profit clients? There was more than one specialist involved in non-profit portfolio management at 1838. Which one handled ABIM's account according to documents you have? Who sought out this arrangement with 1838?
As you may know 1838 Investment Advisors was founded in 1988. What part did 1838 Investments have in guiding the financial planning of the ABIM and ABIMF?
What percentage of money was transferred over time to ABIMF from profits/winnings involving their risky bets that paid out big for the period up until the circa 2001 collapse of the markets?
Especially bloody were many tech stocks that ABIMF held since at least 1991/1992, with new positions being acquired quarterly over a decade. According to more recent ABIM tax documents when 1838 was still a viable enterprise managing money for ABIM, you can clearly see the trading of tens of millions and you can see the heavy losses over three and four million dollars in consecutive years..
These losses were mitigated somewhat by selling longer term holdings with large gains. This buffered the accounts glaring losses, which were substantially more than the realized gains.
Then the trading stopped abruptly when 1838 Investment Advisors went belly up bleeding at the gills.
Did the ABIM's CFO or any other officer have any direct handling of the account and the manner or style in which it was managed?
Was there attempted intervention to preserve capital by the ABIM CFO at any time and halt the heavy trading of risky stocks? Mutual fund holdings were also managed by 1838 Inv Adv and were traditionally a trading vehicle as well for the firm.
Why did ABIM officers allow investing in risky stocks with negative PE's or in the low to high hundreds like JDSU, AOL, CSCO, etc. They lost big in the early 2000's on these trades. They were caught with their pants down and rode the equities down realizing losses of nearly a million dollars each on TYC and JDSU. Half a million on CSCO. They lost big on MSFT, TI, MU, INTC, AIG. The losses were staggering.
Covering over some of the losses on the tax forms are the substantial gains of shares acquired from the previous decade. Trades are a bit difficult to follow due to the trading style of 1838. The trades go on for page after page with the statements added to tax filings. Has anyone audited these forms from the 1990's and early 2000's for irregularities beside the trading?
Did 1838 utilize a stop-loss order/policy on the ABIM investments or did ABIM request to have any safety net when riding such wild stocks in emotionally exuberant markets?
As I mentioned, in the 1990's they purchased equities and made large gains,
what was the level of risk specified by the non-profit managers and what discussion took place with ABIM officers about this momentum trading? What did ABIM state as to their risk tolerance as is required by brokers/managers.
Does ABIM retain discussion of these financial decisions and other discussions related to it?
Do they keep records of their board meetings and private decision-making in general?
Questions:
Past president Kimball signed nothing related to the ABIMF registration document in 1999. Why? Only Christine Cassel the Chairman of the ABIMF signed it. It is strange to me that Kimball would not sign also. Documents as important as that and he did not sign draws up my hackles. Anybody have any personal stories to relate about past president Kimball?
Neither did the past ABIM president Benson in 1989 as I will show below.
The 1989 ABIMF registration document bears the name and address of the incorporator:
Henry F. Strozeski
C/O American Board of Internal Medicine
3624 Market Street, 2nd floor
Philadelphia, Pa. 19104
What are the implications of the above formation/registration document when a financial officer's name appears on the document in this manner and he is the only officer named. Strozeski is named as the incorporator with and in care of address at the ABIM's past offices on Market Street?
It strikes me as odd that the president would not also take credit or bear responsibility in any transparent company dealing with revenue and a good deal of profit.
Is the ABIM or ABIMF engaged in any document destruction routinely. What is kept from the past and how far back are documents preserved? What is required legally?
Seemingly in constant litigation, is ABIM required to retain and not destroy documents?
Hi Wes,
Your data analytics continue to amaze everyone I share the data with and it continues to cement the notion that this entire cottage industry is rife with obvious corruption, nauseating cronyism and worst of all professional cannabalism. It is obviously clear that the ABIM and their MOC process are woefully flawed and the leaders in charge of that organization have lost their stature. The simmering rage at the ABIM will lead to more formal forms of conflict resolution- official complaints with the Federal and State Governments, defunding of their operations etc. Keep up the great work shining a blinding white light into the dark corners of one of the most corrupt Medical institutions in recent history. And let this be a loud warning to those organizations that pretend to hold a monopoly on altruism and morale behavior but hypocritically behave just like the ABIM.
