Yet, after a review of public and tax records, it appears to me this is exactly what has happened.
Background
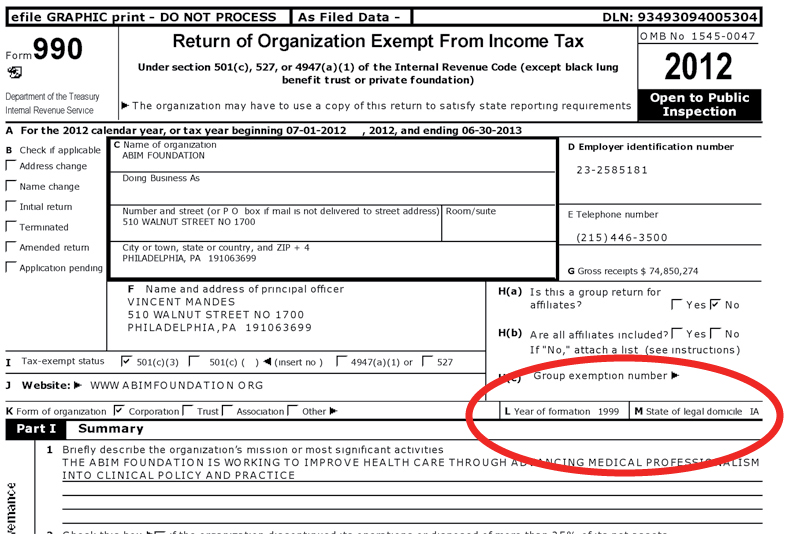
In 1999 for reasons that are unclear, the American Board of Internal Medicine (ABIM), itself a tax-exempt 501 (c) (3) independent non-profit physician evaluation organization domiciled in Iowa, created (Editor's note 10/20/2015: referenced web page has since been edited by the ABIM Foundation; the original referenced web page can be viewed here) a second non-profit tax-exempt 501 (c) (3) organization, the ABIM Foundation (Foundation), to first define and later promote the term "medical professionalism." Both the ABIM and the Foundation share a common address in Pennsylvania and common officers:
{kind=link}
"The American Board of Internal Medicine (ABIM) is related to the ABIM Foundation (Foundation) in that The Foundation is the sole voting member of the ABIM. As such, the two organizations share a common president, a common CFO, and a common senior vice president whose base salaries are allocated between ABIM and The Foundation based on the time spent by each executive."To define "medical professionalism," the new Foundation enlisted other members of the non-profit world including the ABIM, the paid "directors" of the Foundation, the Robert Wood Johnson Foundation, the American College of Physicians-American Society of Internal Medicine and the European Federation of Internal Medicine. The group was chaired by Troy Brennan, MD, JD a paid "Director" of the Foundation who was also President and CEO of Brigham and Women's Physician Organization at the time. (He later became the Chief Medical Officer of Aetna in 2006, and now serves as the Executive Vice President and Chief Medical Officer of CVS Caremark). In 2002 this group published a white paper entitled "Medical Professionalism in the New Millenium: A Physician Charter" without peer review in the Annals of Internal Medicine (here) and The Lancet (here). At least the Annals editor, Harold C. Sox, MD mustered the courage to express concerns about the manuscript in his introductory remarks to his readers:
"The introduction contains the following premise: Changes in the health care delivery systems in countries throughout the industrialized world threaten the values of professionalism. The document conveys this message with chilling brevity. The authors apparently feel no need to defend this premise, perhaps because they believe that it is a universally held truth. The authors go further, stating that the conditions of medical practice are tempting physicians to abandon their commitment to the primacy of patient welfare. These are very strong words. Whether they are strictly true for the profession as a whole is almost beside the point. Each physician must decide if the circumstances of practice are threatening his or her adherence to the values that the medical profession has held dear for many millennia."The paper centered on three fundamental principles that the authors claimed defined "medical professionalism:" (1) the primacy of patient welfare, (2) patient autonomy, and a new concept, (3) the principle of social justice - that is, "the medical profession must promote justice in the health care system, including the fair distribution of health care resources." With this definition, physicians could no longer just be unwavering patient advocates concerned with the "primacy of their patient's welfare," they had also had to serve the financial needs of The System of medicine lest they be labeled "medically unprofessional."
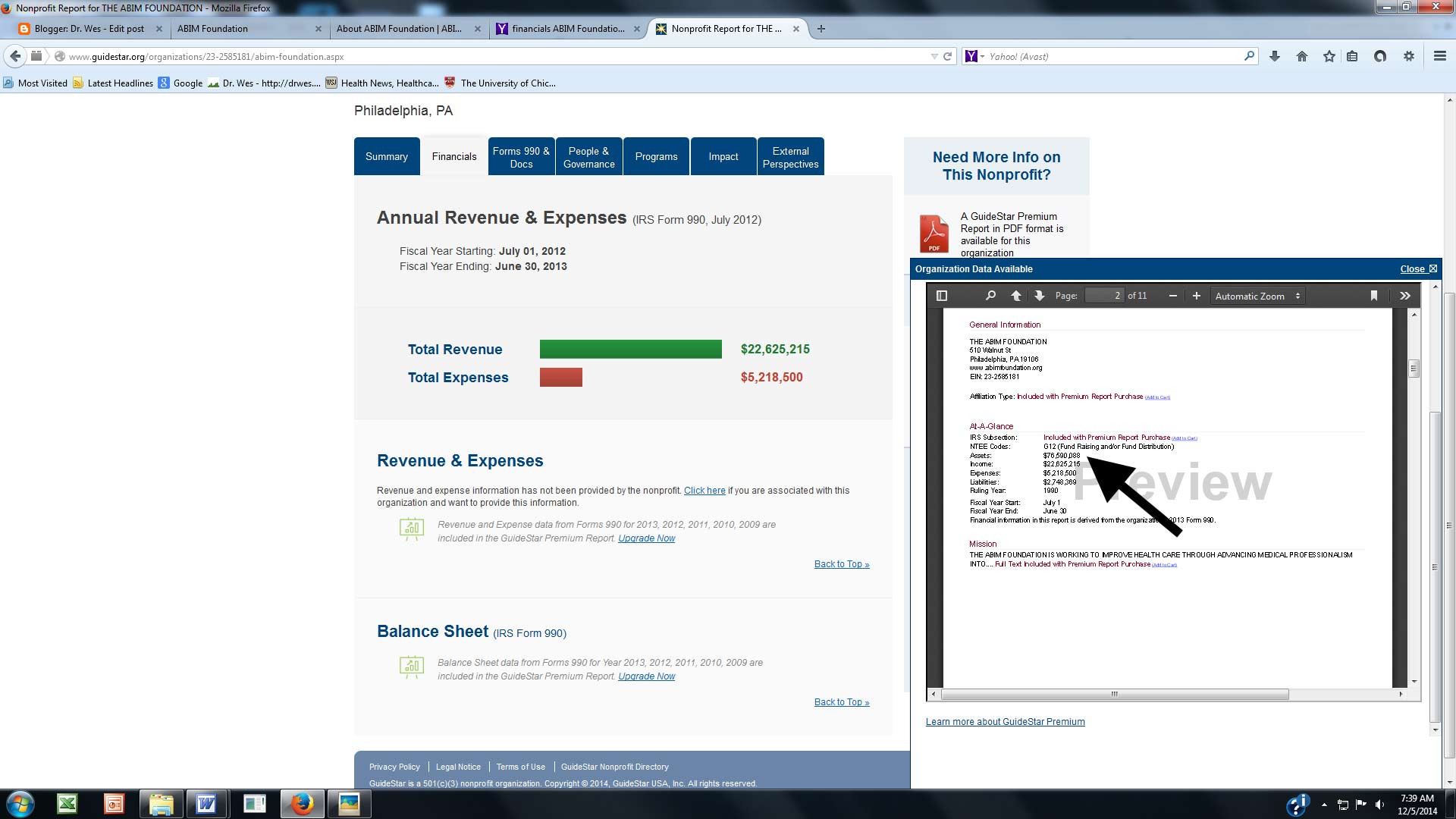
Ten years later after accumulating some $76 million in assets, the Foundation began their hard-to-disagree-with "Choosing Wisely®" campaign to encourage physicians and providers to question the value of medical testing in an effort to eliminate unnecessary tests and procedures. The campaign has grown to include 70 societies and some non-physician organizations, including Consumer Reports, AARP, SEIU, and Univision among others. As part of the campaign, monetary grants from the Robert Wood Johnson Foundation are awarded to institutions willing to "educate practicing physicians about the recommendations from specialty societies, and building physician communication skills to facilitate conversations with their patients about the care they need."
