You are called to evaluate an older woman who presented to the ER complaining of shortness of breath for the past several weeks, but now is spiking fevers to 102 with associated rigors. She had bilateral lower lobe rales and her chest xray suggested the presence of a right lower lobe infiltrate. She had undergone an uncomplicated pulmonary vein isolation procedure two years prior for paroxysmal atrial fibrillation but had some persistent atrial tachycardia after the procedure well-controlled on atenolol 50 mg twice a day. Her white count and troponin levels are normal. A V/Q scan to evaluate for pulmonary embolus was low probability for pulmonary embolus. Interestingly, her initial EKG looked different than her baseline EKG:

Click image to enlarge
Eight minutes later, the nurse notes a change in the EKG and decided to perform another EKG:

Click image to enlarge
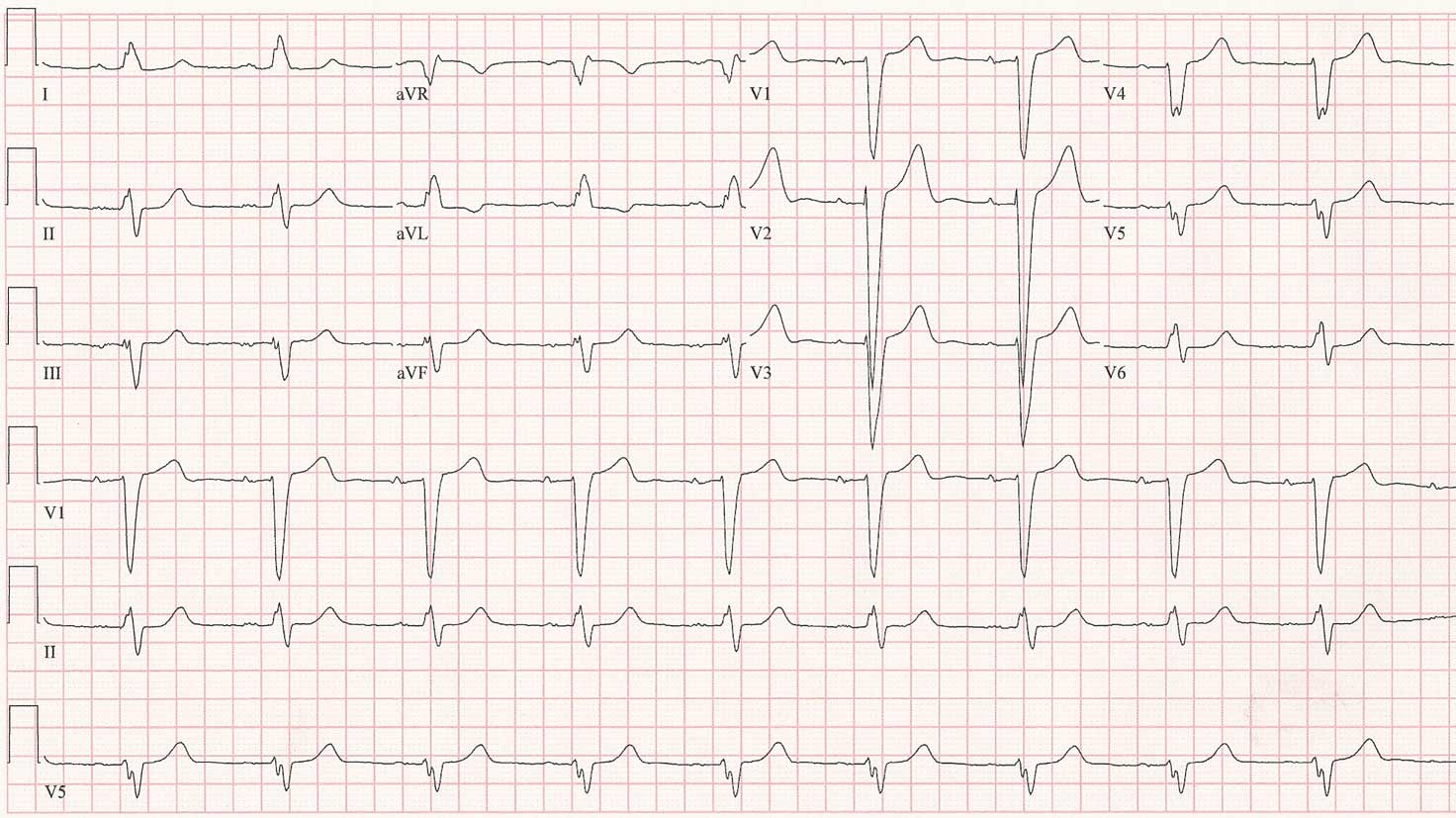
For reference, here's what her baseline EKG looks like on her usual atenolol dose:

