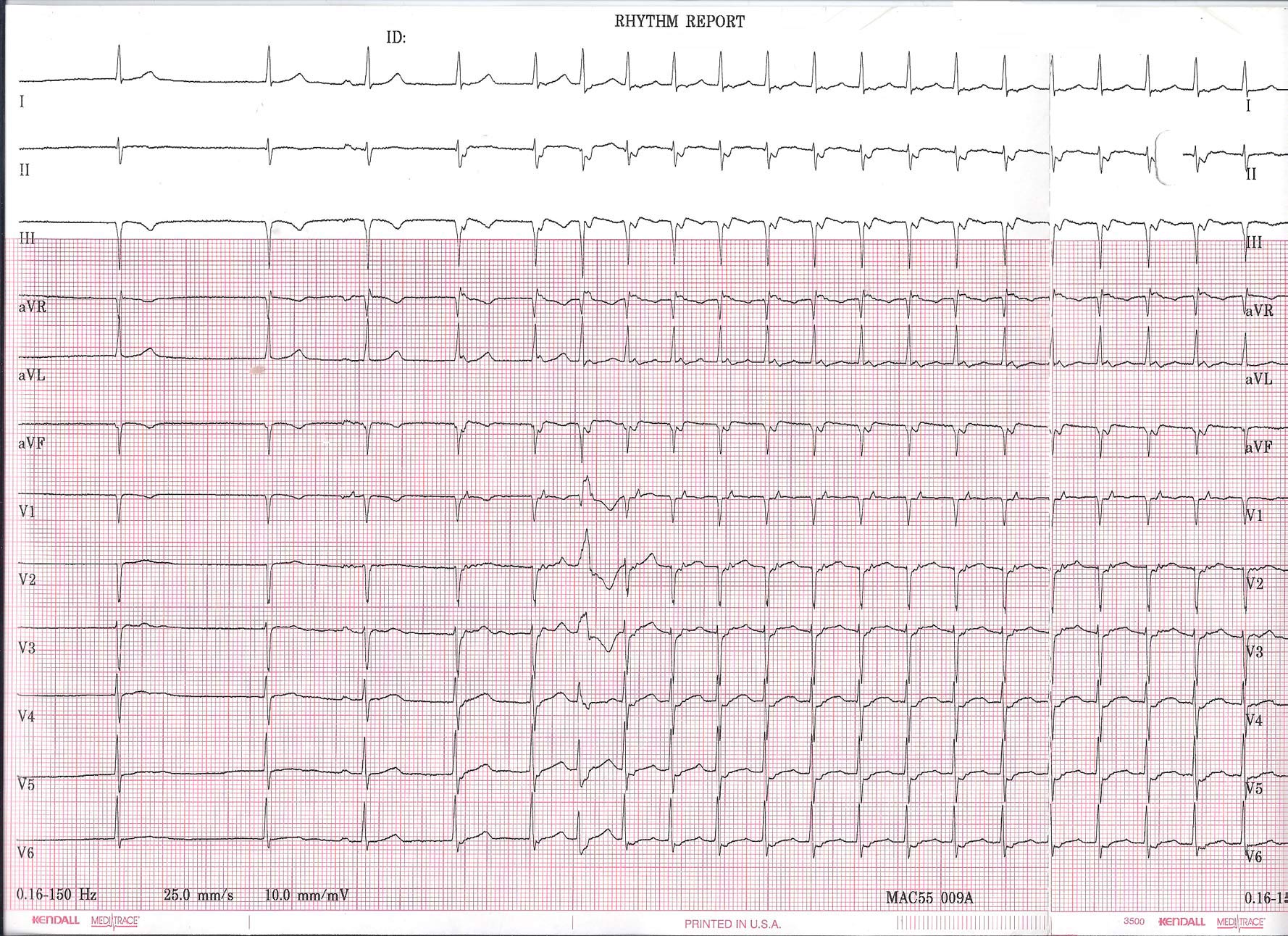
As a refresher, the original 12-lead rhythm strip obtained on this healthy, asymptomatic individual looked like this when he presented for evaluation of two near syncopal spells:
Click image to enlarge
The third beat is where things get interesting. Here, a P wave is clearly seen that conducts to the ventricle with a normal PR interval. What is unsual, however, is the finding that the fourth beat (that appears to be junctional) occurs earlier than one would expect than a junctional escape beat to occur (based on the earlier two junctional beats). In effect, this fourth beat appears "pulled in" earlier to the preceding beat, but also has a clearly visible retrogradely-conducted P wave (best seen in V1) that occurs immediately after the QRS complex. At this point, the patient is in a supraventricular tachycardia that accelerates slightly with the fifth beat occurring earlier - probably because of hemodynamic alterations that occur due to the unusual cardiac activation sequence (slightly decreased BP and increased catecholamine level).
The sixth beat is a widened QRS complex of RBBB morphology. This beat is either a PVC (less likely) or (more likely) an aberrantly-conducted supraventricular beat. This beat aberrates because of the long-short nature of the initiation of the tachycardia that finds the right bundle branch refractory while the left bundle branch conducts to the ventricle. With continued tachycardia, the right bundle branch recovers and the tachycardia continues with a narrow QRS morphology.
