As most readers of this blog are aware, since 2005 the medical device industry in which I work has had widely publicized instances of patient deaths splashed all over the New York Times and other mainstream media outlets from defibrillator malfunctions that resulted in a just a few patient deaths. The backlash in response to these deaths was significant: device registries were developed, software improvements to devices created, and billions of dollars in legal fees and damages paid to patients and their families on the path to improvement. In addition, we also learned about the limits of corporate responsibility for these deaths thanks to legal precedent established by the Reigel vs. Medtronic case.
Should Electronic Medical Records Be Considered Medical Devices?
This week I received a medical record from a large academic medical center somewhere in the United States (the details are unimportant) that has one of these new pioneering EMR systems manufactured by $13 billion-dollar company, Cerner Corporation. Now before I go on a rant about Cerner's EMR system, I should preface my remarks to say that I have never personally used Cerner's system. But I am a doctor who received a note composed on Cerner's system and what I saw was one of the better examples of how EMR's are contributing to misinformation and confusion when health care is delivered.
I received a copy of an internal medicine consult that was performed on a patient at this outside hospital. I have extracted the "medications" portion of the internist's note exactly as it was displayed in the note below (although the list extended over more than one page, so I joined the list together as one figure). Needless to say, I was terrified at what the system had listed as the patient's medications:
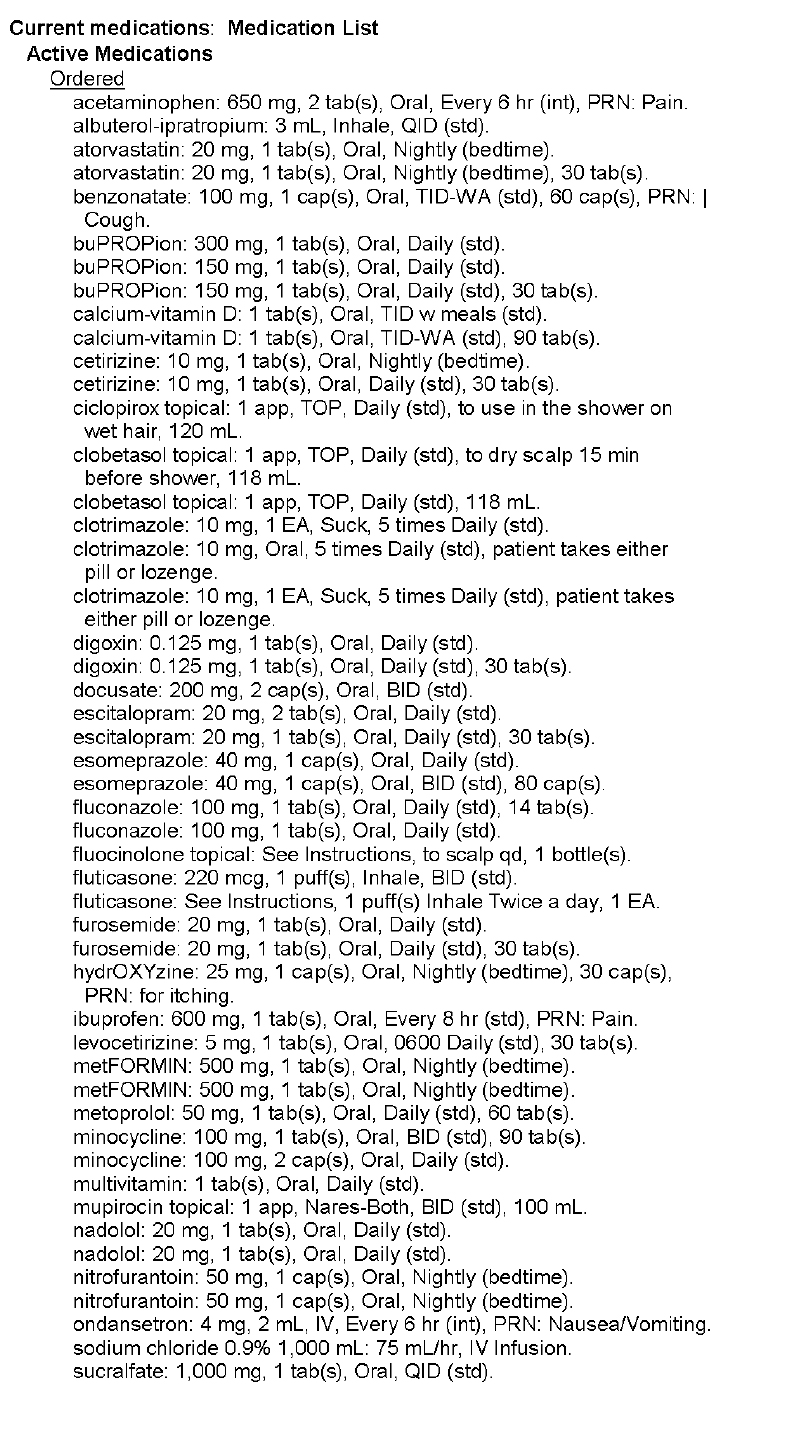 |
| Med List (Page 1) - Click to enlarge |
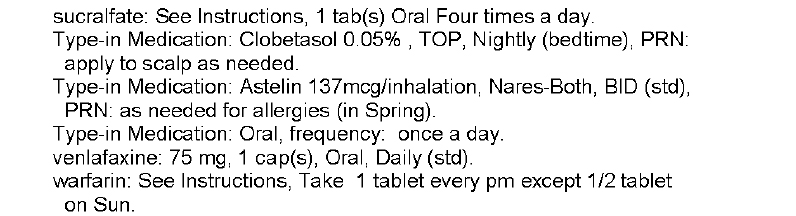 |
| Med List (Page 2) - Click to enlarge |
In this example, we see multitudes of medications listed more than once. We see drugs of similar classes (antihistamines, beta blockers) on the same list. We see warfarin, one of our most dangerous drugs dispensed, without a dose included. We see what seems to be outpatient meds listed with inpatient meds, I'm not sure. Honestly, we really have no idea what medications are actually being taken from this list. And yet this list of medications is listed by the EMR as the patient's "Active Medications."