I often wonder if organizations like the ACC, HRS, ABMS, AHS would stand up to the moral stress test imposed on the ABIM. Do we think that the ACC and the HRS can hold its head up high when it comes to fiscal responsibility and financial modesty? Aren't the conflicts of interest at the ACC truly disturbing? Harlan Krumholz MD FACC is a leader at the ACC and at the ABIM 2020 working group. Does anyone else feel this is hypocrisy and morally wrong? Why such a lukewarm rejection of the ABIM by the ACC? Why do any of us support a dour organization like the ABIM? They have never supported clinicians and have lived off our sweat equity for too long.
I just received notice to pay my ACC membership fees that I have annually forked over for the last 17 years. I wonder where all this money goes and who gets to spend all of it. I wonder if I am getting my money's worth. I wonder if we looked into the ACC's books, would we find lavish spending such as condos, limo service, trips to the Four Seasons?
Such behavior cannot stand the scrutiny of the Internet. I hope I am wrong about the ACC and the HRS.
Wes, if there is a Lasker Award equivalent for a physician who has forever changed the way we look at professional administrator physicians, you would be immediately nominated. I hope we look back at folks like you, Charlie Cutler, Ron Benhasset and realize that courage, morality, and a ethical compass pointed at true North are underappreciated qualities.
Bravo to you and all of us who continue to insist on accountability and transparency in a massively disappointing era of American Medicine.
Charles H Koo MD FACC
If we could only exchange the benevolent paternalism of the ABIM for the AFL-CIO or Teamsters. Of course, we'd have to put up with the same corruption and all, but at least we'd get great benefits and leadership that actually looks out for us.
The Globalization of Medicine, ABMS International
(You are invited to visit their 'current' website.) http://www.abms-i.org/
Using their 'ethical compass' pointed at true North the ABMS is looking to increase revenue with a wholly-owned subsidiary called ABMS International. They are hoping to spin it off someday, but growth is spindly as the franchise meets a lot of global resistance so far.
It appears to be a trust and stress issue regarding anything that demands more time, money, and extra busywork spreading the 'quality assurance' word according to the..."what do you 'guys' call your medical assurance firm again?"
According to the kind organization spokesperson ABMS has only established their important work in Singapore so far. Mostly in education and initial certification after residency. "MOC may be coming next we hope."
But they related they have high hopes for other areas like the Middle East, as well. "Maybe Qatar; they have expressed an interest. We have projects elsewhere in the works, but perhaps Qatar will hopefully listen and be adopting soon."
According to fairly recent and 'reliable intelligence' there are a number of training camps and suitable apartments still available for MOC training programs in Qatar.
But note right now the AMBS is warning its international teams to watch their backs closely for 'friendly fire' as they engage the Middle East in the global war against medical chaos and unprofessional behavior. It is also written in the overseas training manuals that they are engaged in risky business in trying to improve the quality of medical care through cost reduction plans, such as "Choosing Wisely".
Europe for now has expressed doubt about American assurance programs and MOC US, because they have had enough of US bullying in international affairs to last a decade according to some "weak political crybabies" in the European Union (who wish remain anonymous).
"Just stay out of medicine; you already control everything else, they say."
Now let's fly to Singapore and stay at a luxury hotel and shake hands with Asia and spend a lot of greenbacks in the process. It's a reasonable cost for doing business.
Here's an update from the Singapore Journal of Medicine as of April 2015!
(excerpts: three paragraphs, with full article link below)
"The regulatory climate in Singapore currently does not require recertification through participation in an MOC programme or sitting for an examination – yet. However, similar to the requirements of most state medical boards, documentation of participation in accredited continuing medical education sessions is required for renewal of practice certificates (licensure) by the Singapore Medical Council (www.smc.gov.sg). Unlike in the United States (US), medical boards and credentialing committees of Singapore-based hospitals and clinical institutions currently do not require staff physicians to undergo MOC programmes or pass recertification examinations. However, the institution of residency training programmes, along the lines of the US programmes and certification examinations modelled on ABMS, may result in future Singapore-specific MOC programmes. Generally, academic medical institutions require staff physicians to be current with their specialty certifications in order to have practice privileges. Moreover, physician-educators are also usually required to be current with their certifications.