Click image to enlarge
So, how do we explain what's happening in the first two EKG's? Does she need a pacemaker?
-Wes


5 comments:
Her baseline tracing shows LBBB and mild sinus bradycardia.
The current tracings show atrial bigemeny. (Possibly ectopic atrial bigemeny, because the p waves look slightly different from the sinus p waves of the old trace). This may represent a left atrial ectopic focus, as evidenced by the positivity of the p waves in V1, which is sometimes seen after pulmonary vein ablation. That was also probably the focus of the atrial tachycardia she had after ablation.
The premature beats are nonconducted due to their prematurity. The post pause atrial impulses are almost all nonconducted due to interference from the escape rhythm. The latter has RBBB configuration. Why? The escape focus could be in the left ventricle, perhaps from the posterior fascicle, or from the His bundle with an eccentric focus of activation causing preferential conduction down the left bundle. Maybe she just has bilateral bundle branch disease.
Does she need a pacer? If she has bilateral bundle branch disease, maybe. That’s a tough call.
Apparently she now has pneumonia, but why short of breath for several weeks? Has she had this rhythm that long, or is she suffering from pulmonary vein stenosis due to the ablation?
What bothers me is the fact that in the ECGs where she has the RBBB pattern, the PR is very short, and actually seems to be getting shorter with every beat. Is that AV dissociation, and the RBBB is due to an escape rhythm originating in the LV?
I think she does have atrial bigeminy in the context of a complete AV block. If so, then she does need a pacemaker.
RW and commotiocordis-
Great work. Sorry I took so long to respond (vacation – what can I say?). I would add first degree AV block to your interpretation of the patient's baseline sinus bradycardia and LBBB seen in the third EKG, the patient’s baseline tracing.
The first EKG demonstrates a ventricular (or possibly fascicular, as you surmised) escape rhythm of a right bundle morphology that is nearly isorhythmic with the patient's underlying sinus rate, thought the ventricular rate is just a bit faster. Frequent atrial ectopy in a bigeminal pattern is noted in the patient’s T waves on this EKG, but at first glance it is difficult to ascertain if this P wave represents a retrograde P wave conducted from the ventricle via the AV node or a repetitive ectopic atrial focus firing in a bigeminal pattern. The clue comes with the second EKG.
In the second EKG, we see the same nearly isorhythmic competing RBBB ventricular escape rhythm that eventually occurs early enough so that the atrial ectopic beat no longer finds the AV node refractory and conducts to the ventricle by way of the AV node, albeit with a slightly prolonged PR interval. This proves the atrial origin of this complex and would fit nicely with the patient’s history. The AV nodal conduction of the sinus and atrial ectopic beat persists until the ventricular escape rhythm rate again approaches that of the underlying sinus rate. As the ventricular escape rhythm again exceeds the sinus rate, progressive fusion of the QRS complexes between the ectopic focus and the normally-conduced LBBB beats are seen (the best example seen in the second-to-last narrowed QRS complex). In effect, then, there are three rhythms occurring in this series of EKG’s: sinus rhythm, and atrial ectopic rhythm, and a ventricular escape rhythm, likely stimulated by the patient’s competing adrenergic state due to shortness of breath. Since her AV node always conducts as expected, and the patient was not symptomatic from the arrhythmia, but rather her underlying pneumonia, beta blockers were held and a pacer was never deemed necessary.
Overlooked that second to the last QRS. Normalizing fusion. Two wrongs occasionally DO make a right!
I know this is a really old post but I was looking for some information after having my first EKG.
To R.W, not that he'll ever see this I guess, but it'd be interesting to know, since it was a close call as to whether to fit a pace maker or not, how would you have ultimately made that decision?
Considering admitting there was something overlooked, how can I be sure that my doctor isn't going to overlook something and recommend a pacemaker? Of course, I would get a second opinion but as they say, two wrongs don't make a right :)
Post a Comment