What the heck have we created?
Certainly, any capable physician who cares for patients would describe this medication list as worthless. So why is it in there? (Don't get me wrong, the fact that any doctor would allow such crap to be displayed in his or her medical note by using an EMR shortcut to enter them uncorrected is beyond me. Certainly, we as doctors must accept a big portion of the responsibility for this).
But when EMR developers and their hospital administration customers purchase software capable of spewing forth completely useless AND potentially lethal information about our patients that is then transmitted far and wide, (not to mention to local direct caregivers) doctors have an obligation to speak up.
These kinds of documentation problems are the EMR's Achilles' heel. But beyond this, EMR software updates are routinely deployed without real-world real-life testing. Ever. And yet, like patients with a defibrillator who die outside the hospital before a root cause of a defibrillator defect can be discovered, I acknowledge that it is incredibly difficult to prove that the death of an individual was caused by an EMR software problem.
And yet, we must.
So how will we measure problems with EMRs? It seems industry representatives would rather not address these concerns. We should ask ourselves, is anyone thinking about this?
Right now, the prevailing belief is that the electronic medical record might be one of the most important medical devices doctors have at our disposal to care for patients. I tend to agree. But it's potential to do harm is also enormous if it is not used responsibly and accurately. After all, as the above example shows, the potential to introduce unintended yet potentially lethal errors into patient care is huge. More importantly, since nearly every person in the United States will soon have their medical data housed within these systems, the number of people that could be adversely affected by these systems is much larger than what we've seen with our recent defibrillator malfunctions.
Perhaps, like the ICD registry, we should try to to develop an EMR registry of adverse patient outcomes caused by these software systems. That way, every independent EMR company can learn from the other's mistakes. Because, guess what ...
... like other man-made medical devices, EMR's are not perfect either.
-Wes
11 comments:
I couldn't agree more. We've all just moved lock stock and barrel to the EMR without assuring that it is used correctly.
I think forcing EMR companies to do clinical trials of their device, with FDA approval, is fabulous. We'll quickly find out if the EMR improves healthcare or worsens it. I tend to think that overall it has not improved things.
Peggy
I agree with you completely, but while some of it is including every medication that was ever taken (somebody has to understand that a patient's medications change over time)a lot of it has to do with coding. I have instances where the code DIAB W/O COMP TYPE II/UNS NOT STATED UNCNTRL is used for Pre-diabetes and Hypoglycemia is used instead of Hyperinsulinemia from the same doctor at the same appointment. In the "All Insurance Information" tab of my PHR for a recent hospitalization lists Coronary atherosclerosis as a diagnosis when a Cardiologist and his PA both came into my room to tell me that the nuclear stress test showed no signs of blockage. This is just the record that is contained in my insurance file and (I hope) is not a part of any national EMR. The thought that any physcian would use faulty information like this to actually treat me is terrifying. Way back in the far away reaches of this same record is a diagnosis for Lymphoma, which I have never had. It used to contain a diagnosis of prostate cancer. I only have to wonder who made that mistake, but that one was fought quite sustinctly as I am a female. It's really sad, because this could be such a useful tool, but it is too fraught with errors to be relied on.
Unf***ing believable! The last science course I had was in high school and I could see that the list was a joke. And I gave myself extra points because I noted there was NO dosage on the warfarin before the good doctor pointed it out.
It's up to you docs to scream when you get this kind of junk. You know. Sorta like the NYT splashing medical device failures across their pages. But patients like Lisa may be able to provide some help if given a printout. Loved that she was able to point out she didn't have a prostate.
