Next week I'll be attending our medical school graduation and I wondered what I would tell them if I were chosen to give them a commencement address. This would not be an easy speech to write right now, given all of the uncertainties in health care that lie ahead, but I thought it would be interesting to try. Readers are invited to add their words as well in the comments section.
Dear Graduating Class of 2013 -
I appreciate the opportunity to address such an impressive pool of medical school attendees. From the first day of medical school when you were introduced to your cadaver, you have endured countless lectures and lab hours, physical examination and sensitivity training sessions, and ward rotations under the watchful eye of senior residents and attendings. Today, you will hold something that few people are privileged to sign behind their name: the letters "M.D."
This time in medicine is both a particularly exciting and particularly challenging one for doctors. How you deal with these challenges will determine your staying power in the profession.
During your training and long hours, you carefully cultivated your taste for fine coffee. At first, time allowed for a daily Venti-sized Starbucks mocha latte, but later as you learned the contributions of carbohydrates to your waist line, you switched to "only" black Ethiopian Harrar. Good for you. No doubt your upcoming days of residency will allow you some time to enjoy these delights a bit longer, but rest assured that by the time you call yourself an attending physician, you will be satisfied to drink a late night splash of automated coffee machine chemicals called "Coffee, Black" as you clean up the remaining work load left by residents who have exceeded the work hour restrictions you once enjoyed yourself. With this graduation, your sheltered medical workshop days are quickly coming to a close.
While most of you think this day is about you, realize there are some very important team players that have helped you get to where you are today. First and foremost are members of your family. They have encouraged you, guided you, and likely funded much of your way to this point. And the funding for medical school has been significant. The average medical school costs today, when one includes living expenses, exceeds $200,000. For those of you who did not have family members supporting you, realize that $200,000 of debt obligations translates to $843.21 per month if you plan to pay that loan off over 30 years at a low 3% interest rate. If your interest rate is higher, I feel for you. Yes, Virginia, medical school has become much too expensive.
But there is some good news. For the first time ever, instead of paying in to the health care education system, the health care system will start "giving back" and paying
you. Admittedly at a very low rate. But at least it's your first tiny step in the right financial direction. Hopefully by the end of your residency training, the additional clinical experience you gain will finally allow you to make a bit higher salary than the nurse practitioners you work beside.
Fortunately, each of you began life as a medical student-doctor in the Gilded Age of Information Technology. Anything, you were taught, is possible with enough Big Data. But more data is not always better data. More data can confuse and obfuscate. More data might not be important data. And all that data comes at a cost to you: repetetive motion injuries. You see, Big Data is created from the information you will be asked to enter on your keyboard, iPAD, or via mouseclick or Google Glass. And since Big Data must now include a myriad of new procedure and diagnosis codes that you must learn, residency is not only a time to master disease states, but also a time to master your typing and coding skills. What ever you do, don't let Big Data detract from what matters most: your patient.
Your greatest challenge as a newly minted doctor in this Information Age will be to put your cellphone down. Looking up from its glowing screen will let you see your patient's downward stare as they tell you their deepest, personal secrets. If recognized, a trusting doctor-patient relationship will blossom. If missed, a feeling that you don't care may result. Remember that despite what the information technology zealots have been telling you, patients are not digital widgets, but analog, non-linear, feeling creatures who demand respect and intelligence. If you remember this, you will go far.
Many of you will be switching to new cities and new institutions to begin your residency training at a highly-esteemed medical school now that you've "matched." As you work to learn the clinical side of medicine, stay flexible. Fellowship positions are getting harder to come by as cuts to income for specialists continue. So hang on to those cardboard moving boxes - they might be needed sooner than you think. Honing hospitalist skills will probably be a wise choice, too.
And be prepared to have your heart broken. People will die despite your very best efforts. Complications occur, even to the most skilled and most cautious. Administrators will tell you to do things a certain way when you know that way's inefficient, but it pays your salary. People will deny payments for things that you know they shouldn't. A single malpractice lawsuit, even if ultimately found to be unwarranted, will forever change you - not for the better - but for the worse. And your wife and kids will
still be affected when you arrive home late after missing your daughter's dance recital even though she says, "That's okay, Dad."