{kind=link}
The Money Trail
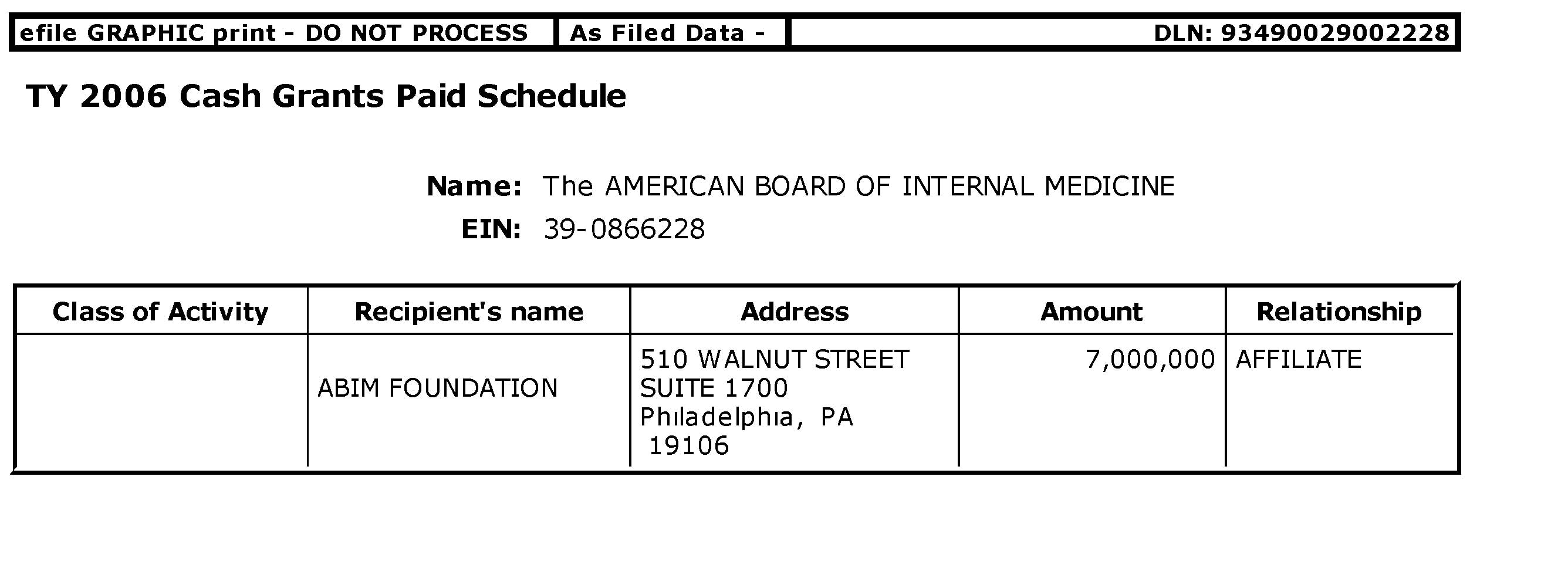
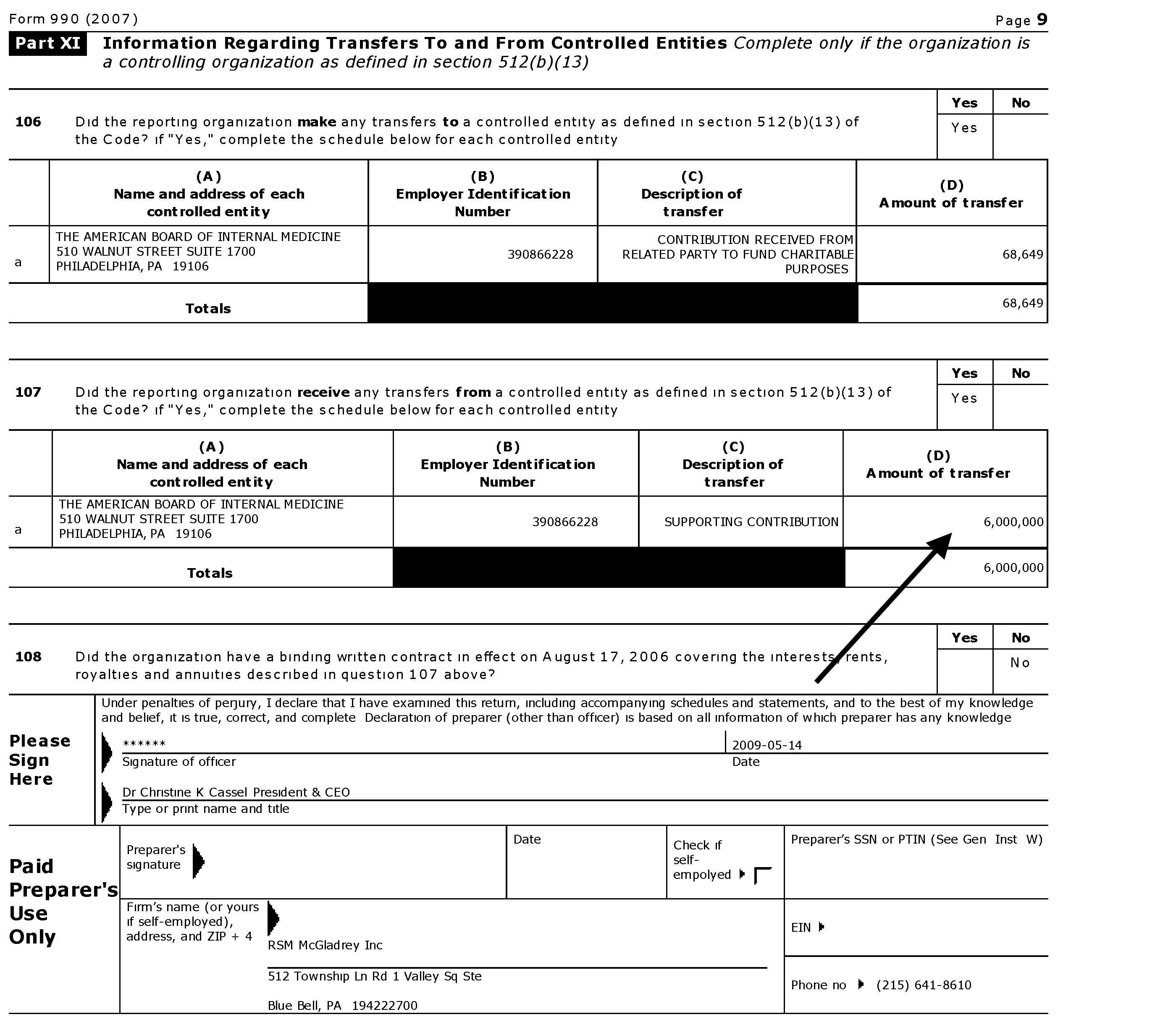
So how did the ABIM Foundation accumulate all that money? Reviewing public tax records of the ABIM and its Foundation reveals a significant portion of the Foundation's revenues came directly from the ABIM. Recall that ABIM receives 97% of its annual revenues from physician certification (62%) and re-certification fees (35%), with only 14% of these fees going toward physician examination development. In 2007 and 2008 alone, cash grants from the ABIM to its Foundation of $7 million and $6 million respectively were issued. The public records disclosed that $17,360,000 from the ABIM were made to its Foundation in the 7 years ending 6/30/2008. As a three-time participant in the ABIM certification process (candidate #127308), I can attest that to the best of my knowledge physicians were never made aware of this use of the testing fees they paid the ABIM.