CONCLUSION
It is inevitable that continuous professional competence assessment, recertification, re-licensure or revalidation will come to Singapore. While we continue to debate the relative merits, I think it is more important to determine the methodology of doing so, without duplication of efforts. Singapore is a small country and the professional community is small in number, even smaller when considering specialties and subspecialties. It is clear that the professional societies and regulatory agencies will not be able to implement credible and non-controversial programmes. To increase efficiency and productivity, and reduce costs to the Singapore society, it would be better to outsource this process or work with larger professional bodies. Physicians should be able to choose a programme that best fits their scope of practice. However, it is likely that, besides the efforts put in by physicians themselves as a commitment to professionalism, the economic price will be borne by patients in the name of public assurance of medical competence and safety. If the burden becomes too onerous, one can always become a banker.
Endnote: The ABIM programme changed slightly from January 2014. It now reports certification status and 'meeting MOC requirements'. Diplomates have to continuously achieve MOC points to meet the requirements."
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4415094/
ABMS International, LLC, a wholly-owned subsidiary of the American Board of Medical Specialties, provides international services relating to physician certification. The American Board of Medical Specialties is a not-for-profit organization and has assisted its Member Boards in developing standards for physician certification in the United States since 1933.
©2015 ABMS International, LLC. All rights reserved.
ABMS International and the ABMS shield design are registered trademarks in China, the EU, Israel, and Singapore and property of ABMS International, LLC.
Dr Fisher-
I am not a physician, but I have read much of your blog. It is a rare compendium of medical news with references to research that you and others have engaged in.
The worst bits have been the news about how the ABMS has gained so much power in such a short period of time--a few decades only--and how they continue to dictate such onerous policies. I really can't understand why this has not been stopped immediately by authorities.
I can tell from reading your blog that you are a family man with strong values and that you love your country and profession. You seem fair and honest to me.
I sometimes wondered why you spent so much time on the ABIM. I'm not sure they are worth it.
Then I happened upon a blog where you introduced your daughter to an average workday. It was splendid to meet such a bright caring person coming to witness your world as a physician. That one blog and many other blogs here helped me also to see and have a taste of all the changes in medicine.
I understood something clearly at that point. I'll try to explain. I was touched by your daughter's comments about all the typing you do (I remember the days of dictation and paper charts in offices and hospitals). Then the emotion struck home to me that we must stand up for what is right, good, and true for our children. Strive for it in medicine and in life. Not let them inherit a world that is less than what they deserve (or we deserve today)
You might not understand what I mean, because it was a dual perception of how things are and how we would like them to be. I wish the people at the ABIM would just talk to all of you openly. But I understand the complicated nature of the organization and so many things I can't even imagine that are involved.
Anyone with children can understand why you persist in trying to bring to light the embedded culture at the ABIM, ABMS, and the other organizations I never knew existed before. No one even knows about the ABIM, for goodness sake.
I don't want to say it is like a shadow government exactly, but it certainly appears to have been doing things beneath the radar without any oversight. I would say that medicine has a shadow bureaucracy that I don't agree with at all.
And all the executive compensation is ridiculous when most of us struggle on a small fraction. I won't address the corruption, because it was not my point in writing, but I would hope that it is investigated and cleaned up.
Please, I hope others in medicine will stand up and not let this inequity of money, power and politics to continue.
I saw a video of Dr Cutler(?), someone mentioned. He has very valid points and people should see it. No vetting for conflicts of interest stood out, cost of buying condo and maintaining versus renting an apartment with pool. So many good points. I'll bet you my daughter could run it better with complete transparency, and completely fairly. She is bright and looking for work.
I am a property manager, by the way, with a masters in business. A neighbor who is a doctor showed me your site.
Webb-
Thanks for your nice note. I think the reason I persist in this endeavor is because, like you, I care about medicine being a profession of integrity and honesty, not lies and half-truths. We are talking about a system of re-certification that uses fear to exact large sums of money from physicians, has the ability to destroy careers, has (in my view) stolen from vulnerable practicing physicians to fund a shadow organization that purports to impart "social justice" imperatives and re-distributes grants to groups that promise to "teach physicians" about cost savings and some skewed definition of "professionalism" that ignores honesty, transparency and integrity. I'm not sure I've ever seen such corruption by a group of (supposedly) peer physicians. It's deplorable and inexcusible, IMO.
