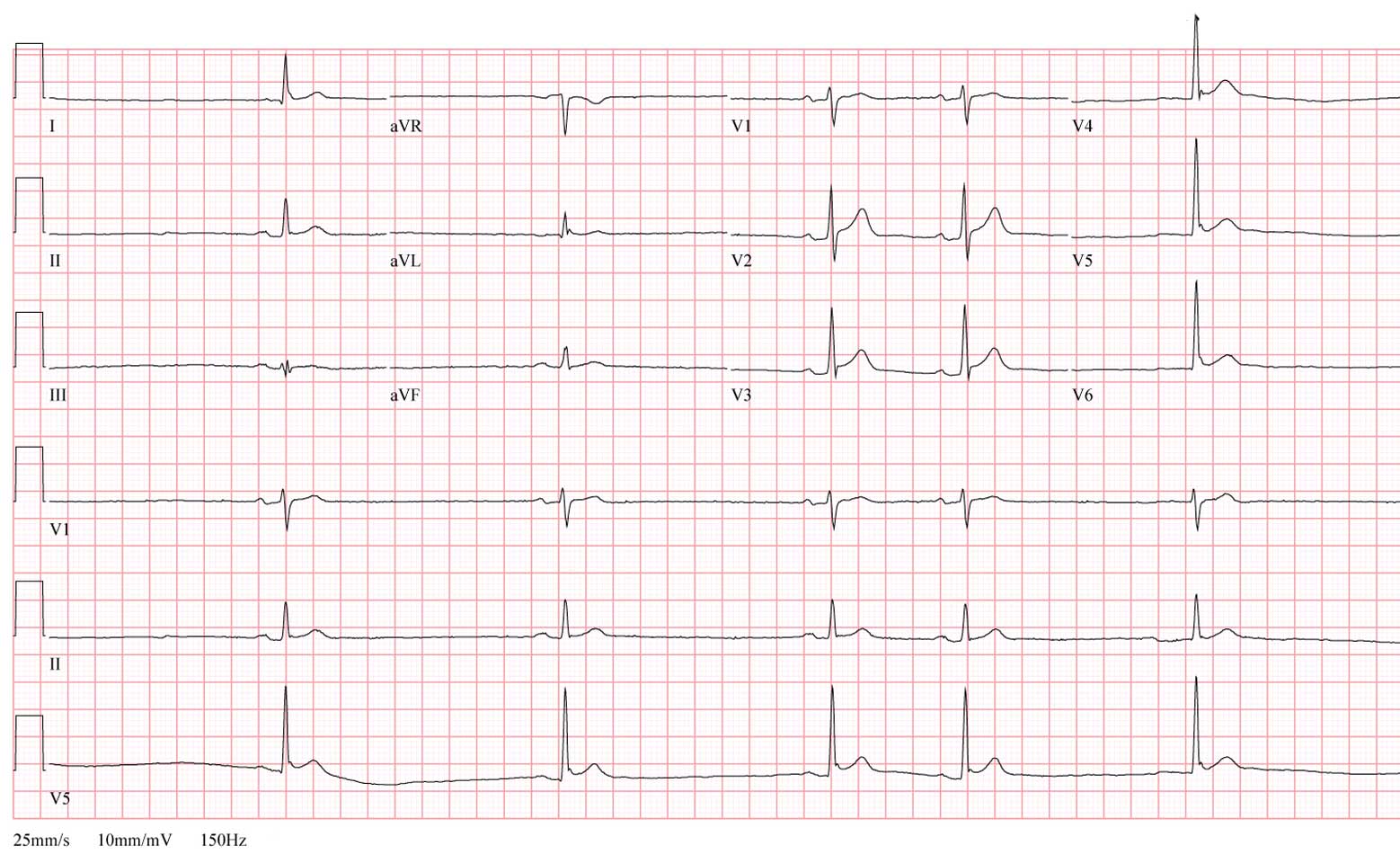
A 60 year-old man was found obtunded, unable to ambulate or communicate at home by a house cleaning service. He was brought to the emergency room and found to by hypotensive, bradycardic and was intubated emergently due to poor ventillatory effort. His initial potassium was found to be 7.6 meq/L and a slow junctional escape rhythm of 40 b/min. He was administered calcium, insulin and glucose, and the EKG, shown below, improved a bit.
Click image to enlarge
An astute observer glanced at the EKG and posed an important question to the ER staff.
What was the question?
-Wes
Addendum 18:45 CST - The EKG image was updated to permit better enlarged viewing.
"Was the initial blood specimen hemolyzed?"
ReplyDeleteI don't see the tall peaked T-waves associated with hyperkalemia*. Was the initial potassium level spuriously high from a hemolyzed specimen, and therefore not the actual cause of his condition?
*That's about all I know about EKGs and electrolytes.
#1 Dino-
ReplyDeleteThe potassium was treated, so the T-waves you were expecting resolved. (Realize that with VERY high potassiums - typically greater than 7.5 - the QRS and T wave also widen...) That's why you don't see the peaked T waves on this tracing, but the potassium value was confirmed...
What's his dig level?
ReplyDeleteHow long was pt down? Body temp? Is there a J wave in V4-V5?
ReplyDeleteThanks to all who gave it a shot, but Michael Katz saw the finding. (I have recently updated the EKG so it can be seen better when enlarged.)
ReplyDeleteThe question asked was "What's the patient's core body temperature?"
When measured, the patient's temperature was 33.2 degrees Celcius (92.1 degrees Farenheit). The EKG shows sinus bradycardia with an occasional PAC, but most importantly demonstrates the early manifestation of an "Osborn wave" (or J wave) of hypothermia in leads V4, V5 and V6. A more prominent example of an Osborne wave in a patient with a core temperature of 85 degrees Farenheit was published in Circulation for comparison.
Over the next 24 hours after rewarming and correcting the metabolic disturbances, the patient's EKG returned to normal.
Yeah. I saw the osborne wave (tiny in this case) but i figured it was.
ReplyDelete1). Not that easy
2). The patient was in doors
I once had a patient with unbelievable classic Osborne waves. You never forget them
I did undergrad and med school in Rochester, NY. Gotta know the J wave. The only thing missing was tremor artifact (aka pseudo flutter). :-)
ReplyDeleteHow did the patient get so cold?
ReplyDeleteNice case. One comment though: it's not a PAC. The P wave morphology is exactly the same, and the coupling interval of the "PAC" is exactly half of the normal P-P interval. This suggests 2:1 sinoatrial block with occasional 1:1 conduction.
ReplyDeletethermodynamics and heat transfer.
ReplyDeleteas long as the room is colder than the combination of (a) his body temperature, (b) his body's ability to generate heat, and (c) his clothing's ability to prevent heat loss, his body temperature and the ambient temperature will always reach equilibrium. especially when given enough time.