{kind=link}
{kind=link}
The Luxury Condominium
 |
| Street View, "The Ayer Buidling," 210 W. Washington Square |
{kind=link}
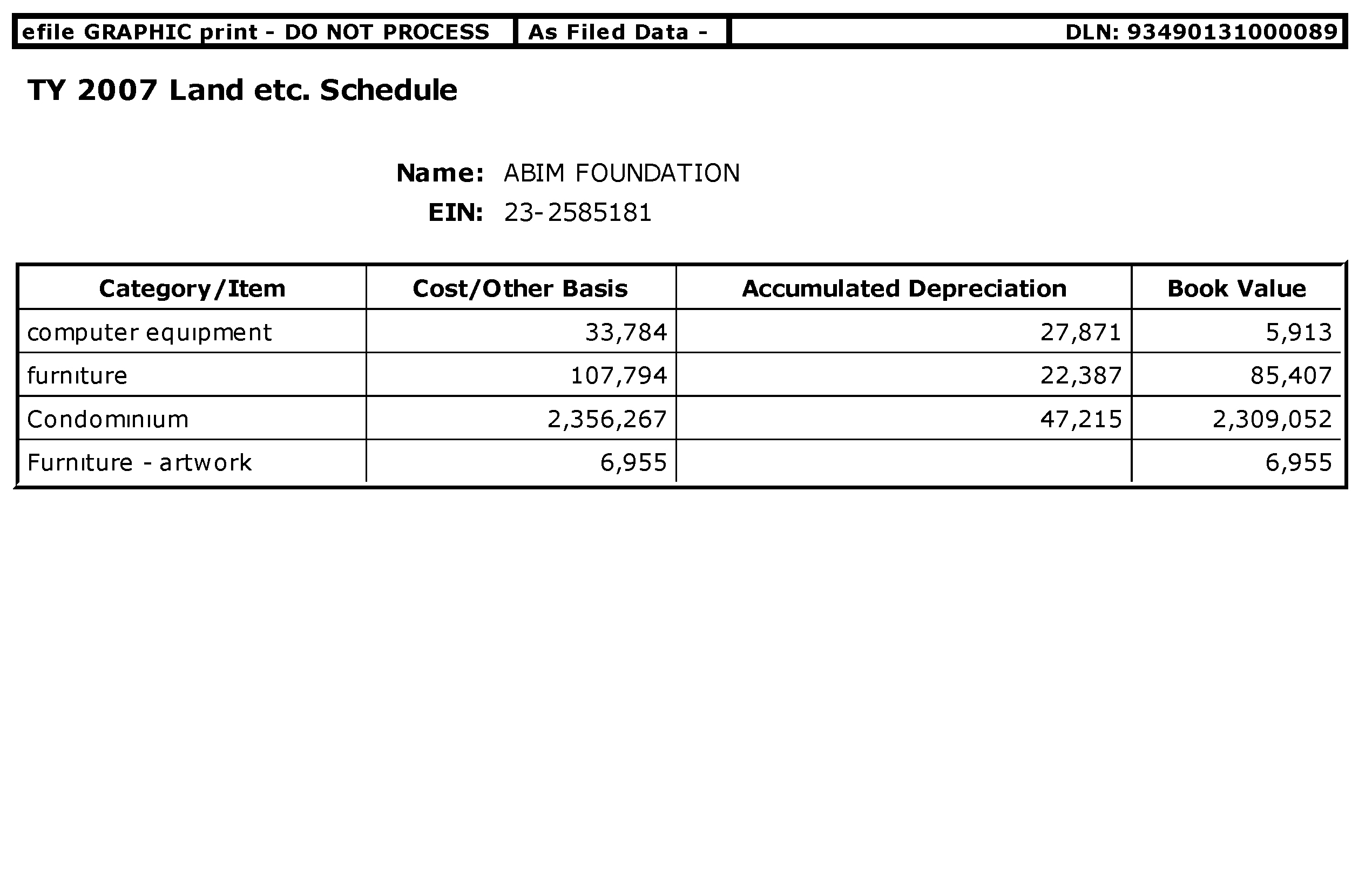
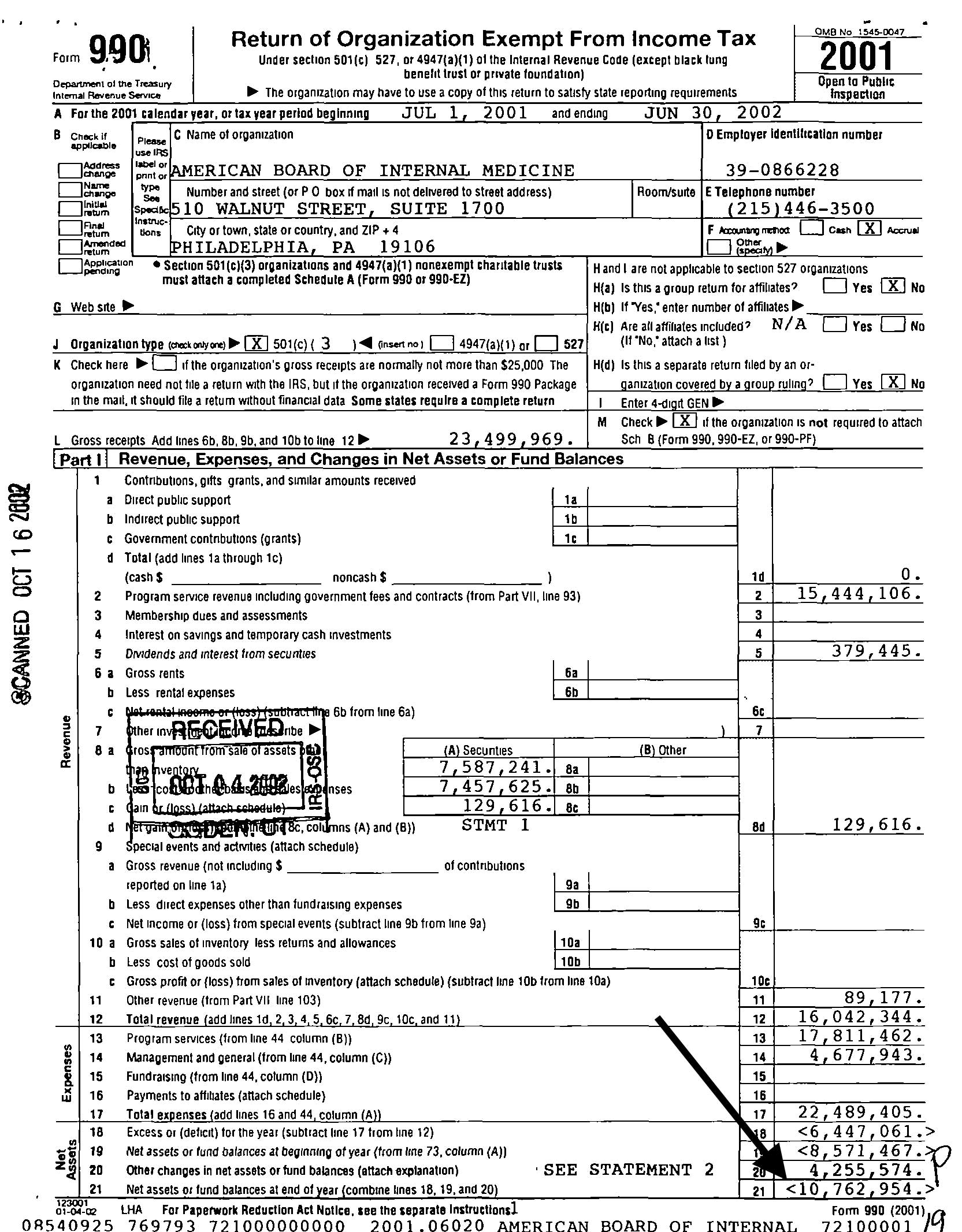
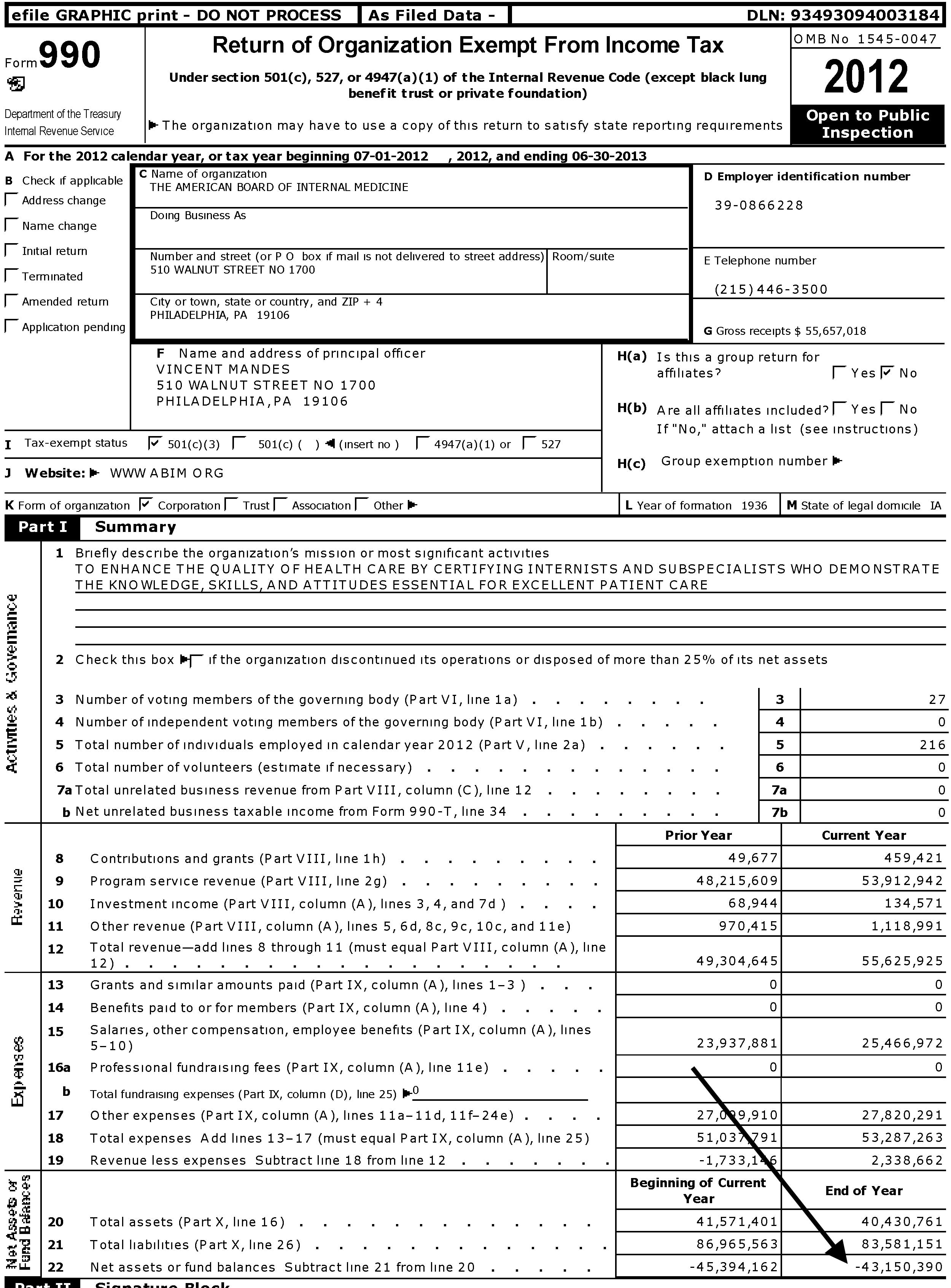
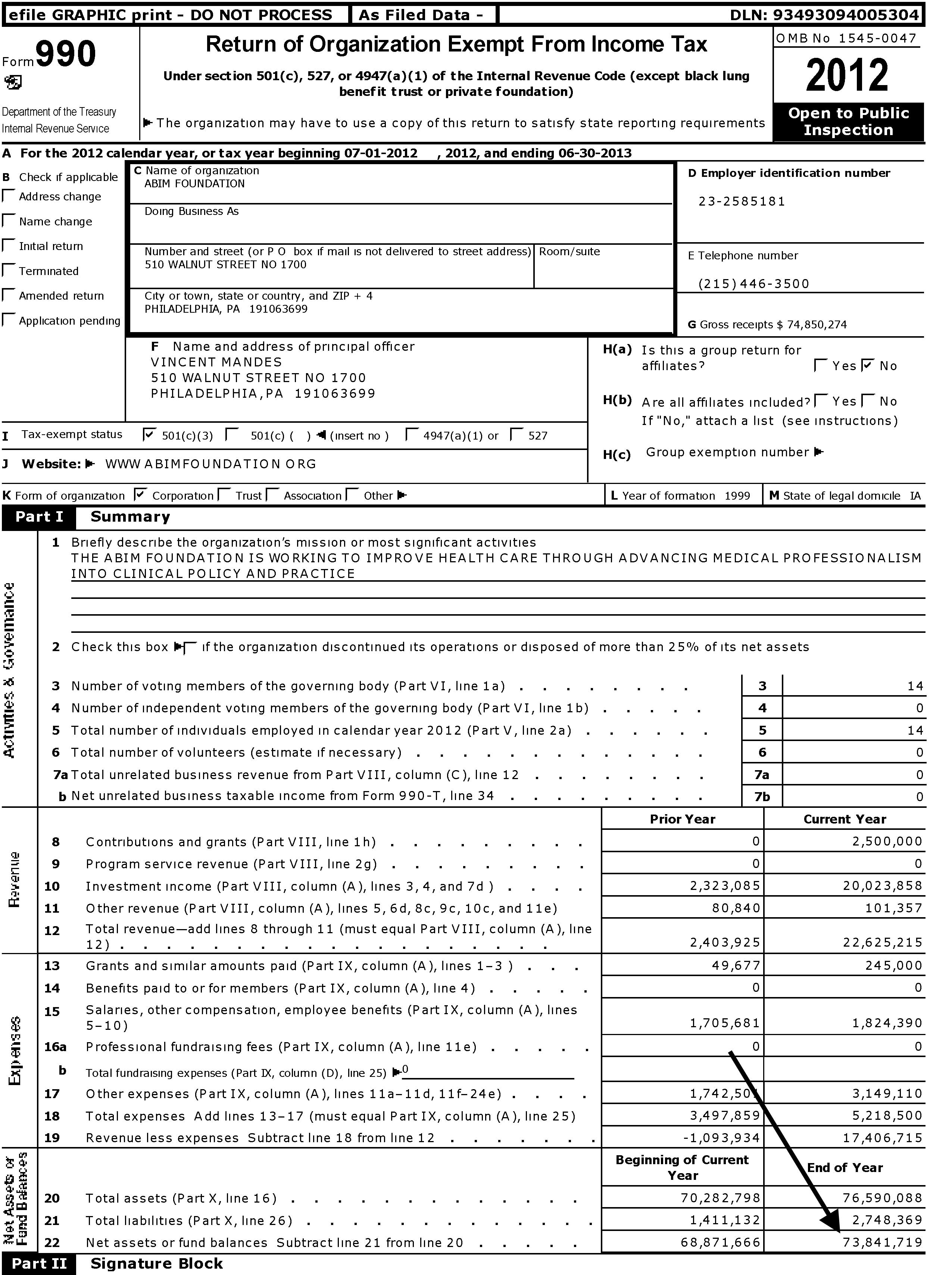
Since then, the Foundation has reported "condominium expenses" totaling $850,340 from December 2007 through June 30, 2013 (FY 2008: $42,522, FY 2009: $164,460, FY 2010: 161,957, FY 2011: $165,982, FY 2012: $161,980, FY 2013: $153,439 (most of these reported as "program service expenses")). In my view, these expenses were accrued while the ABIM appears to have been on an inherently unsustainable financial course from 2001 to 2012 with its net asset or fund balances on 6/30/2002 beginning with a negative balance of $10,762,954 and growing to a negative balance of $43,150,390 ending 6/30/2013. Meanwhile, over the same period its shadow organization, the ABIM Foundation, fund balance was $73,841,719 on 6/30/2013.