Granted, not all physicians in these organizations are bad people, but our specialty board system has become bloated and self-serving - full of unaccountable burned-out academic and practicing physicians that no longer see patients but are more than happy to criticize the colleagues with whom they have no idea of their scope of practice and coerce them into paying handsomely into their scheme of quasi-quality in the name of "public good."
I train residents and fellows and like to think I lead by example. I'll be damned if the profession of medicine is going to go down some financial/busy-work rabbit hole in the name of a funding this broken, bloated, and self-serving ABMS/ACGME/JCAHO/FSMB bureaucracy. We are better than this and these bureaucrats need to wake up to the fact that their methods are now understood and bright shining lights will continue to illuminate their activities.
Like you, I have no idea why the IRS, state Attorney Generals, or OIG of the Department of Health and Human Services has allowed such transgressions to occur for so long and only hope that a formal investigation of these organizations will be forthcoming by the authorities. I eagerly await the anti-trust suit ruling by the AAPS against the ABMS as well, for this might be the stake in the heart of our Specialty Board monopoly that is a deplorable example of what physicians should become.
Here's to physicians and patients waking up together! Thanks again for taking the time to noctice and comment.
Wes:
Thank you for keeping the pressure on the ABIM. However, we are fighting a hydra. For every head you try to battle, there are many others.
1. Witness the new ICD-10 incarnation. This has been a horrible disrupter of clinic flow this week. It adds NOTHING to patient care and only serves the bureaucrats with their databases who can sell their information to CMS.
2. No matter how you feel about planned parenthood, seeing a political operative (bureaucrat de jour) from Nancy Pelosi's office paid $600k is upsetting. As an interventional cardiologist who is paid less, I would feel better about her salary if she had to get out of bed in the middle of the night to perform an abortion and only had 20 minutes to be in the office. Don't forget the press ganey scores to boot. Does anyone remember Obama criticizing cardiologists (vascular) who cut the legs off diabetics for a buck. Here is the CEO who is paid handsomely from government funds for ending lives--pure hypocrisy.
3. Can you graph the inflation adjusted reimbursement for cardiac cath or stent implantation during AMI vs. ABIM charges over the last 20 years? We know that opening an artery during AMI saves lives whereas MOC has never been proven to save a life. In addition, the Choose Wisely guidelines from ABIM actually killed numerous Americans.
Speaking about another head of the Hydra!
PROPOSED IAC (Intersocietal Accreditation Commission) CARDIAC ELECTROPHYSIOLOGY STANDARDS
Another production fostered by C Cassel, et al.
Interested parties should visit the IAC website and advise against limiting their certification to ABIM/ ABOIM certificate holders. There may be lab staff who wish to comment upon their credentialing requirements as well. I submitted mine tonight.
http://www.intersocietal.org/ep/main/newsroom.htm
Please Read, Review, and Publicly Comment Upon:
http://www.intersocietal.org/ep/standards/IACCardiacEPStandardsSection1A.pdf
1.1.1.1A
1.1.3.1Aii
1.2.1.2Aii
1.2.3.1Aii
Wes... I think it's official ...
You are now the ABIMs WORST NIGHTMARE !!!
(Be careful... They're not used to losing)
Into the Streets (of DC)
http://www.c-span.org/video/?320749-5/washington-journal-conspiracy-theories
Mr. Eichenwald. This is a great video. On another occasion can we get the ABIM questions on C-span somehow with some live callers from physicians, legislators and the public? Or another venue on the MSM.
Also could you and Dr. Fisher arrange for a series of questions on c-span with an interview with Senator Grassley, who could be briefed on the ABIM/ABMS related issues to get his take on the problems of ABMS excesses, quality assurance racket, and conflict of interests. I am concerned about the clandestine political activism, corruption, fraud, MOC and so on. Grassley is familiar with the NQF's Christine Cassel and most likely has a keen interest in the ABIM's finances as Senator from the state of domicile and principal on the finance committee. He is on another key Senate committees as well as you know. Perhaps open it up for a few questions from physicians and general voting public as well.
