These days, pacemakers and defibrillators are often interrogated via a home-monitoring system that uploads information contained in the implanted cardiac devices automatically to a central server so it can be accessed by physicians remotely. This feature was added to most defibrillators after the rash of recalls struck the industry in 2005-6. Not only can the information be uploaded electively by the patient, it can also be automatically uploaded if a nightly self-check detects a parameter out of range. In this case, the patient was being monitored by Medtronic's Carelink remote monitoring system.
"Dr. Fisher, I think we have a problem with Mr. Smith's RV lead (not his real name)," my device nurse said as she handed me the Carelink transmission that triggered an superior vena cava (SVC) high voltage coil impedance warning:
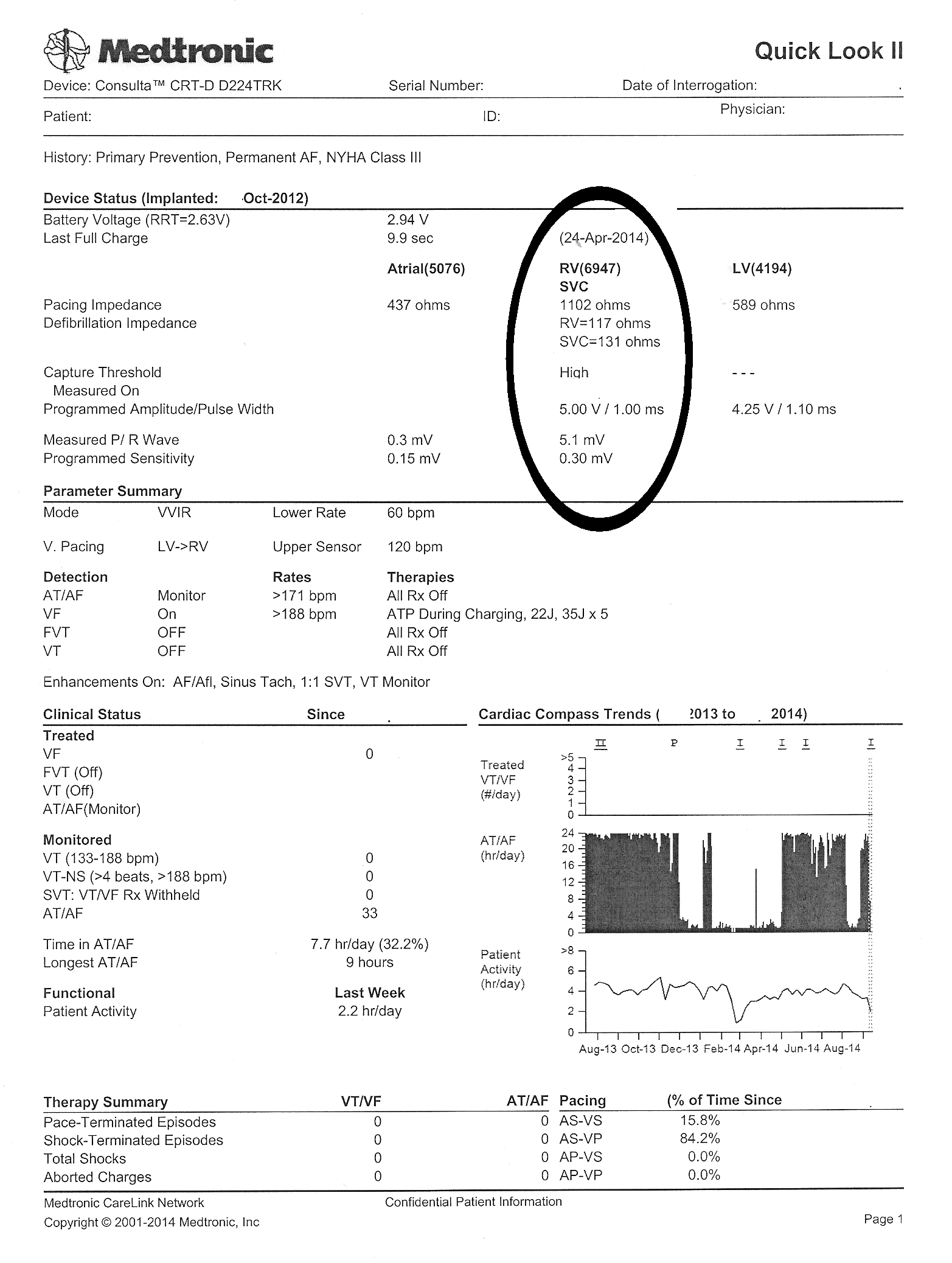 |
| Click to enlarge |
"What did the last interrogation look like?" I asked.