To focus this conversation, we should all realize just who is the "bogeyman".
http://www.healthcareitnews.com/news/farzad-mostashari-man-digital-mission
Dr. Mostashari understands that adoption of electronic records will be 'disruptive' but he could care less. It is full speed ahead. Do you think that Cerner, GE medical, microsoft, Oracle, Dell, etc., etc., had any lobbyists in DC ensuring that the porkulus bill contained free money for them?!
Hello doctors, are you listening. Your practices were just a pass-through used to move money to technology companies. We don't have enough to pay the doctors but miraculously there is plenty to spend on technology 'upgrades' that will 'improve' patient care. That message was bought and paid for by YOUR tax dollars. Think about it for a minute.
Garbage in; garbage out. Many of the notes that I see are largely constructed through cut and paste and predetermined population of the note with gobs of extraneous information. All designed, as best as I can tell, to increase reimbursement. In doing so, what is created are notes that are difficult to disect and find the information that is most important.
These systems for the most part are not ready for prime time. They have little in the way of clinical support and as best as I can tell, have done nothing to actually improve quality of care or diminish the cost.
Hell yes, they should be more closely regulated and subjected to the rigors of clinical testing. But in the tradition of American medicine, we tend to hype the product (think Da Vinci robots and Proton Beam radiation) before we fully understand the proper place and limitations of a new technology.
"the prevailing belief is that the electronic medical record might be one of the most important medical devices doctors have at our disposal to care for patients"
Really? I don't know any practicing doc who still thinks that.
It's become very clear that EMRs are all about data collection, and for docs are just one more obstacle that we need to work around.
Oh yes, others are thinking about this.
See my posts since 2004 at Healthcare Renewal blog starting with http://hcrenewal.blogspot.com/2012/05/why-non-medical-amateurs-need-to-be.html as well as my longstanding academic site "Common Examples of Healthcare IT Difficulties" at http://www.ischool.drexel.edu/faculty/ssilverstein/cases/.
-- SS
As it happens, I practice at a hospital that's implementing the Cerner system right now, and I can say with absolute certainty that I've contributed to more life-threatening near-miss errors (thankfully, as far as I'm aware no one's actually been injured by my care, although I've heard some stories...) in the last 72 hours than in the previous five years. EMR's, especially with CPOE implemented, have the potential to make medicine safer, more efficient, and more based on data with appropriately designed decision support tools. They also have a tendency to encourage gobbledygook (and largely false) documentation, interfere with the cognitive process, and enable whole new categories of errors, especially when the programmers of said systems seem to have left their last job programming inventory systems for a widget factory without noticing that every decision they make about data architecture, information display, etc., etc. has actual, real-world consequences for the care of real patients.
But, hey, if having the doctors spend their mental energy on data entry rather than thinking about how best to treat th patient makes life easier for the billing department and the purchasing people, then where could the harm possibly be?
Spot on, Dr.Wes You exemplify the toxic impact that the CPOE device has on medical care.
****The FDA has been informed of the magnitude of the problem but has been marginalized by The POTUS via Sebelius and ONC Chief, then Blumenthal.
After the FDA leadership was educated around 2007, it recognizes that EHR, CPOE and CDS instruments are devices according to the definition set forth in the F D and C Act.
What can get the FDA to do something when it has been told not to do anything by Sebelius?
In my impression, you need to report every incident, injury, death, near miss, downtime delays in care and associated neglect, defect, flaw etc involving the device to the FDA at MedWatch; try to get stories of such in the mainstream media eg NY Times (they drink HIT kool aid); complain to your Congress Reps and Sens; and instigate negligence lawsuits against hospital folks who bought the devices and the HIT vendors themselves.
Good luck and spread the word.
Dr. Mostashari understands which adoption of electronic registers is 'disruptive' however he could care less. It is complete speed ahead. Do you think which Cerner, GE medical, microsoft, Oracle, Dell, etc., etc., had any lobbyists in DC ensuring which the porkulus bill contained free funds for them?!
Hi doctors, are really you hearing. Your own practices were simply a pass-through accustomed move money to technologies companies. We don't have enough to pay the doctors however miraculously there is loads to spend on tech 'upgrades' that will 'improve' individual care and attention. That message was actually bought and also paid for by YOUR income tax bucks. Think about it for a minute.
One of the most important things I've learned over the years is that its the people that make or break the (EHR) system.
My question is why the patient's meds had not been reconciled at what I assume was the last transfer of care? We can't blame the software for this lack of use. Some EHRs are easier to use and more intuitive than others, but I am of the opinion that they are ready for prime use, but only for providers that will be proprerly trained and able to handle the major differences in transferring from the paper to the digital realm (which does NOT include either of my parents who have clinical backgrounds). I have experience with dozens of EHRs and while Cerner certainly is not one of my favorites, it has a completely functional medication tracking fucntion, but it does not update itself.
Post a Comment