{kind=link}
{kind=link}
{kind=link}
It should be noted that in the year of the condominium purchase the President and CEO of the ABIM, Christine Cassel, MD, earned $484,883 from the ABIM and $161,627 from the Foundation. Dr. Cassel continues to serve as President and CEO of the National Quality Forum despite a history of other seemingly conflicted financial dealings. Other executives of ABIM that year included F. Daniel Duffy, MD who served as Executive Vice President of the ABIM earning $379,915 from the ABIM, and Cary Sennett, MD, PhD who served as Senior Vice President earning $185,122 from the ABIM and $185,122 from the Foundation and now serves as a Vice President of Anthem, Inc., formerly Wellpoint. That year Dr. Richard Baron, the current President and CEO of the ABIM and Foundation, served as the secretary/treasurer of the ABIM Board earning $59,729 until 7/1/2008 when he became an unpaid Director of the Board. By comparison, according to one reliable source, the median general internal medicine physician salary in the U.S. was $205,441 in 2009.
More Questions
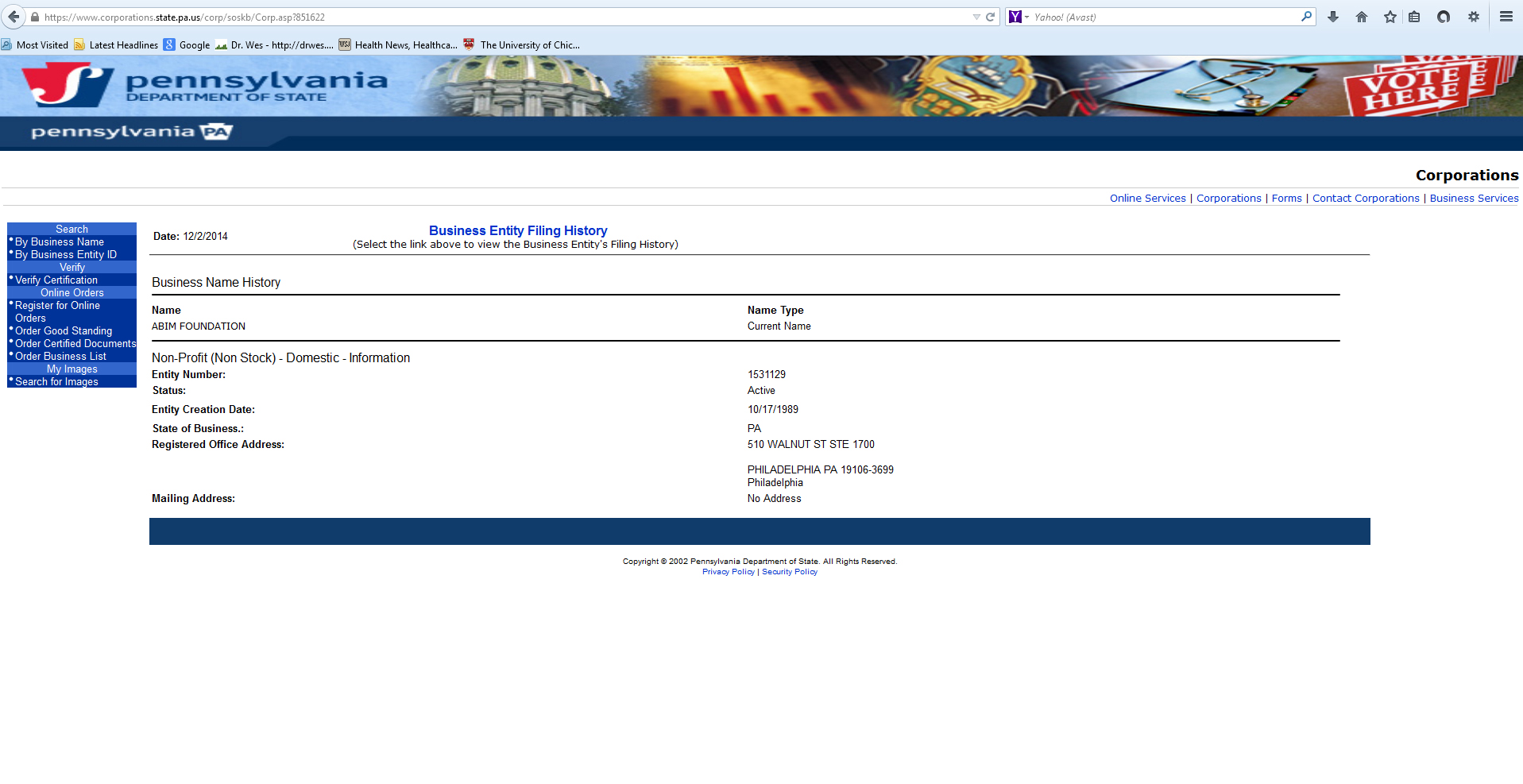
Reviewing the public record on when and where the ABIM Foundation was actually created discloses another discrepancy. We observe that the Foundation has recorded on their tax returns as being founded in 1999 with its "legal domicile" in Iowa, like the ABIM. However, a search for the organization in Iowa comes up empty, while a search in Pennsylvania Department of State (screen shot here) shows the Foundation was actually created in Pennsylvania in 1989. Which is correct?
{kind=link}
{kind=link}
We should note that non-profits are not required to file financial statements with the state of Iowa, while Pennsylvania requires them. This raises uncomfortable questions. Is the Foundation's Iowa domicile sheltering the sources and uses of its funds? Why does a non-profit promoting "medical professionalism" need to accumulate this much revenue? Is this how the Foundation demonstrates their "medical professionalism" to the public? To whom is the ABIM and Foundation "accountable?" Anyone?