"Here's the old one was sent just three days before and looked fine," she said. "It's so weird. We've not had a problem with this patient's device since it was implanted in 2012."
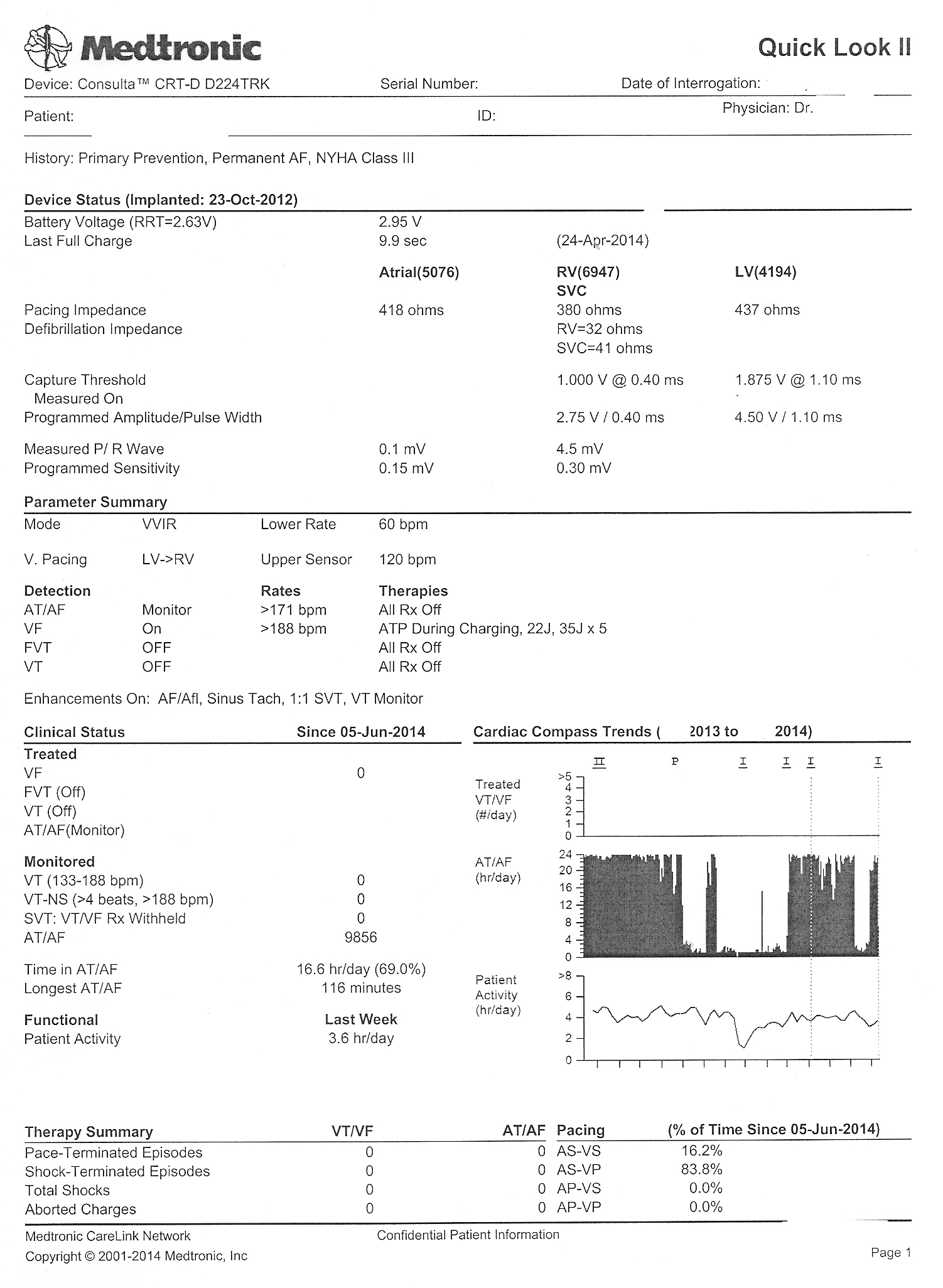 |
| Click to enlarge |
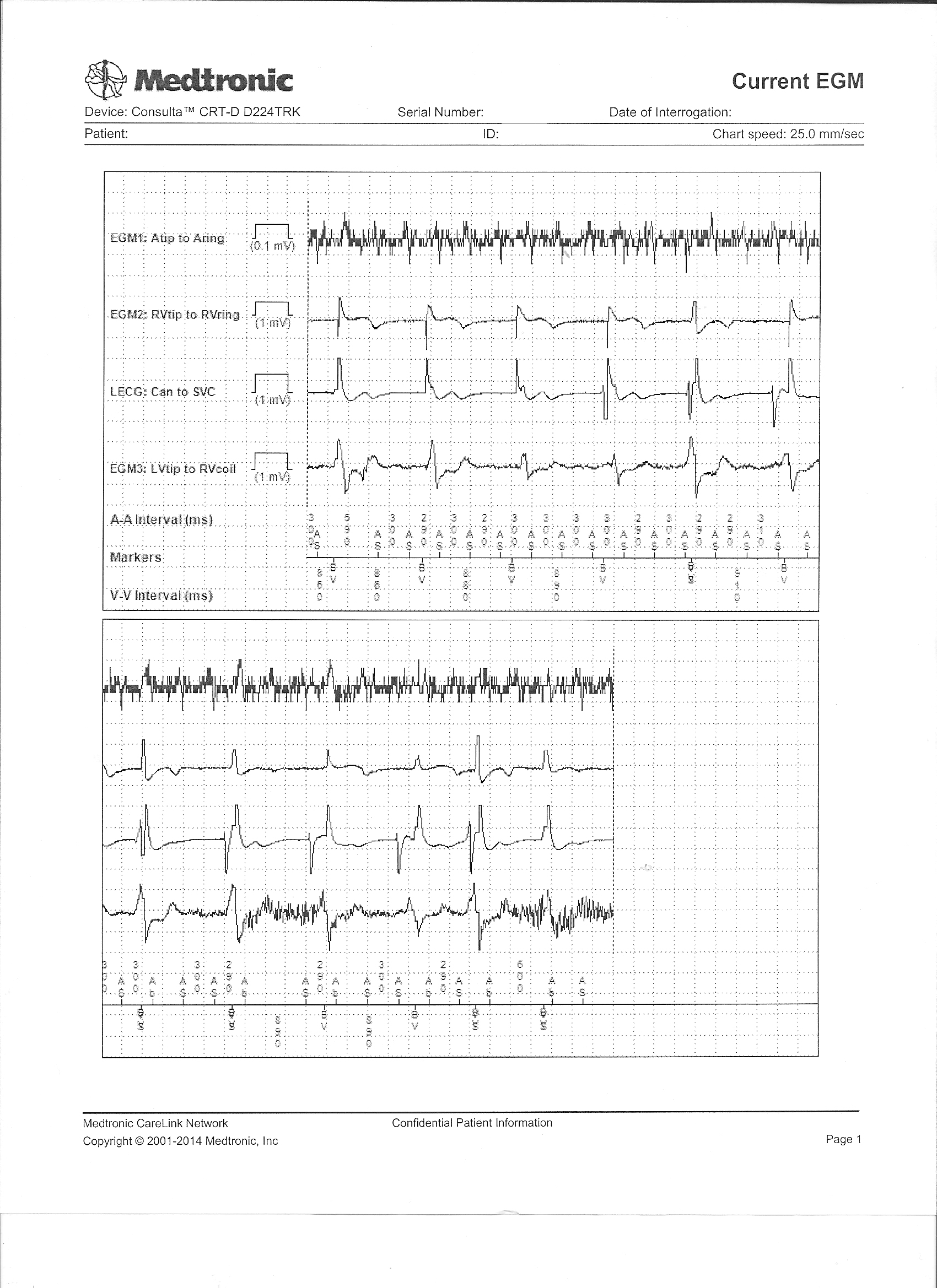 |
| Real-time intracardiac electrograms seen on the earlier transmission - Click to enlarge |
"Strange. I'm not sure what to make of this. Give him a call - we might have to change that RV lead," I said.
"Okay," she said, then returned to the device clinic and I went back to seeing patients.
Some time later, my nurse returned.