Elizabeth Warren is another legislator that has a sub-committee regarding health of our aging populations. Consider another interview with her for c-span and your you-tube channel.
Since Dr. Baron refuses to speak with you, could you get a few presidential candidates to weigh in with key questions and responses so the issue can be a part of our healthcare reform and debate.
I think it is time to take the case to the legislators and let voters know of the excesses under their noses. Ben Carson, Hillary Clinton, etc would be a very interesting mix of views so we can consider our choices. I would like to get Joe Biden's views on how things could be improved to help physicians serve the public better free of onerous red tape and bureaucrats that only seem to have self interests on the agenda.
I appreciate your interest and welcome a civil rights march out into the public. Arm and arm with democrat and republican and independents. This truly is a bipartisan issue that affects so many lives. I am a democrat who wishes for the pursuit of fairness for patient and physician in the medical arena. And time for health and happiness in life.
I am totally opposed to MOC and Choosing Wisely part of the ABIMF. The latter initiative has no place at the ABIM. I would like to have a chance to state the case and present it more to the public well in advance of our upcoming elections.
I would like to have a referendum in which physicians could vote on MOC and Choosing Wisely as well. It is time for phycians and the patient to have a voice again.
This is truly a socially responsible way to proceed and I believe corruption in the medical bureaucracy constitutes a crisis in broad terms, but also the violation of civil rights of US physicians and patients.
We must debate it openly on a larger scale in order to be heard.
Dear Dr. Charles Koo:
There has never been an issue which has united the ACC membership like the opposition of MOC. The ACC membership has spoken loudly against MOC and the ABIM racket. Sadly, the ACC is replete with physicians in powerful positions who have an allegiance to the ABIM. The one physician/board of Trustees/former president at the ACC and serving on ABIM is Dr. John Harold.
This is clearly a conflict of interest. How can a person have a fiduciary responsibility to ACC and ABIM at the same time? It is obvious that we have traitors in our ranks. Until these turncoats are exposed and deposed, the ACC does not represent me.
Here here! Get the debate out into the public. Look at how they debate in the British Parliament. It's a bloody intellectual brawl. IN YOUR FACE AND VOCAL TO THE EXTREME. Get this debate going where it counts with the voter and your real advocate representatives. Pick the legislators with known integrity and who want to clean things up. Let's get it all on the 'tube' presses, and digital media.
Hey Kurt Eichenwald! Don't just go to the Trump rally. Bring Trump, Carson, Clinton, Sanders, and all the rest of the presidential wannabes into YOUR RALLY for US physicians against MOC and corruption. Create a Physician and Patient RALLY FOR JUSTICE in the medical system. Make it a fun, fair and clean fight to be a part of. You can do it!
Get Joseph Biden to break ranks and start distinguishing himself as someone who will fight against the special interests that dominate medicine and the rest of American society.
Get one of the Dwight Eisenhower family to weigh in on the medical industrial complex and how we got here today.
Fisher, get a publicist, media backing. You deserve to be on 60 minutes with Kurt or on your own. Do the Sunday rounds making the case with a few physicians, legislators and a non-profit tax specialist.
Kurt, write a song about it! Too much talk and not enough action. Get creative and go public for real. Get the democrats, republicans, independents to see the vital problems in medicine today. Problems that need to be addressed and fixed. Study it completely and objectively. Do it. Save the many who don't see the truth, not the few who already see and suffer.
Pick up your bed and walk.
Rothman D. Leadership by example: saying no to health industry board
membership. BMJ. 2015 Sep 29;351:h5065. http://www.ncbi.nlm.nih.gov/pubmed/?term=26419423
Prohibition is the best way to safeguard scientific and clinical integrity.