My Call to the ABIM
On 4 December 2014 I contacted the ABIM and requested an explanation regarding the condominium, the ongoing condominium expenses, and the discrepancy of the ABIM Foundation domicile and founding date. Richard Baron, MD, the current President and CEO of the ABIM returned my call and explained the following:
- Dr. Baron stated that the condominium was purchased as a "investment property" and part of the investment portfolio of the Foundation. He mentioned that real estate holdings were not uncommon with other similar non-profits. The condominium was used for several purposes, including housing ABIM personnel who resided out of state and returned to Philadelphia for meetings, by contractors (for instance, to house an IT team from India), and for off-site retreats and meetings with the Communications Group of the ABIM, for instance. He noted that when ABIM members use the Foundation's condominium, the Foundation is paid $150/night from the ABIM (compared to the "usual" Philadelphia hotel rate of about $190/night) and there was cash flow to the Foundation from the ABIM for the use of their facility.
- After revelations of the luxury condominium were disclosed at a 2 Dec 2014 Pennsylvania Medical Society town hall meeting, Dr. Baron mentioned in passing that the ABIM was putting the condominium up for sale. I asked Dr. Baron the name of the listing agent and the price. He stated he could not comment because "the paperwork was not in order" and the those details had not been finalized because they were advised that the real estate market would be better in the Spring.
- When asked about the high ongoing condominium expenses and the discrepancy about the ABIM Foundation's creation date and domicile, Dr. Baron could not immediately respond but sent this follow-up e-mail 4 Dec 2014 at 2:39PM (CST):
"Hi Dr. Fischer (sic)-
Attached please find the breakdown of the condo expenses. As I explained the depreciation $$ are a required reporting artifact for the condo as a business investment. The other costs are covered by the condo usage fees.
Regarding the 1989/1999 question - In 1999 ABIM Foundation became a separate operating foundation.
Thanks,
Rich
Richard J. Baron, MD
MACP
President and Chief Executive Officer
American Board of Internal Medicine" - In closing, Dr. Baron expressed his willingness to be open to further questions.
- Today I learned that the condominium is now listed with the following description:
"Extremely Spacious Three Bedroom, 3.5 Bath Home at the Ayer Condominium. Tremendous Entertaining Space. 11’7’’ ceiling heights. Bulthaup b-3 kitchen system, Miele and Subzero Appliances. Huge windows with northwest views. High floor offering stupendous sunsets. Gorgeous stone bathrooms. Abundant closet space. One garage parking space included. Concierge, doormen, valets, gym, chauffeur driven BMW 7-Series." (More details here.)
Larger Implications
Sadly, the medical profession has become a house divided. On one side are many non-clinical physicians who have become far removed from patient care and are firmly embedded in the non-profit, academic, and public policy circles making handsome salaries while seeing little problem with coercing their colleagues to pay fees to support their various economic, policy, or personal agendas. In the words of my colleague Jordan Grumet, MD: "they talk about 'accountability' as if they are the ones in the ICU having the family meetings. They pray at the altar of 'quality' yet fail to define the specifics of such a term. They resent 'over treatment' but never have suffered the consequences of not doing enough."
On the other side are the physicians buried in the work-a-day world of patient care, busy doing the best they can for their patients in our increasingly complicated health care system, working as "excellent sheep" as they do their difficult job and try not to rock the boat. While such a dichotomy is not unique to medicine (look to education, the public service sector, and politics, for instance), is ignoring this new reality useful to our profession? Might the unintended consequences of these unaccountable non-profit organizations and revolving-door employment practices with government and business interests be causing unimaginable harm to the integrity and credibility of our profession while simultaneously wasting valuable resources?
It is a shame that most physicians, particularly younger doctors saddled with exorbitant training debt and concerns of job acquisition and job security, are not in a position to protest the actions of the ABIM and its sycophants, particularly since their ability to practice medicine is increasingly tied to these ABIM board certification and their new perpetual maintenance of certification payments. But this is the point, isn't it? Regulatory capture. As these younger doctors gain experience and awaken to the realities of their new health care arena that is increasingly dominated by unaccountable organizations led by non-clinical members of our own profession, we risk creating cynicism in our ranks and physicians who must be more concerned with passing a test than providing direct patient care. Even worse, we risk promoting ourselves, career or cause over the complicated needs of our patients as the divide grows ever deeper. As a result, the brittle credibility and hard-earned trust with our patients is squandered beyond repair. In my opinion, this is what we risk when we have corruption within.
Is this what our profession and the public wants?
I can only hope that practicing US physicians and the public will demand a full accounting of the ABIM and their Foundation's entire financial dealings and non-transparent co-mingling of funds. I hope that Congress decides to investigate the ABIM's role in including their MOC program as a physician quality reporting measure in the Affordable Care Act (see pages 247 and 844-845) to determine its legitimacy in light of these findings. Furthermore, an investigation into possible violations of federal policy on the protection of human subjects (in this case practicing physicians involved in direct patient care) regarding the American Board of Medical Specialties' requirement for practice and patient survey collection for Part IV of their trademarked Maintenance of Certification® program that the ABIM helps conduct should occur, especially in light of lack of informed consent afforded to physicians regarding how the fees and data they collect are used.
It is time we hold the non-clinical members of our own profession that lead these organizations accountable to all physicians and the public at large. Until this occurs, physician-members of every ABIM subspecialty organization that profits from educational content provided to the ABIM should divest themselves and work to create their own, more credible, simplified and transparent life-long learning pathways. The American Association of Clinical Endocrinologists has already set a good example. While I understand that refusing to buck the coercion created by the multimillion dollar ABIM and its Foundation will be difficult, our credibility as stewards of our patients' best interests and the preservation of the integrity of our profession demands nothing less.
-Wes
Acknowledgement
I am indebted to Charles P. Kroll, CPA for his invaluable assistance collecting tax records of the ABIM and ABIM Foundation before 2007 and assisting in the understanding of the nuances of not-for-profit accounting methods. Mr. Kroll provided forensic accounting analysis to the Minnesota attorney general's office during the Medica-Allina scandal and testified at the Minnesota Senate hearing on the matter.
34 comments:
Read a sad statistic recently that 20-25% of med school grads never practice medicine. Instead, they go into law, pharma, "consulting," or "public policy." Maybe there should be a requirement that you actually practice the profession for at least 5 years before you get to regulate it.
Wanna hear from uber commenter W.O.R.M.
If you're out there, speak up!!
Jay
JAMA hosted a webcast today on MOC. No opposition voices were invited. No response to tough questions including my question on the $2.3 million condo. See the twitter stream #MOCDebate for the whole rundown.
Disgusting. I was naive enough to think this was a debate. This was no debate. This was a 90 min ABIM infomercial.
Jay
RICO (Racketeer Influenced and Corrupt Organizations Act) provides for civil cause of action.
http://en.wikipedia.org/wiki/Racketeer_Influenced_and_Corrupt_Organizations_Act
How long will it be before we establish a legal fund and go after these racketeering, corrupt, and influence peddling ABIM directors???
Dr. Wes,
Physicians,especially internists,owe you a debt of gratitude for this masterful,detailed,documented expose of what is going on at the ABIM and ABIMF .It deserves to be widely read.I have been chipping away at various aspects of what you outline in this white paper.I plan to quote liberally and often from this paper.Good work.
What I do not understand is, why ABIM has so much power, and we, the people who pays the fees, have no leverage whatsoever? They traval around, showing up in every "debate", acting like they are listening. However, nothing has changed. Who has this much "executive power"? Why do our opinion mean nothing?
Time to impeach the board members. Anyone knows how? I am for a nationwide strike.
If other doctors are like me, the biggest issue keeping them locked up with the ABIM may be the importance of Board Certification in the credentialing process.
To "strike" against the ABIM with the possibility of losing your hospital privileges and insurance panel membership would take a brave doctor, indeed.