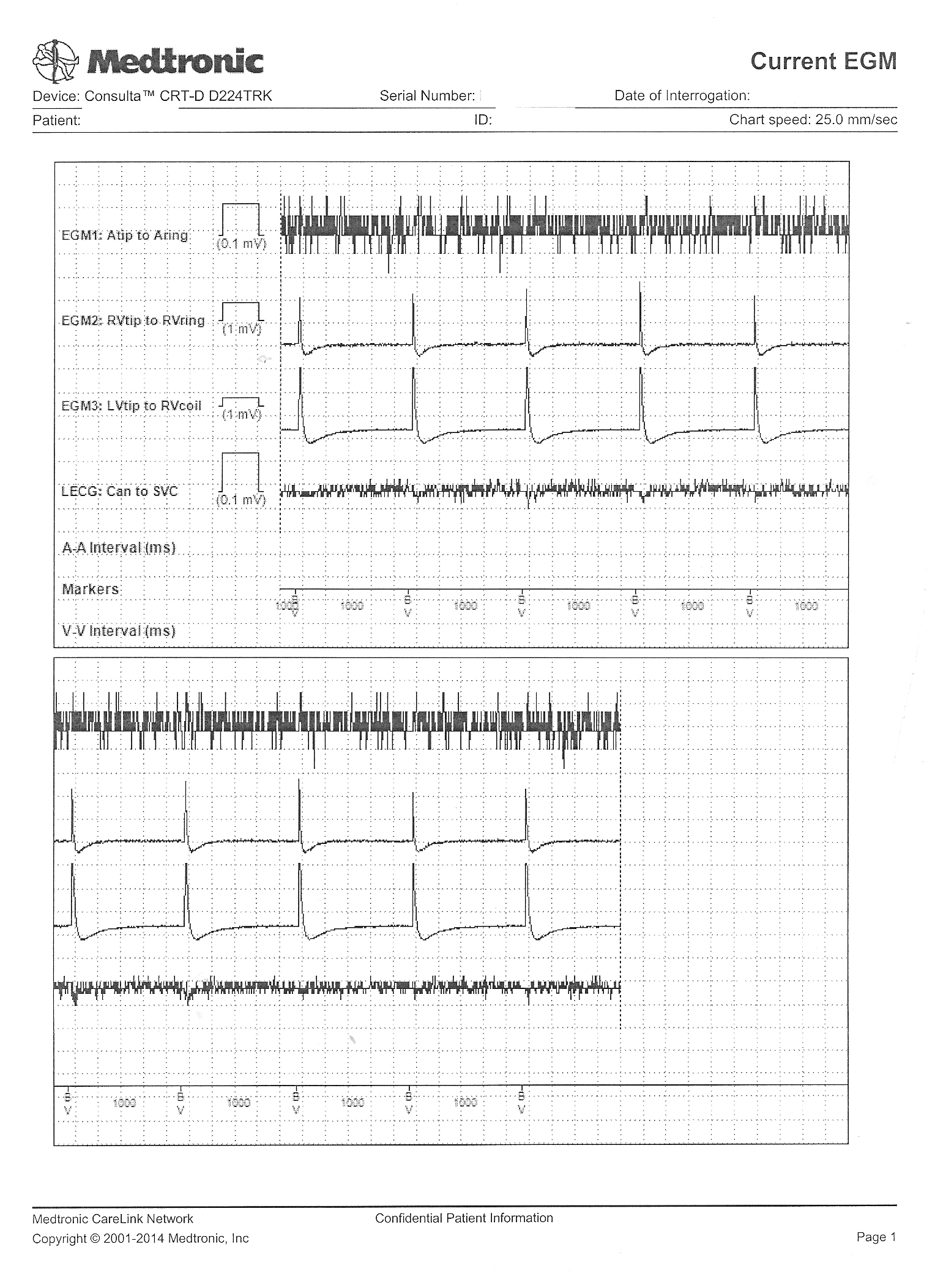
"Um, Dr. Fisher, could I speak with you a moment?" she asked. "I got some more information. I think you better look at this" and she handed me his most recently transmitted real-time intracardiac electrogram recording that was sent with the latest transmission.
{kind=link}
What did it show and why were the RV lead parameters abnormal?
-Wes
5 comments:
Did you have the patient check their pulse? Thanks for sharing!
What time did the patient pass away? Looks like the technology outlived the patient, unfortunately.
Anony 07:18 and 12:47 -
The absence of a 'CAN-SVC' electrogram (which substitutes as a surrogate for a surface EKG) as well as (1) the rise in impedance (and RV 'capture' threshold) across all electrodes on the RV lead and (2) the absence of an evoked potential on the intracardiac electrograms obtained confirms the fact that the patient had expired some time before the most recent transmission and was in proximity to the base station at the time. The lack of cardiac arrhythmias detected by the device suggests (but does not exclude) a non-cardiac etiology for the patient's death.
It is rare to see the physiologic consequences of death as 'witnessed' by our newer transtelephonic means of device interrogation - hence the reason I thought this case might be educational.
Hi Wes, perfect, It blends perfectly with the concept that home-monitoring is one thing and patient monitoring a different one. May I use this case and tracings (with the adequate credits) for teaching purposes)? Rgds
Dr. Halperin -
Please feel free to use these images for your teaching efforts. Thanks for asking.
Post a Comment