The very last beat of the tracing defines the end of the run of supraventricular tachycardia.
So how did the tachycardia initiate?
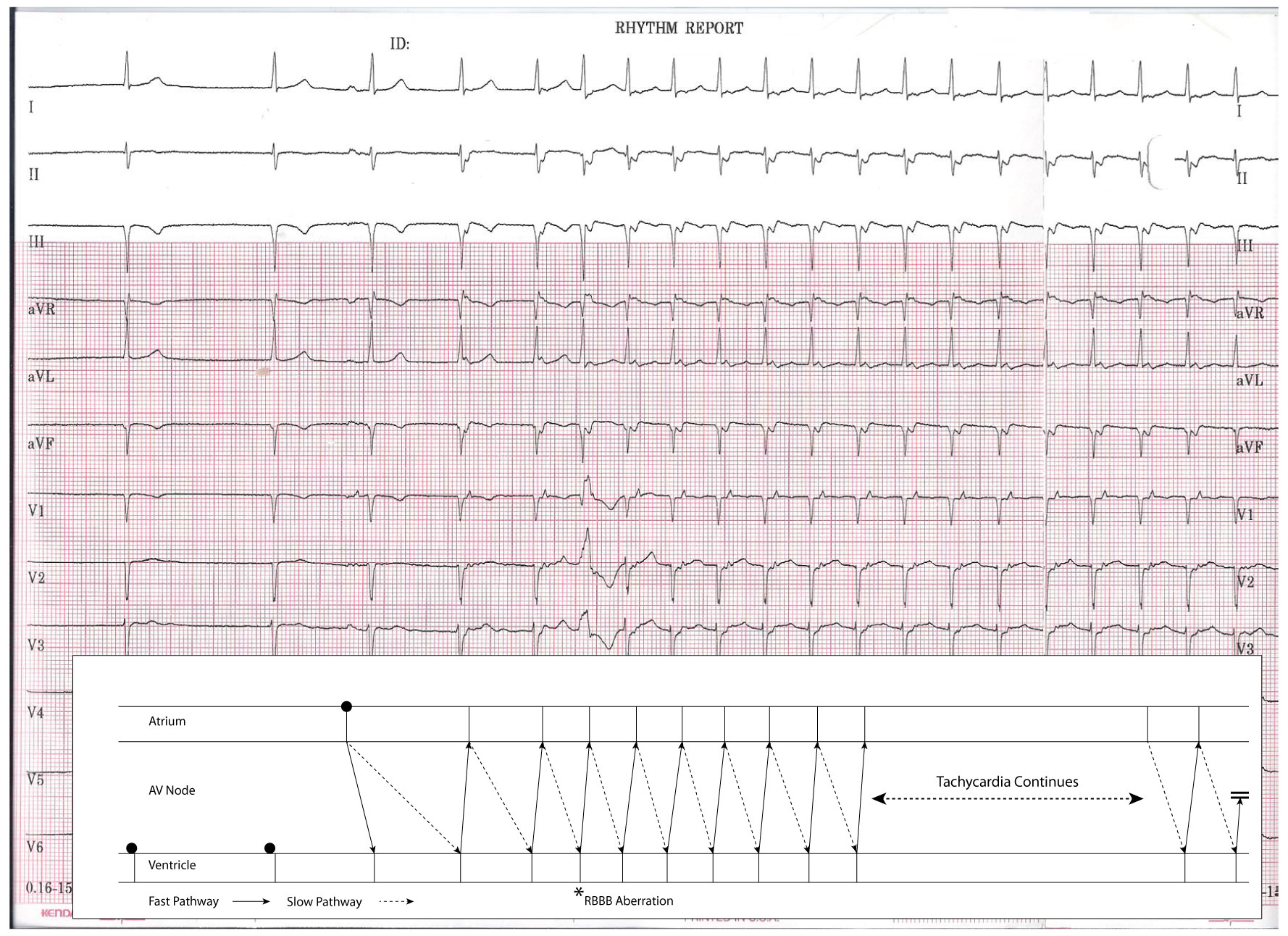
This is an example of a normal P wave initiating SVT due to AV nodal "double-fire." That is, a single atrial beat conducts down BOTH the fast and slow pathway of the AV node. In this case, typical AV nodal reentrant tachycardia was initiated by a single sinus beat in this gentleman.
Here is the above tracing explained using a favorite of EP's -- a ladder diagram:
Click image to enlarge
-Wes
Very interesting; the fact that the P wave was the initiator of the SVT had me focused on atrial conduction travelling along either the fast OR the slow pathway, but not both.... sleight of hand, I tell you!!! This was a great one
ReplyDeleteI happened upon your blog when I googled biventricular pacing. I am new to the world of EKG's (working in a telemetry unit) and this is amazing! Thank you for the education, even though I am still puzzled about a case of v pacing in the 70's(underlying atrial flutter) with a 11 second 17 beat run of WQRS/biventricular pacing. I am going to keep coming back here, very interesting!!!!
ReplyDelete