 |
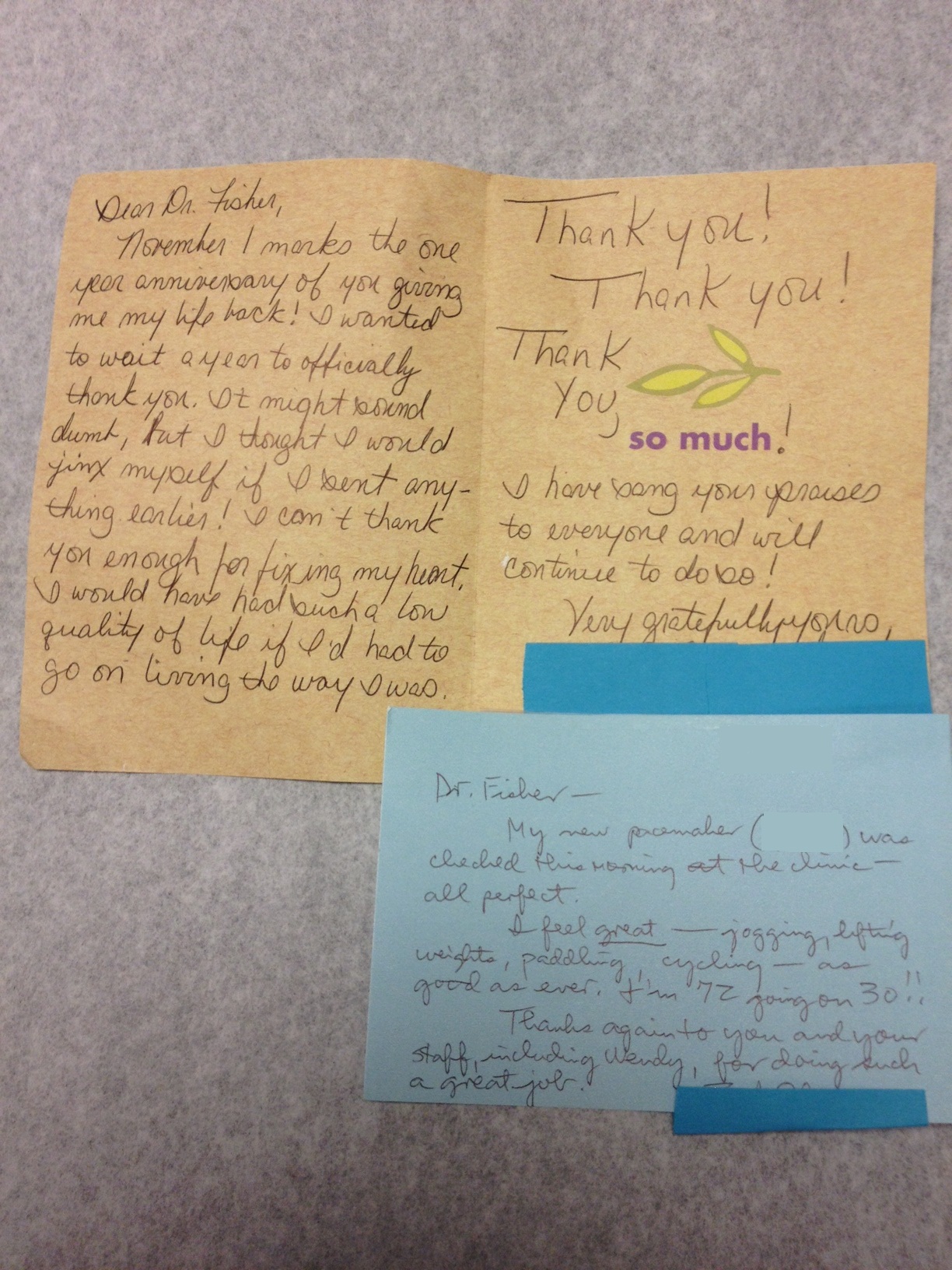
An example of a few much-appreciated
thank-you notes you'll receive
(Click to enlarge) |
But despite all of these realities, there remain some wonderful aspects of medicine. People still will look up to you. People will still respect what you do and say. People will trust you, confide in you, and appreciate your efforts. You can do amazing things for people if you don't let the system get you down. Get involved in the process. Work to set the needs of your patients before that of the system and you'll usually be rewarded.
Because in the end, this is what really matters.
So go forward, not with an artificial glow about all that you have achieved, but with the stark reality of what lies ahead. These are challenging times for doctors as we increasingly encounter efforts to devalue all we've learned and experienced. Work to make the system better. Stay strong, work hard, and appreciate all you've got.
After all, there's plenty of people who would give anything to be in your shoes.
Good luck and God bless each and every one of you.
-Wes