Maybe it's time to refocus our political efforts to creating an "unwinding" process from the ABIM. We'd need to create an alternative certification process (likely through our individual specialty boards) and then petition to remove ABIM from our credentialing documents.
Until we can assure MDs that dumping MOC will not cause them to lose their jobs, this movement won't go very far.
I've started to talk to our hospital leadership about this. Others should do the same. We need to continue to petition our specialty societies with our concerns, and support the creation of alternative pathways.
This is a big job, but may be achievable. In my 18 years of practice, I've never seen doctors this united about anything.
Jay
@EJSMD
I think that decentralization of whatever entity deems one to be 'board certified' is the best way to keep the process honest. The ONLY reason anybody gives the ABIM money is because they've cornered the market on what it means to be an internist.
If state societies could establish an alternative state IM certification board, the ABIM would finally start to make some meaningful effort at overhauling the MOC process. And it really doesn't involve re-inventing the wheel. Here are my proposed criteria for being State Board Certified in IM:
1) Candidate has passed INITIAL certification exam provided by the ABIM *ONE* time in their life (really-- you don't need to reinvent the wheel. Use what's already there). Does not have to be currently 'board certified' by the ABIM's misguided criteria. You can look up any internist on the ABIM website and it will tell you when they passed their boards even if they are not meeting MOC criteria and the ABIM yanked their endorsement.
2) Maintains medical license in good standing by current state license requirements (requisite CME hours in whatever categories-- child abuse, patient safety etc-- state has already established)
3) Whatever else the state boards (in conjunction with the state society and local chapters with their ELECTED leaders) deems useful in continuing education, be it required additional CME, smaller less intrusive and tedious quality improvement projects than those terrible PIMs/Patient Voice projects the ABIM vomited out onto their website, special symposia or educational modules
If #3 is done poorly, at least we can let our local chapter know and oust them if they don't listen (which we can't do to the ABIM). States can look at what other state IM boards are doing and refine the good ideas and get rid of the bad ones faster than the glacial pace the ABIM takes since they're the only ones allowed to do anything in the certification game. If a state really needs to attract physicians, they can make themselves more attractive by offering better options in continuing improvement and physician education. It will properly align incentives and make the state certification boards give actual effort to help their physicians improve instead of the current situation where the ABIM gets paid MORE by every failure on their certification exam (which IMHO explains them tightening the screws on the exam and inducing a worsening failure rate). I see a conflict of interest there and it won't ever change unless the system gets undermined.
BRAVO. A wonderful transparent assessment of the inner workings of an ABIM that will no longer be trusted by the nation's physicians. The ABIM has unfortunately transformed itself into an opaque quasi-regulatory organization whose recent sloppy decision to subject physicians to odious “recertification” burdens, at a time when the profession is already under massive amounts of redundant oversight, has provoked a violent reaction from physicians across the nation. There is no reason why we, as cardiologists, need to be subjugated by the ABIM. I would suggest that the ACC, HRS, TCT organizations, who have all had a strong track record supporting clinical activity and clinical physicians, lead the effort to offer our own recertification process totally independent of the ABIM. Why do ACC members need ABIM certification when the Steering Committees for the Cardiology Exams are all ACC members anyway? The ACC has the resources, the background and the talent to construct our own Board Certification process that is more economical, more relevant, less onerous, more common sense filled, and most importantly more respectful of our sub speciality. I find it oxymoronic that the ABIM leadership relies on overpaid, aloof non-clinicians to adjudicate what makes a competent cardiologist, interventional cardiologist, cardiac electrophysiologist and transplant cardiologist. I would like to appeal to my colleagues, peers and friends to lobby the ACC to construct an independent Board Certification process that is not reliant on the ABIM.
- See more at: http://blog.acc.org/post/acc-response-abims-moc-requirements/#sthash.FuqqI5fB.dpuf
rotten to the core. abim=mafia
These organizations, above all, sell “tests,” not education, as a “corporate product.” Historically, they have facilitated the establishment of significant modern national standards for physicians in education, residency training, and state licensure acquisition over the past century. These stringent and uniform training regulations have now been established as basic requirements for initial state licensure. However, these corporations continue imposing more testing bureaucracies on physicians as a means to somehow improve quality of care further, in what is already recognized as one of the best medical systems in the world. The next goal is to impose additional, lifelong, expensive mandatory hurdles to jump in order to maintain professional licensure.
These increased bureaucratic requirements clearly expand the power and revenue of these organizations, but there is no evidence of better protection of the public. Rather, the transgres- sions of practitioners who have lost their licenses typically have had little to do with inadequate knowledge; rather, they are ethical or drug-related issues, often involving individuals likely capable of passing testing hurdles. While physicians have commonly striven to obtain board certification as an index of superior competency, the FSMB is now striving to impose this as a recurrent basic requirement for licensure, at significant cost to physicians and the general population as everyone ultimately pays the bills to finance this unproven method. As such, board certification is being degraded from a mark of excellence to become a common requirement to practice medicine.
Wes:
Can you pass this info on to the FTC? I believe a federal investigation is warranted.
The ABIM says the >$2M luxury condo was purchased to house "out-of-town personnel".
What this means it was used by the CEO at the time, Chris Cassel, who lived in Arizona, so she would have an appropriate place for a >$1M executive to stay when she came to the ABIM offices in Philly. Ben
Well said. Also, it's still not too late to sign the petition to recall the ABIM's MOC program that feeds their bottom line. PLEASE SIGN TODAY!
http://www.petitionbuzz.com/petitions/recallmoc
Send this beautiful work directly to authors of essays about MOC that were recently published in New York Times. It will add nicely to a growing voice of dissent against all this regulation.
You (and others) have done a "60 Minutes" expose on the ABIM scam. Now, if 60 Minutes would do their own, change will become possible...
The answer is for physicians to band together and form their own certification entity - abandon the ABIM. It cannot survive without us.
Remarkable job. Thank you for your efforts here.
Great Effort Indeed. Thank You for devoting your valuable time to the cause.
Wow. As far as I can tell based on a review of their policies both the ACP and the AMA primarily represent East Coast liberals. Moderate and conservative physicians in America have no national voice. Where do I donate to this cause??
Very nice investigation - Loved it
All the more disappointing that now, as I am sure you have herad, KevinMD now opines that we should forget this nonsense about opposing MOC ...
Thank you for this amazing research, these boards are completely corrupt and there is no question in my mind, there is racketeering going on. I'm inspired to do my own investigation of the AB Derm, which in the past month suddenly slammed the brakes and changed all the requirements, unilaterally and midstream, to "accommodate" busy physicians. They decreased the amount of modules and peer/patient surveys immediately. I think they were feeling some heat from somewhere and they reversed course. I will try my own attempt at researching this. THANK YOU.
Terrific encapsulation of the "haves and have-nots" within our profession at the close of your piece. Sorry I just happened to see it now. This dichotomy you speak of is writ large in academic medicine. The clinical "leadership" (division chiefs, department chairs, program and center directors) not to mention the hospital and practice plan executive staff, and the army of deans, vice-deans, etc at the medical schools -- all of them are practically exempt from the RVU-based compensation systems imposed on rank and file faculty. Why do we allow this to continue? The isolated departures of individual faculty for greener pastures (I myself am guilty of this) will never address the unsustainable inequities that are now hardwired into most modern academic medical enterprise. What we need are a few individuals with real vision and freedom and real power at their respective institutions to start moving things back to a more sensible model.
Dr. Wes
Thank You, Thank you... I will not re- certify and I am not going to enroll in their ridiculous money making scheme. I have been denied jobs and hospital privileges for not re- certifying but I don't care. Medicine has become hard enough to practice and now we have a bunch of low life mafia self serving ABIM and ABMS beurocrats
who are feeding the public and legislatures unsubstantiated garbage about certification and competency and their MOC process.
