I've encountered this about eight times in my professional career and used to dread finding this. Now, providing it's not too late on Friday afternoon, I rather enjoy tackling a case like this.
I know the electrophysiologists out there know what the main finding is here, but do others?
-Wes
Nice, won't give it away.
ReplyDeleteAbout a half dozen for me.
Seems always when the schedule is full.
JMM
Absolutely no clue, of course - but I'm interested to find out.
ReplyDeleteMy first guess was maybe it had something to do with lungs, I'm not an EP so my next best guess will probably be just as amusing to you but I think the SVC is in the wrong position. Judging by DrJohnM and your comments, this then leads me to guess that the lead positions will need to be verified, especially the atrial lead, maybe the SVC is emptying into the left atrium?
ReplyDeleteApologies in advance if you were drinking something while reading this and your screen/keyboard is ruined.
Saline bubbles from the left arm?!?
ReplyDeleteGood thing you weren't putting in a CRT...
ReplyDeleteThis looks like the 5PM retinal detachment in my office on a Friday afternoon.
ReplyDeleteGary L
Persistent Left SVC?....its kinda hard to see the loop in the fluoro.
ReplyDeletePersistent L SVC?
ReplyDeleteCardioNP
Love these too. Sometimes when I'm having a good day I'll actually hope to find this when I'm getting access.
ReplyDeleteI actually was lucky enough to have three during my fellowship at Cleveland Clinic. Since then, I've probably seen another 8-10.
I've done two BiV's with this finding. I'll pass on a technique that works later if anyone wants to know.
Jay
Not being an EP, I can provide possibly absurd guesses:
ReplyDeleteleads implanted via subclavian artery ?
or a transposed SVC ?
and
right atrial wall puncture ?
A.B. PhD
I don't know but the path of the leads look weird. I thought the leads usually swept right into the SVC into the RA and RV. In this case, it looks like the leads take an arterial passage into the LV. But I can't imagine a cardiologist would mistaken that.
ReplyDeleteIs this an azygous or a left SVC that the wires have traversed?
So, it is actually an IPod running a Cardiac-Monitor app?
ReplyDeletePersistent L SVC.
ReplyDeleteDo you worry about increased risks down the road with more lead bends/tortuosity (esp RV and/or LV) for rare chance these leads need to get extracted well in the future? vs. just moving to R-sided implant with this anatomy
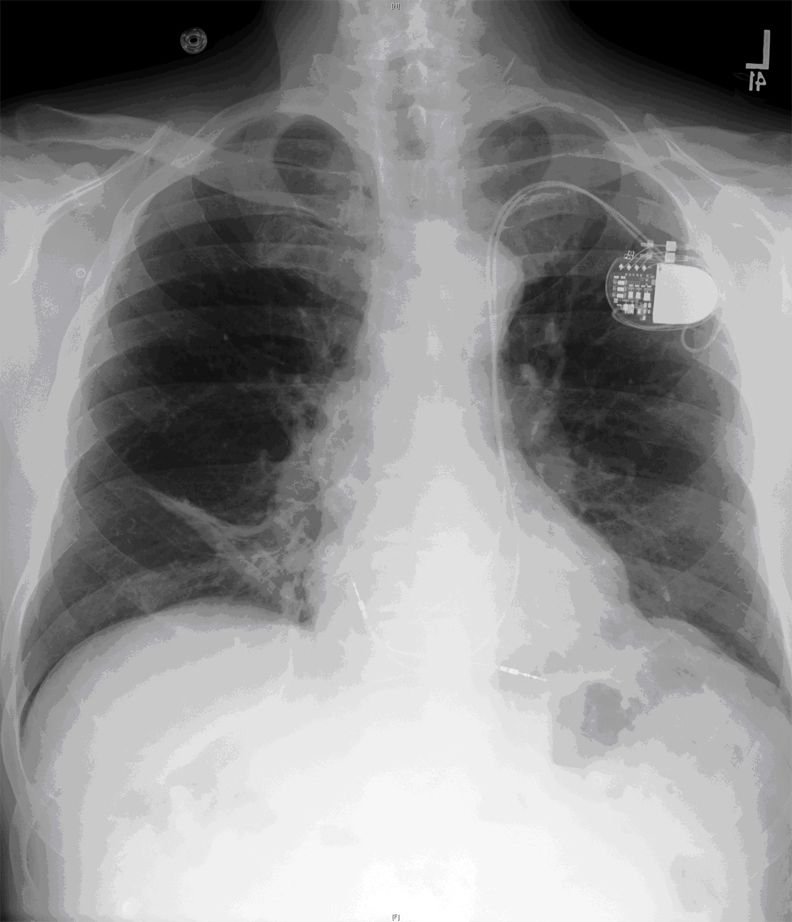
The chest xray demonstrates the presence of a persistent left-sided superior vena cava (SVC) that communicates with the coronary sinus (posterior to the mitral valve annulus) and then drains into the right atrium.
ReplyDeleteLeft sided SVC is the most common congenital venous anomaly in the chest, seen in 0.3 - 0.5% of the normal population and in 4.4% of those with congenital heart disease. The vast majority of the cases have the left sided SVC drain into the coronary sinus which drains into the right atrium, causing little functional problem. A small minority of cases can result in a right to left shunt if the coronary sinus is "unroofed" and drains into the left atrium.
It commonly (90%) occurs with a persistent normal right sided SVC which is also termed SVC duplication, however in 10% of cases it is found isolation with no right sided vessel.
The enlarged size of the coronary sinus in these patients makes localizing branch vessels that might accommodate the left-sided pacing lead used in biventricular devices challenging. Performing a coronary arteriogram and looking qat the levophas to identify branch vessels can be a helpful manuever in challenging cases.
Hmm. late. Sorry about the typos. Translation of above:
ReplyDelete"qat" = "at"
levophas = "levophase"