Although medicine came late to managing conflict of interest and promoting transparency, well after law, finance, and government, it now confronts many of the critical issues. Part of the impetus to change was externally driven, with state and federal legislation playing a key role in the United States. For example, US senator Charles Grassley led the initiative to compel drug and device companies to disclose all payments over $10 (£6.47; €8.95) to physicians and teaching hospitals, with the data accessible, name by name, on a public website.1 But part of the impetus also came from within medicine. Several medical school deans believed that cozy ties between industry and faculty violated professional standards.2 At the same time, medical researchers documented the extent and impact of these relations. In a linked paper (doi:10.1136/bmj.h4826) a study of this problem by Anderson and colleagues is an excellent case in point.3
The research into physician-industry ties helped alter attitudes and practices. Dozens of well designed articles refuted some physicians’ self serving claims that “you can’t buy me for a steak dinner,” or for stays in lavish resorts, or sizeable payments to promote a new drug or device. As the researchers found, recipients of company gifts were much more likely to prescribe and use the company’s products. Indeed, the company expended its funds to gain market share.4 5
Investigators also illuminated institutional conflicts of interest that had remained obscure. One study found that 60% of medical department chairs had financial relations with industry.6 A commentary on these and other findings noted that academic health centres and industry have different missions. Academic medical institutions seek to expand knowledge through research and to deliver effective patient care; industry looks to enlarge markets and profits to benefit shareholders. Boston’s not for profit health system, Partners, did limit the sums its administrators could receive from serving on a healthcare company board of directors, to $5000 a day. Even so, much more needs to be done to curb industry influence over academic institutions.7
The study by Anderson and colleagues strengthens the case for more stringent policies, by documenting the extent of these ties. In total, 279 academically affiliated directors, including chief executive officers, presidents, trustees, provosts, deans, and department chairs from 85 non-profit academic institutions received in aggregate $55m in compensation for serving on for profit health industry boards; on average they received annual payments of $193 000 and, in addition, stock options. The sums are unsettling—hardly a steak dinner—but effective institutional guidelines have yet to be agreed upon or widely implemented....
Non-profit Triple Dipping at the ABMS, et al. The Theft of Billions of Tax Dollars
Medical bureaucrats at the "not-for-profit" NGO's have stolen from physicians. They have stolen from their foundations; and they steal huge sums from the 'common pool' by placing a huge burden on the United States taxpayer.
It's time the profiteers at the ABIM and ABMS who skim the cream start paying their fair share of the tax burden.
Physicians and patients need a raise; and the fat cat bureaucrats need a haircut and a shave to help pay for it. And physicians and patients need more time.
There's plenty of fast and free cash out there going to waste. Organization in the quality assurance racket such as the ABMS and ABIM. They ABIM claims a motto of "of the profession, for the patient".
But their real motto is "wasting money and wasting lives."
We have seen clearly and sufficiently that the ABIM and its parasol apparatus the ABMS hide from the sun of truth preferring to languish in their tax-free dens. They see nothing wrong with inequity, but hypocritically make it their professional creed.
How strange how the fat cat bureaucrats live behind secure gates in "luxury land" casting lordly shadows on the common physicians, the common woman and man - who can barely pay for their travel and parking to and from the place where they give or receive their medical care.
And that point of care is getting further and further from the consumer and provider.
The ones who decide the fate of hundreds of millions - whether that consumer enjoys health and success, or poverty and morbidity - are living aloof in their plush penthouses in the sky.
Why is that Mr. and Ms. fat cat bureaucrat get to live under the tax umbrella of the non-profit NGO?
I think it is time to recognize these organizations have changed. They have changed so far from the voluntary humanitarian missions for which they were conceived that it's time we recognize and applaud all the progressive success and wealth at the ABMS by clapping our hands and uplifting their status as well with the IRS.
Let's get real. Let's get the tax codes changed to reflect reality. These fat cat bureaucrats cast their long shadows over us while dwelling in luxury on their "flying islands."
Let's tax the troublemaking quality assurance NGO's and tack on a luxury tax so that others can afford the precious luxury of being able to eat, see a doctor and live.
Now we are starting to understand where the rest of the missing money to pay for health care is going to come from.
ABIM, ABMS, the free ride is over. The Triple dipping ends here where the people draw a red line.
What does it mean, the professionalism and equity?
It means waking up to the common reality, which summons you and your organizations to pay their fair share of the tax burden to help us all out.
No more hoarding and consuming the better part of the American pie.
The taxpayer has won. Now the common citizen can go out and enjoy a hot dinner and they can save up for insulin.
The fat cat bureaucrat can still have his/her steak dinner, but the consumer will no longer pick up the tab.
Post a Comment