Do not let them get away with it. We must push for total elimination of the MOC and re-certification process .
In fact I will join an alternative board. If all the Internists and specialities banded together this will happen.
You think ABIM is bad, look at the salaries of ABP executives. Obscene. Pediatricians are among the lowest paid physicians, but have the highest salaries for our ABP executives. 1.3 million per year.
Anony 3 Mar 2014 @ 4:38 PM CST:
ABP isn't the only one. Here's the full list for your review I compiled some time ago:
http://www.medtees.com/content/ABMSBoardMemberSalary.pdf
Just to note that DrWes was here first but Newsweek and others are piling on now
Besides exposing the scandal of ABIM, who else can help us, the physicians battle this unscrupulous bureaucracy?
Thank you for this post. Many of us suspected this was creating a financial machine and not about maintaining certification....All of us want to work next to competent people. No defense , none for someone making 3x a doctor's income to head this non profit. Thanks again.
Thank you for your hard work. As a 30-year practicing physician, it's about time someone exposed the ABIM for what they are: nothing but a protection racket. After you've devoted your career to keeping up to date with CME, the ABIM comes along asking for money when they should be protecting our interests, not fostering their own greed. Can't wait for a "60 Minutes" piece on this. Fear is still keeping many MD's on the sidelines.
ABIM: Entrenched milieu of corporate and governmental instruments corrupted in degree only by level of involvement, compensation, duration, and proximity.
Original Purpose: Governmental/corporate influence/control of physicians to create specific time-limited goals and aims in healthcare management.
Present Purpose: Corporate/governmental influence/control of physicians to create specific open-ended goals and aims in healthcare management.
Original Certification. Aim: lifetime sheepskin. Pride of keeping one's skin.
Present Certification. Ongoing aim: Loss of pride of ownership of one's life and work. Lifetime sheep without skin.
Future ongoing plans: Corporate/government controlled healthcare system with employed model only. Interim slowdowns will kill individual and group practice: accessibility, EHR, bureaucratic clerical distractions, reimbursement levels/denial/delays. Eventual demise of all independent metropolitan, urban, and rural healthcare. Slowly chopping the remaining backbone of all private enterprise merging into a national monoculture with a few trusted brands and trademarks.
Orwellian newspeak will replace the reality of suffering physicians/providers/patients with a progression false data and statistics proving the opposite is true.
The fleecing of all physicians of the right to share in corporate decisions but expected to follow an ethical practice of "choosing wisely" with patients utilizing a shared decision model (SDM). Corporate medicine will be in complete control over medical decisions, cost, payroll, benefits.
Excluding medical and human conscience and its interaction for the 'perfect static order' in society. MSM controls all thought and opinions. Black and white reality of domestic and global affairs.
Unless a truly human dialogue is established between us where we stop lying and hiding reality from one another we are doomed. What is wrong with the ABIM is what is wrong with the current state of society. Impartial reason and conscience guides too infrequently to make any difference. This must change. If an ethical society of doctors at the ABIM cannot lead us out of our present morass it is only because they try to autocratically decide our present course. Most physicians cannot follow such 'people of false images' and a 'bagful of pretentious notions'. We simply do not wish to be corrupted by the ABIM and assist them in creating a world in their mythological medical image. It is a horrendous thought that no child could accept. Such cheating of us out of the right to a democratic process where we all discuss and decide the right course for medicine and the maintenance of measure is reprehensible. Greed and politics has no place here. That is what the ABIM culture must change. ABIM heal thyself first and put the measure where it is most needed!
External measure/coercion cannot replace internal "knowledge and empowerment" which elicits us to follow pathways where we choose to exercise reason and conscience in our relationship to life.
Physician deserve to be ruled by ABIM. We are the most spineless community, watching only our interest. Its such a shame that NBPAS is only acceptable in 14 hospitals across the entire country. What have we done for the people who stood up for us, and if ABIM is listening to us – Its not because of their generosity but fear of competition. One man has the balls to do it, yet end result is far from happening.If we don’t get it approved in 80% of the hospitals in a year- Its going to be pointless creating NBPAS. I tried my best in my hospital – Guess what, No one wants to stand up. How many years we have felt in pain of memorizing ” last minute stuff” before the boards. Absolutely useless stuff in real life, driven by stress of running a practice and fear of a lawsuit, yet predictable questions and answers. What is the board useful in practical life when ” This will be asked only on the boards” is repeated 16 times on ACP lectures. So let me ask all of you writing all the comments – Is NBPAS acceptable in your hospital ? We can all talk but actions will make a difference. Please get your hospital to approve NBPAS, and make others aware. And may I ask you a question” how do you justify writing this article when you knew people scamming million in deferred payments”. Can you explain why lobbies were involved. Why ” we were wrong” came out only after NBPAS was formed. Why is there question in the on chemotherapy for IM boards – Try giving a chemo in your office and you will be in the front news. Show me a single interest who doesn’t call am ID consult when RPR is positive – or patient has a cardiac CP. And don’t even try to manage this stuff, once in court – “are you a cardiologist” “NO” is enough to get you your license and all you made working 30 years.
Power in Numbers
Patience
look at the sky
listen to the wind
ask yourself "who am I"
put your ear to the ground
shhh! Listen
the movement is rumbling in the earth
feel it all around
the falseness of their lies
falls from the sky
crumbling
like an old picture
the mind is a comet
your heart a falcon
the wind is your ally
all the earth has heard your cries
look around
feel the immensity of the world
octaves of vibrating light
from one plucked chord
comes all
life's diversity
if I told you it all started
with only three colors
painted on a pallet of darkness
would you believe me
your mind is a comet
the heart a red falcon
the solemn sun is your friend
'cause the earth has heard your cries
a friend in the beginning
is a friend in the end
?8-Rumi-8?
Entered Medical School at age 19, in 1972.
Completed Medical education in India 1982 MD in Internal medicine.
Completed MRCP in England 1993.
Nephrology Fellowship 1996 in England
Repeated Internal medicine Residency 1996 to 1998
Passed American Board of Internal medicine 1999.
Passed American Board of Internal Medicine again in 2009( ABIM DOES NOT ACKNOWLEDGE THIS AT ALL ON MY PROFILE).
Passed Royal College of physicians(UK) Nephrology Board exam 2013
ABIM started to enforce another board certification and MOC requirement in 2015, well ahead of 10 years.
Tried to re-certify in 2020 through, ABIM endorsed, 2 Year Knowledge Check-in Pathway. Applied for this pathway, Fees Paid, Examination date fixed for 11/11/2020
"MOC" requirement completed, still ABIM Unilaterally cancelled the examination and forcing me to write a "10 year certification examination"
ABIM Gives me a Choice of 2 year KCI pathways and then ABIM cancelles it on its whims causing a huge practice disruption at the time of COVID pandemic.
The question I have is:
1. Do I Not have "Life-time learning experience in Medicine" from age 19 to age 66 ?
2. If ABIM does not like a 2 year Knowledge check-in pathway, Why they allowed me to schedule an examination for Nev 2020 and then unilaterally cancelled it?
3. Do I have any recourse other than just submitting to ABIM mandate to write yet another 10 year certification exam or die "Not Certified". After all, I am 67 years old and may not live long enough(quickly approaching average life expectancy).
"Write the exam or die un-certified" - that is the question.
Passed several Board examinations successfully, but still labelled "not-certified"
Never accused of a medical malpractice in 45 years of medical practice( No law suites or reports to license boards)
Am I a typical example of "Borded to Death" ?
Post a Comment